
Abstract
Background
Rheumatic heart disease (RHD) is a serious health concern in developing countries. Rheumatic mitral stenosis (RMS) is the most long-term sequel in RHD. The neutrophil to lymphocyte ratio (NLR) is a novel marker, and a higher NLR has been associated with poor clinical outcomes in various cardiovascular disorders. We evaluated the availability of NLR to predict severity of mitral stenosis (MS) in patients with RHD.
Methods
We analyzed 300 consecutive patients with RMS. The patients were divided into tertiles according to NLR: 0.85< NLR ≤1.85 (n=100, tertile 1), 1.86≤ NLR ≤2.46 (n=100, tertile 2), and 2.47≤ NLR ≤7.08 (n=100, tertile 3). Patients with RMS were divided into three groups based on the degree of MS as mild, moderate, and severe MS. After the initial evaluation, 187 patients with moderate-to-severe RMS (Group 1) and 113 patients with mild RMS (Group 2) were reassessed.
Results
The patients with severe RMS had significantly elevated NLR, mean platelet volume, and pulmonary artery systolic pressure values compared to patients with moderate and mild MS (P<0.001, P<0.001, P<0.001 respectively). Multivariate binary logistic regression analysis revealed that high levels of NLR was an independent predictor of severe RMS (odds ratio =0.68, P=0.008). Moderate-to-severe RMS incidence was significantly higher among patients in the tertile 3 (odds ratio =2.8, P=0.001).
Conclusion
NLR is a new inflammatory marker and a simple, rapid, and easily accessible prognostic parameter that can be associated with severity of RMS in patients with RHD.
Introduction
Rheumatic heart disease (RHD) is a chronic acquired heart disorder resulting from acute rheumatic fever (ARF). Although rare in developed countries, RHD continues to be a major cause of cardiac morbidity and mortality among children and young adults in the developing countries.Citation1,Citation2 So far about 15 million cases of RHD are reported worldwide, with 282,000 new cases and 233,000 deaths occurring annually.Citation3 RHD is more common in females.Citation4 Although ARF causes pancarditis, it primarily affects the endocardium and repeated episodes of autoimmune reactions cause chronic inflammation in the valvular apparatus. Rheumatic mitral stenosis (RMS) is a common manifestation of RHD.
While the pathophysiology has not been fully understood, it is postulated that inflammatory response is the most important part of the pathogenesis of RHD.Citation5,Citation6 The total white blood cell count is an easy, inexpensive, and widely available means of detecting inflammation. Neutrophils are the major components of leukocytes in peripheral blood. The neutrophil to lymphocyte ratio (NLR) was recently reported to be a marker of thrombosis and inflammation and was found to be associated with the severity and prognosis of several cardiovascular diseases.Citation7–Citation9
The aim of this study was to evaluate the relationship between NLR and the degree of RMS.
Methods
Study population
This multicenter retrospective study included 300 mitral stenosis (MS) patients who had been admitted to the Department of Cardiology at the Diyarbakır Gazi Yaşargil Education and Research Hospital in Diyarbakır and Ankara Yüksek İhtisas Education and Research Hospital in Ankara, from January 2013 to June 2014. All the patients underwent a clinical examination, ECG, and transthoracic echocardiography. Patients with diabetes mellitus, hypertension, malnutrition, coronary artery disease, acute corticosteroids use, acute infection, chronic renal and hepatic disease, and hematological disease were excluded from the study.
The patients were divided into tertiles according to NLR: 0.85< NLR ≤1.85 (n=100), 1.86≤ NLR ≤2.46 (n=100), and 2.47≤ NLR ≤7.08 (n=100). Patients with RMS were divided into three groups based on the degree of MS as mild, moderate, and severe RMS. Valve disease severity was defined according to the American Society of Echocardiography and American College of Cardiology/American Heart Association guidelines for the management of valvular heart disease.Citation10 Venous peripheral blood samples were taken on admission. Blood samples were drawn into standardized tubes containing dipotassium ethylenediaminetetraacetic acid (EDTA) and delivered to the laboratory within a few minutes. All hematological measurements were performed using an XT-2000i analyzer (Sysmex Corp of America, Long Grove, IL, USA). This study was approved by the Ethics Committee of Ankara Yüksek İhtisas Education and Research Hospital, and informed consent was obtained from all study participants.
