
Abstract
Although depression has generally been explained with monoamine theory, it is far more multifactorial, and therapies that address the disease’s pathway have not been developed. In this context, an understanding of neuroinflammation and neurovascular dysfunction would enable a more comprehensive approach to depression. Inflammation is in a sense a type of allostatic load involving the immune, endocrine, and nervous systems. Neuroinflammation is involved in the pathophysiology of depression by increasing proinflammatory cytokines, activating the hypothalamus–pituitary–adrenal axis, increasing glucocorticoid resistance, and affecting serotonin synthesis and metabolism, neuronal apoptosis and neurogenesis, and neuroplasticity. In future, identifying the subtypes of depression with increased vulnerability to inflammation and testing the effects of inflammatory modulating agents in these patient groups through clinical trials will lead to more concrete conclusions on the matter. The vascular depression hypothesis is supported by evidence for the association between vascular disease and late-onset depression and between ischemic brain lesions and distinctive depressive symptoms. Vascular depression may be the entity most suitable for studies of the mechanisms of depression. Pharmacotherapies used in the prevention and treatment of cerebrovascular disease may help prevent vascular depression. In future, developments in structural and functional imaging, electrophysiology, chronobiology, and genetics will reveal the association between depression and brain lesions. This article aims to give a general review of the existing issues examined in the literature pertaining to depression-related neuroinflammatory and vascular functions, related pathophysiology, applicability to depression treatment, and directions for future research.
Introduction
Inflammation can be defined as a type of immunoresponse to tissue injuries. In the past, it could only be diagnosed based on visual findings or changes in white-blood-cell counts, but even microinflammation can be measured today using substances released by cells during inflammation, such as cytokines or CRP, as markers. As a result, a considerable amount of research has been directed toward the measurement of the underlying inflammatory changes in several psychiatric disorders, including depression, and the link between physical and mental diseases is being interpreted in relation to inflammation. These efforts have risen from interest in sickness behaviors, such as fatigue and depressive symptoms, which develop in nearly 90% of patients undergoing interferon therapy for hepatitis C or cancer.Citation1 Initially, investigations focused mostly on the effects of systemic inflammation on the central nervous system (CNS). However, current research also explores neuroinflammation that occurs within the CNS.
The vascular depression hypothesis states that cerebrovascular diseases may be a predisposing or stimulating factor of depression and may cause depression to persist.Citation2 In other words, the presence of vascular risk factors or vascular diseases per se increases the risk of depression. This theory is supported by epidemiological studies reporting a higher prevalence of depression in patients with hypertension, diabetes mellitus, coronary artery disease, and stroke. Silent cerebral ischemia and white-matter hyperintensity (WMH) are more commonly observed in late-onset depression, and evidence suggests that depressive symptoms are related to the collapse of cortico striato pallido thalamo cortical circuits.Citation3,Citation4
Such a view of neuroinflammation or neurovascular function in depression addresses the shortcomings of the monoamine theory, the classic pathological model for depression thus far. From this view, depression can be thought of as a result of failure of adjustment to allostatic load, and neuroinflammatory reaction and neurovascular functions are two factors that mediate this. This article aims to give a general review of the issues examined in the literature pertaining to depression-related neuroinflammatory and vascular functions, related pathophysiology, applicability to depression treatment, and directions of future research.
The source of the literature we reviewed was the electronic database Medline (1980–2017). The initial search was for combinations of the following terms: depression/major depressive disorder inflammation/immune/cytokine/neurogenesis/anti-inflammatory/cerebrovascular disease/vascular depression/vascular disease/ischemic. Inclusion criteria were original articles examining immune or vascular mechanisms underlying depression in animal or human subjects, “practice guidelines” for “type of article” from systematic reviews published by PubMed, and articles written in English. Exclusion criteria were letters to editors and editorials without data and studies outside the time window. Based on these criteria, we reviewed the titles of all citations and retrieved relevant abstracts for more detailed evaluation. When there was uncertainty, we studied the full article. We also hand-searched the reference lists of relevant studies and reviews to aid identification of further studies. We identified 965 references of interest, of which 118 were included in this review.
The limitation of this paper is that it is written in the format of narrative review for diverse topics, such as concept, hypothesis, current understanding, and treatment. We may have had certain biases in data-search method and conclusions. However, we used this format to provide a broad overview of a topic-related research area and easy understanding and interpretation.
Stress, cytokines, and depression
Cytokines are a broad and loose category of small proteins (~5–20 kDa) important in cell signaling as inflammatory mediators and they also affect neurotransmitter systems, brain functionality, and mood.Citation5–Citation7 Although cytokine function itself is not specific to major depressive disorder (MDD), recent research suggests that disease-specific molecular differences within the cytokines might be useful for differentiating patients with MDD from undepressed control subjects ().Citation6–Citation16
Table 1 Potential biomarkers in peripheral blood for the diagnosis of MDD
Stress is intimately related to the hypothalamic–pituitary–adrenal (HPA) axis and the sympathoadrenal system activated by corticotrophin-releasing hormone (CRH). CRH acts on the CRH1 and CRH2 receptors: the former is in charge of the “fight or flight” response, while the latter deals with adjustment to and recovery from stress.Citation17 When CRH1 receptors in the paraventricular nucleus of the hypothalamus are activated, the fight-or-flight response occurs, and when CRH1 receptors in the anterior pituitary are activated, adrenocorticotropic hormone is released, and the adrenal cortex is stimulated to increase synthesis and release of glucocorticoids. Furthermore, CRH stimulates the locus ceruleus to activate the central sympathetic nerve. An acute increase in glucocorticoids, such as cortisol, activates the mineralocorticoid receptors in the pituitary gland and hypothalamus, leading to a reduction in CRH release in a negative-feedback loop. However, exposure to chronic and high-intensity stress continuously increases cortisol secretion, desensitizing the glucocorticoid receptors. In the past, such hypersecretion of cortisol was thought to undermine immune functions, but today hypersecretion of proinflammatory cytokines as a result of activated immune functions is seen as a cause of a continuous rise in cortisol secretion. A previous report suggested that immune cells are not affected by glucocorticoids in depression and chronic stress, because the activation of cytokine pathways, such as p38 MAPK, hinders glucocorticoid signaling.Citation18,Citation19 In other words, cytokines inhibit the negative-feedback regulation of the HPA axis, maintaining hypercortisolemia. Previous study suggested that an injection of IL1 increases CRH, adrenocorticotropic hormone, and corticosteroid, whereas cytokines, such as IFNα and IL6, increase HPA-axis activity.Citation19
Cytokines are also associated with monoamines, such as serotonin, norepinephrine, and dopamine. Recent study findings have suggested that cytokines are involved in serotonin depletion in the CNS. When IL1β, which plays a similar role in stress reactions, is systemically injected, it increases the use of serotonin in the paraventricular nucleus of the hypothalamus and central amygdala, which increases the release of serotonin from the limbic system and norepinephrine from the hypothalamus.Citation19,Citation20
Moreover, stress increases proinflammatory cytokines and NFκB in its signaling pathway in the peripheral and CNS, as well as activating microglia in the brain, thereby elevating sensitivity to immunostimulation.Citation21,Citation22 Brain-derived neurotrophic factor ultimately affects sickness behavior through the growth and development of neurons and synaptic plasticity, and stress-induced IL1 decreases the expression of this protein.Citation23,Citation24
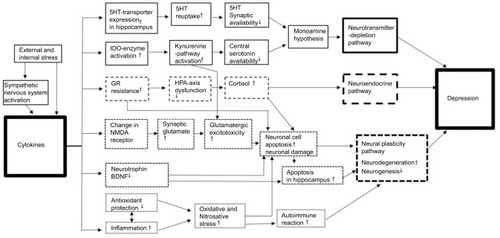
Many clinical and experimental studies have proposed the hypothesis that cytokines play an important role in the onset and persistence of depressive symptoms in vulnerable individuals. They suggest that proinflammatory cytokines increase HPA-axis activity and disturb serotonin metabolism and neurogenesis, thereby causing depressive symptoms.Citation25 Recent studies on the brain–immunity system have presented a few important results pertaining to the association between cytokines and depression as evidence for the cytokine hypothesis of depression ().Citation5,Citation25
Figure 1 Neuroinflammatory pathways in the pathogenesis of depression.
