
Abstract
Background
Advanced-stage hepatocellular carcinoma (HCC), especially huge HCC or portal vein tumour thrombus (PVTT), is difficult to treat, and the prognosis is poor. The advantages of hepatic artery infusion chemotherapy (HAIC) combined with targeted therapy and immunotherapy for this complex disease are gradually becoming apparent. However, HAIC still has some inevitable disadvantages, such as arterial perfusion therapy requiring a long time, which results in many patients having difficulty completing the procedure. Modified HAIC (mHAIC)-based oxaliplatin and S-1 is a new treatment option for huge HCC or PVTT that can reduce complications and improve patient compliance. We report two cases of huge HCC or PVTT that were successfully treated with mHAIC combined with lenvatinib and camrelizumab. The clinical presentations, treatment strategies, and outcomes of these cases are presented.
Case Presentation
Case 1: A 52-year-old female was found to have a huge HCC with a size of 14×11 cm. She was treated with one cycle of mHAIC combined with transcatheter arterial chemoembolization (TACE), lenvatinib and camrelizumab and 3 cycles of mHAIC in combination with lenvatinib and camrelizumab. The patient’s follow-up maintenance therapy with lenvatinib and camrelizumab has been evaluated for efficacy in achieving complete response (CR). Case 2: A 57-year-old man was diagnosed with advanced HCC in combination with PVTT. He achieved partial remission (PR) after four cycles of mHAIC combined with lenvatinib and camrelizumab. This was followed by treatment with lenvatinib and camrelizumab with an efficacy assessment for CR, and progression-free survival (PFS) was 7 months.
Conclusion
For advanced HCC with a large mass or PVTT, mHAIC combined with lenvatinib and camrelizumab is a safe and effective treatment with good patient compliance.
Keywords:
Introduction
Huge (>10 cm in diameter) hepatocellular carcinomas (HCCs) are usually unresectable due to insufficient surgical margins, a residual liver volume estimated to be less than 30% after resection, or macrovascular invasion and are an independent risk factor due to a high risk for initial extrahepatic recurrence.Citation1 Compared to HCC without PVTT, HCC with PVTT is characterized by an aggressive disease course, worse hepatic function, a higher chance of complications related to portal hypertension, and poorer tolerance to treatment. It occurs in 30–62% of patients with HCC and has a direct impact on patient prognosis.Citation2 Previous studies found that transcatheter arterial chemoembolization (TACE) in huge HCC had a poor effect, and TACE-related mortality rates of 6.5–20% were reported.Citation3 Similarly, the efficacy of TACE is limited for HCC combined with PVTT.
Hepatic artery infusion chemotherapy (HAIC) has been shown to be an effective treatment for advanced HCC in Asian countries, especially in Japan.Citation4 The clinical response of HAIC was significant, and responders had the best survival rates from 7 to 81%, with a median survival time (MST) of approximately 6–15.9 months.Citation5 Long et al reported that sorafenib plus HAIC was associated with significantly better OS, PFS, and ORR than sorafenib alone in advanced HCC.Citation6 Mei et al reported that for patients treated with HAIC combined with PD-1 inhibitors and lenvatinib, the overall response rate was 40.0%, the disease control rate was 77.6%, and the median overall survival was 15.9 months.Citation7
S-1 (ie, tegafur/gimeracil/oteracil potassium, known as Tijiao capsule in China) is a novel oral 5-fluoro-2,4(1H, 3H)-pyrimidinedione (5-FU) analogue that contains tegafur and two biochemical modulators for 5-FU. S-1 is mainly distributed in the liver and has a selective antagonistic effect on the 5-FU catabolic enzyme dihydropyrimidine dehydrogenase (DPD), which leads to an increase in the concentration of 5-FU converted from S-1 and the persistence of the phosphorylated metabolite of 5-FU, 5-FUMP, in high concentrations in the tumour, and S-1 can enhance the antitumour effect.Citation8
Here, we report two cases: the first is a huge HCC, while the second is an HCC combined with PVTT. Using a modified HAIC (mHAIC) method, S-1 was used in place of standard 5-FU and oxaliplatin injection into the hepatic artery. Both cases also received lenvatinib and camrelizumab.
