
Abstract
Aim
Nurses play a major role in critical care units (CCUs), providing care to critically ill patients while also facing numerous health challenges that impair their quality of life. This was especially evident during the COVID-19 pandemic. The aim of this study was to assess the professional quality of life (ProQOL) and establish the prevalence of compassion satisfaction and compassion fatigue among CCU nurses in Saudi Arabia.
Methods
A cross-sectional survey of CCU nurses was conducted using the ProQOL Scale, consisting of three subscales: 1) compassion satisfaction and compassion fatigue, 2) burnout, and 3) secondary traumatic stress. The data were analyzed to obtain descriptive and inferential statistics.
Results
A total of 238 ICU nurses, who were predominantly female (83%) and had a bachelor’s degree (80%), participated in this study. The ProQOL subscales exhibited varied mean scores across demographic variables. Statistically significant differences were observed in the compassion satisfaction (p=0.014) of CCU nurses working in public hospitals, and in the secondary traumatic stress (p=0.006) among nurses working in night shifts. The percentage distribution of CCU nurses’ individual levels for all the ProQOL subscales were within the average to high levels.
Conclusion
The ProQOL was significantly affected by the COVID-19 pandemic. Furthermore, varied ProQOL mean scores across demographic characteristics suggest that interpersonal differences should be considered when developing improvement initiatives.
Introduction
Nurses play a major role in critical care units (CCUs), where they provide healthcare in a complex and challenging work environmentCitation1 and are frequently subjected to fulfilling high demands.Citation2 Working in a CCU involves complex multitasking, high workloads, and providing specialized care to critically ill and reliant patients, all of which can be overwhelming for nurses,Citation3 especially during emergencies such as the coronavirus (COVID-19) pandemic. The COVID-19 pandemic has evidently been the most disruptive force to the CCU work environment, since CCU staff worldwide were overwhelmed with surges in critically ill patients being admitted for treatment.Citation4 The quality of life of CCU staff has been at risk since they are particularly exposed to the COVID-19 epidemic on the front lines. Studies indicated several factors that could be detrimental to the health of CCU staff, including the lack of access to adequate protective equipment,Citation5 exhaustion brought on by wearing personal protective equipment all day long,Citation6 long working hours and unexpected changes in the type of work,Citation7 worry about trapping or infecting their family members,Citation8 and abandoning their homes to avoid infecting their family members. The risk of developing various psychological symptoms and mental health disorders is evident, given that CCU staff are under tremendous psychological pressure.Citation8 Therefore, it is unsurprising that the COVID-19 epidemic has decreased professional quality of life (ProQOL) and aggravated pre-existing issues like burnout.Citation9
Caring is an essential value in nurses’ personal and professional livesCitation10 and is a complex element of professional nursing practice. The quality of patient care and outcomes depends mainly on a caregiver’s ProQOL. ProQOL is defined as the quality of a person’s life perceived in relation to his/her work, which comprises compassion satisfaction (CS) and compassion fatigue (CF). CS encompasses the positive elements of caring for others, while CF encompasses its negatives.Citation11–13 The former refers to a person’s satisfaction with their ability to do their job wellCitation12 while the latter refers to a state of exhaustion that limits one’s ability to engage in caring relationships and has been recognized as a critical component affecting professional nursing performance.Citation14 CF is composed of burnout and secondary traumatic stress. While burnout refers to exhaustion caused by emotionally demanding situations, resulting in poor attitudes and detachment,Citation13,Citation15 secondary traumatic stress was described by Charles Figley as an event occurring to one person but affecting many.Citation16 CCU nurses are subjected to secondary traumatic stress through indirect exposure, resulting in fear and helplessness.Citation13,Citation17 All of these elements collectively constitute ProQOL, which is affected by work environment.Citation11,Citation18 Unhealthy work environments have been reported to result in increased turnover rates, lower productivity, physical exhaustion, and CF.Citation11,Citation19
CS is positively related to the ability to communicate (effective interactions among nurses, colleagues, or patients), collaborate (contributing to making the work environment more positive to establish a stable connection among team members), and lead, wherein high CS among nurses is supported by welfare, appreciation, achievement, joy, gratitude, and hope.Citation20,Citation21 CCU nurses attain satisfaction by providing compassionate care to patients and their families. However, they are susceptible to CF as a result of repeated exposure to traumatic events. CCU nurses are responsible for treating patients who are sick, injured, traumatized, or vulnerable, which routinely exposes them to pain, trauma, and suffering.Citation22 Although the signs and symptoms of CF may not be easily recognized by nurses or co-workers,Citation23 it is recognized as a problem in which CCU nurses are more susceptible to experiencing CF compared to non-CCU nurses.Citation22
In light of the definition of ProQOL, the circumstances created by the COVID-19 epidemic have put CCU staff’s mental health at risk and may have contributed to their levels of CF and CS. The CCU nurses’ ProQOL are of special concern because providing care to patients who are at high risk of actual or potential life-threatening health problems requires intensive and vigilant care.Citation24 The impact of the ProQOL of nurses is an important field of nursing research, especially because it is related to a healthy work environment, patient safety, and quality of care.Citation25 Nursing research has progressively demonstrated the impact of nurses’ QOL on the quality of their work experiences and patient outcomes in CCUs.Citation1,Citation2,Citation12,Citation14 However, research on the assessment of the ProQOL of CCU nurses in the aftermath of the COVID-19 pandemic is still scarce, especially in Saudi Arabia. Therefore, the aim of this study was to assess the ProQOL of CCU nurses in Saudi Arabia.