Notes: Cytokine production is initially activated by stress and sympathetic nervous system activation. In turn, cytokines have an important role by acting via neurotransmitter-depletion, neuroendocrine, and neural plasticity pathways. There are multiple interactions among these pathways, suggesting existence of a complex model for pathogenesis of depression. Reproduced from Jeon SW, Kim YK. Neuroinflammation and cytokine abnormality in major depression: cause or consequence in that illness? World J Psychiatry. 2016;6:284–293.Citation144
Abbreviations: HT, hydroxytryptamine; BDNF, brain-derived neurotrophic factor; GR, glucocorticoid receptor; HPA, hypothalamic–pituitary–adrenal; NMDA, N-methyl-d-aspartate.
First, the plasma concentration of proinflammatory cytokines is elevated in patients with depression. Studies have reported that plasma IL1, IL6, IL2 receptors, IL6 receptors, and plasma concentrations of acute-phase protein are elevated in patients with MDD.Citation25,Citation26 Furthermore, there are reports that sensitivity to depression increases in patients with gene polymorphisms for particular cytokines, such as TNFα and IL1.Citation27,Citation28 Second, the incidence of depression increases in diseases related to inflammatory responses. For example, the incidence of depression increases in cases of Cytomegalovirus infection, influenza infection, and chronic hepatitis.Citation29 Moreover, studies consistently report that autoimmune diseases, such as rheumatoid arthritis and myelosclerosis, and chronic inflammation diseases, such as cancer, are associated with depression.Citation30 Study findings that administration of cytokine antagonists improves depressive symptoms in depressed patients with immunoresponses and findings that injection of a trace amount of lipopolysaccharide (LPS; too low to feel physical symptoms) in healthy people induces depression, anxiety, and cognitive impairment serve as evidence.Citation31,Citation32 Third, regarding the relationship between cytokine-related treatment and depression, at least 25%–50% of patients who are administered IFNα, which is used for patients with such viral infections as hepatitis C or cancer patients, develop depression. Furthermore, behavioral changes, such as depressive mood, anxiety, irritability, apathy, cognitive impairment, fatigue, and pain, have been reported to follow administration of IFNα.Citation33 Among patients with malignant melanoma receiving IFNα treatment, MDD incidence was reduced more than fourfold, and treatment cessation due to severe depression and neurotoxicity was significantly lower among those who received paroxetine compared to a control group.Citation34
Through what mechanism do cytokines affect depression? Cytokines are thought to play an important role in depression through their interaction with monoamines, particularly serotonin, which has the closest relationship to depression. Tryptophan is a key amino acid in serotonin synthesis and is metabolized by IDO. Cytokines, including IL1, IL2, IL6, and IFN, activate IDO, which metabolizes tryptophan, ultimately lowering serum-tryptophan concentration. There are reports that IDO enzymatic activity increases and serum-tryptophan concentration decreases in immunocompromised patients, such as those undergoing immunotherapy and patients with acquired immunodeficiency syndrome, atherosclerosis, and rheumatoid arthritis. In particular, unlike TDO, which is mediated by cortisol, IDO is increased directly by IFNγ and TNFα.Citation24
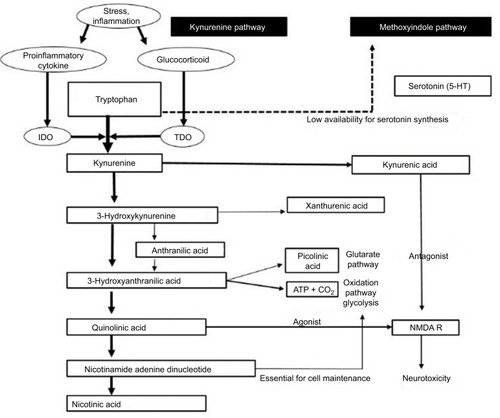
The association between cytokine-induced activation of IDO and depression can also be explained by the kynurenine pathway, which metabolizes tryptophan (). There is evidence suggesting that LPS and proinflammatory cytokines increase tryptophan consumption and serotonin turnover in the brain. This is believed to be because cytokine is involved not only in tryptophan deficiency caused by IDO activation but also in the production of neuroactive tryptophan metabolites. Tryptophan is metabolized to kynurenine by TDO and IDO, and kynurenine is in turn metabolized to kynurenic acid (KynA) and 3OH-Kyn. 3OH-Kyn is then metabolized to quinolinic acid (QA). Eventually, QA, a tryptophan metabolite, induces neurotoxicity as an agonist of the N-methyl-d -aspartate (NMDA) receptor, while KynA protects the brain from neurotoxicity as an antagonist of the NMDA receptor. In normal situations, KynA is usually produced because astrocytes have an inadequate reserve of enzymes that convert kynurenine to QA, but during local injuries or inflammation, microglia and macrophage infiltration facilitate QA production and ultimately induce neurotoxicity.Citation35,Citation36
Figure 2 Tryptophan-breakdown metabolic pathway in immunochallenge.
Abbreviations: NMDA R, N-methyl-d-aspartate receptor.
Second, the HPA axis is associated with depression. Elevated HPA-axis activity is intimately related to stress, as well as the pathophysiology of depression. Animal studies have reported that CRH injection induces such behaviors as depression and anxiety, sleep disturbance, dietary problems, and reduced activity.Citation37 Cytokines increase HPA-axis activity by increasing mRNA and the protein of CRH. Moreover, they inhibit the normal negative feedback system of the HPA axis by inducing resistance of corticosteroid receptors in some areas of the brain, such as the hypothalamus and pituitary gland. It has been suggested that these mechanisms through which cytokines affect the HPA axis contribute to the onset of depression.Citation38
Third, cytokines may induce depression by altering local brain activity. Neuroimaging findings of patients with depression have shown reduced basal activity in the frontal lobe, temporal lobe, and insula and increased activity in the cerebellum, subcortical structure, and limbic system.Citation39,Citation40 Of these, the dorsal part of the anterior cingulate cortex (dACC) is an important area that enables individuals to detect physical or social risk and minimize harm by increasing concentration to cope with such risks. Elevated dACC activity increases the risk of affective and anxiety disorders, and it has been confirmed that an IFNα injection increases local blood flow to the dACC on functional magnetic resonance imaging (MRI).Citation41 Furthermore, a study using 18F positron-emission tomography (PET) reported that IFNα injection affected the activity of the prefrontal cortex and basal ganglia, both of which are associated with fatigue and depressive symptoms.Citation42,Citation43 Animal studies have also demonstrated that cytokine injection inhibits memory function by affecting the hippocampus.Citation42
Neuroinflammation and neurogenesis in depression
Neurogenesis is the creation of new brain cells in adult brains. Considerable evidence supports the view that depression is accompanied by neurodegenerative processes and decreased neurogenesis.Citation43,Citation44 Chronic stress activates microglia in the brain, and cytokines released by microglia affect neurogenesis. A recent study revealed that neurogenesis may be suppressed or increased depending on the level of microglia activity.Citation45 This means that microglia have various functions, with some stimulating neurons and others suppressing them. Inflammation and cytokines generally directly suppress neurogenesis. Proinflammatory cytokines, such as TNFα and IFNα, suppress neurogenesis by regulating IL1.Citation46 In a recent study, inhibiting IL1β activity prevented neurogenesis suppression caused by stress.Citation47 Meanwhile, administration of drugs that inhibit inflammation leads to recovery or enhancement of neurogenesis.Citation48 These results support the view that chronic stress stimulates cytokine secretion in peripheral blood and microglia and that cytokines in turn affect neurogenesis.