Case Presentation
Case 1
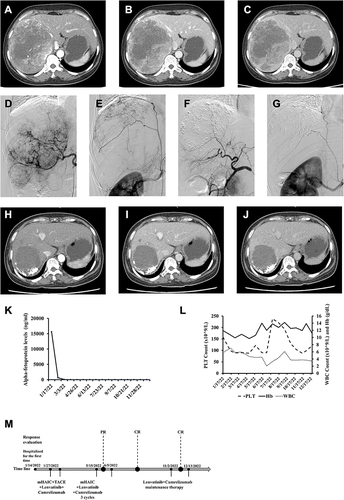
On January 14, 2022, a 52-year-old female was referred to our hospital when a large tumour mass on the liver was found on abdominal ultrasound sonography. The patient had a 14-year history of hepatitis B infection, and has not undergone any prior anti-tumor therapies or antiviral therapy. After admission, abdominal enhanced computed tomography (CT) showed a 14×11 cm liver tumour (). The right branch of the portal vein was compressed, and there were many hypointense shadows smaller than 0.7–3.0 cm in diameter across the rest of the liver. The alpha-fetoprotein (AFP) level was 15,598 ng/mL (normal range: 0–5 ng/mL), and the liver function Child‒Pugh classification was grade A. There was no evidence of extrahepatic metastases on CT scan. The Barcelona Clinic Liver Cancer (BCLC) stage was B. On January 27, 2022, she received a single treatment with TACE, mHAIC (oxaliplatin and S-1), lenvatinib and camrelizumab. Digital subtraction angiography (DSA) via an implantable port-catheter system before mHAIC demonstrated multiple tumour stains of HCC (). The subphrenic artery from the renal artery supplied some of the blood to the tumour, as seen on DSA (). The TACE procedure consisted of subphrenic artery injection of a mixture of lipiodol and epirubicin 50 mg. mHAIC with oxaliplatin (85 mg/m2) was administered continuously for 2 h via an implanted catheter system. Beginning on the second day, the patient received S-1 (80 mg/m2/day on Days 1–14) with camrelizumab (200 mg, once every 3 weeks) and lenvatinib (8 mg, qd). After 4 cycles of mHAIC, DSA clipping of the hepatic and subphrenic arteries showed no tumour staining ( and ). On May 15, 2022, the entire abdomen was inspected again with an enhanced CT scan after 4 cycles of mHAIC. The liver volume had grown, the shadow of the large mass in the right lobe of the liver had decreased, and the mass itself was mainly necrotic with no appreciable enhancement (). The AFP level decreased to 15.8 ng/mL () during the treatment period, and laboratory tests revealed haemoglobin (HGB), white blood cell (WBC), and platelet (PLT) changes with only grade 1 bone marrow suppression (). According to RECIST 1.1, the target lesion response was classified as a partial response (PR), whereas according to mRECIST, it was a complete response (CR). Since then, the patient has been receiving maintenance therapy with lenvatinib and camrelizumab, and while she is currently in a stable condition, the patient regrettably declined to undergo surgery.
Figure 1 Changes in case 1 in imaging and laboratory tests during clinical treatment. Enhanced CT images before introducing mHAIC. A 14×11 cm mass is shown in the right liver in the arterial phase (A), portal phase (B) and delayed phase (C). Enhanced CT images after introducing mHAIC. (D) DSA via an implantable port-catheter system, before mHAIC, demonstrated large tumour stains of HCC. (E) The subphrenic artery develops from the beginning of the renal artery and supplies blood to the tumour area. (F and G) After 4 cycles of mHAIC, DSA clipping of the hepatic and subphrenic arteries showed no tumour staining. A 7×6 cm mass is shown in the right liver in the arterial phase (H), portal phase (I) and delayed phase (J). (K) AFP level changes during postoperative mHAIC. (L) Changes in WBC, PLT, and HGB of patients during treatment. (M) Timeline of the treatment process.
