
Abstract
Rationale
Eosinophilic inflammation is related to the progression and outcomes of acute exacerbation of chronic obstructive pulmonary disease (AECOPD). Till now, few studies have focused on low EOS in AECOPD.
Objective
To reveal the clinical characteristics, therapeutic responses and prognosis of patients hospitalized of AECOPD with low EOS.
Methods
The electronic database of Zhongshan Hospital, Fudan University was used. Cohort 1 included 608 patients with hospitalized AECOPD. Study population 2 consisted of 166 patients with AECOPD admission at least twice. Impact of low EOS on NIMV treatment, length of hospital stays and 12-month AECOPD-related readmission were analyzed with multivariable logistic regression model. Thirty-five hospitalized AECOPD patients were prospectively recruited as cohort 3 to explore the association between EOS and other immune cells using Spearman correlation coefficient for ranked data.
Results
EOS level was suppressed on admission in AECOPD patients, and significantly improved after hospitalized treatment (P < 0.05). For inflammatory markers, leucocytes, neutrophils and lactate dehydrogenase levels were higher, while lymphocytes, monocytes and interleukin-6 levels were lower in the low-EOS group than those in the non-low EOS group (P < 0.05). Low EOS (EOS < 50 cells/μL) was an independent risk factor of NIMV use (OR = 1.86, 95% CI = 1.26 ~ 2.73). The EOS percentage was positively correlated with the T cell percentage (r = 0.46, P < 0.05) and negatively correlated with the natural killer cell percentage (r = −0.39, P < 0.05). The patients with low EOS had lower level of CD4+ T cell (P < 0.05) than that of patients with non-low EOS.
Conclusion
Low EOS might be a stable phenotype in patients with hospitalized AECOPD and could be used to inform NIMV management, hyperinflammatory state and impaired immunity situation.
Background
Chronic obstructive pulmonary disease (COPD) is characterized by airflow obstruction or impaired lung function. The prevalence of spirometry-defined COPD in China was 13.7% among people aged 40 years or older.Citation1 Though classically mediated by neutrophilic and Th1 cells,Citation2 different COPD inflammatory profiles have recently gained more interest.Citation3 Studies demonstrated that a higher blood eosinophil (EOS) count was associated with higher risk of developing COPD in individuals from general population.Citation4,Citation5 In patients with stable COPD, higher blood eosinophil count may predict increased risk of severe acute exacerbations of COPD (AECOPD). Severe AECOPD requiring hospitalization is associated with poorer outcomes, including accelerated lung function decliningCitation6 and significant higher risk of mortality.Citation7 Therefore, adequately phenotyping eosinophilic inflammation in COPD is worthwhile.
Previous studies mainly focused on high EOS in AECOPD by different cut-off values of 150 to 300 cells/μL.Citation8–10 The results supported that patients with elevated blood eosinophil counts were at higher risk of acute exacerbations.Citation11 COPD-related readmission rates were significantly greater at 30, 60, and 90 days and 12 months after discharge for patients with eosinophil counts >300 cells/μL (versus lesser) (OR range = 1.52–1.97).Citation12 It was also well established that patients with high eosinophilic exacerbations responded better to inhaled corticosteroids (ICS) therapy than patients with non-high eosinophilic exacerbations.Citation13 ICS combined with long-acting β2-agonists (LABA) is already recommended for AECOPD treatment if EOS ≥ 300 cells/μL.Citation14 However, this treatable trait presented significant variability throughout the course of COPD, making it difficult to be a reliable predictor.Citation15 It was demonstrated that AECOPD patients with eosinophil counts <50 cells/μL were more strongly associated with infection, longer median hospital stay and shorter 12-month survival than patients with eosinophil counts >150 cells/μL.Citation8 However, a study from Utah suggested that a blood eosinophil count ≤70 cells/µL identified a patient group that was unlikely to require readmission.Citation12 Given that high EOS acts in AECOPD, low EOS might link to certain important clinical evidence. Studies on the clinical characteristics of patients with low EOS and outcomes of hospitalized AECOPD were scarce and need to be further investigated.
Thus, the objective of this study was to investigate whether AECOPD patients with low EOS had special clinical characteristics and to explore the associations of low EOS with inflammation and immunity.