The neurogenic theory of depression states that impaired neurogenesis is related to the etiology of depression and that successive antidepression therapy would strengthen neurogenesis.Citation26 Findings that support this theory suggest that stress suppresses neurogenesis, and is a risk factor for depression in vulnerable individuals, patients with depression show cognitive impairment and reduced hippocampal volume caused by weakened neurogenesis, antidepressants increase neurogenesis and prevent the inhibition of neurogenesis caused by stress, it takes approximately 3–4 weeks for most antidepressants to have an effect, which is equal to the time required for newly produced neurons to mature, and removing the hippocampus – the site for neurogenesis – in animal studies prevents the behavioral effects induced by antidepressant therapy.Citation26,Citation44 However, hippocampus-volume loss and neurogenesis suppression are not necessarily specific to depression, but are also evident in schizophrenia, dementia, addiction, and anxiety disorders.Citation49–Citation51 Furthermore, the specific role of neurogenesis in the regulation of depressive symptoms remains unclear. Therefore, some researchers argue that neurogenesis only contributes to cognitive dysfunction, which is common among all the diseases mentioned. However, most researchers agree that antidepressants increase neurogenesis, which is closely related to mechanisms of antidepressant action.Citation44 Although it may not be the main cause of depression or an essential factor contributing to the onset of depression, neurogenesis may be a necessary component of effective antidepression therapy. As such, increasing neurogenesis may be a promising strategy for treating depression.Citation43
Neuroinflammation, gonadal hormones, and gut–brain axis
Mounting evidence suggests that women are more susceptible to stress-induced depression than males.Citation52 Stress can disrupt activation of both the HPA and hypothalamic–pituitary–gonadal axes, both of which modulate neuroinflammatory pathways and brain regions involved in depression.Citation53,Citation54 Therefore, there is a hypothesis that stress differentially alters neuroinflammatory mechanisms associated with depression based on sex.Citation55,Citation56 Glucocorticoid, estradiol, and progesterone are also known modulators of neuroinflammation.Citation57 For example, ovariectomy inhibits LPS-induced brain microglial cytokines in mice, whereas estradiol therapy rescues this function.Citation58
Gut microbiota have bidirectional interactions with the CNS and immune system, and involve the immune (cytokines), endocrine (HPA axis), autonomic nervous system, and enteric nervous system forming the microbiota–gut–brain axis.Citation59 Neuroactive substances derived from the intestinal lumen can penetrate the gut mucosa. They are transported by blood, cross the blood–brain barrier, and influence the CNS.Citation60 It seems likely that gut microbiota play a role in depression through their ability to synthesize or mimic a range of host-signaling immunoactive molecules, such as monoamine and catecholamines.Citation61,Citation62
Clinical applications in neuroinflammatory depression
If inflammatory responses contribute to the development of depression, it can be anticipated that anti-inflammatory agents could be therapeutic in depression. Thus far, selective Cox2 inhibitors (eg, celecoxib), nonsteroidal anti-inflammatory drugs (NSAIDs), aspirin, tetracycline antibiotics (eg, minocycline), omega-3 fatty acids, and neurosteroids (eg, pregnenolone, allopregnanolone) have been used as supplementary treatments for depression.Citation63–Citation71 Recently, TNF inhibitors, such as etanercept, have been used as monotherapies for depression,Citation72 but they have also been used as supplementary therapies with conventional treatment in most studies.
Among these agents, that subject to the most intense research interest has been celecoxib. Small-scale randomized studies have outlined the positive effects of celecoxib on depression.Citation63 A meta-analysis reviewing 14 clinical trials reported that celecoxib decreased depressive symptoms without the risk of adverse reactions while considerably increasing response rate (OR 7.89, 95% CI 2.94–21.17) and remission rate (OR 6.59, 95% CI 2.24–19.42).Citation65 However, other NSAIDs had relatively unclear effects, though they were more effective than the placebo.Citation66 The effects of celecoxib seem to arise from the mechanism in which prostaglandin E2 synthesis is suppressed while the synthesis of 15-deoxy-ΔCitation12,Citation14-prostaglandin J2 and its receptor PPARγ is increased.Citation67
In fact, there have been studies showing that adding celecoxib, a Cox2 inhibitor, to conventional selective serotonin-reuptake inhibitor (SSRI) therapy generates better treatment response than SSRI monotherapy.Citation68,Citation69 Further, supplementary celecoxib therapy for depressive episodes in bipolar disorder has been found to induce earlier treatment responses; acetylsalicylic acid (aspirin) also augmented the effects of the SSRI.Citation70,Citation71 However, one report found that combining SSRI and NSAIDs undermined antidepressant effects: the effects of citalopram, which normally regulates TNFα and IFNγ in the frontal lobe, were inhibited by ibuprofen in rats.Citation73 Such laboratory results were also confirmed by data from the STAR*D study, where the proportion of depression-treatment failure was higher among people who took citalopram and AIDs together than among those who took only citalopram.Citation73,Citation74 However, these results have been rebutted by follow-up studies.Citation75 Such inconsistency in results should be addressed by establishing a standard for inflammation markers for depression and identifying the subtypes of depression for which AIDs have benefits.
Furthermore, ω3 fatty acids such as eicosapentaenoic acid and docosahexaenoic acid, can be used for rheumatoid arthritis, psoriasis, asthma, and inflammatory bowel disease due to their reduction of proinflammatory cytokines, and they have been effective as a supplementary treatment with antidepressants.Citation76 Angiotensin-receptor blockers, which are used to treat hypertension, have been found not only to be effective in cardiovascular diseases but also to have anti-inflammatory effects in the CNS.Citation77 Once their specific mechanism is revealed, they may be used to treat dementia and depression as well. There have been attempts to use IL1ra as a treatment for various mental illnesses, and more recently TNFα has been targeted as a disease-modifying treatment for bipolar disorder.Citation78 TNFα antagonists, such as adalimumab, etanercept, and infliximab, which have traditionally been used to treat rheumatic diseases, are currently undergoing clinical trials as treatments for depressive episodes in bipolar disorder. It is not yet clear how effective they will be.
A meta-analysis investigating 22 types of antidepressants found that IL-1β and IL-6 decreased in response to treatment and that these results were more evident in SSRI treatment.Citation79 Antidepressants are thought to regulate cytokines through the effects of cyclic adenosyl monophosphate, serotonin metabolism, the HPA axis, and neurogenesis.Citation80 Studies have also shed light on the anti-inflammatory effects of riluzole and ketamine, which are glutamatergic modulators. Inflammation increases microglial cell activity while inducing loss of astroglial cells, which will cause the release of glutamates and upregulated NMDA receptors.Citation81 During this process, riluzole and ketamine prevent neurotoxicity and reduce inflammation by inhibiting glutamate secretion and NMDA receptors. In addition, based on suggestions that CRF receptor antagonists modulate behavioral and endocrine responses to stress, their potential therapeutic efficacy on depression is now being investigated.Citation82–Citation84 There are enough evidences to show that antidepressant treatment induces a measurable change in the serum level of cytokines ().Citation8,Citation16,Citation83–Citation89
Table 2 Potential biomarkers in peripheral blood for antidepressant-treatment outcomes
All in all, using anti-inflammatory agents as part of routine treatment for depression would be premature at this point, but selective use in patients for whom inflammation plays a significant role in the course of the disease and in those who are vulnerable to inflammation might have benefits. In such cases, proinflammatory cytokine-receptor inhibitors, antibodies for proinflammatory cytokines, and anti-inflammatory cytokines, as well as the conventional anti-inflammatory agents, may theoretically be used for treatment. In the future, identifying the subtypes of depression with increased vulnerability to inflammation and testing the effects of anti-inflammatory agents in these patient groups through clinical trials will yield more concrete conclusions.