Case 2
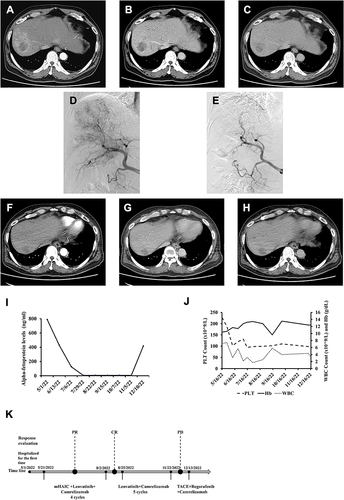
A 57-year-old Chinese male patient was admitted to our hospital in April 2022 due to right hepatic occupying lesions for one week. He had a history of chronic viral hepatitis B for more than 20 years with no previous antiviral therapy to control it and nor any treatment. Laboratory examinations of the patient before therapy revealed that the AFP level was 789 ng/mL. The examination results suggested that the patient’s the BCLC stage was stage C. The patient’s liver function Child‒Pugh classification was grade B. The patient was diagnosed with HCC with PVTT, cirrhosis, and chronic viral hepatitis after an enhanced CT scan revealed a tumour measuring 8.9×7.8 cm (). On May 16, 2022, a diagnostic examination of the liver mass was conducted. The patient underwent a needle biopsy prior to mHAIC and a HCC was identified. Beginning on May 21, 2022, two cycles of mHAIC (oxaliplatin and S-1), S-1 (60 mg bid; d1-d14, q3w), camrelizumab (200 mg once every 3 weeks) and lenvatinib (12 mg, qd) were administered. A therapy cycle lasted for three weeks. Every cycle, liver, coagulation, blood, and renal functions were assessed, and CT was performed every six weeks. The DSA right hepatic arteriogram showed an obscure staining of the right lobe of the liver, a triangular staining of the left lobe of the liver in the arterial phase, and a double track sign of the right hepatic artery and the main trunk of the left branch of the accompanying portal vein (). After 4 cycles of mHAIC, DSA clipping of the hepatic arteries showed no tumour staining (). On July 7, 2022, the patient returned to the hospital for a follow-up exam. An enhanced CT scan of the entire abdomen revealed that the abnormal improvement lesion in the lamellar blood vessel stage of the right lobe of the liver had shrunk significantly from its previous size, measuring approximately 2.0×1.5 cm with a blurred border (). During the treatment period, the AFP level decreased to 5.8 ng/mL (), and there were also changes in laboratory test results for HGB, WBC, and PLT, with a particularly marked decrease in platelets, but only grade 1 myelosuppression (). According to RECIST 1.1, the target lesion response was classified as PR, whereas according to mRECIST, it was classified as CR. Similarly, the patient was advised to undergo surgery, which he declined. When he was examined again in December 2022, an enhanced CT of his abdomen revealed that the tumour was still growing and progressing.
Figure 2 Changes in case 2 in imaging and laboratory tests during clinical treatment. Enhanced CT images before introducing mHAIC. A 6×5 cm mass is shown in the right liver in the arterial phase (A), portal phase (B) and delayed phase (C). (D) Hepatic angiography showing the thread and streaks sign, which implies a vascularized tumour thrombus. (E) After 4 cycles of mHAIC, DSA clipping of the hepatic arteries showed no tumour staining. Enhanced CT images after introducing mHAIC. A 2.0×1.5 cm mass is shown in the right liver in the arterial phase (F), portal phase (G) and delayed phase (H). (I) AFP level changes during postoperative mHAIC. (J) Changes in WBC, PLT and HGB of patients during treatment. (K) Timeline of the treatment process.
Discussion
We report two cases characterized by rarely reported treatment with mHAIC (oxaliplatin and S-1) combined with lenvatinib and camrelizumab for advanced HCC. Regarding the response rate according to mRECIST criteria, two patients achieved CR ( and ; and ). HAIC incessantly infuses high-concentration cytotoxic medicine directly into tumours through viscus arteries to maximize its killing impact on tumour cells and reduce its harmful impact on traditional liver tissue. Compared with TACE, HAIC is also appropriate for primary cancer of liver patients with venous blood vessel cancer coagulum.Citation9,Citation10 The median survival time of patients with HCC and PVTT was only 2.7 monthsCitation11 and that with unresectable HCC was less than 6 months if left untreated.Citation12 TACE alone also has limited efficacy in HCC with PVTT,Citation13,Citation14 and the efficacy of TACE is largely dependent upon tumor size. Additionally, HAIC may be beneficial since it decreases tumor size and by this, it reduces the risk of HCC rupture.Citation15 For patients with particular large tumors (>7 cm), the OS after TACE was only 11.2–13.2 months.Citation16,Citation17 Therefore, patients with huge mass HCC and PVTT were included in the study and are reported in this report.
