Abstract
Systemic sclerosis (scleroderma) is a chronic, multisystem, fibrotic disease. Although the pathogenesis is not completely understood, early vascular damage leads to an inflammatory reaction and a severe fibrotic response. Therapy of systemic sclerosis is still not convincing and is mainly restricted to the management of organ complications. A wide choice of immunosuppressive and antifibrotic drugs has been used to try to modify the course of the disease, but significant breakthroughs are still lacking. Imatinib is a tyrosine kinase inhibitor known to regulate growth, proliferation, and differentiation as well as apoptosis of cells and is already widely used for several malignancies, eg, chronic myeloid leukemia and gastrointestinal stromal tumors. It has been used in preclinical as well as clinical studies to modulate the fibrotic process in patients with systemic sclerosis. This is based on its activity to interfere selectively with both the transforming growth factor-β and platelet-derived growth factor signaling pathway. Preclinical studies in mouse models of scleroderma showed significant anti-inflammatory and antifibrotic effects; however, several clinical, proof-of-concept trials have not yet confirmed these initially promising results.
Introduction to scleroderma
Scleroderma, or systemic sclerosis (SSc), is a multisystem disorder with a very heterogeneous course. It is characterized by the development of fibrosis of the skin and several internal organs. The pathogenesis of scleroderma is still not completely uncovered. It is based on vascular/endothelial cell injury, an altered immune response as well as an extensive fibrotic process, finally leading to induced production and deposition of collagen as well as other extracellular matrix proteins.Citation1
The accumulation of extracellular matrix proteins results in distinctive hardening of the skin and is responsible for the severe dysfunction/failure of affected organs (lung, heart, kidneys, gastrointestinal tract, and vascular system).Citation1
Due to the heterogeneous character of the disease and according to the different SSc subsets, the incidence, prevalence, mortality rates vary widely. Incidence rates vary from 0.1–4.3 patients per 100.000 inhabitants. This is also reflected in the prevalence rates, which vary between 1.5–34 patients per 100.000 inhabitants per year.Citation2–Citation11
The American College of Rheumatology published in 1980 preliminary classification criteria for patients suffering from SSc to simplify the classification of those patients with definite SSc disease.Citation12 LeRoy et al differentiated between limited versus diffuse cutaneous SSc based on a number of clinical characteristics, including extension of skin hardening, specific autoantibodies, and changes of capillaries localized within the nailfold.Citation13
Patients suffering from the limited form of SSc represent 43% (data from the German Network for SSc), the most common subgroup.Citation14–Citation16 These patients develop disease manifestations with skin hardening and/or internal organ involvement, usually with a delay of several years after the initial Raynaud’s phenomenon. The skin of these patients is mainly affected below the elbow and knee joints and often the face will also be involved. They also show an increased risk of developing gastrointestinal involvement as well as primary pulmonary arterial hypertension (PAH) in later stages of disease. Furthermore, patients with limited SSc more frequently show acral, facial, and/or intestinal telangiectasias. They are frequently characterized by anticentromere autoantibodies.Citation15,Citation16
Patients suffering from the diffuse form of SSc (32%) are characterized by an early onset of Raynaud’s phenomenon and the development of further non-Raynaud’s phenomenon symptoms within 1 year. The course of this disease variant is more progressive with more extensive skin involvement of the trunk, face, upper arms, and thighs shortly after Raynaud’s phenomenon onset. Patients with diffuse SSc are most frequently anti-Scl 70 (anti-topoisomerase-I) or anti-ribonucleic acid polymerase-III antibody positive, with a higher risk of developing interstitial lung disease, cardiac involvement, and scleroderma renal crisis during the course of disease.Citation15,Citation16
Patients with symptoms of SSc simultaneously with those of other connective tissue diseases such as myositis, Sjogren’s syndrome, or lupus erythematosus are classified as scleroderma overlap syndrome and are characterized by typical autoantibodies such as Pm-Scl, U1-RNP, and Jo-1.Citation15,Citation17,Citation18
Damage of the vascular system and endothelial cells is an early event in SSc. This leads to the release of cytokines/chemokines, causing tissue inflammation with the response of the immune system and resulting in the production of scleroderma-specific autoantibodies. Cytokines, chemokines, and growth factors play a key role in the transformation of fibroblasts to myofibroblasts and the overproduction of collagen and extracellular matrix proteins.Citation1
Fibrosis represents one of the main hallmark features in SSc based on the synthesis of increased quantities of fibronectin, fibrillins, proteoglycan core proteins, and particularly collagen types I and III. Profibrotic cytokines and chemokines, such as transforming growth factor-β (TGF-β), connective tissue growth factor (CCN2), platelet-derived growth factor (PDGF), endothelin-1, interleukins, and monocyte chemoattractant proteins (MCP-1 and MCP-3), participate as major proponents in the initiation of fibrosis.Citation19