Methods
Population and Study Area
This cross-sectional study was conducted between January 2021 and June 2022 at public and private hospitals affiliated with the Southern Region Health Administration in Saudi Arabia. Data were collected using a self-administered and structured questionnaire. The survey population comprised full-time CCU nurses. Sample size was estimated using a priori power analysis with the G*Power (version 3.1.9) software to determine the minimum sample size required.Citation26 Results indicated the required sample size to achieve 80% power for detecting a medium effect, at a significance criterion of α = 0.05, was N = 130 for the Independent Sample t-test. Due to the lack of accessibility to the contact information of all CCU nurses and the difficulty of finding data on population size, nursing supervisors in the hospitals were contacted and asked to distribute the survey among CCU nurses in their hospitals. Nurse supervisors sent 326 invitations to the CCU nurses via email. A reminder email was sent two weeks after the initial invitation. Multiple responses were avoided by sending the survey by email, which creates a unique, one-time use link for each participant. A sample of 238 CCU nurses was collected for this study, which is considered adequate to avoid potential sources of bias.
The questionnaire was distributed online, for the purposes of cost, time, and geographical coverage,Citation27 using Qualtrics Research Core (Qualtrics, Provo, USA). The survey’s cover page included an introductory information sheet that contained the study’s objective, duration, and the option to withdraw at any time, besides privacy and confidentiality statements. Additionally, the first page included a consent form, where participants had to indicate their approval for participation in order to access the survey. Before data collection began, this study acquired the approval of the ethical committee at Jazan University. Furthermore, participant confidentiality was protected by de-identifying all responses.
Survey
The demographic data collected from the participants included age, sex, education level, years of experience, time of shift, and type of hospital. ProQOL version 5 was used in the study, with permission from the instrument’s author.Citation12 The ProQOL survey consisted of 3 subscales: 1) CS and CF, 2) burnout, and 3) secondary traumatic stress. Each subscale was unique, and the results of the scales could not be combined to provide a single, meaningful score. The instrument included 30 items, 10 for each scale, which were rated numerically on a 5-point Likert scale, ranging from 0 (never) to 5 (very often).
A pilot study was conducted to test the feasibility and applicability of the questionnaire. Twenty participants were surveyed and took 10–15 min to complete the questionnaire, their responses were excluded from analysis of the main data. Amendments in the questionnaire were not warranted. The reliability statistical parameter was calculated using Cronbach’s alpha for each subscale. The internal consistency reliability values for each of the ProQOL subscales are presented in . Cronbach’s alpha was 0.92, 0.76, and 0.89 for CS, burnout, and secondary traumatic stress, respectively. Previous testing conducted by the author of the ProQOL instrument indicated acceptable levels of Cronbach’s alpha for each of the ProQOL subscales.Citation12 The coefficients obtained in this study were appropriate and could therefore be used in this study.