Materials and Methods
Study Population and Design
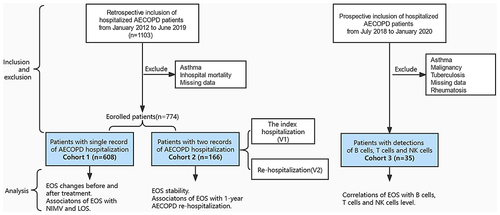
The electronic database of Zhongshan Hospital, Fudan University was used for this study. From January 2012 to June 2019, there were altogether 1103 cases with AECOPD diagnosisCitation16 as shown in . Three hundred and twenty-nine patients were excluded as they were diagnosed with asthma or had incomplete baseline characteristics. Finally, 608 patients with hospitalized AECOPD were included as study population 1. Besides, 166 patients with AECOPD admission at least twice were included as Study population 2. At the same time, 35 patients were prospectively recruited during consecutive hospital admission for AECOPD from July 2018 to January 2020 and were included as Study population 3. The Ethics Committee of Zhongshan Hospital, Fudan University approved the protocol (B2021-818R) and this study was conducted in accordance with the Declaration of Helsinki. As the data were anonymized, the institutional Ethics Committee gave their approval for the study with no need for informed consent from participants.
Figure 1 Cohort diagram: Study population.
Data Collection
Patients’ characteristics and comorbid diseases were collected from the hospital database. Hemogram parameters, C reactive protein (CRP) levels, biochemistry values on admission and discharge date, noninvasive ventilation (NIMV) usage, length of hospitalization (days), and readmissions were exported for the analysis. TNF-α, IL-2R, IL-6, IL-8 and CRP in serum were measured using multiplex bead sets from a variety of vendors (R&D Systems, Minneapolis, MN) according to the manufacturer’s instructions. The percentages of B cells, T cells, cluster of differentiation (CD) 4, CD8 positive cells and natural killer (NK) cells were determined on a Coulter EPICS Profile flow cytometer (Coulter Cytometry, Hialeah, FL, USA) at Zhongshan Hospital, Fudan University. The normal range of the percentage of eosinophils in leucocytes used in Zhongshan hospital, Fudan University is 0.4–2.0%.
Eosinophil Profiling and Outcomes
As for primary endpoints, treatment with NIMV and length of hospital stay were selected. Further analyses described long-term outcome of AECOPD (12-month AECOPD-related readmission within our hospital) according to blood EOS count strata (50 cells/μLCitation8 and 0.4% of leucocytes).
Statistical Analyses
The study variables were compared between the low EOS and non-low EOS patients using the chi-2 test for categorical variables, and the t-test or the Wilcoxon rank test for continuous variables. The change of eosinophil levels is described as the EOS value at discharge subtracted from that on admission. Concordance was defined as blood eosinophil values persistently lower than or persistently higher than 50 cells/μL or 0.4%, respectively. Discordance was defined when the blood eosinophil values varied between two AECOPD hospitalization. For binary outcomes, associations of eosinophilia with outcomes were estimated using logistic regression with stepwise selection (variables were considered if they reached statistical significance). All statistical analyses were performed by SPSS for Windows (Version 26.0, Chicago, IL, USA). All P values were two-sided and a difference was considered statistically significant at P < 0.05.
Results
Study Population
Baseline demographics and clinical characteristics, including EOS counts for all cohorts, are presented in Table S1. Study population 1 consisted of 80.9% men, with a median age (range) of 75 (68 to 82) years old. There were 215 subjects (35%) having diagnosis of concomitant pulmonary infection or pneumonia on admission and 251 subjects (41%) suffering from respiratory failure. For all subjects, either oral or systemic corticosteroids was administered in 49.5% patients and NIMV treatment was performed in 35.0% patients. The median (range) length of hospital stay was 10.5 days (7.5 to 15). Length of hospital stay equal or longer than 15 days was considered an extended stay.
The median (interquartile range) absolute peripheral eosinophil count and eosinophil count percentage of leucocytes was 35 cells/µL (0 to 150 cells/µL) and 0.4% (0.0 to 1.9), respectively. The low EOS phenotype defined as peripheral blood eosinophil count <0.4% of total leukocyte count occurred in 49.3% patients (n = 300). A peripheral blood eosinopenia less than 50 cells/µL occurred in 328 subjects (53.9%). There were no differences with respect to age, gender, complications, or comorbidities between subjects of low EOS and non-low EOS phenotype in all cohorts, except that more subjects with low EOS phenotype were admitted during winter than those with non-low EOS phenotype in cohort 1 (45.4% vs 30.7%, P<0.05) (, S2 and S3).