Echocardiography
Two-dimensional and Doppler echocardiography were performed. (Vivid 5 System, 2.5 MHz transducer, GE-Vingmed Ultrasound AS, Horten, Norway). All measurements were taken according to the American Society of Echocardiography guidelines. Mitral valve area was measured by using the pressure half-time method and planimetry of the mitral valve orifice from the short-axis view at the tip of the mitral leaflets. The mean transmitral diastolic pressure gradient was determined by using the Doppler method in the apical four-chamber view. Pulmonary arterial systolic pressure (PASP) was calculated by measuring the velocity of the tricuspid regurgitation jet. Severity of stenosis as defined by the American Society of Echocardiography and endorsed by the American College of Cardiology/American Heart Association valve disease guidelines are as follows:
Severe stenosis is associated with a mean transvalvular gradient >10 mmHg, PASP >50 mmHg, and valve area <1.0 cm2.
Moderate stenosis is associated with a mean transvalvular gradient of 5–10 mmHg, PASP pressures of 30–50 mmHg, and a valve area of 1.0–1.5 cm2.
Mild stenosis is associated with a mean transvalvular gradient of <5 mmHg, PASP pressures <30 mmHg, and a valve area >1.5 cm2.
Statistical analysis
Data were analyzed with the SPSS software version 15.0 for Windows (SPSS Inc., Chicago, IL, USA). Categorical variables were presented as frequency and percentage. The χ2 test and Fisher’s exact test were used to compare categorical variables. The Kolmogorov–Smirnov test was used to assess the distribution of continuous variables. Student’s t-test was used for variables with normal distribution, and the values were presented as mean ± standard deviation. Continuous variables without normal distribution were analyzed using Mann–Whitney U-test, and the values obtained were presented as median (50th) values and interquartile ranges (25th and 75th). One-way analysis of variance and Kruskal–Wallis test were used for parametric and nonparametric variables to compare tertiles, respectively. Multivariate logistic regression analysis was used to evaluate the independent association of the risk of severe RMS. Parameters with a P-value of less than 0.1 in univariate analysis were included in the model. The odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. A two-tailed P-value of <0.05 was considered statistically significant.
Results
A total of 300 consecutive patients were enrolled in the study. The mean age of the patients were 48.5±12.1 years, and 64 (21.3%) were male. The baseline characteristics are presented in . No significant differences were found in the presence of mitral regurgitation, hypertension, diabetes mellitus, and biochemical parameters. The patients with severe RMS had significantly elevated NLR, mean platelet volume, and PASP values compared to patients with moderate and mild MS (P<0.001, P<0.001, P<0.001, respectively). Spearman’s correlation analysis revealed a weak negative correlation between NLR and mitral valve area (rs=−0.244, P<0.001) and a positive moderate correlation between NLR and mean transmitral gradient (rs=0.277, P<0.001) values.
Table 1 Comparison of the patient’s baseline characteristics according to severity of mitral stenosis
After the initial evaluation, 187 patients with moderate-to-severe RMS (Group 1) and 113 patients with mild RMS (Group 2) were reassessed (). The patients in Group 1 had higher NLR values. An univariate linear regression analysis for the relationship between severity of MS and other variables is shown in . Multivariate binary logistic regression analysis revealed that high levels of NLR, PSAP, and left atrium size were independent predictors of severe RMS (). RMS was associated with NLR (OR =0.65, 95% CI: 0.47–0.89, P=0.008), left atrium size (OR =0.49, 95% CI: 0.29–0.82, P=0.006), and PSAP values (OR =0.94, 95% CI: 0.90–0.97, P<0.001).
Table 2 Comparison of the NLR levels according to MVA<1.5 cm or not
Table 3 Independent predictors of severity of mitral stenosis
Patients were divided into three tertiles based on the NLR levels. The relationship between RMS and NLR tertiles are presented in and . Moderate-to-severe RMS incidences were significantly higher among patients in the tertile 3 (OR =2.8, 95% CI: 1.5–5.0, P<0.001).
Figure 1 Patients were divided into three tertiles based on the NLR levels.