Table 1 Cronbach’s Alpha (α): Comparison with Cronbach’s Alpha Coefficients Reported by Stamm
Statistical Analyses
The Statistical Package for Social Sciences (SPSS) (Version 27, IBM Corp., Armonk, N.Y., USA) was employed to conduct the statistical analyses in this study. Descriptive statistics were calculated for the continuous (mean, standard deviation [SD]) and categorical variables (n, %). The internal consistency reliability of the ProQOL scale was examined using Cronbach’s alpha. The raw data of the subscales were converted to t scores, as indicated in the ProQOL manual.Citation12 The use of t scores produced a standardization of each subscale in which the scale means equaled 50, with an SD of 10. The standardized t scores were classified as low (≤ 43), average (43–56), or high (≥ 57). Next, the percentage distribution of the CCU nurses at each scoring threshold for the ProQOL sub-scales was obtained. The normality of distribution of the quantitative variables was evaluated using the Kolmogorov–Smirnov test. In addition, Mann–Whitney U and Kruskal–Wallis tests were conducted to compare the demographic variables with the ProQOL subscales, wherein significance was set at p < 0.05.
Results
Demographic Characteristics
A total of 238 CCU nurses participated in this study, with a response rate of about 73%. As depicted in , the demographic data indicated that 83% of the respondents were female, 50% were in the age group of 22–30 years, and most had a bachelor’s degree (80%). Moreover, 45% of the respondents had 6–10 years of work experience, 65% worked alternate shifts, and 55% were employed in private hospitals.
Table 2 Summary of Demographic Characteristics
ProQOL and Demographic Characteristics
As shown in , the ProQOL subscales—CS, burnout and secondary traumatic stress—were compared across demographic variables. When the groups in each demographic category were compared, variations in the mean scores of their ProQOL subscales were observed. The CS was higher for male nurses, nurses aged ≥41 years, those with postgraduate education, with work experience of >10 years, working alternate shifts, and those in private hospitals. The burnout was higher for female nurses, nurses aged 22–30 years, those with a bachelor’s degree, with work experience of 0–5 years, working night shifts, and in public hospitals. The secondary traumatic stress was higher for male nurses, nurses aged 31–40 years, those with a bachelor’s degree, with work experience of 6–10 years, working night shifts, and in private hospitals. CCU nurses working in public hospitals experienced significantly higher CS (p=0.014), while those working night shifts reported significantly greater secondary traumatic stress (p=0.006).
Table 3 Mean Standardized t Scores for Compassion Satisfaction, Burnout, and Secondary Traumatic Stress Among CCU Nurses
ProQOL and Individual Levels of Compassion Satisfaction and Compassion Fatigue
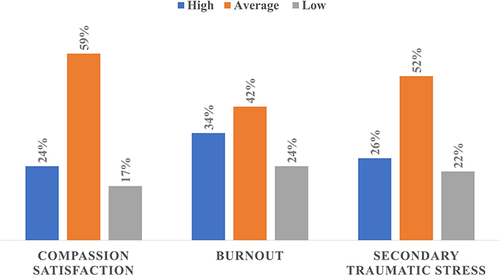
depicts the percentage distribution of CCU nurses at each scoring threshold for the ProQOL subscales. The CS levels were high for 24% (n=56), average for 59% (n=141), and low for 17% (n=41) of the CCU nurses. The burnout levels were high for 34% (n=81), average for 42% (n=101), and low for 24% (n=56) of the CCU nurses. Again, the secondary traumatic stress levels were high for 26% (n=62), average for 52% (n=124), and low for 22% (n=52) of the CCU nurses. Overall, all the subscales were within the average to high levels.
Figure 1 Individual levels of compassion satisfaction and compassion fatigue: low (≤ 43), average (43–56), or high (≥ 57).
Discussion
CCU nurses are frequently exposed to factors that can affect their mental health because they deal with physical and emotional pain in serious and complex situations and are often faced with tense situations at work. Thus, nurses are susceptible to CS, burnout, and secondary traumatic stress, which influence their health and can negatively affect the care they perform. Studies indicated that the circumstances created by the COVID-19 epidemic have put CCU staff’s mental health at risk and may have contributed to their levels of CF and CS.Citation9,Citation28–33 In this study, the CCU nurses reported encountering all elements of the ProQOL scale at an average level, leaning toward the higher level. This finding is consistent with that of a previous study.Citation11 Other studies have found that nurses in CCUs are at risk of feeling higher CF than CS.Citation22,Citation34 Compared with before and after the COVID-19 pandemic, studies suggest that healthcare professionals had high scores for compassion fatigue,Citation28–33 while other studies reported the levels of CS were within average or high and similar to those from before the COVID-19 pandemic.Citation9
ProQOL and Demographic Characteristics
ProQOL may be impacted by demographic characteristics, suggesting that nurses coping with stressful environments may be affected by intrinsic qualities. When the groups in each demographic category were compared, the mean scores of their ProQOL subscales were observed to be varied. These findings may indicate an opportunity for developing improvement plans that take interpersonal differences into consideration.