Table 1 Comparison of Clinical Characteristics Between AECOPD Patients with and without Low EOS in Cohort 1
Stability of the Low EOS in AECOPD
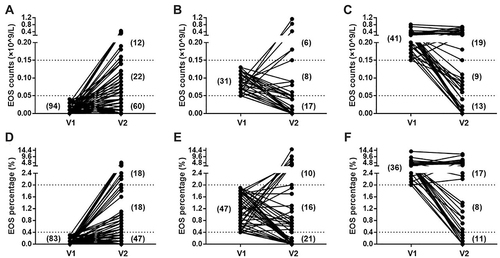
The median blood eosinophil level for all subjects was 20 (0–130) cells/μL on admission, which was 90 (20–180) cells/μL at discharge (). The median EOS percentage of leucocytes on admission was also lower compared with that after hospitalization treatment, ranging from 0.3% (0~1.7) to 1% (0.2~2.7) (). In the low EOS subgroup, the level of EOS at discharge was significantly higher than that on admission, which remained stable between two measurements in the non-low EOS subgroup ( and ). In patients with EOS values <50 cells/μL on the index date of hospitalized AECOPD, significantly higher proportion of patients were still in low EOS levels on the re-admission date for AECOPD compared with that of patients with EOS ≥ 50 cells/μL (63.8% vs 36.2%; P < 0.05) (; ). The same difference was seen when stratifying low eosinophil level according to EOS percentage of leucocytes <0.4% (56.6% vs 43.4%; P < 0.05) (; ). In patients without EOS values <50 cells/μL on the index date of hospitalized AECOPD, the levels of eosinophils on the second admission showed a greater discordance compared with that of the first admission ().
Table 2 Longitudinal Change in Blood Cell Counts by AECOPD Admission or Discharge in Study Population 1
Table 3 Stability and Variability of the Low EOS Between Two Hospitalizations, Stratified by EOS Values of 50 Cells/μL
Figure 2 Longitudinal change of the median percentage of eosinophils by AECOPD admission or discharge.
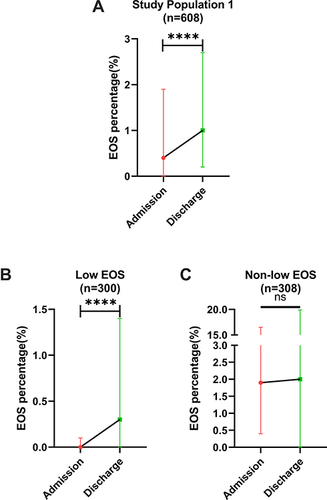
Figure 3 Stability of the low EOS between two visits in cohort 2, ascertained from two cut-points. Eosinophil blood cell count strata was based on absolute numbers (A–C) or on a percentage of leukocytes (D–F), respectively.
Association of Low EOS with Infection
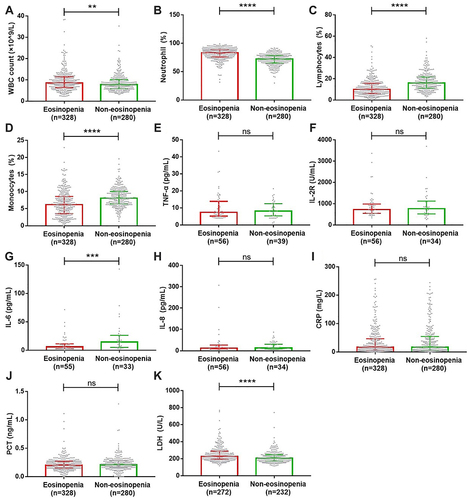
There was no difference with respect to the incidence of pulmonary infection between the low EOS and non-low EOS group (). As shown in , the white blood cell (WBC) count, the neutrophil percentage of leucocytes and lactate dehydrogenase (LDH) concentration were significantly higher in patients with low EOS compared to those in patients with non-low EOS, whereas the lymphocyte and monocyte percentage of leucocytes and interleukin (IL)-6 concentration in the low EOS group were markedly lower compared with those in the non-low EOS group. Some other infectious parameters’ levels were not statistically different between the low EOS and non-low EOS group, including tumor necrosis factor (TNF)-α, IL-2 receptor, IL-8, CRP and procalcitonin (PCT).