TGF-β is one of the most potent profibrotic growth factors, stimulating fibroblasts to proliferate, migrate, and transdifferentiate into myofibroblasts. Enhanced levels of TGF-β have also been observed in serum/plasma, skin tissue, bronchoalveolar lavage, and blister fluid. It is overexpressed in the early fibrotic process, leading to the induction of signaling through both the Smad-dependent (Smad2/3) and Smad-independent pathway.Citation1,Citation20 TGF-β is also capable of inducing fibrosis independently of the Smad2/3 complex as well as PDGF receptor (PDGFR) signaling through the c-Abelson (c-Abl) kinase pathway.Citation21
PDGF is a dimeric peptide growth factor which can induce migration, differentiation, and transformation of different cells. These broad activities explain why PDGF also plays an important role in other disease processes, such as wound healing,Citation22 PAH,Citation23 and interstitial lung disease.Citation24 A recent preclinical study analyzed the impact of PDGFR and its signaling pathways in the pathogenetic process of pulmonary vascular remodeling, which showed that overexpression of PDGFRs and its ligands are increased compared to healthy subjects. In vitro and in vivo investigations have shown that the combination of PDGFR/c-Abl together with Src-inhibition reduced the response of pulmonary arterial smooth muscle cells to growth factor effects and improved vascular remodeling in experimental PAH.Citation25
Imatinib: mode of action, pharmacology, pharmacokinetics, and comparison with other therapy options
Imatinib (Glivec®; Novartis Pharma AG, Basel, Switzerland) is a small-molecule tyrosine kinase inhibitor that regulates many physiological cellular processes, including metabolism, growth/proliferation, differentiation, adhesion, and apoptosis.Citation26–Citation28
Imatinib has been approved for the treatment of several malignancies, ie, chronic myeloid leukemia (associated with the Philadelphia chromosome transformation; Bcr-Abl translocation),Citation29 myelodysplastic/myeloproliferative diseases associated with PDGFR gene rearrangements,Citation30 hypereosinophilic syndrome,Citation31 chronic eosinophilic leukaemia,Citation32 gastrointestinal stromal tumors,Citation33,Citation34 aggressive systemic mastocytosis (with D816V mutation),Citation35 and nonresectable dermatofibrosarcoma protuberans.Citation36
Imatinib is administered orally and absorbed with a mean time to maximum plasma concentration of 2–4 hours,Citation37,Citation38 without significant changes when taken in combination with food or under fasting conditions.Citation39 The standard dose in adults is 400–800 mg/day, whereas children are treated with a standard daily dosage of 340 mg/m2.Citation40 Plasma levels of imatinib usually remain stable after achieving the steady state.Citation37 The bioavailability of imatinib exceeds 90% from either tablets or capsules and its metabolism takes place predominantly in the liver, mediated by isoenzymes of the cytochrome P450 (CYP450) system, including CYP3A4/5 and, to a lesser extent, CYP1A2, CYP2D6, CYP2C9, and CYP2C19.Citation38 It is a substrate for the adenosine triphosphate-binding cassette (ABC) transporters ABCB1 and ABCG2 and is mainly bound to plasma proteins such as α-1 acid glycoprotein,Citation40 which influences its pharmacokinetics.Citation41 Imatinib and its main and also active metabolite, N-demethylated piperazine derivative, are eliminated through the bile and feces with just a small amount of the given dose of imatinib, secreted via the urine. This explains why a variation in bioavailability is mainly caused by changes in metabolism or distribution of imatinib.Citation42 Other drugs are known to induce CYP3A4/5 levels (eg, rifampicin, St John’s wort), leading to a reduction in imatinib plasma levels, while drugs which inhibit CYP3A4/5 can cause an increase in imatinib concentrations (eg, ketoconazole, itraconazole, clarithromycin, grapefruit juice). Conversely, imatinib may also act as an inhibitor of CYP3A4, CYP2C9, and CYP2D6 and may therefore alter the plasma levels of other drugs such as cyclosporin A, simvastatin, pimozide, warfarin, metoprolol, and paracetamol. The toxicities of imatinib are mainly dose-related.Citation38,Citation40
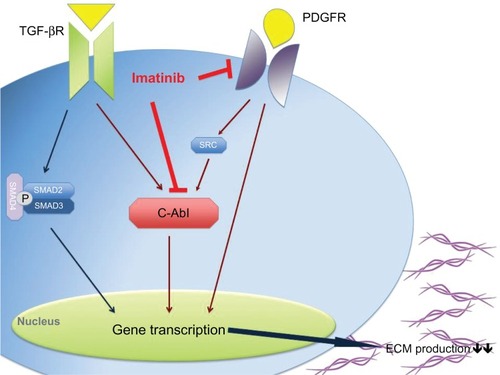
Imatinib is a 2-phenylaminopyrimidine derivative and works through inhibition of several tyrosine kinases. It binds to the adenosine triphosphate-binding site of the kinase, blocking the phosphorylation of its targets (protein tyrosine phosphorylation) and consequently inhibiting the induction of intracellular signal transduction pathways. It is known to interfere selectively with both TGF-β and PDGF signaling pathways by blocking c-Abl and PDGFR, respectively (). Apart from that, imatinib also works through Arg (Abl-related genes) kinases and c-Kit (stem cell factor receptor).Citation43–Citation46
Figure 1 Imatinib seems to work in systemic sclerosis patients through the inhibition of the TGF-β and PDGF signaling pathway via c-Abl and directly by blocking PDGFR, which results in a decrease of gene transcription and consequently in a decrease in collagen production.