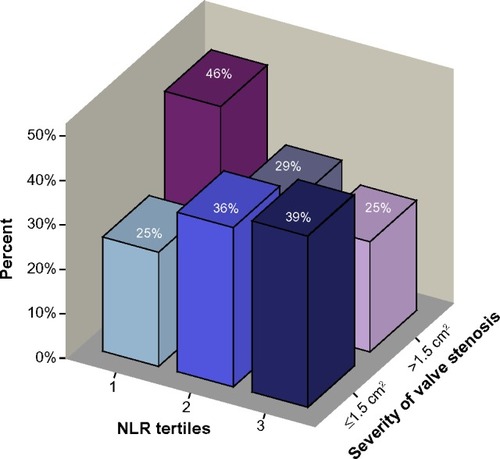
Table 4 The patients were divided into tertiles according to NLR
Discussion
In the present study, we found that an increased NLR was independently associated with the degree of RMS.
Chronic RHD is one of the latest sequels of ARF occurring in approximately 30% of patients with rheumatic fever.Citation11 In case of ARF, several inflammatory cells, such as neutrophils, macrophages, and T and B lymphocytes, infiltrate both the myocardium and the valves. The healing process of rheumatic carditis results in varying degrees of fibrosis and valve damage. RMS is a common manifestation of RHD. Inflammatory process plays a key role in RHD, and previous studies have shown that there is ongoing chronic inflammation in rheumatic mitral valve disease. In the previous studies, it was shown that levels of chronic inflammatory markers were higher in patients with rheumatic valve disease than control groups.Citation12 Gölbasi et al reported that levels of C-reactive protein were higher in patients with rheumatic valve disease than in the control groups and they concluded that this could be a sign of chronic ongoing inflammation.Citation13 Similarly, Alyan et al showed that C-reactive protein was significantly higher in patients with RMS than in the control group and independently correlated with the Wilkins valve score.Citation14 Low-grade inflammation and oxygen radicals released by activated neutrophils can be shown in circulation in the coronary sinus.Citation15–Citation17 NLR, which can be derived from the white blood cell count, is a new marker of systemic inflammation. NLR provides an indicator of the inflammatory status that combines both neutrophils and lymphocytes. The main cause of increased NLR was probably the increased apoptosis of lymphocytes triggered by the increased inflammatory status in RMS. In a recent study, Öztürk et al reported that higher NLR was associated with spontaneous echocardiographic contrast in RMS.Citation18 NLR is a new marker of inflammation that is associated with the severity of coronary artery disease, long-term mortality in patients undergoing primary percutaneous coronary intervention, and cardiac mortality in patients with stable coronary artery disease.Citation7–Citation9 In a recent study, it was reported that a high NLR was associated with thrombolysis failure in ST-elevation myocardial infarction patients treated with thrombolytic therapy.Citation19 Horne et al reported that higher NLR was associated with worse clinical outcome in patients with ischemic heart disease without ST-elevation myocardial infarction.Citation20 In addition to those studies, Cho et al report that NLR at 24 hours after admission is a predictor of mortality in patients with ST-elevation myocardial infarction who undergo percutaneous coronary intervention.Citation21 Turak et al showed that a high NLR predicted in-hospital mortality and cerebrovascular events in patients with infective endocarditis.Citation22
Although Akboğa et al found that NLR was significantly increased in patients with RMS than control groups, NLR did not reach statistical significance in MS groups.Citation23 On the other hand, in a recent study, it was shown that high NLR predicted presence and severity of MS in patients with rheumatic mitral valve disease.Citation24 However, Akboğa et al subdivided the RMS into mild-moderate and severe MS groups; we not only assessed mild, moderate and severe MS groups, but also reassessed mild and moderate-severe MS. Our study differs from the previous studies in that we evaluated the relationship between NLR and the degree of RMS. We subdivided the RMS into mild, moderate, and severe MS groups and showed that high NLR is associated with severity of MS.
Therefore, it may be an auxiliary parameter when used in combination with other parameters known to be associated with RMS.
Our study had several limitations. First, this was a retrospective study and included a relatively small number of patients. Second, we enrolled only patients with complete blood counts at admission. Therefore, the present results cannot be directly extrapolated to all patients with RHD. Third, there is no control group, and this is another limitation of the study.
Conclusion
NLR is a new inflammatory marker and a simple, rapid, and easily accessible prognostic parameter that can be associated with severity of RMS in patients with RHD.