In this study, CS was observed to be higher for older and more experienced CCU nurses, who also exhibited lower scales of burnout and secondary traumatic stress compared to their younger counterparts, which is consistent with a previous study by Sacco et al.Citation11 The fact that older nurses have more professional and life experience may have prepared them to better cope with the challenges of CCU nursing. Another study found a significant difference in the burnout and secondary traumatic stress scales in terms of age and years of CCU experience, justifying that older and more experienced CCU nurses possess more knowledge and skills, which, in turn, lowers their risk of experiencing CF.Citation35,Citation36 However, several studies reached conclusions that were contrary to the current study,Citation35–38 indicating that further studies are warranted to fully examine this relationship.
In this study, male CCU nurses reported higher scores for the CS and secondary traumatic stress scales and lower burnout scores compared to their female counterparts. Several previous studies have indicated differences in terms of gender in the ProQOL subscales.Citation11,Citation22 This may be attributable to the “status shield”, a term coined by HochschildCitation39 to describe the management of emotional labor in the workplace.
Furthermore, the ProQOL scores indicated some differences based on educational level. In this study, CCU nurses with postgraduate education had higher CS and lower burnout and secondary traumatic stress scales compared to their counterparts. Notably, higher education levels have previously been associated with higher levels of CS and lower levels of CF.Citation40 Education levels may influence healthcare professionals’ perceptions of responsibility and duty toward patients.Citation41 However, a previous study found that CCU nurses with a bachelor’s degree had lower CS scores than those with diploma or postgraduate qualifications,Citation11,Citation21 while another study found that educational level had no effect on CS and CF.Citation42
Regarding hospital sitting and work shifts, this study found that CCU nurses in public hospitals and those working night shifts reported lower scores on CS and higher scores on CF compared to those working in private hospitals. This result warrants work environment interventions. A healthy work environment and ProQOL are interrelated and can substantially affect the level of CS and CF experienced by CCU nurses.Citation1,Citation34
Limitations and Scope for Future Research
The strengths of this study lie in its usage of a reliable and valid assessment tool—the ProQOL scale—to support continuous improvement through regular assessments and benchmarking. In addition, the use of such an assessment tool allows for performing a meta-analysis, which contributes to the evidence-based literature on nursing ProQOL. However, some limitations of this study must be acknowledged. The cross-sectional design used in this study indicates that the data could only be representative of the specific study period. Therefore, a longitudinal design study is recommended to properly evaluate and reflect on the ProQOL. Future studies using longitudinal data are required to confirm the causal relationships suggested by our findings. Moreover, the study’s sample methodology may restrict the study’s generalizability.
Conclusion
The ProQOL assessment scores can be used to measure the effectiveness of work environment interventions. The ProQOL was significantly affected by the COVID-19 pandemic, indicating average to high levels for ProQOL subscales. Moreover, the ProQOL subscale scores were observed to vary across demographic characteristics, suggesting that interpersonal differences should be considered when developing improvement initiatives. Interventions could contribute to better work environments, ProQOL, and healthcare services. Regular periodic assessments should be conducted, and their results used as benchmarks for future comparisons to monitor the implemented improvement initiatives and identify shortfalls.
Data Sharing Statement
The data is available upon request.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Jazan University (REC-43/11/279).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Disclosure
The authors declare no conflicts of interest.
Acknowledgments
The authors would like to thank the nursing department’s supervisors in Saudi Arabia.
Additional information
Funding
References
- Ulrich B, Barden C, Cassidy L, Varn-Davis N. Critical care nurse work environments 2018: findings and implications. Crit Care Nurse. 2019;39(2):67–84. doi:10.4037/ccn2019605
- Woodrow P. Intensive Care Nursing: A Framework for Practice. Routledge; 2018.