Imatinib is thought to affect the main pathways in the fibrotic process instead of inhibiting the immune reaction and inflammation in SSc patients. It is hypothesized that imatinib might prevent the progression of skin hardening and organ fibrosis, whilst improving established fibrotic tissue alterations.Citation47
In previous clinical trials, for example in patients with chronic myeloid leukemia, imatinib has been well tolerated with the number of severe adverse side effects (eg, edema, rash, muscle cramps, diarrhea, bone marrow suppression) being less than 1% of subjects compared to SSc patients who developed overtly greater and more severe side effects in clinical studies.Citation48
In some patients, imatinib can cause congestive heart failure (toxic cardiomyopathy/cardiotoxicity) – with an incidence of 1.7% – and hepatotoxicity.Citation49,Citation50
Rationale for imatinib for the treatment of scleroderma
Scleroderma (SSc) is a heterogeneous, multisystem disease. Its pathogenesis has not been fully elucidated, explaining the lack of optimal treatment options. It is characterized by a severe fibrotic reaction in response to tissue damage caused by cytokines/growth factors such as PDGF and TGF-β, which have been identified as key mediators and result in the activation of fibroblasts in SSc. PDGF is also a major regulator of the vascular processes/angiogenesis and is known to be involved in SSc-associated PAH.Citation51
Imatinib can interact with both important profibrotic pathways contemporarily through PDGFR/c-Abl (important downstream signaling molecule of TGF-β and PDGF) and the Smad1/CCN2 pathway.Citation52,Citation53
Preclinical studies have shown that the inhibition of c-Abl leads to a decrease in type I collagen and fibronectin-1 synthesis by dermal fibroblasts and myofibroblasts.Citation54 They also showed a reduction in messenger ribonucleic acid synthesis of collagen and fibronectin in scleroderma and normal fibroblasts after imatinib treatment.Citation54
Hinchcliff et al demonstrated in their study that imatinib changed the gene signature of SSc dermal fibroblasts after treatment compared to healthy subjects.Citation55
Soria et al showed that imatinib was able to block the proliferation of normal and scleroderma fibroblasts by inhibiting the phosphorylation of PDGFRs.Citation56 In addition, Furspan et al demonstrated a positive correlation of the degree of vasoconstriction of isolated arterioles of SSc patients and healthy controls with the degree of tyrosine phosphorylation in vascular smooth muscle cells. Additionally, imatinib improved and reduced vasoconstriction after cold exposure.Citation57
Mice that developed lung fibrosis after bleomycin-exposure were treated with imatinib at doses of 50 mg/kg/day and 150 mg/kg/day, with a clear beneficial antifibrotic effect with minimal toxic side effects.Citation21
Another study using animal models demonstrated that imatinib could prevent bleomycin-induced fibrosis, but failed to improve bleomycin-induced preexisting dermal fibrosis.Citation54 These findings indicate that imatinib is more effective in blocking early ongoing fibrotic processes than dissolving already established, burned-out fibrotic tissue. Imatinib was also effective in preventing bleomycin or radiation-induced interstitial lung disease in mouse models.Citation21,Citation58–Citation60
A positive effect of imatinib has also been reported in other sclerotic diseases such as graft-versus-host disease,Citation61–Citation63 localized scleroderma (morphea),Citation64 and nephrogenic systemic fibrosis.Citation65,Citation66
Efficacy, safety, and tolerability studies and patient-focused perspectives: quality of life, satisfaction and acceptability, adherence, and uptake
On the basis of all preclinical studies, several case reports have suggested a clinical benefit within 3–6 months of treatment with imatinib in patients with SSc. All reported a reduction in skin fibrosis detected by modified Rodnan skin score (MRSS) and an increase in lung function.Citation47,Citation67,Citation68 A recent case series of six scleroderma patients reported a clear reduction in skin hardening as well as a stabilization in lung function after treatment with a dosage of 200 mg/day for a median period of 23 months.Citation69
To confirm these findings, several clinical trials were initiated with controversial results.