Recently, oxaliplatin-based HAIC has achieved positive therapeutic results and has become a replacement analysis hotspot within the field of liver cancer.Citation18,Citation19 Compared with lenvatinib alone, triple combination therapy with lenvatinib, toripalimab, and HAIC showed longer progression-free survival (11.1 vs 5.1 months), longer overall survival (not reached vs 11 months), and a higher objective response rate (RECIST: 59.2% vs 9.3%; modified RECIST: 67.6% vs 16.3%).Citation20 Some clinical studies have shown that for patients with advanced liver cancer, HAIC combined with targeted medical care and immunotherapy has a greater therapeutic response and survival advantages.Citation7,Citation21 In an irregular clinical test study (9810) presented at ESMO 2020, there was a large distinction in the surgical conversion rate between HAIC-FOLFOX and TACE for unresectable carcinoma, with 23.8% within the HAIC cluster and 11.5% within the TACE cluster (p< 0.004).Citation22 HAIC seems to provide further survival advantages for Asian patients with unresectable HCC.Citation23,Citation24 It is proposed in many studies that HAIC yields an expressively higher response rate than systemic chemotherapy or sorafenib and among TACE refractory cases, especially HCC with PVTT.Citation25–27 Recently, a randomized Phase III trial study showed that HAIC-FOLFOX showed a higher response rate than the TACE (46% vs 18%) and a longer median progression-free survival (9.6 vs 5.4 months), and the median overall survival in the HAIC-FOLFOX group was 23.1 months versus 16.1 months in the TACE group in the unresectable hepatocellular carcinoma (largest diameter $ 7 cm).Citation28 As a result, in patients with combined PVTT or large HCC, HAIC seems to be more effective than TACE.
However, during HAIC-FOLFOX, the patient needs to receive a typical blood vessel infusion of therapy medication for 46 h, requiring the patient to be strictly confined to bed and immobilized for a minimum of 52 h, which results in increased pain and affects the patient’s comfort during hospitalization. Therefore, patients receiving HAIC-FOLFOX (oxaliplatin + leucovorin + 5-fluorouracil) have an increased risk of catheter displacement and catheter-related infections due to their bed rest time.
Combining these three treatment modalities may have a possible synergistic impact and show encouraging early effectiveness findings in advanced HCC due to the distinct anti-malignancy mechanisms of TKIs, PD-1 inhibitors, and HAIC. Chemotherapy can increase antigenicity via immunogenic cell death of tumor cells as well as reduction of “off-target” immunosuppression in the tumor microenvironment.Citation29 Lenvatinib is more effective than sorafenib in inhibiting VEGFRs and fibroblast growth factor receptors, and blocking these pathways can improve the effectiveness of PD-1 inhibitors by reducing immunosuppression in the tumor and its surrounding tissue.Citation30,Citation31 mHAIC relies on HAIC-FOLFOX but replaces fluorouracil with S-1. S-1 is an oral fluorouracil chemotherapy drug, made up of tegafur, gimeracil and oteracil potassium. Existing literature has shown that the effectiveness of S-1 combined with oxaliplatin in the treatment of advanced HCC is comparable to that of sorafenib, and the incidence of adverse reactions is lower; thus, it is a safe and effective treatment strategy.Citation32 In addition, oral S-1 maintains a high blood concentration and prolongs the action time of fluorouracil in neoplasm tissues and blood, therefore enhancing the antitumour impact and causing less irritation and adverse reactions to the GI tract.Citation33 Compared with the blood vessel infusion of 5-FU, oral S-1 may greatly reduce the absolute bed rest time of patients undergoing HAIC (only 8 h absolute bed rest when undergoing mHAIC), modify the treatment procedure, improve the patient’s treatment compliance, and reduce the chance of thrombosis. Here, we reported two cases that had only grade 1 adverse reactions, such as a decrease in PLTs, and no significant adverse responses ().
However, considering the limited data of mHAIC in HCC reported thus far, this study provides a background for further development of mHAIC combined with lenvatinib and camrelizumab in advanced HCC. We are currently preparing a Phase II study of mHAIC combined with lenvatinib and camrelizumab as a treatment in advanced HCC (http://www.chictr.org.cn, Chinese Clinical Trial Register number: ChiCTR2300067295).
Ethics Statement
Details of the case reported in the article were approved by the central institution, The Affiliated Hospital of Yanbian University.
Consent for Publication
This report and any attendant pictures were revealed with the patients’ written consent.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We give thanks to the patients and everyone involved in this study.