Cerebrovascular disease and depression
Depression is a common complication of stroke.Citation90 About 20%–50% of all stroke patients experience depression in the first year after a stroke.Citation91 Studies have argued that depression is associated with cerebral infarction (CI) in particular areas, such as the frontal lobe of the left hemisphere and basal ganglia,Citation92,Citation93 but subsequent research has reported that the onset of depression is not associated with the site of CI.Citation94 In one study, investigators argued that the incidence of post-stroke depression varies according to time.Citation95 They suggested that depression develops with high incidence (25%–31%) within the first month after stroke, but that the incidence of depression declines (16%) about 1–2 years after a stroke. By year 3 after a stroke, they suggested, depression recurs in about 29% of stroke patients who initially suffered from depression. The authors argued that the risk for depression is high within the first month of stroke due to poor physical condition, aphagia, or living alone. Furthermore, 1–2 years after stroke, patients’ social relationships are weakened, and by year 3, cerebral atrophy develops, all of which have an important impact on the onset of depression.
A considerable proportion of patients with late-onset depression exhibit silent CI (SCI), which shows no neurologic signs.Citation96 One study defined cases showing hyperintense lesions greater than 5 mm in nonperiventricular regions as SCI. A total of 22 of 41 patients with late-onset depression had SCI and CNS side effects, such as delirium, akathisia, parkinsonism, and dyskinesia, more common with poorer treatment prognoses in this group of patients than in those without SCI.Citation97 In another study, SCI was observed in 23% of patients aged ≥65 years, and the radius of the lesions was >3 mm in 79% of these patients.Citation98 In a postmortem-pathology study, patients who developed late-onset depression had markedly increased cerebral atherosclerosis compared to the normal population.Citation99 Other studies have also found that WMH on MRI is markedly increased in patients who develop late-onset depression compared to the normal population, which confirms that depression is associated with SCI.Citation100 Cerebral WMH shown in these patients is associated with extracranial carotid disease, decreased cerebral blood flow, hypertension, diabetes, and heart disease. These findings suggest that cerebrovascular diseases may play an important role in depression.
Neurovascular depression and neurotransmitters
Changes in neurotransmitters that lead to ischemic lesions may be related to depression. Stroke patients with depression have lower 5-hydroxyindolacetic acid levels in their cerebrospinal fluid than those in undepressed stroke patients and normal controls.Citation101 In a study using PET, 5HT2-receptor (a serotonin receptor) binding was found to be elevated in the cortex of the temporal and parietal lobes by 16 months after a left-hemisphere stroke, which could represent receptor upregulation caused by low serotonin levels.Citation102 In an animal study, norepinephrine levels decreased in the cortex and hippocampus and increased in the striatum and midbrain after ventrolateral ischemic lesion.Citation103 Some have hypothesized that lesions in the frontal lobe and head of the caudate nucleus may lead to depression, due to damage to the monoamine pathway.Citation104 An animal study observed elevated dopamineCitation103 and acetylcholineCitation105 levels as a result of ischemic lesions, but their roles in depression after a stroke remain unclear.Citation106 Another animal study confirmed that γ-aminobutyric acid (GABA) uptake was altered after an ischemic injury, and administering a GABA agonist after an ischemic injury had neuroprotective effects.Citation106 These results suggest that vascular injury of the brain may alter the neurotransmitter system and lead to the development of depression.
Pathophysiology of neurovascular depression
To understand the mechanism of vascular depression, one must consider the location of the lesion, clinical manifestations, age at onset of depression, presence of cognitive impairment, and nonbiological factors. Thus far, two theories have been most frequently cited in the mechanism of vascular depression. The first theory states that lesions that disrupt key brain pathways may be the direct cause of vascular depression. This theory was supported by study findings that lacunar infarcts in the left caudate head or left frontal pole in stroke patients induced depression.Citation107 However, this theory can only be applied to a small subset of patients who develop depression immediately after a stroke. The second theory suggests that an accumulation of small lesions eventually reaches a threshold that can lead to the onset of depression. In other words, this “threshold” theory hypothesizes the possibility of vulnerabilities caused by wide cerebrovascular disturbances, and it would be the most appropriate theory to explain depression in patients with latent neurologic lesions or those who have suffered a stroke. In clinical studies, neurocognitive function tests conducted on the elderly have revealed deficits in attention and executive function when the total area of WMH exceeded 10 cm2.Citation108 Such cognitive dysfunction was also evident in patients with late-onset depression with vascular risk factors, and these findings support the threshold theory as a mechanism of vascular depression.Citation109
Studies investigating the association between the region of white-matter injury and depressive symptoms have consistently found that white-matter injuries in the left frontal lobe are more clearly associated with depressive symptoms than white-matter damage in other areas.Citation110 Whereas age was significantly associated with deep WMH (DWMH) in the bilateral frontal lobes and left parietal lobe in patients with late-onset depression, age was significantly associated only with DWMH in the bilateral temporoparietal lobes in the study’s control group.Citation95 A clear conclusion has not been drawn on whether DWMH or periventricular WMH (PWMH) are more commonly associated with depression. Based on the vascular depression hypothesis, some studies have suggested a stronger association between depression and DWMH, which are more strongly associated with ischemic damage than periventricular lesions.Citation111,Citation112 Other researchers have found evidence of an association with both DWMH (frontoparietal) and PWMH and depression,Citation113 while others have found stronger associations between PWMH and depression.Citation114,Citation115 The discrepancies in these relationships may be the presence of cognitive impairment, which may be associated both with depressive symptoms and periventricular lesions. Periventricular lesions have been linked to cognitive impairment and ventricular enlargement in several studies of undepressed subjects.Citation116
Frontal subcortical circuits originate from the prefrontal cortex and pass through the caudate nucleus, globus pallidus, and dorsomedial thalamus to connect back to the prefrontal cortex. DWMH, a characteristic feature of vascular depression, is speculated to contribute to the onset of depression symptoms through mechanisms involving the injury of these circuits.Citation3 Although the cause of WMH is multifactorial, most WMH observed in patients with depression can be explained by cerebral ischemia. In a study that performed postmortem brain-tissue autopsy of 20 patients with late-onset depression and 20 controls, ischemia-induced DWMH findings were present in only a third of the control group, while all patients in the depression group had DWMH induced by ischemia.Citation117 WMH is not only associated with attention deficit and executive dysfunction but also observed in late-onset depression patients with vascular risk factors.Citation118 One meta-analysis reported that the OR for WMH was more than four times that of a late-onset-depression group than in an early-onset-depression group.Citation118