Pope et al performed a 6-month, randomized, double-blind, placebo-controlled, proof-of-concept pilot study that included patients with active diffuse SSc. Ten diffuse SSc patients were randomized, and four completed the study with a dosage of 400 mg/day. After randomizing, further enrollment was stopped due to a poor overall tolerance (fatigue, weakness, tiredness, fluid retention, nausea, constipation, diarrhea, and anemia) and two serious adverse events. Side effects occurred in both patients at very early stages during treatment, with relapses of side effects also after readministration of reduced dosages. No significant effect was detectable.Citation70
Tamaki et al showed in their pilot study that a dose of 100 mg/day improved symptoms in five patients with PAH, including three SSc patients, over a period of 6 months. No significant effects were detectable on hemodynamics or exercise capacity, but two SSc patients showed a reduction in vascular pulmonary resistance as well as an improvement in the predicted diffusion lung capacity for carbon monoxide. All three patients showed an improvement in skin thickening and mobility. Nailfold capillary changes, especially hemorrhages, disappeared after 6 months of treatment. Interestingly, none of the three patients developed side effects; only one patient suffered from transient renal dysfunction.Citation71 These data indicate that imatinib has more beneficial effects on skin manifestation than on pulmonary involvement. This could be in agreement with the four-fold increase in the α-1 acid glycoprotein level in bronchoalveolar lavage fluids compared to serum levels of SSc patients and healthy controls, which is known to block the inhibitory effects of imatinib.Citation71–Citation73
Hatano et al showed that patients with PAH have increased PDGF-BB serum levels, which declined after the treatment with imatinib. Interestingly, patients with increased PDGF-BB levels within the early stage of disease showed an improvement (>15% decrease in pulmonary vascular resistance) following imatinib treatment.Citation74
Khanna et al conducted a 1-year, Phase I/IIa, open-label pilot study that treated 20 SSc patients with SSc-associated interstitial lung disease with oral imatinib (up to 600 mg/day). Five patients developed adverse events, including generalized edema, shortness of breath, diastolic dysfunction, generalized rash, diarrhea, hepatotoxicity, elevated creatine kinase levels, and anemia. Three of these five patients suffered from marked anemia, fatigue, and muscle weakness combined with gastric antral vascular ectasia. Dyspnea and generalized edema was observed in the other two patients. There was a significant improvement in MRSS (3.9 units; P < 0.001) as well as a trend towards improvement in parameters in lung function tests (1.74% increase in forced vital capacity, 4.17% increase in total lung capacity, and a 1.46% increase in the diffusing capacity of the lung for carbon monoxide).Citation75
Spiera et al administered imatinib in their 1-year, Phase IIa, single-arm, open-label study in a daily dosage of 400 mg for 12 months in 30 patients with early diffuse SSc. Of these, 24 patients completed the 12-month treatment period. There were 171 adverse events that appeared to be related to the drug intake. Serious adverse events were detectable in 24 patients; however, they were not all related to the study medication. An improvement in skin thickening was detectable in early and late stage patients (decline in MRSS by 6.6 points or 22.4%; P < 0.001), as well as a significant improvement in forced vital capacity (improvement by 6.4%; P < 0.008), while the diffusion capacity just stabilized and skin morphology (collagen deposition) changed. Health-related quality of life assessment improved or remained stable during the study.Citation76
A multicenter, open-label, proof-of-concept, Phase IIa study enrolled 27 patients who were started on 200 mg/day imatinib, which was then titrated up to 600 mg/day. Sixteen of the 27 patients completed 24 weeks of treatment, but unfortunately no significant changes in skin score and/or lung function was observable.Citation77
Chung et al investigated whether treatment with imatinib would have an impact on gene expression signature in skin biopsies. They included seven patients with diffuse SSc and two patients with limited SSc and administered dosages between 100–400 mg/day for 24 weeks. Improvement in skin thickening (32% improvement in MRSS; P = 0.05) was detectable in seven patients who completed 24 weeks of treatment with a mean dose of 300 mg/day. Changes of gene expression pre- and posttreatment with imatinib were investigated and a change in gene signature of skin biopsies in three patients who responded to the treatment (upregulation of genes involved in collagen metabolism and downregulation of genes involved in mitosis and cell cycle) was detected.Citation77,Citation78
Sabnani et al showed, that a combination therapy of imatinib (200 mg/day) together with cyclophosphamide (500 mg every 3 weeks) was well-tolerated in five patients with scleroderma-associated interstitial lung disease.Citation79
An improvement in PAH and right ventricular function in a patient with SSc-associated cardiac involvement after imatinib treatment (200–400 mg/day) was reported by ten Freyhaus et al, who suggested that the benefit was induced by an antiproliferative rather than by a vasodilatative effect.Citation23
Prey et al recently reported their data of a Phase II, multicenter, randomized, double-blinded, controlled study on patients with morphea (n = 3) and SSc (n = 25). Each patient received after randomization either 400 mg/day imatinib or placebo for 6 months, with a follow-up after discontinuation of a further 6 months. The primary outcome was the efficacy based on the change in MRSS; unfortunately no changes in MRSS were observable. Adverse events were more frequent in the group treated with imatinib.Citation80
Conclusion and place in therapy
SSc and its treatment is still a major burden for the affected patient and a challenge for clinicians. To date, SSc is not curable; however, immunosuppressive drugs are frequently used as modifying treatments. Basic research, the search for new therapeutic targets, and new controlled clinical studies/trials are urgently required to improve the course of disease, mortality, and prognosis as well as the quality of life of SSc patients.