Additional information
Funding
References
- Wakayama K, Kamiyama T, Yokoo H, et al. Huge hepatocellular carcinoma greater than 10 cm in diameter worsens prognosis by causing distant recurrence after curative resection. J Surg Oncol. 2017;115(3):324–329. doi:10.1002/jso.24501
- Yang B, Li CL, Guo WH, et al. Intra-arterial ethanol embolization augments response to TACE for treatment of HCC with portal venous tumor thrombus. BMC Cancer. 2018;18(1):101. doi:10.1186/s12885-018-3989-2
- Huang YH, Wu JC, Chen SC, et al. Survival benefit of transcatheter arterial chemoembolization in patients with hepatocellular carcinoma larger than 10 cm in diameter. Aliment Pharmacol Ther. 2006;23(1):129–135. doi:10.1111/j.1365-2036.2006.02704.x
- Ueshima K, Kudo M, Takita M, et al. Hepatic arterial infusion chemotherapy using low-dose 5-fluorouracil and cisplatin for advanced hepatocellular carcinoma. Oncology. 2010;78(Suppl 1):148–153. doi:10.1159/000315244
- Obi S, Sato S, Kawai T. Current status of hepatic arterial infusion chemotherapy. Liver Cancer. 2015;4(3):188–199. doi:10.1159/000367746
- Long Y, Song X, Guan Y, et al. Sorafenib plus hepatic arterial infusion chemotherapy versus sorafenib alone for advanced hepatocellular carcinoma: a systematic review and meta-analysis. J Gastroenterol Hepatol. 2022;38(4):486–495.
- Mei J, Tang YH, Wei W, et al. Hepatic arterial infusion chemotherapy combined with PD-1 inhibitors plus lenvatinib versus PD-1 inhibitors plus lenvatinib for advanced hepatocellular carcinoma. Front Oncol. 2021;11:618206. doi:10.3389/fonc.2021.618206
- Huang W, You L, Yang S, et al. Metronomic S-1 chemotherapy plus transcatheter arterial chemoembolization (TACE): a promising treatment of hepatocellular carcinoma refractory to TACE. J BUON. 2016;21(4):909–916.
- Ikeda M, Shimizu S, Sato T, et al. Sorafenib plus hepatic arterial infusion chemotherapy with cisplatin versus sorafenib for advanced hepatocellular carcinoma: randomized Phase II trial. Ann Oncol. 2016;27(11):2090–2096. doi:10.1093/annonc/mdw323
- Hu J, Bao Q, Cao G, et al. Hepatic arterial infusion chemotherapy using oxaliplatin plus 5-fluorouracil versus transarterial chemoembolization/embolization for the treatment of advanced hepatocellular carcinoma with major portal vein tumor thrombosis. Cardiovasc Intervent Radiol. 2020;43(7):996–1005. doi:10.1007/s00270-019-02406-3
- Llovet JM, Bustamante J, Castells A, et al. Natural history of untreated nonsurgical hepatocellular carcinoma: rationale for the design and evaluation of therapeutic trials. Hepatology. 1999;29(1):62–67. doi:10.1002/hep.510290145
- Llovet JM, Di Bisceglie AM, Bruix J, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. J Natl Cancer Inst. 2008;100(10):698–711. doi:10.1093/jnci/djn134
- Kim GA, Shim JH, Yoon SM, et al. Comparison of chemoembolization with and without radiation therapy and sorafenib for advanced hepatocellular carcinoma with portal vein tumor thrombosis: a propensity score analysis. J Vasc Interv Radiol. 2015;26(3):320–329 e326. doi:10.1016/j.jvir.2014.10.019
- Koo JE, Kim JH, Lim YS, et al. Combination of transarterial chemoembolization and three-dimensional conformal radiotherapy for hepatocellular carcinoma with inferior vena cava tumor thrombus. Int J Radiat Oncol Biol Phys. 2010;78(1):180–187. doi:10.1016/j.ijrobp.2009.07.1730
- Pavlek G, Romic I, Juzbasic K, et al. Case report: urgent liver pathologies: all in one. Front Surg. 2022;9:940856. doi:10.3389/fsurg.2022.940856
- Lo CM, Ngan H, Tso WK, et al. Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology. 2002;35(5):1164–1171. doi:10.1053/jhep.2002.33156
- Shi M, Lu LG, Fang WQ, et al. Roles played by chemolipiodolization and embolization in chemoembolization for hepatocellular carcinoma: single-blind, randomized trial. J Natl Cancer Inst. 2013;105(1):59–68. doi:10.1093/jnci/djs464