Diffusion-tensor imaging studies can assess the extent of white-matter injury by measuring fractional anisotropy (FA). These studies have found that elderly with depression show lower FA in the bilateral superior frontal gyri, anterior cingulate cortex, and left-middle frontal gyrus than control groups.Citation119 Furthermore, one report suggested that patients with late-onset depression had low FA in the right superior frontal gyrus, implying that minimal changes in the white matter of the frontal lobe are related to the onset of depression.Citation120
Some have argued that atherosclerosis increases the concentration of inflammatory markers in the blood caused by cerebral ischemia, which in turn stimulates the central monoamine system, inducing neurotoxicity in the monoamine system and ultimately causing depression.Citation121 In one report, postmortem autopsies of elderly with depression revealed that ICAM1 and VCAM1, which are detected following microvascular disease and ischemia, were significantly elevated in the dorsolateral prefrontal cortex in these individuals.Citation122
Clinical applications in neurovascular depression
Many studies have reported that vascular depression does not respond well to antidepressant therapy. WMH observed on MRI was associated with low response to antidepressant treatment.Citation123 Diffusion-tensor imaging revealed that low response to antidepressant treatment was associated with low FA in various frontal subcortical areas and the limbic system.Citation124 However, some studies also reported no association between vascular depression and the effects of antidepressant therapy.Citation125 Furthermore, a study that compared the effects of antidepressants by measuring cerebral blood flow through single-photon-emission computed tomography found that the initial effects of antidepressants increased with decreasing blood flow in the left prefrontal lobe area. This finding contradicted the existing hypothesis that response to antidepressants would be lower with lower blood flow, ie, when blood circulation is disturbed by ischemic disease.Citation126
Meanwhile, some studies have reported that vascular depression was also associated with poor progress and prognosis in addition to poor response to pharmacotherapy.Citation127,Citation128 In a long-term follow-up study, WMH was related to more chronic progression of depression, and an increase in WMH volume during follow-up was related to poor prognosis of late-onset depression.Citation94 MRI of patients with severe depression showed that the likelihood of developing vascular dementia was significantly higher during a 6- to 24-month follow-up when WMH was present.Citation127,Citation129,Citation130 Depressed patients with WMH have also been reported to exhibit more severe disabilities.Citation129
Elderly patients with vascular depression have shown a superior remission rate and response to transcranial magnetic stimulation treatment over a placebo group.Citation130 Furthermore, augmenting antidepressants with calcium-channel blockers for treating vascular depression was effective in reducing depressive symptoms and lowering recurrence rates.Citation131 Problem-solving therapy was more effective than supportive therapy for achieving remission in depression with executive dysfunction, and the former was also associated with fewer residual symptoms or functional disturbances.Citation132
In animal studies, haloperidol, an antagonist of dopamine or σ1-receptors, prazosin, an antagonist of α1-adrenergic receptors, clonidine, an agonist of α2-adrenergic receptors, diazepam, an agonist of GABA, and phenytoin, a voltage-dependent blocker of voltage-gated sodium channels, inhibited recovery of motor function after ischemic injury.Citation133–Citation137 Meanwhile, amphetamine, an indirect adrenergic agonist, bromocriptine, an agonist of dopamine receptors, and yohimbine and idazoxan, antagonists of α2-adrenergic receptors, facilitated recovery from an ischemic injury.Citation133,Citation134 In a study examining pharmacotherapies for poststroke depression, trazodone, nortriptyline, amphetamine, methylphenidate, and selective SSRIs were found to be effective.Citation135,Citation136 Further research is needed to examine the effects of each antidepressant on the recovery of neurologic deficits in poststroke depression. These studies could shed light on the most appropriate antidepressants for preventing and treating vascular depression.Citation132–Citation135
Effective treatment for hypertension and hyperlipidemia lowers cerebrovascular diseases and the subsequent mortality rate.Citation137 Warfarin and aspirin lowered the risk of stroke in patients with atrial fibrillation. Ticlopidine, aspirin, and dipyridamole reduced the recurrence of stroke in patients who had suffered ischemic stroke.Citation138,Citation139 Whether antihypertensive drugs, antihyperlipidemic drugs, and anticoagulants improve the outcomes of depression remains controversial. One study found that using nimodipine, a calcium-channel blocker, with antidepressants for patients with vascular depression improved depression more quickly with lower recurrence and a higher complete remission rate.Citation140 Other researchers have suggested that antihypertensive drugs themselves should be used with caution, because they increase the incidence of depression, and argued that vascular depression was no exception.Citation141 Incidence of depression with β-blockers is reportedly higher than with calcium antagonists.Citation142 In one study, verapamil showed a significant improvement in depressive symptoms, but atenolol did not.Citation143
Conclusion
Although depression has generally been explained thus far with the monoamine theory, it is far more multifactorial, and medications that correct the disease pathway have still not been developed. In this context, an understanding of neuroinflammation and neurovascular dysfunction enables a more comprehensive approach to depression.
Inflammation is in a sense a type of allostatic load involving the immune, endocrine, and nervous systems that induces changes in cytokines, the HPA axis, and neurotransmitters. That is, inflammation is involved in the pathophysiology of depression by increasing proinflammatory cytokines, activating the HPA axis, and increasing glucocorticoid resistance, as well as affecting serotonin–norepinephrine–dopamine synthesis and metabolism, neuronal apoptosis, neurogenesis, and neuroplasticity. Therefore, there are continued research efforts to explore neuroinflammation indicators that can be used as depression markers and to investigate the effects of anti-inflammatory medications on depression. However, it is very difficult to establish a consistent indicator amid complex interactions among numerous factors in a tightly knit network and the presence of countless confounding factors. Therefore, it is important to identify the genetic, physiological, and epidemiological characteristics of specific populations vulnerable to inflammatory responses and identify the relevant subtype of depression. Although neuroinflammation cannot yet be deemed a finding specific to depression, it does account for a considerable part of the pathophysiology of depression, and it may be an important factor in certain populations. Moreover, an understanding of neuroinflammatory mechanisms may yield novel depression treatments, suggesting the need for continued research.
Vascular depression may be particularly useful in studying the mechanism of depression. Depending on the site of brain vascular injury, depression can be aggravated, unaltered, or even prevented. Advances in brain imaging, electrophysiology, and chronobiology would enable quantitative measurements of brain lesions, as well as systematic research, such as studies investigating functional changes related to vascular injuries of particular brain areas. The vascular depression theory enables novel therapeutic approaches while laying the foundation for pharmacological studies. Aggressive pharmacotherapy for vascular diseases or vascular risk factors may affect the recovery and prognosis of patients with vascular depression. However, the efficacy of psychotropic medications on vascular depression has not been firmly established, necessitating further research. Investigating depression as an inflammatory and vascular disease will expand our understanding of the relationship between the body and mind and open a new chapter in psychiatry.
Acknowledgments
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, South Korea (HC15C1405).
Disclosure
The authors report no conflicts of interest in this work.