- Rosa WE, Ferrell BR, Wiencek C. Increasing critical care nurse engagement of palliative care during the COVID-19 pandemic. Crit Care Nurse. 2020;40(6):e28–e36. doi:10.4037/ccn2020946
- Sumner S. Impact of the COVID-19 pandemic on the work environment and mental health of intensive care unit nurses: reflections from the United States. Nurs Crit Care. 2022. doi:10.1111/nicc.12759
- Pfefferbaum B, North CS. Mental health and the Covid-19 pandemic. N Engl J Med. 2020;383(6):510–512. doi:10.1056/NEJMp2008017
- Liu X, Chen J, Wang D, et al. COVID-19 outbreak can change the job burnout in health care professionals. Front Psychiatry. 2020;11:563781. doi:10.3389/fpsyt.2020.563781
- Galli F, Pozzi G, Ruggiero F, et al. A systematic review and provisional metanalysis on psychopathologic burden on health care workers of coronavirus outbreaks. Front Psychiatry. 2020;11:568664. doi:10.3389/fpsyt.2020.568664
- Şahin CU, Kulakaç N. Exploring anxiety levels in healthcare workers during COVID-19 pandemic: Turkey sample. Curr Psychol. 2022;41(2):1057–1064. doi:10.1007/s12144-021-01730-7
- Lluch C, Galiana L, Doménech P, Sansó N. The impact of the COVID-19 pandemic on burnout, compassion fatigue, and compassion satisfaction in healthcare personnel: a systematic review of the literature published during the first year of the pandemic. Healthcare. 2022;10(2):364. doi:10.3390/healthcare10020364
- Mohammadi M, Peyrovi H, Mahmoodi M. The relationship between professional quality of life and caring ability in critical care nurses. Dimensions Crit Care Nurs. 2017;36(5):273–277. doi:10.1097/DCC.0000000000000263
- Sacco TL, Ciurzynski SM, Harvey ME, Ingersoll GL. Compassion satisfaction and compassion fatigue among critical care nurses. Crit Care Nurse. 2015;35(4):32–43; quiz 31p following 43. doi:10.4037/ccn2015392
- Stamm B. The Concise ProQOL Manual: The Concise Manual for the Professional Quality of Life Scale. 2nd ed. Scientific Research; 2010.
- van Mol MMC, Kompanje EJO, Benoit DD, Bakker J, Nijkamp MD. The prevalence of compassion fatigue and burnout among healthcare professionals in intensive care units: a systematic review. PLoS One. 2015;10(8):e0136955. doi:10.1371/journal.pone.0136955
- Nolte AG, Downing C, Temane A, Hastings-Tolsma M. Compassion fatigue in nurses: a metasynthesis. J Clin Nurs. 2017;26(23–24):4364–4378. doi:10.1111/jocn.13766
- Smart D, English A, James J, et al. Compassion fatigue and satisfaction: a cross-sectional survey among US healthcare workers. Nurs Health Sci. 2014;16(1):3–10. doi:10.1111/nhs.12068
- Figley C. COMPASSION FATIGUE: Coping with Secondary Traumatic Stress Disorder in Those Who Treat the Traumatized. NY: Brunner/Routledge; 1995.
- Wentzel D, Brysiewicz P. The consequence of caring too much: compassion fatigue and the trauma nurse. J Emerg Nurs. 2014;40:95–97. doi:10.1016/j.jen.2013.10.009
- Tunlind A, Granström J, Engström Å. Nursing care in a high-technological environment: experiences of critical care nurses. Intensive Crit Care Nurs. 2014;31:116–123. doi:10.1016/j.iccn.2014.07.005
- Mason V, Leslie G, Clark K, et al. Compassion fatigue, moral distress, and work engagement in surgical intensive care unit trauma nurses: a pilot study. Dimensions Crit Care Nurs. 2014;33:215–225. doi:10.1097/DCC.0000000000000056
- Kelly L, Lefton C. Effect of meaningful recognition on critical care nurses’ compassion fatigue. Am J Crit Care. 2017;26:438–444. doi:10.4037/ajcc2017471
- Sacco T, Copel L. Compassion satisfaction: a concept analysis in nursing. Nurs Forum. 2017;53:76–83. doi:10.1111/nuf.12213
- Hooper C, Craig J, Janvrin D, Wetsel M, Reimels E. Compassion satisfaction, burnout, and compassion fatigue among emergency nurses compared with nurses in other selected inpatient specialties. J Emerg Nurs. 2010;36:420–427. doi:10.1016/j.jen.2009.11.027
- Crewe CD. The Watson room: managing compassion fatigue in clinical nurses on the front line. 2016.