On the basis of the data available, it is still very difficult to reach a final conclusion on whether imatinib or its related variants are effective drugs for SSc. This is due to (1) the heterogeneity of this disease, which exacerbates the grading of improvement of symptoms; (2) the severity of organ involvements and progression of disease, with an increased risk of developing side effects such as edema, cardiotoxicity, and alveolitis; and (3) the self-limitation of skin-hardening, usually after a period of 3–4 years.
Interestingly, in some reports not only fibrosis improved under treatment, but also vascular alterations. This could be explained by the finding that target molecules of imatinib are also expressed in vascular structures.Citation81
Studies using imatinib in the treatment of chronic myeloid leukemia always reported low frequencies of drug-induced adverse events. Much higher doses (up to 800 mg/day) have been used compared to initial studies involving scleroderma patients, which more frequently showed dose-dependent adverse events. This has been the reason for some study interruption and loss to follow-up of patients. SSc patients treated with lower doses of imatinib (200 mg/day) showed a better tolerability.Citation69,Citation71 One might hypothesize that this could be explained by the fact that SSc patients suffer from a multisystem disease, including impairment of renal function and/or cardiopulmonary function. Ohnishi et al reported that imatinib-induced interstitial lung disease, occurred more frequently in patients with preexisting lung impairment, which was reversible after stopping treatment.Citation82
Due to the variation of efficacy in all mentioned case reports and studies, it would be important to identify patients who would benefit the most. This could be achieved by the development of biomarkers to identify patients, which are associated with a progressive versus mild course of disease, which are associated with rather fibrotic or vascular features and which correlate with the response to therapies.
Tamaki et al suggested that plasma levels of PDGF-BB could serve as a marker for responsiveness to imatinib due to the finding that PDGF plays a major role in skin and vascular involvement in SSc patients and that it decreased after the administration of imatinib.Citation71
To date, placebo-controlled studies are still lacking and the published observational studies show conflicting results, balanced with negative and positive effects/findings. Therefore, it is impossible to distinguish between the definite effects of the drug and the normal course of disease. Also, the fact that patients have been treated with other immunosuppressive drugs falsifies the findings and should be considered in future well-designed, placebo-controlled trials.
There are still many open questions about the efficacy and tolerability of imatinib as an antifibrotic drug in SSc patients. Until now, all studies had limitations, which makes any judgment about positive and negative results very difficult. Further studies should also focus much more on the molecular effects of these antifibrotic drugs. Beyer et al nicely explained in their paper that patients with fibrotic diseases and especially with SSc would need a detailed molecular characterization with the focus on biomarkers which indicate specific profibrotic signaling pathways.Citation83
In vitro studies don’t completely reflect real life, especially the interplay between different cells and the impact of these cells among one another and under different conditions. Therefore, it would be important to uncover in vivo whether imatinib directly affects human fibroblasts through inhibition within the TGF-β and PDGF signaling pathway or whether it also acts indirectly through alteration of other cell types. Furthermore, it should be investigated whether the combination of different tyrosine kinase inhibitors with their corresponding targeted tyrosine kinases would amplify the therapeutic effect. Further studies should also address whether combination with immunosuppressive drugs or other antifibrotic drugs would improve the effect of imatinib.
Disclosure
The authors report no conflicts of interest in this work.