References
- KelleyKWBluthéRMDantzerRCytokine-induced sickness behaviorBrain Behav Immun200317S112S11812615196
- AizensteinHJBaskysABoldriniMVascular depression consensus report: a critical updateBMC Med20161416127806704
- AlexopoulosGSMeyersBSYoungRCCampbellSSilbersweigDCharlsonM‘Vascular depression’ hypothesisArch Gen Psychiatry1997549159229337771
- SneedJRCulang-ReinliebMEThe vascular depression hypothesis: an updateAm J Geriatr psychiatry2011199910321328801
- AnismanHMeraliZCytokines, stress and depressive illness: brainimmune interactionsAnn Med20033521112693607
- RaisonCLCapuronLMillerAHCytokines sing the blues: inflammation and the pathogenesis of depressionTrends Immunol200627243116316783
- MillerAHMaleticVRaisonCLInflammation and its discontents: the role of cytokines in the pathophysiology of major depressionBiol Psychiatry20096573274119150053
- LanquillonSKriegJCBening-Abu-ShachUVedderHCytokine production and treatment response in major depressive disorderNeuropsychopharmacology20002237037910700656
- HowrenMBLamkinDMSulsJAssociations of depression with C-reactive protein, IL-1, and IL-6: a meta-analysisPsychosom Med20097117118619188531
- DowlatiYHerrmannNSwardfagerWA meta-analysis of cytokines in major depressionBiol Psychiatry20106744645720015486
- AlesciSMartinezPEKelkarSMajor depression is associated with significant diurnal elevations in plasma interleukin-6 levels, a shift of its circadian rhythm, and loss of physiological complexity in its secretion: clinical implicationsJ Clin Endocrinol Metab2005902522253015705924
- YangKXieGZhangZLevels of serum interleukin (IL)-6, IL-1β, tumour necrosis factor-α and leptin and their correlation in depressionAust N Z J Psychiatry20074126627317464708
- SuSMillerAHSniederHCommon genetic contributions to depressive symptoms and inflammatory markers in middle-aged men: the Twins Heart studyPsychosom Med20097115215819073752
- ClericiMArosioBMundoECytokine polymorphisms in the pathophysiology of mood disordersCNS Spectr20091441942519890236
- WongMLDongCMaestre-MesaJLicinioJPolymorphisms in inflammation-related genes are associated with susceptibility to major depression and antidepressant responseMol Psychiatry20081380081218504423
- TuğluCKaraSHCaliyurtOVardarEAbayEIncreased serum tumor necrosis factor-alpha levels and treatment response in major depressive disorderPsychopharmacology200317042943312955291
- ChrousosGPStressors, stress, and neuroendocrine integration of the adaptive response: the 1997 Hans Selye Memorial LectureAnn N Y Acad Sci19988513113359668623
- WangXWuHMillerAHInterleukin 1α (IL-1α) induced activation of p38 mitogen-activated protein kinase inhibits glucocorticoid receptor functionMol Psychiatry20049657514699442
- PaceTWHuFMillerAHCytokine-effects on glucocorticoid receptor function: relevance to glucocorticoid resistance and the pathophysiology and treatment of major depressionBrain Behav Immun20072191917070667
- SongCMeraliZAnismanHVariations of nucleus accumbens dopamine and serotonin following systemic interleukin-1, interleukin-2 or interleukin-6 treatmentNeuroscience19998882383610363820
- PaceTWMletzkoTCAlagbeOIncreased stress-induced inflammatory responses in male patients with major depression and increased early life stressAm J Psychiatry20061631630163316946190
- FrankMGBarattaMVSprungerDBWatkinsLRMaierSFMicroglia serve as a neuroimmune substrate for stress-induced potentiation of CNS pro-inflammatory cytokine responsesBrain Behav Immun200721475916647243
- BarrientosRMSprungerDBCampeauSWatkinsLRRudyJWMaierSFBDNF mRNA expression in rat hippocampus following contextual learning is blocked by intrahippocampal IL-1β administrationJ Neuroimmunol200415511912615342202
- JeonSWKimYKInflammation-induced depression: Its pathophysiology and therapeutic implicationsJ Neuroimmunol2017313929829153615
- JeonSWKimYKNeuroinflammation and cytokine abnormality in major depression: cause or consequence in that illness?World J Psychiatry2016628329327679767
- KimYKNaKSMyintAMLeonardBEThe role of pro-inflammatory cytokines in neuroinflammation, neurogenesis and the neuroendocrine system in major depressionProg Neuropsychopharmacol Biol Psychiatry20166427728426111720
- JunTYPaeCUHoonHPossible association between –G308A tumour necrosis factor-α gene polymorphism and major depressive disorder in the Korean populationPsychiatr Genet20031317918112960751
- FertuzinhosSMOliveiraJRNishimuraALAnalysis of IL-1α, IL-1β, and IL-1RA [correction of IL-RA] polymorphisms in dysthy-miaJ Mol Neurosci20042225125614997019
- AdinolfiLENevolaRRinaldiLRomanoCGiordanoMChronic hepatitis C virus infection and depressionClin Liver Dis20172151753428689590
- PollakYYirmiyaRCytokine-induced changes in mood and behaviour: implications for ‘depression due to a general medical condition’, immunotherapy and antidepressive treatmentInt J Neuropsychophar-macol20025389399
- YirmiyaRWeidenfeldJPollakYCytokines, “depression due to a general medical condition”, and antidepressant drugsAdv Exp Med Biol199946128331610442179
- DantzerRAubertABluthéRMMechanisms of the behavioural effects of cytokinesAdv Exp Med Biol19994618310510442169
- al-HuthailYRNeuropsychiatric side-effects of interferon alfa therapy for hepatitis C and their management: a reviewSaudi J Gastroenterol200612596719858587
- KrausMRSchäferAScheurlenMParoxetine for the prevention of depression induced by interferon alfaN Engl J Med2001345375376
- SavitzJDrevetsWCSmithCMPutative neuroprotective and neurotoxic kynurenine pathway metabolites are associated with hippocampal and amygdalar volumes in subjects with major depressive disorderNeuropsychopharmacology20154046347125074636
- RéusGZJansenKTitusSCarvalhoAFGabbayVQuevedoJKynurenine pathway dysfunction in the pathophysiology and treatment of depression: evidences [sic] from animal and human studiesJ Psychiatr Res20156831632826028548
- HolsboerFCorticotropin-releasing hormone modulators and depressionCurr Opin Investig Drugs200344650
- de SouzaEBCorticotropin-releasing factor receptors: physiology, pharmacology, biochemistry and role in central nervous system and immune disordersPsychoneuroendocrinology1995207898198834089
- Yurgelun-ToddDASavaSDahlgrenMKMood disordersNeuroimaging Clin N Am20071751152117983967
- GongQHeYDepression, neuroimaging and connectomics: a selective overviewBiol Psychiatry20157722323525444171
- PaulusMPFeinsteinJSSimmonsASteinMBAnterior cingulate activation in high trait anxious subjects is related to altered error processing during decision makingBiol Psychiatry2004551179118715184037
- CapuronLRavaudADantzerRTiming and specificity of the cognitive changes induced by interleukin-2 and interferon-α treatments in cancer patientsPsychosom Med20016337638611382265
- EischAJPetrikDDepression and hippocampal neurogenesis: a road to remission?Science2012338727523042885
- MaharIBambicoFRMechawarNNobregaJNStress, serotonin, and hippocampal neurogenesis in relation to depression and antidepressant effectsNeurosci Biobehav Rev20143817319224300695
- EkdahlCTKokaiaZLindvallOBrain inflammation and adult neurogenesis: the dual role of microgliaNeuroscience20091581021102918662748
- KanekoNKudoKMabuchiTSuppression of cell proliferation by interferon-alpha through interleukin-1 production in adult rat dentate gyrusNeuropsychopharmacology2006312619262616823390
- KooJWDumanRSIL-1β is an essential mediator of the antineurogenic and anhedonic effects of stressProc Natl Acad Sci U S A200810575175618178625
- JeonSWKimYKMolecular neurobiology and promising new treatment in depressionInt J Mol Sci20161738126999106
- KempermannGKrebsJFabelKThe contribution of failing adult hippocampal neurogenesis to psychiatric disordersCurr Opin Psychiatry20082129029518382230