Figure 4 Comparison of inflammatory biomarkers between patients with eosinopenia and without in cohort 1. The WBC count (A), the neutrophil percentage (B) and LDH concentration (K) were significantly higher in patients with eosinopenia compared to those in patients with non-eosinopenia, whereas the lymphocyte (C) and monocyte (D) percentage and IL-6 concentration (G) in eosinopenia group were markedly lower compared with those in the non-eosinopenia group. Some other infectious parameters’ levels were not statistically different between eosinopenia and non-eosinopenia group, including TNF-α (E), IL-2 receptor (F), IL-8 (H), CRP (I) and PCT (J).
Association of Low EOS with Outcomes of AECOPD
Patients with low EOS were more likely to be treated with NIMV than patients with non-low EOS (0.4%: 43.0% vs 27.3%; 50 cells/μL: 41.5% vs 27.5%; P < 0.001, ). In a logistic regression analysis adjusting for confounders (hypertension, respiratory failure, the lymphocyte percentage of leucocytes and the level of PCT), patients with EOS < 50 cells/µL were more likely to be treated with NIMV than those with non-low EOS (OR = 1.86, 95% CI = 1.26~2.73; ). However, no significant difference of length of hospital stay was observed between the low EOS and non-low EOS group (Table S4). In addition, patients with low EOS were prone to be re-admitted for AECOPD than patients with non-low EOS, although the difference was not statistically significant (0.4%: 55.6% vs 44.4%, P = 0.051; 50 cells/μL: 59.3% vs 40.7%, P = 0.350; Table S5). The low EOS phenotype was not included in the risk factors for twelve-month AECOPD-related readmission, which consisted of hospitalization in winter (OR = 2.45, 95% CI = 1.17~5.15), ICS administration (OR = 2.90, 95% CI = 1.42~5.94) and non NIMV treatment (NIMV treatment vs non NIMV treatment, OR = 0.49, 95% CI = 0.25~0.97) (Figure S1).
Table 4 Results from the Logistic Regression Model Showing NIMV Use for Low EOS Subgroups (<50 Cells/µL) Compared with the Reference Subgroup (≥50 Cells/µL) and Other Covariates (N = 608)
The Relationship Between EOS and Immune Cells
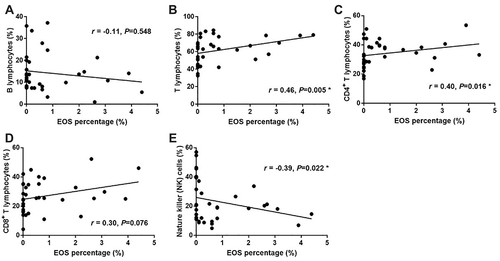
Total and CD4+ T cells percentage were both markedly less in the low EOS group than those in the non-low EOS group (54.0% vs 85.7% for total T cells; 22.5% vs 43.4% for CD4+ T cells; P < 0.05, ). However, differences of the percentage of B cells, CD8+ T cells percentage, CD4+/CD8+ ratio and NK cells account between the eosinopenia and the non-eosinopenia groups were not significant (P > 0.05). Stronger positive associations between total T cells, CD4+ T cells and the EOS percentage of leucocytes were observed in study population 3 (r = 0.46 for total T cells; r = 0.40 for CD4+ T cells, P < 0.05; ). Blood EOS percentage correlated negatively with NK cell percentage (r = −0.39, P < 0.05; ).
Figure 5 Comparison of different immune parameters between patients with eosinopenia and without. Total (B) and CD4+ T cells (C) percentage were both markedly less in the eosinopenia group than those in the non-eosinopenia group. Differences of the percentage of B cells (A), CD8+ T cells percentage (D), CD4+/CD8+ ratio (E) and NK cells account (F) between the eosinopenia and the non-eosinopenia groups were not significant.
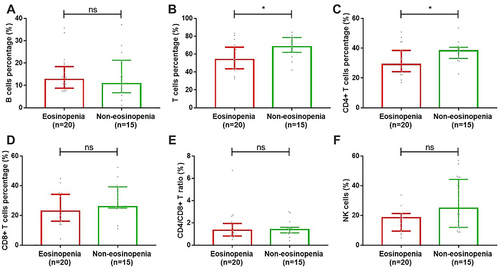
Figure 6 Correlation between EOS percentage (%) and different immune cells.