- Zhang H, Zeng X, Peng Y, Tan C, Wan X. Cost-effectiveness analysis of hepatic arterial infusion chemotherapy of infusional fluorouracil, leucovorin, and oxaliplatin versus transarterial chemoembolization in patients with large unresectable hepatocellular carcinoma. Front Pharmacol. 2022;13:849189. doi:10.3389/fphar.2022.849189
- Li S, Lyu N, Han X, et al. Hepatic artery infusion chemotherapy using fluorouracil, leucovorin, and oxaliplatin versus transarterial chemoembolization as initial treatment for locally advanced hepatocellular carcinoma: a propensity score-matching analysis. J Vasc Interv Radiol. 2021;32(9):1267–1276 e1261. doi:10.1016/j.jvir.2021.06.008
- He MK, Liang RB, Zhao Y, et al. Lenvatinib, toripalimab, plus hepatic arterial infusion chemotherapy versus lenvatinib alone for advanced hepatocellular carcinoma. Ther Adv Med Oncol. 2021;13:17588359211002720. doi:10.1177/17588359211002720
- Luo L, Xiao Y, Zhu G, et al. Hepatic arterial infusion chemotherapy combined with PD-1 inhibitors and tyrosine kinase inhibitors for unresectable hepatocellular carcinoma: a tertiary medical center experience. Front Oncol. 2022;12:1004652. doi:10.3389/fonc.2022.1004652
- Zhou H, Song T. Conversion therapy and maintenance therapy for primary hepatocellular carcinoma. Biosci Trends. 2021;15(3):155–160. doi:10.5582/bst.2021.01091
- Guo W, Gao J, Zhuang W, Wu Z, Li B, Chen S. Efficacy and safety of hepatic arterial infusion chemotherapy combined with transarterial embolization for unresectable hepatocellular carcinoma: a propensity score-matching cohort study. JGH Open. 2020;4(3):477–483. doi:10.1002/jgh3.12285
- Kondo Y, Fukuda R. 肝細胞癌治療における肝動注療法の最先端 [Cutting edge of hepatic artery infusion chemotherapy for hepatocellular carcinoma]. Gan To Kagaku Ryoho. 2020;47(1):1–5. Japanese.
- Ahn YE, Suh SJ, Yim HJ, et al. Comparison of sorafenib versus hepatic arterial infusion chemotherapy-based treatment for advanced hepatocellular carcinoma with portal vein tumor thrombosis. Gut Liver. 2021;15(2):284–294. doi:10.5009/gnl19367
- Moriguchi M, Aramaki T, Nishiofuku H, et al. Sorafenib versus hepatic arterial infusion chemotherapy as initial treatment for hepatocellular carcinoma with advanced portal vein tumor thrombosis. Liver Cancer. 2017;6(4):275–286. doi:10.1159/000473887
- He M, Li Q, Zou R, et al. Sorafenib plus hepatic arterial infusion of oxaliplatin, fluorouracil, and leucovorin vs sorafenib alone for hepatocellular carcinoma with portal vein invasion: a randomized clinical trial. JAMA Oncol. 2019;5(7):953–960. doi:10.1001/jamaoncol.2019.0250
- Li QJ, He MK, Chen HW, et al. Hepatic arterial infusion of oxaliplatin, fluorouracil, and leucovorin versus transarterial chemoembolization for large hepatocellular carcinoma: a randomized Phase III trial. J Clin Oncol. 2022;40(2):150–160. doi:10.1200/JCO.21.00608
- Mathew M, Enzler T, Shu CA, Rizvi NA. Combining chemotherapy with PD-1 blockade in NSCLC. Pharmacol Ther. 2018;186:130–137. doi:10.1016/j.pharmthera.2018.01.003
- Tohyama O, Matsui J, Kodama K, et al. Antitumor activity of lenvatinib (e7080): an angiogenesis inhibitor that targets multiple receptor tyrosine kinases in preclinical human thyroid cancer models. J Thyroid Res. 2014;2014:638747. doi:10.1155/2014/638747
- Courau T, Nehar-Belaid D, Florez L, et al. TGF-beta and VEGF cooperatively control the immunotolerant tumor environment and the efficacy of cancer immunotherapies. JCI Insight. 2016;1(9):e85974. doi:10.1172/jci.insight.85974
- Lv Y, Liang R, Hu X, et al. Combination of oxaliplatin and S-1 versus sorafenib alone in patients with advanced hepatocellular carcinoma. Pharmazie. 2014;69(10):759–763.
- Liu B, Ying J, Luo C, Xu Q, Zhu L, Zhong H. S-1 combined with oxaliplatin as first line chemotherapy for Chinese advanced gastric cancer patients. Hepatogastroenterology. 2012;59(114):649–653. doi:10.5754/hge11893