- Urden L, Kathleen M, Lough M. Priorities in Critical Care Nursing. 8th ed. Elsevier Health Sciences; 2019.
- Institute of M. Keeping Patients Safe: Transforming the Work Environment of Nurses. Washington (DC): National Academies Press (US) Copyright 2005 by the National Academy of Sciences; All rights reserved.. 2004.
- Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
- Dykema J, Jones NR, Piché T, Stevenson J. Surveying clinicians by web: current issues in design and administration. Eval Health Prof. 2013;36(3):352–381. doi:10.1177/0163278713496630
- Arpacioglu S, Gurler M, Cakiroglu S. Secondary traumatization outcomes and associated factors among the health care workers exposed to the COVID-19. Int J Soc Psychiatry. 2021;67(1):84–89. doi:10.1177/0020764020940742
- Buselli R, Corsi M, Baldanzi S, et al. Professional quality of life and mental health outcomes among health care workers exposed to Sars-Cov-2 (Covid-19). Int J Environ Res Public Health. 2020;17(17):6180. doi:10.3390/ijerph17176180
- Çelmeçe N, Menekay M. The effect of stress, anxiety and burnout levels of healthcare professionals caring for COVID-19 patients on their quality of life. Front Psychol. 2020;11:597624. doi:10.3389/fpsyg.2020.597624
- Rapisarda F, Vallarino M, Cavallini E, et al. The early impact of the Covid-19 emergency on mental health workers: a survey in Lombardy, Italy. Int J Environ Res Public Health. 2020;17(22):8615. doi:10.3390/ijerph17228615
- Secosan I, Virga D, Crainiceanu ZP, Bratu T. The mediating role of insomnia and exhaustion in the relationship between secondary traumatic stress and mental health complaints among frontline medical staff during the COVID-19 pandemic. Behav Sci. 2020;10(11):164. doi:10.3390/bs10110164
- Wahlster S, Sharma M, Lewis AK, et al. The coronavirus disease 2019 pandemic’s effect on critical care resources and health-care providers: a global survey. Chest. 2021;159(2):619–633. doi:10.1016/j.chest.2020.09.070
- Monroe M, Morse E, Price J. The relationship between critical care work environment and professional quality of life. Am J Crit Care. 2020;29:145–149. doi:10.4037/ajcc2020406
- Burtson P, Stichler J. Nursing work environment and nurse Caring: relationship among motivational factors. J Adv Nurs. 2010;66:1819–1831. doi:10.1111/j.1365-2648.2010.05336.x
- Young J, Derr D, Cicchillo V, Bressler S. compassion satisfaction, burnout, and secondary traumatic stress in heart and vascular nurses. Crit Care Nurs Q. 2011;34:227–234. doi:10.1097/CNQ.0b013e31821c67d5
- Highfield J, Parry-Jones J. Professional quality of life in intensive care medicine: the 2018 faculty of intensive care medicine workforce survey. J Intensive Care Soc. 2019;21(4):299–304. doi:10.1177/1751143719877102
- Quijada-Martínez P, Cedeño-Idrogo I, Terán-ángel G. Quality of professional life and burnout of the nursing staff at an intensive care unit in Venezuela. Investigación y Educación en Enfermería. 2021;39. doi:10.17533/udea.iee.v39n2e08
- Hochschild AR. The Managed Heart. University of California Press; 2012.
- Sinclair S, Raffin-Bouchal S, Venturato L, Mijovic-Kondejewski J, Smith-MacDonald L. Compassion fatigue: a meta-narrative review of the healthcare literature. Int J Nurs Stud. 2017;69:9–24. doi:10.1016/j.ijnurstu.2017.01.003
- Ruiz-Fernández MD, Ramos-Pichardo JD, Ibáñez-Masero O, Cabrera-Troya J, Carmona-Rega MI, Ortega-Galán ÁM. Compassion fatigue, burnout, compassion satisfaction and perceived stress in healthcare professionals during the COVID-19 health crisis in Spain. J Clin Nurs. 2020;29(21–22):4321–4330. doi:10.1111/jocn.15469
- Jakimowicz S, Perry L, Lewis J. Compassion satisfaction and fatigue: a cross-sectional survey of Australian intensive care nurses. Austral Crit Care. 2017;31:396–405. doi:10.1016/j.aucc.2017.10.003