Discussion
There has been a growing appreciation for the importance of blood eosinophil levels as a biomarker of future exacerbation risk and responsiveness to ICS in COPD patients.Citation9,Citation17 This simple dichotomization of eosinophil counts as “high” or “not high” may overlook important clinical evidence linked to low eosinophil counts. A recent study showed that a blood eosinophil threshold of 70 cells/µL showed the most discriminatory power to predict 30-day all-cause readmission (highest AUC) compared with that of 300 cells/µL.Citation12 Howeverto date, there has been few data about the link of low eosinophil counts to the occurrence and prognosis of AECOPD. With an observational study design, we concluded that there existed low EOS phenotype and it was relatively stable between two hospitalizations for AECOPD. Low EOS was an independent risk factor for NIMV treatment in AECOPD. These exacerbations are usually associated with a decrease of CD4+ T cells, suggesting that the causative effect of CD4+ T cells on EOS can be explored.
The peripheral blood eosinopenia on admission of AECOPD, less than 50 cells/µL, occurred in 328 (53.9%) and 90 (54.2%) subjects among study population 1 and 2, suggestive of the prevalence of the low EOS phenotype. In this study, we also evaluated peripheral blood eosinophil count at discharge. Notably, the median percentage of EOS at discharge was significantly higher than that on admission in the low EOS subgroup. However, EOS count remained similar between two measurements in the non-low EOS subgroup. As for the stability of the low EOS during AECOPD, there was a concordance of 63.8% and 56.6% when using the 50 cells/µL and 0.4% cutoffs, respectively. Our results suggested that a low EOS phenotype might be a characteristic phenotype of AECOPD. Though we did not evaluate the stability of the low EOS between the stable state and acute exacerbations, Schumann et al demonstrated that the eosinophil counts between two exacerbations showed higher accordance than that between two measurements in stable state.Citation15 These study data suggest that the low EOS phenotype presents relatively stability during AECOPD, and attention should be paid to the influence of the low EOS on the clinical characteristics and outcomes of AECOPD.
Infection is the most common cause of AECOPD and the low eosinophilic group is predisposed to have clinical diagnosis of pulmonary infection than the non-low eosinophilic group.Citation8,Citation18 Viral infection, especially rhinoviruses, is one of the major risk factors of acute exacerbations of COPD.Citation19,Citation20 A case–control study showed viral respiratory pathogens were more often tested in sputum and nasal lavage of hospitalized patients with AECOPD than in patients with stable COPD (56% versus 19%).Citation21 Low EOS is a common feature of different types of viral infection.Citation22 Furthermore, Bafadhel et al reported that patients presenting to hospital with non-eosinophilic exacerbations of COPD had lower levels of CRP.Citation17 Contrary to their reports, no significant associations between low EOS with the diagnosis of clinical pulmonary infection or the levels of CRP and PCT were observed in our study. Multiple studies reported that AECOPD due to viral infection is more common in the winter seasons.Citation23,Citation24 Considering in our analysis more subjects with low EOS phenotype were admitted during winter than those with non-low EOS phenotype (45.4% vs 30.7%, P < 0.05), it did hint that there might be some relationship of low EOS with viral infection in AECOPD. Hence, further prospective studies are needed.
Low EOS combined with the increased leukocytes has already been described as a risk factor for 30-day all-cause mortality in patients with cardiogenic shock complicating acute myocardial infarction.Citation25 It was also identified as a reliable marker of admission to medical intensive care units in patients with sepsis.Citation26 Both 30-day all-cause mortality and ICU admission mirror the severity of diseases, therefore we wondered whether low EOS was a potential predictor of AECOPD severity or not. In line with our hypothesis, we noted that eosinophil levels <50 cells/µL or <0.4% at admission for a severe AECOPD was associated with an almost double increase in the treatment with NIMV. The DECAF Score including “eosinopenia” was designed to identify those with higher risk of hospital mortality in exacerbations of COPD.Citation27 AECOPD patients could benefit from appropriate antibiotic and systemic corticosteroid therapy. In the first 72 hours of care, corticosteroids significantly improve dyspnea, lung function and ventilation-perfusion mismatch compared with placebo.Citation28 But recent studies reported that patients with low EOS did not respond to systemic corticosteroids as well as patients with non-low EOS.Citation29 In our analysis, the low eosinophilic group was prone to be suffered from respiratory failure than the non-low eosinophilic group. Respiratory failure is an indication for NIMV treatment in the clinical practice. More prospective trials are needed to verify this assertion. We aim to identify and prospectively validate biomarkers that allow the identification of patients in need of impending mechanical ventilation.