References
- GabrielliAAvvedimentoEVKriegTSclerodermaN Engl J Med2009360191989200319420368
- AlamanosYTsifetakiNVoulgariPVEpidemiology of systemic sclerosis in northwest Greece 1981 to 2002Semin Arthritis Rheum200534571472015846586
- AllcockRJForrestICorrisPACrookPRGriffithsIDA study of the prevalence of systemic sclerosis in northeast EnglandRheumatology (Oxford)200443559660214872101
- Arias-NunezMCLlorcaJVazquez-RodriguezTRSystemic sclerosis in northwestern Spain: a 19-year epidemiologic studyMedicine (Baltimore)200887527228018794710
- Lo MonacoABruschiMLa CorteRVolpinariSTrottaFEpidemiology of systemic sclerosis in a district of northern ItalyClin Exp Rheumatol2011292 Suppl 65S10S1421586212
- MayesMDScleroderma epidemiologyRheum Dis Clin North Am200329223925412841293
- MedsgerTAJrEpidemiology of systemic sclerosisClin Dermatol19941222072168076257
- SilmanAJanniniSSymmonsDBaconPAn epidemiological study of scleroderma in the West MidlandsBr J Rheumatol19882742862903261609
- SilmanAJEpidemiology of sclerodermaAnn Rheum Dis199150Suppl 48468531750796
- SteenVDMedsgerTAJrEpidemiology and natural history of systemic sclerosisRheum Dis Clin North Am19901611102406801
- TamakiTMoriSTakeharaKEpidemiological study of patients with systemic sclerosis in TokyoArch Dermatol Res199128363663711796818
- Subcommittee for scleroderma criteria of the American Rheumatism Association Diagnostic and Therapeutic Criteria CommitteePreliminary criteria for the classification of systemic sclerosis (scleroderma)Arthritis Rheum19802355815907378088
- LeRoyECBlackCFleischmajerRScleroderma (systemic sclerosis): classification, subsets and pathogenesisJ Rheumatol19881522022053361530
- HunzelmannNKriegTThe German Network for Systemic Sclerosis (DNSS): current data on diagnostics and therapyHautarzt201263Suppl 17175 German22543950
- HunzelmannNGenthEKriegTThe registry of the German Network for Systemic Scleroderma: frequency of disease subsets and patterns of organ involvementRheumatology (Oxford)20084781185119218515867
- MoinzadehPFehrADammBKriegTHunzelmannNThe German Network for Systemic SclerodermaHautarzt20075810858863 German17846731
- BennettRMScleroderma overlap syndromesRheum Dis Clin North Am19901611851982406807
- PakozdiANihtyanovaSMoinzadehPOngVHBlackCMDentonCPClinical and serological hallmarks of systemic sclerosis overlap syndromesJ Rheumatol201138112406240921844148
- MoinzadehPDentonCPAbrahamDBiomarkers for skin involvement and fibrotic activity in sclerodermaJ Eur Acad Dermatol Venereol201226326727621819452
- ReinerJEDattaPKTGF-beta-dependent and -independent roles of STRAP in cancerFront Biosci201116105115
- DanielsCEWilkesMCEdensMImatinib mesylate inhibits the profibrogenic activity of TGF-beta and prevents bleomycin-mediated lung fibrosisJ Clin Invest200411491308131615520863
- CromackDTPierceGFMustoeTATGF-beta and PDGF mediated tissue repair: identifying mechanisms of action using impaired and normal models of wound healingProg Clin Biol Res19913653593731862144
- ten FreyhausHDumitrescuDBovenschulteHErdmannERosenkranzSSignificant improvement of right ventricular function by imatinib mesylate in scleroderma-associated pulmonary arterial hypertensionClin Res Cardiol200998426526719219392
- SaggarRLynchJPBelperioJAPulmonary arterial hypertension and lung transplantationSemin Respir Crit Care Med201031214716020354928
- PullamsettiSSBerghausenEMDabralSRole of Src tyrosine kinases in experimental pulmonary hypertensionArterioscler Thromb Vasc Biol20123261354136522516066
- BuchdungerEZimmermannJMettHInhibition of the Abl protein-tyrosine kinase in vitro and in vivo by a 2-phenylaminopyrimidine derivativeCancer Res19965611001048548747
- DrukerBJTamuraSBuchdungerEEffects of a selective inhibitor of the Abl tyrosine kinase on the growth of Bcr-Abl positive cellsNat Med1996255615668616716
- RobinsonDRWuYMLinSFThe protein tyrosine kinase family of the human genomeOncogene200019495548555711114734
- DrukerBJTalpazMRestaDJEfficacy and safety of a specific inhibitor of the BCR-ABL tyrosine kinase in chronic myeloid leukemiaN Engl J Med2001344141031103711287972
- MesaRASteensmaDPHoyerJKetterlingRPConcomitant myelodysplastic syndrome and chronic myeloid leukaemia: treatment outcomes with imatinib mesylateBr J Haematol2003123236636714531922
- AntoniuSAImatinib mesylate for the treatment of hypereosinophilic syndromesCurr Opin Investig Drugs2006711980984
- CoutreSGotlibJTargeted treatment of hypereosinophilic syndromes and chronic eosinophilic leukemias with imatinib mesylateSemin Cancer Biol200414430731515305431