- RevestJMDupretDKoehlMAdult hippocampal neurogenesis is involved in anxiety-related behaviorsMol Psychiatry20091495996719255582
- ThompsonABoekhoornKvan DamAMChanges in adult neurogenesis in neurodegenerative diseases: cause or consequence?Genes Brain Behav20087284218184368
- SolomonMBHermanJPSex differences in psychopathology: of gonads, adrenals and mental illnessPhysiol Behav20099725025819275906
- McCormickCMMathewsIZHPA function in adolescence: role of sex hormones in its regulation and the enduring consequences of exposure to stressorsPharmacol Biochem Behav20078622023316901532
- NaninckEFLucassenPJBakkerJSex differences in adolescent depression: do sex hormones determine vulnerability?J Neuroendocrinol20112338339221418338
- BaleTLNeuroendocrine and immune influences on the CNS: it’s a matter of sexNeuron200964131619840541
- HanamsagarRBilboSDSex differences in neurodevelopmental and neurodegenerative disorders: focus on microglial function and neuroinflammation during developmentJ Steroid Biochem Mol2016160127133
- KippMBeyerCImpact of sex steroids on neuroinflammatory processes and experimental multiple sclerosisFront Neuroendocrinol20093018820019393685
- SoucyGBoivinGLabrieFRivestSEstradiol is required for a proper immune response to bacterial and viral pathogens in the female brainJ Immunol20051746391639815879140
- MayerEAGut feelings: the emerging biology of gut-brain communicationNat Rev Neurosci20111245346621750565
- TheoharidesTCWeinkaufCContiPBrain cytokines and neuropsychiatric disordersJ Clin Psychopharmacol20042457758115538117
- KoopmanMel AidySDepressed gut? The microbiota-diet-inflammation trialogue in depressionCurr Opin Psychiatry20173036937728654462
- PetraAIPanagiotidouSHatziagelakiEStewartJMContiPTheoharidesTCGut-microbiota-brain axis and its effect on neuropsychiatric disorders with suspected immune dysregulationClin Ther20153798499526046241
- KrebsMLeopoldKHinzpeterASchaeferMNeuroprotective agents in schizophrenia and affective disordersExpert Opin Pharmacother2006783784816634707
- NajjarSPearlmanDMAlperKNajjarADevinskyONeuroinflammation and psychiatric illnessJ Neuroinflammation2013104323547920
- KöhlerOBenrosMENordentoftMEffect of anti-inflammatory treatment on depression, depressive symptoms, and adverse effects: a systematic review and meta-analysis of randomized clinical trialsJAMA Psychiatry2014711381139125322082
- EyreHAAirTProctorSBauneBTA critical review of the efficacy of non-steroidal anti-inflammatory drugs in depressionProg Neuropsychopharmacol Biol Psychiatry201557111625455584
- Garcia-BuenoBPerez-NievasBGLezaJCIs there a role for the nuclear receptor PPARγ in neuropsychiatric diseases?Int J Neuropsychopharmacol2010131411142920800014
- JohanssonDFalkAMarcusMMSvenssonTHCelecoxib enhances the effect of reboxetine and fluoxetine on cortical noradrenaline and serotonin output in the ratProg Neuropsychopharmacol Biol Psychiatry20123914314822691715
- MüllerNSchwarzMJDehningSThe cyclooxygenase-2 inhibitor celecoxib has therapeutic effects in major depression: results of a double-blind, randomized, placebo controlled, add-on pilot study to reboxetineMol Psychiatry20061168068416491133
- NeryFGMonkulESHatchJPCelecoxib as an adjunct in the treatment of depressive or mixed episodes of bipolar disorder: a double-blind, randomized, placebo-controlled studyHum Psychopharmacol200823879418172906
- WangYYangFLiuYFGaoFJiangWAcetylsalicylic acid as an augmentation agent in fluoxetine treatment resistant depressive ratsNeurosci Lett2011499747921640159
- SchmidtFMKirkbyKCHimmerichHThe TNF-alpha inhibitor etanercept as monotherapy in treatment-resistant depression: report of two casesPsychiatr Danub20142628829025191779
- Warner-SchmidtJLVanoverKEChenEYMarshallJJGreengardPAntidepressant effects of selective serotonin reuptake inhibitors (SSRIs) are attenuated by antiinflammatory drugs in mice and humansProc Natl Acad Sci U S A20111089262926721518864
- HowlandRHSequenced treatment alternatives to relieve depression (STAR*D): part 2 – study outcomesJ Psychosoc Nurs Ment Health Serv2008462124
- UherRCarverSPowerRANon-steroidal anti-inflammatory drugs and efficacy of antidepressants in major depressive disorderPsychol Med2012422027203522391106
- LinPYMischoulonDFreemanMPAre omega-3 fatty acids antidepressants or just mood-improving agents? The effect depends upon diagnosis, supplement preparation, and severity of depressionMol Psychiatry2012171161116722824812
- DaviesNMKehoePGBen-ShlomoYAssociations of antihypertensive treatments with Alzheimer’s disease, vascular dementia, and other dementiasJ Alzheimers Dis20112669970821709373
- BrietzkeEKapczinskiFTNF-α as a molecular target in bipolar disorderProg Neuropsychopharmacol Biol Psychiatry2008321355136118316149
- HannestadJDellaGioiaNBlochMThe effect of antidepressant medication treatment on serum levels of inflammatory cytokines: a meta-analysisNeuropsychopharmacology2011362452245921796103
- JanssenDGCaniatoRNVersterJCBauneBTA psychoneuroimmunological review on cytokines involved in antidepressant treatment responseHum Psychopharmacol20102520121520373471
- McNallyLBhagwagarZHannestadJInflammation, glutamate, and glia in depression: a literature reviewCNS Spectr20081350151018567974
- ZoumakisEChrousosGPCorticotropin-releasing hormone receptor antagonists: an updateEndocr Dev201017364319955754
- UherRGenes, environment, and individual differences in responding to treatment for depressionHarv Rev Psychiatry20111910912421631158
- MaesMBosmansEde JonghRIncreased serum IL-6 and IL-1 receptor antagonist concentrations in major depression and treatment resistant depressionCytokine199798538589367546
- MaesMThe immunoregulatory effects of antidepressantsHum Psychopharmacol2001169510312404604
- CattaneoAGennarelliMUherRCandidate genes expression profile associated with antidepressants response in the GENDEP study: differentiating between baseline ‘predictors’ and longitudinal ‘targets’Neuropsychopharmacology20133837738522990943
- PowellTRSchalkwykLCHeffernanALTumor necrosis factor and its targets in the inflammatory cytokine pathway are identified as putative transcriptomic biomarkers for escitalopram responseEur Neuropsychopharmacol2013231105111423142150
- TsaoCWLinYSChenCCCytokines and serotonin transporter in patients with major depressionProg Neuropsychopharmacol Biol Psychiatry20063089990516616982
- EllerTVasarVShlikJPro-inflammatory cytokines and treatment response to escitalopram in major depressive disorderProg Neuropsychopharmacol Biol Psychiatry20083244545017976882
- RobinsonRGJorgeREPost-stroke depression: a reviewAm J Psychiatry201617322123126684921
- HouseADennisMMogridgeLWarlowCHawtonKJonesLMood disorders in the year after first strokeBr J Psychiatry199115883922015456
- RobinsonRGPriceTRPost-stroke depressive disorders: a follow-up study of 103 patientsStroke1982136356417123596
- RobinsonRGKubosKLStarrLBRaoKPriceTRMood disorders in stroke patients: importance of location of lesionBrain198410781936697163
- CarsonAJMacHaleSAllenKDepression after stroke and lesion location: a systematic reviewLancet200035612212610963248
- AströmMAdolfssonRAsplundKMajor depression in stroke patients: a 3-year longitudinal studyStroke1993249769828322398
- FengCFangMLiuXYThe neurobiological pathogenesis of post-stroke depressionScientificWorldJournal2014201452134924744682
- FujikawaTYokotaNMuraokaMYamawakiSResponse of patients with major depression and silent cerebral infarction to antidepressant drug therapy, with emphasis on central nervous system adverse reactionsStroke199627204020428898812
- BryanRNManolioTASchertzLDA method for using MR to evaluate the effects of cardiovascular disease on the brain: the cardiovascular health studyAJNR Am J Neuroradiol199415162516337847205