Although studies reported that patients with low EOS were accompanied with poor responsiveness to ICS therapy, elevated risk of infectionCitation13,Citation17,Citation30,Citation31 and we also showed high proportion of NIMV treatment in low EOS group, there was no difference in the length of hospital stay between the low and non-low EOS group in our study. MacDonald et al tentatively concluded that eosinophil count <50 cells/μL was more strongly associated with longer median hospital stay than eosinophil count >150/μL. Careful attention to methodological differences revealed that an extended stay in their study was defined as 5 days or longer,Citation8 which is much shorter than our definition of 15 days. The confounding effect of medical insurance policy might mask the effect of low EOS on length of hospital stay. These findings require further confirmation in a larger prospective clinical trial by controlling for corticosteroid prescription and pre-defined discharge criteria. Additionally, we investigated whether long-term clinical outcomes, including readmission rate, differed by EOS level at the initial admission. In consistent with Bafadhel’s conclusion,Citation17 readmission rate over 12 months was not significantly different between the exacerbation phenotypes studied. First, patients might be admitted to another hospital when they were re-admitted with acute exacerbations. Second, the long-term outcomes of AECOPD or readmission rate might be more closely related to the underlying condition of the patient, such as comorbidities.Citation32,Citation33 Pool-analysis with rigorously prospective design is required to explore the association of low EOS with 12-month AECOPD-related readmission.
Not only systemic inflammation, but also immune response are the major factors influencing the outcomes of AECOPD.Citation34–36 Our data indicated that less CD4+ T cells were frequently present in patients with eosinophil count <50 cells/μL, with a stepwise decrease accompanied by gradual eosinophil count increment. It has been suggested that eosinophils are responsible for damage to bronchial epithelial cells by releasing toxic eosinophil granule proteins.Citation37 Our study showed that IL-6 level was lower in patients with low EOS than that in patients with non-low EOS. It was well established that elevated IL-6 levels could drive inflammation in a wide range of diseases, some of which were also characterized by enhanced T cell responses to IL-6.Citation38 Thus, we hypothesize that the level of IL-6 in the low EOS subgroup might be too low to enhance T cell differentiation, with the result of low CD4+ T cells percentage.
There are inevitable limitations in our study. We did not prove the causative effect of CD4+ T cells on EOS because it was an observational study. It has been proposed by us and othersCitation39 that AECOPD patients with low EOS are associated with an increased risk of NIMV treatment and a decrease of CD4+ T cells. Furthermore, based on observations that accumulation of eosinophils can be mediated by activated CD4+ cells through numerous cytokines,Citation40,Citation41 including tumor necrosis factor-alpha (TNF-alpha), we have hypothesized that low EOS was possibly due to a decrease of CD4+ T cells. AE-COPD would be associated with inappropriate immune activation, especially of the adaptive immune systemCitation42 where CD4+ T cells have been shown to play a central role. Further experimental studies are needed to confirm the association of EOS and CD4+ T cells during AECOPD.