- BlankeCDEisenbergBLHeinrichMCGastrointestinal stromal tumorsCurr Treat Options Oncol20012648549112057094
- van OosteromATJudsonIVerweijJSafety and efficacy of imatinib (STI571) in metastatic gastrointestinal stromal tumours: a phase I studyLancet200135892911421142311705489
- DalalBIHorsmanDEBruyereHForrestDLImatinib mesylate responsiveness in aggressive systemic mastocytosis: novel association with a platelet derived growth factor receptor beta mutationAm J Hematol2007821777917133421
- Johnson-JahangirHShermanWRatnerDUsing imatinib as neoadjuvant therapy in dermatofibrosarcoma protuberans: potential pluses and minusesJ Natl Compr Canc Netw20108888188520870634
- DrukerBJImatinib mesylate in the treatment of chronic myeloid leukaemiaExpert Opin Pharmacother20034696397112783592
- van ErpNPGelderblomHGuchelaarHJClinical pharmacokinetics of tyrosine kinase inhibitorsCancer Treat Rev200935869270619733976
- SparanoBAEgorinMJPariseRAEffect of antacid on imatinib absorptionCancer Chemother Pharmacol200963352552818500518
- PetainAKattygnarathDAzardJPopulation pharmacokinetics and pharmacogenetics of imatinib in children and adultsClin Cancer Res200814217102710918981009
- DelbaldoCChatelutEReMPharmacokinetic-pharmacodynamic relationships of imatinib and its main metabolite in patients with advanced gastrointestinal stromal tumorsClin Cancer Res20061220 Pt 16073607817062683
- BoddyAVSluddenJGriffinMJPharmacokinetic investigation of imatinib using accelerator mass spectrometry in patients with chronic myeloid leukemiaClin Cancer Res200713144164416917634544
- OkudaKWeisbergEGillilandDGGriffinJDARG tyrosine kinase activity is inhibited by STI571Blood20019782440244811290609
- BuchdungerECioffiCLLawNAbl protein-tyrosine kinase inhibitor STI571 inhibits in vitro signal transduction mediated by c-kit and platelet-derived growth factor receptorsJ Pharmacol Exp Ther2000295113914510991971
- HeinrichMCGriffithDJDrukerBJWaitCLOttKAZiglerAJInhibition of c-kit receptor tyrosine kinase activity by STI571, a selective tyrosine kinase inhibitorBlood200096392593210910906
- AnXTiwariAKSunYDingPRAshbyCRJrChenZSBCR-ABL tyrosine kinase inhibitors in the treatment of Philadelphia chromosome positive chronic myeloid leukemia: a reviewLeuk Res201034101255126820537386
- DistlerJHDistlerOIntracellular tyrosine kinases as novel targets for anti-fibrotic therapy in systemic sclerosisRheumatology (Oxford)200847Suppl 5v10v1118784126
- DrukerBJGuilhotFO’BrienSGFive-year follow-up of patients receiving imatinib for chronic myeloid leukemiaN Engl J Med2006355232408241717151364
- KerkelaRGrazetteLYacobiRCardiotoxicity of the cancer therapeutic agent imatinib mesylateNat Med200612890891616862153
- AtallahEDurandJBKantarjianHCortesJCongestive heart failure is a rare event in patients receiving imatinib therapyBlood200711041233123717449798
- BarstRJPDGF signaling in pulmonary arterial hypertensionJ Clin Invest2005115102691269416200204
- BhattacharyyaSIshidaWWuMA non-Smad mechanism of fibroblast activation by transforming growth factor-beta via c-Abl and Egr-1: selective modulation by imatinib mesylateOncogene200928101285129719151753
- PannuJAsanoYNakerakantiSSmad1 pathway is activated in systemic sclerosis fibroblasts and is targeted by imatinib mesylateArthritis Rheum20085882528253718668566
- DistlerJHJungelAHuberLCImatinib mesylate reduces production of extracellular matrix and prevents development of experimental dermal fibrosisArthritis Rheum200756131132217195235
- HinchcliffMHuangCCIshidaWImatinib mesylate causes genome-wide transcriptional changes in systemic sclerosis fibroblasts in vitroClin Exp Rheumatol2012302 Suppl 71S86S9622691216
- SoriaACario-AndreMLepreuxSThe effect of imatinib (Glivec) on scleroderma and normal dermal fibroblasts: a preclinical studyDermatology2008216210911718216472
- FurspanPBChatterjeeSFreedmanRRIncreased tyrosine phosphorylation mediates the cooling-induced contraction and increased vascular reactivity of Raynaud’s diseaseArthritis Rheum20045051578158515146428
- AkhmetshinaAVenalisPDeesCTreatment with imatinib prevents fibrosis in different preclinical models of systemic sclerosis and induces regression of established fibrosisArthritis Rheum200960121922419116940
- AonoYNishiokaYInayamaMImatinib as a novel antifibrotic agent in bleomycin-induced pulmonary fibrosis in miceAm J Respir Crit Care Med2005171111279128515735062