- ThomasAJFerrierINKalariaRNPerryRHBrownAO’BrienJTA neuropathological study of vascular factors in late-life depressionJ Neurol Neurosurg Psychiatry200170838711118253
- KhalafAEdelmanKTudorascuDAndreescuCReynoldsCFAizensteinHWhite matter hyperintensity accumulation during treatment of late-life depressionNeuropsychopharmacology2015403027303526058663
- BryerJBStarksteinSEVotypkaVParikhRMPriceTRRobinsonRGReduction of CSF monoamine metabolites in poststroke depression: a preliminary reportJ Neuropsychiatry Clin Neurosci199244404421384852
- MaybergHSRobinsonRGWongDFPET imaging of cortical S2 serotonin receptors after stroke: lateralized changes and relationship to depressionAm J Psychiatry19881459379433394877
- FinklesteinSCampbellABaldessariniRJMoyaKLHaberSNLate changes in cerebral monoamine metabolism following focal ventrolateral cerebrocortical lesions in ratsBrain Res19853442052102412650
- SantosMKövariEGoldGThe neuroanatomical model of post-stroke depression: towards a change of focus?J Neurol Sci200928315816219264329
- BertrandNIshiiHBeleyASpatzMBiphasic striatal acetylcholine release during and after transient cerebral ischemia in gerbilsJ Cereb Blood Flow Metab1993137897958360285
- KurodaHBaskinDSMatsuiTLohHHHosobuchiYLeeNMEffects of dynorphin1–13 on opiate binding and dopamine and GABA uptake in stroked cat brainBrain Res198637968742874866
- FolsteinMFMaibergerRMcHughPRMood disorder as a specific complication of strokeJ Neurol Neurosurg Psychiatry19774010181020591971
- BooneKBMillerBLLesserIMNeuropsychological correlates of white-matter lesions in healthy elderly subjects: a threshold effectArch Neurol1992495495541580819
- YangSHuaPShangXA significant risk factor for poststroke depression: the depression-related subnetworkJ Psychiatry Neurosci20154025926825871495
- FirbankMJLloydAJFerrierNO’BrienJTA volumetric study of MRI signal hyperintensities in late-life depressionAm J Geriatr Psychiatry20041260661215545328
- de GrootJCde LeeuwFEOudkerkMHofmanAJollesJBretelerMMCerebral white matter lesions and depressive symptoms in elderly adultsArch Gen Psychiatry2000571071107611074873
- KrishnanMSO’BrienJTFirbankMJRelationship between periventricular and deep white matter lesions and depressive symptoms in older people: the LADIS studyInt J Geriatr Psychiatry20062198398916955428
- JormAFAnsteyKJChristensenHMRI hyperintensities and depressive symptoms in a community sample of individuals 60–64 years oldAm J Psychiatry200516269970515800141
- IidakaTNakajimaTKawamotoKSignal hyperintensities on brain magnetic resonance imaging in elderly depressed patientsEur Neurol1996362932998864711
- BaldwinRJeffriesSJacksonATreatment response in late-onset depression: relationship to neuropsychological, neuroradiological and vascular risk factorsPsychol Med20043412513614971633
- BarberRGholkarAScheltensPBallardCMcKeithIGO’BrienJTMRI volumetric correlates of white matter lesions in dementia with Lewy bodies and Alzheimer’s diseaseInt J Geriatr Psychiatry20001591191611044873
- ThomasAJO’BrienJTDavisSIschemic basis for deep white matter hyperintensities in major depression: a neuropathological studyArch Gen Psychiatry20025978579212215077
- HerrmannLLle MasurierMEbmeierKPWhite matter hyperintensities in late life depression: a systematic reviewJ Neurol Neurosurg Psychiatry20087961962417717021
- BaeJNMacFallJRKrishnanKRPayneMESteffensDCTaylorWDDorsolateral prefrontal cortex and anterior cingulate cortex white matter alterations in late-life depressionBiol Psychiatry2006601356136316876144
- TaylorWDMacFallJRPayneMELate-life depression and microstructural abnormalities in dorsolateral prefrontal cortex white matterAm J Psychiatry20041611293129615229065
- ConnorTJLeonardBEDepression, stress and immunological activation: the role of cytokines in depressive disordersLife Sci1998625836069472719
- DimopoulosNPiperiCSaloniciotiAElevation of plasma concentration of adhesion molecules in late-life depressionInt J Geriatr200621965971
- HickieIScottEMitchellPWilhelmKAustinMPBennettBSubcortical hyperintensities on magnetic resonance imaging: clinical correlates and prognostic significance in patients with severe depressionBiol Psychiatry1995371511607727623
- AlexopoulosGSMurphyCFGunning-DixonFMMicrostructural white matter abnormalities and remission of geriatric depressionAm J Psychiatry200816523824418172016
- KrishnanKRHaysJCGeorgeLKBlazerDGSix-month outcomes for MRI-related vascular depressionDepress Anxiety199881421469871815
- NavarroVGastóCLomeñaFPrognostic value of frontal functional neuroimaging in late-onset severe major depressionBr J Psychiatry200418430631115056574
- HickieIScottEWilhelmKBrodatyHSubcortical hyperintensities on magnetic resonance imaging in patients with severe depression: a longitudinal evaluationBiol Psychiatry1997423673749276077
- O’BrienJAmesDChiuESchweitzerIDesmondPTressBSevere deep white matter lesions and outcome in elderly patients with major depressive disorder: follow up studyBMJ19983179829849765166
- SteffensDCBosworthHBProvenzaleJMMacFallJRSubcortical white matter lesions and functional impairment in geriatric depressionDepress Anxiety200215232811816049
- JorgeREMoserDJAcionLRobinsonRTreatment of vascular depression using repetitive transcranial magnetic stimulationArch Gen Psychiatry20086526827618316673
- TaraganoFEBagnattiPAllegriRFA double-blind, randomized clinical trial to assess the augmentation with nimodipine of antidepressant therapy in the treatment of “vascular depression”Int Psychogeriatr20051748749816252380
- AlexopoulosGSRauePJKiossesDNProblem-solving therapy and supportive therapy in older adults with major depression and executive dysfunction: effect on disabilityArch Gen Psychiatry201168334121199963
- GoldsteinLBBasic and clinical studies of pharmacologic effects on recovery from brain injuryJ Neural Transplant Plast199341751928018750
- GoldsteinLBCommon drugs may influence motor recovery after strokeNeurology1995458658717746398
- CholletFTardyJAlbucherJFFluoxetine for motor recovery after acute ischaemic stroke (FLAME): a randomised placebo-controlled trialLancet Neurol20111012313021216670
- RedingMJOrtoLAWinterSWFortunaIMDi PontePMcDowellFHAntidepressant therapy after stroke: a double-blind trialArch Neurol1986437637653729755
- PedeltyLGorelickPBManagement of hypertension and cerebrovascular disease in the elderlyAm J Med20081212331
- BellavanceAEfficacy of ticlopidine and aspirin for prevention of reversible cerebrovascular ischemic events: the Ticlopidine Aspirin Stroke StudyStroke199324145214578378945
- SiveniusJRiekkinenPJLaaksoMSmetsPLowenthalAEuropean Stroke Prevention Study (ESPS): antithrombotic therapy is also effective in the elderlyActa Neurol Scand1993871111148442393
- TaraganoFEAllegriRVicarioABagnattiPLyketsosCGA double blind, randomized clinical trial assessing the efficacy and safety of augmenting standard antidepressant therapy with nimodipine in the treatment of ‘vascular depression’Int J Geriatr Psychiatry20011625426011288158
- BeeversDGBeta-blockers for hypertension: time to call a haltJ Hum Hypertens1998128078109883700
- KoDTHebertPRCoffeyCSSedrakyanACurtisJPKrumholzHMβ-Blocker therapy and symptoms of depression, fatigue, and sexual dysfunctionJAMA200228835135712117400
- RiedLDTuethMJHandbergEKupferSPepineCJA study of antihypertensive drugs and depressive symptoms (SADD-Sx) in patients treated with a calcium antagonist versus an atenolol hypertension treatment strategy in the International Verapamil SR-Trandolapril Study (INVEST)Psychosom Med20056739840615911902
- JeonSWKimYKNeuroinflammation and cytokine abnormality in major depression: cause or consequence in that illness?World J Psychiatry20166284293