Conclusion
To conclude, low EOS in AECOPD was a relatively stable phenotype. Low EOS was an independent risk factor for NIMV treatment in AECOPD. These exacerbations were usually accompanied with a decrease of CD4+ T cells, suggesting that the causative effect of CD4+ T cells on EOS might be explored.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
- Barnes PJ. Immunology of asthma and chronic obstructive pulmonary disease. Nat Rev Immunol. 2008;8(3):183–192. doi:10.1038/nri2254
- Bafadhel M, McKenna S, Terry S, et al. Acute exacerbations of chronic obstructive pulmonary disease: identification of biologic clusters and their biomarkers. Am J Respir Crit Care Med. 2011;184(6):662–671. doi:10.1164/rccm.201104-0597OC
- Tan WC, Bourbeau J, Nadeau G, et al. High eosinophil counts predict decline in FEV 1: results from the CanCOLD study. Eur Respir J. 2021;57(5):2000838. doi:10.1183/13993003.00838-2020
- Park HY, Chang Y, Kang D, et al. Blood eosinophil counts and the development of obstructive lung disease: the Kangbuk Samsung Health Study. Eur Respir J. 2021;58(4):2003823. doi:10.1183/13993003.03823-2020
- Donaldson GC, Seemungal TA, Bhowmik A, et al. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847–852. doi:10.1136/thorax.57.10.847
- Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. doi:10.1136/thx.2005.040527
- MacDonald MI, Osadnik CR, Bulfin L, et al. Low and high blood eosinophil counts as biomarkers in hospitalized acute exacerbations of COPD. Chest. 2019;156(1):92–100. doi:10.1016/j.chest.2019.02.406
- Couillard S, Larivée P, Courteau J, et al. Eosinophils in COPD exacerbations are associated with increased readmissions. Chest. 2017;151(2):366–373. doi:10.1016/j.chest.2016.10.003
- Greulich T, Tüffers J, Mager S, et al. High eosinophil blood counts are associated with a shorter length of hospital stay in exacerbated COPD patients - a retrospective analysis. Respir Res. 2020;21(1):106. doi:10.1186/s12931-020-01365-5
- Vedel-Krogh S, Nielsen SF, Lange P, et al. Blood eosinophils and exacerbations in chronic obstructive pulmonary disease. The Copenhagen General Population Study. Am J Respir Crit Care Med. 2016;193(9):965–974. doi:10.1164/rccm.201509-1869OC
- Hegewald MJ, Horne BD, Trudo F, et al. Blood eosinophil count and hospital readmission in patients with acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2020;15:2629–2641. doi:10.2147/COPD.S251115
- Pascoe S, Locantore N, Dransfield MT, et al. Blood eosinophil counts, exacerbations, and response to the addition of inhaled fluticasone furoate to vilanterol in patients with chronic obstructive pulmonary disease: a secondary analysis of data from two parallel randomised controlled trials. Lancet Respir Med. 2015;3(6):435–442. doi:10.1016/S2213-2600(15)00106-X
- Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
- Schumann DM, Tamm M, Kostikas K, et al. Stability of the blood eosinophilic phenotype in stable and exacerbated COPD. Chest. 2019;156(3):456–465. doi:10.1016/j.chest.2019.04.012
- Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
- Bafadhel M, Greening NJ, Harvey-Dunstan TC, et al. Blood eosinophils and outcomes in severe hospitalized exacerbations of COPD. Chest. 2016;150(2):320–328. doi:10.1016/j.chest.2016.01.026
- Choi J, Oh JY, Lee YS, et al. The association between blood eosinophil percent and bacterial infection in acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2019;14:953–959. doi:10.2147/COPD.S197361
- Viniol C, Vogelmeier CF. Exacerbations of COPD. Eur Respir Rev. 2018;27:147. doi:10.1183/16000617.0103-2017
- Jang JG, Ahn JH, Jin HJ. Incidence and prognostic factors of respiratory viral infections in severe acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2021;16:1265–1273. doi:10.2147/COPD.S306916
- Rohde G, Wiethege A, Borg I, et al. Respiratory viruses in exacerbations of chronic obstructive pulmonary disease requiring hospitalisation: a case-control study. Thorax. 2003;58(1):37–42. doi:10.1136/thorax.58.1.37
- Du Y, Tu L, Zhu P, et al. Clinical features of 85 fatal cases of COVID-19 from Wuhan. A retrospective observational study. Am J Respir Crit Care Med. 2020;201(11):1372–1379. doi:10.1164/rccm.202003-0543OC
- Cameron RJ, de Wit D, Welsh TN, et al. Virus infection in exacerbations of chronic obstructive pulmonary disease requiring ventilation. Intensive Care Med. 2006;32(7):1022–1029. doi:10.1007/s00134-006-0202-x
- Ko FW, Ip M, Chan PK, et al. Viral etiology of acute exacerbations of COPD in Hong Kong. Chest. 2007;132(3):900–908. doi:10.1378/chest.07-0530
- Sasmita BR, Zhu Y, Gan H, et al. Leukocyte and its subtypes as predictors of short-term outcome in cardiogenic shock complicating acute myocardial infarction: a Cohort Study. Shock. 2021. doi:10.1097/SHK.0000000000001876
- Abidi K, Khoudri I, Belayachi J, et al. Eosinopenia is a reliable marker of sepsis on admission to medical intensive care units. Crit Care. 2008;12(2):R59. doi:10.1186/cc6883
- Steer J, Gibson J, Bourke SC. The DECAF Score: predicting hospital mortality in exacerbations of chronic obstructive pulmonary disease. Thorax. 2012;67(11):970–976. doi:10.1136/thoraxjnl-2012-202103
- Walters JA, Tan DJ, White CJ, et al. Systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;9:Cd001288.