- LiMAbdollahiAGroneHJLipsonKEBelkaCHuberPELate treatment with imatinib mesylate ameliorates radiation-induced lung fibrosis in a mouse modelRadiat Oncol200946620025728
- PapadakisVKarakasisDSfikakisPPIs imatinib mesylate a promising drug in scleroderma due to extensive chronic graft-versus-host disease?Leuk Lymphoma200950347147419253137
- MagroLCatteauBCoiteuxVBrunoBJouetJPYakoub-AghaIEfficacy of imatinib mesylate in the treatment of refractory sclerodermatous chronic GVHDBone Marrow Transplant2008421175776018762765
- OlivieriJColuzziSAttolicoIOlivieriATirosin kinase inhibitors in chronic graft versus host disease: from bench to bedsideScientific World Journal2011111908193122125447
- BibiYGottliebABA potential role for imatinib and other small molecule tyrosine kinase inhibitors in the treatment of systemic and localized sclerosisJ Am Acad Dermatol200859465465818571768
- ElmholdtTRBuusNHRamsingMOlesenABAntifibrotic effect after low-dose imatinib mesylate treatment in patients with nephrogenic systemic fibrosis: an open-label non-randomized, uncontrolled clinical trialJ Eur Acad Dermatol Venereol12202011 Epub ahead of print
- KayJHighWAImatinib mesylate treatment of nephrogenic systemic fibrosisArthritis Rheum20085882543254818668587
- SfikakisPPGorgoulisVGKatsiariCGEvangelouKKostopoulosCBlackCMImatinib for the treatment of refractory, diffuse systemic sclerosisRheumatology (Oxford)200847573573718326532
- van DaelePLDikWAThioHBIs imatinib mesylate a promising drug in systemic sclerosis?Arthritis Rheum20085882549255218668570
- GuoLChenXXGuYYZouHJYeSLow-dose imatinib in the treatment of severe systemic sclerosis: a case series of six Chinese patients and literature reviewClin Rheumatol20123191395140022875698
- PopeJMcBainDPetrlichLImatinib in active diffuse cutaneous systemic sclerosis: results of a six-month, randomized, double-blind, placebo-controlled, proof-of-concept pilot study at a single centerArthritis Rheum201163113547355121769850
- TamakiZAsanoYHatanoMEfficacy of low-dose imatinib mesylate for cutaneous involvement in systemic sclerosis: a preliminary report of three casesMod Rheumatol2012221949921633912
- FiettaABardoniASalviniRAnalysis of bronchoalveolar lavage fluid proteome from systemic sclerosis patients with or without functional, clinical and radiological signs of lung fibrosisArthritis Res Ther200686R16017044913
- AzumaMNishiokaYAonoYRole of alpha1-acid glycoprotein in therapeutic antifibrotic effects of imatinib with macrolides in miceAm J Respir Crit Care Med2007176121243125017717205
- HatanoMYaoAShigaTKinugawaKHirataYNagaiRImatinib mesylate has the potential to exert its efficacy by down-regulating the plasma concentration of platelet-derived growth factor in patients with pulmonary arterial hypertensionInt Heart J201051427227620716845
- KhannaDSaggarRMayesMDA one-year, phase I/IIa, open-label pilot trial of imatinib mesylate in the treatment of systemic sclerosis-associated active interstitial lung diseaseArthritis Rheum201163113540354621769849
- SpieraRFGordonJKMerstenJNImatinib mesylate (Gleevec) in the treatment of diffuse cutaneous systemic sclerosis: results of a 1-year, phase IIa, single-arm, open-label clinical trialAnn Rheum Dis20117061003100921398330
- BourniaVKEvangelouKSfikakisPPTherapeutic inhibition of tyrosine kinases in systemic sclerosis: a review of published experience on the first 108 patients treated with imatinibSemin Arthritis Rheum7102012 Epub ahead of print
- ChungLRuizPWoodTEvaluation of an imatinib response gene signature in patients with systemic sclerosisArthritis Rheum201062S239
- SabnaniIZuckerMJRosensteinEDA novel therapeutic approach to the treatment of scleroderma-associated pulmonary complications: safety and efficacy of combination therapy with imatinib and cyclophosphamideRheumatology (Oxford)2009481495218815156
- PreySEzzedineKDoussauAImatinib mesylate in scleroderma-associated diffuse skin fibrosis: a phase II multicentre randomized double-blinded controlled trialBr J Dermatol201216751138114423039171
- BeyerCDistlerJHDistlerOAre tyrosine kinase inhibitors promising for the treatment of systemic sclerosis and other fibrotic diseases?Swiss Med Wkly2010140w1305020419513
- OhnishiKSakaiFKudohSOhnoRTwenty-seven cases of drug-induced interstitial lung disease associated with imatinib mesylateLeukemia20062061162116416598305
- BeyerCDistlerJHTyrosine kinase signaling in fibrotic disorders: translation of basic research to human diseaseBiochim Biophys Acta6192012 Epub ahead of print