Acknowledgments
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- ThakurJSNegiPCAhluwaliaSKVaidyaNKEpidemiological survey of rheumatic heart disease among school children in the Shimla Hills of Northern India: prevalence and risk factorsJ Epidemiol Community Health19965062678762356
- CarapetisJRSteerACMulhollandEKThe Current Evidence for the Burden of Group A Streptococcal Diseases (WHO/FCH/CAH/05.07)GenevaWorld Health Organization2004
- CarapetisJRSteerACMulhollandEKWeberMThe global burden of group A streptococcal diseasesLancet Infect Dis200556859416253886
- EssopMRNkomoVTRheumatic and nonrheumatic valvular heart disease: epidemiology, management, and prevention in AfricaCirculation20051123584359116330700
- GuilhermeLKalilJRheumatic heart disease: molecules involved in valve tissue inflammation leading to the autoimmune process and anti-vaccineFront Immunol2013435224198818
- HabeebNMAl HadidiISOngoing inflammation in children with rheumatic heart diseaseCardiol Young20112133433921303581
- ShenXHChenQShiYLiHWAssociation of neutrophil/lymphocyte ratio with long-term mortality after ST elevation myocardial infarction treated with primary percutaneous coronary interventionChin Med J20101233438344322166528
- PapaAEmdinMPassinoCMichelassiCBattagliaDCocciFPredictive value of elevated neutrophil-lymphocyte ratio on cardiac mortality in patients with stable coronary artery diseaseClin Chim Acta2008395273118498767
- KayaHErtasFIslamogluYAssociation between neutrophil to lymphocyte ratio and severity of coronary artery diseaseClin Appl Thromb Hemost201420505422790659
- QuinonesMAOttoCMStoddardMWaggonerAZoghbiWARecommendations for quantification of Doppler echocardiography: a report from the Doppler quantification task force of the nomenclature and standards committee of the American Society of EchocardiographyJ Am Soc Echocardiogr200215216718411836492
- Rheumatic fever and rheumatic heart diseaseWorld Health Organ Tech Rep Ser20049231122 backcover15382606
- DavutoğluVÇelikAAksoyMContribution of selected serum inflammatory mediators to the progression of chronic rheumatic valve disease, subsequent valve calcification and NYHA functional classJ Heart Valve Dis200514225125615792187
- GölbasiZUçarOKelesTIncreased levels of high sensitive C-reactive protein in patients with chronic rheumatic valve disease: evidence of ongoing inflammationEur J Heart Fail20024559359512413502
- AlyanOMetinFKacmazFHigh levels of high sensitivity C-reactive protein predict progression of chronic rheumatic mitral stenosisJ Thromb Thrombolysis2009281636918622582
- DrakopoulouMToutouzasKStefanadiETsiamisETousoulisDStefanadisCAssociation of inflammatory markers with angiographic severity and extent of coronary artery diseaseAtherosclerosis200920633533919264307
- TanındıAŞahinarslanAElbegSCemriMRelationship between MMP-1, MMP-9, TIMP-1, IL-6 and risk factors, clinical presentation, extent and severity of atherosclerotic coronary artery diseaseOpen Cardivasc Med J20115110116
- RicevutiGMazzoneADe ServiSSpecchiaGFratinoPNew trends in coronary artery disease: the role of granulocyte activationAtherosclerosis1989782612652551307
- ÖztürkDErturkMCelıkOThe role of the neutrophil/lymphocyte ratio in patients with rheumatic mitral stenosis as an indicator of spontaneous echocardiographic contrastKardiol Pol2014721096997624846361
- BaysalECetinMYaylakBRoles of the red cell distribution width and neutrophil/lymphocyte ratio in predicting thrombolysis failure in patients with an ST-segment elevation myocardial infarctionBlood Coagul Fibrinolysis201526327427825396765
- HorneBDAndersonJLJohnJMWhich white blood cell subtypes predict increased cardiovascular risk?J Am Coll Cardiol20054510451638451643
- ChoKHJeongMHAhmedKValue of early risk stratification using hemoglobin levels and neutrophil-to-lymphocyte ratio in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary interventionAm J Cardiol201110784985621247535
- TurakOÖzcanFIşleyenAUsefulness of neutrophil-to- lymphocyte ratio to predict in-hospital outcomes in infective endocarditisCan J Cardiol201329121672167823916736
- AkboğaMKAkyelASahinarslanANeutrophil-to-lymphocyte ratio is increased in patients with rheumatic mitral valve stenosis?Anadolu Kardiyol Derg2014
- PolatNYildizAYukselMAssociation of neutrophil-lymphocyte ratio with the presence and severity of rheumatic mitral valve stenosisClin Appl Thromb Hemost201420879379824335245