- Bafadhel M, McKenna S, Terry S, et al. Blood eosinophils to direct corticosteroid treatment of exacerbations of chronic obstructive pulmonary disease: a randomized placebo-controlled trial. Am J Respir Crit Care Med. 2012;186(1):48–55. doi:10.1164/rccm.201108-1553OC
- Pavord ID, Lettis S, Locantore N, et al. Blood eosinophils and inhaled corticosteroid/long-acting β-2 agonist efficacy in COPD. Thorax. 2016;71(2):118–125. doi:10.1136/thoraxjnl-2015-207021
- Siddiqui SH, Guasconi A, Vestbo J, et al. Blood eosinophils: a biomarker of response to extrafine beclomethasone/formoterol in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192(4):523–525. doi:10.1164/rccm.201502-0235LE
- Agboado G, Peters J, Donkin L. Factors influencing the length of hospital stay among patients resident in Blackpool admitted with COPD: a cross-sectional study. BMJ Open. 2012;2(5):e000869. doi:10.1136/bmjopen-2012-000869
- Greening NJ, Harvey-Dunstan TC, Chaplin EJ, et al. Bedside assessment of quadriceps muscle by ultrasound after admission for acute exacerbations of chronic respiratory disease. Am J Respir Crit Care Med. 2015;192(7):810–816. doi:10.1164/rccm.201503-0535OC
- Xiong G, Xu L, Wei L, et al. Atomization inhalation of terbutaline and budesonide efficiently improved immunity and lung function of AECOPD patients. Cell Mol Immunol. 2008;5(4):287–291. doi:10.1038/cmi.2008.35
- Lugade AA, Bogner PN, Thatcher TH, et al. Cigarette smoke exposure exacerbates lung inflammation and compromises immunity to bacterial infection. J Immunol. 2014;192(11):5226–5235. doi:10.4049/jimmunol.1302584
- Rovina N, Koutsoukou A, Koulouris NG. Inflammation and immune response in COPD: where do we stand? Mediators Inflamm. 2013;2013:413735. doi:10.1155/2013/413735
- Takafuji S, Ohtoshi T, Takizawa H, et al. Eosinophil degranulation in the presence of bronchial epithelial cells. Effect of cytokines and role of adhesion. J Immunol. 1996;156(10):3980–3985.
- Jones BE, Maerz MD, Buckner JH. IL-6: a cytokine at the crossroads of autoimmunity. Curr Opin Immunol. 2018;55:9–14. doi:10.1016/j.coi.2018.09.002
- Freeman CM, Martinez CH, Todt JC, et al. Acute exacerbations of chronic obstructive pulmonary disease are associated with decreased CD4+ & CD8+ T cells and increased growth & differentiation factor-15 (GDF-15) in peripheral blood. Respir Res. 2015;16(1):94. doi:10.1186/s12931-015-0251-1
- Ohkawara Y, Lei XF, Stämpfli MR, et al. Cytokine and eosinophil responses in the lung, peripheral blood, and bone marrow compartments in a murine model of allergen-induced airways inflammation. Am J Respir Cell Mol Biol. 1997;16(5):510–520. doi:10.1165/ajrcmb.16.5.9160833
- Gaspar Elsas MI, Joseph D, Elsas PX, et al. Rapid increase in bone-marrow eosinophil production and responses to eosinopoietic interleukins triggered by intranasal allergen challenge. Am J Respir Cell Mol Biol. 1997;17(4):404–413. doi:10.1165/ajrcmb.17.4.2691
- Geerdink JX, Simons SO, Pike R, et al. Differences in systemic adaptive immunity contribute to the “frequent exacerbator” COPD phenotype. Respir Res. 2016;17(1):140. doi:10.1186/s12931-016-0456-y