
Abstract
Objective
Krebs von den Lungen-6 (KL-6) is expressed on regenerating type II pneumocytes and has been recognized as biomarkers in interstitial lung disease (ILD). We aim to identify the role of the serum KL-6 level in patients with newly diagnosed Sjögren syndrome (SS), as well as the correlation between the immunoassays.
Methods
Patients with newly diagnosed SS and receiving HRCT for clinical reason during follow-up were included. Baseline KL-6 level was measured via enzyme-linked immunosorbent assay (ELISA) and latex particle-enhanced turbidimetric immunoassay (LETIA).
Results
Of the 39 patients, 21 (53.85%) developed interstitial lung disease (ILD) by the conclusion of the follow-up period. The median time to diagnosis of ILD was 2.24 years (IQR 1.15–4.34) in the ILD group. The median serum KL-6 level, measured using ELISA, was 1232 U/mL (IQR 937–2242) and 764.5 U/mL (IQR 503.25–1035.75) in the ILD group and the non-ILD group, respectively (p = 0.001). The median LETIA for serum KL-6 was 329 U/mL (IQR 235–619) and 245 U/mL (IQR 215.25–291) in the ILD group and the non-ILD group, respectively (p = 0.074).
Conclusion
Serum KL-6 levels were higher in newly diagnosed SS patients with ILD diagnosis during follow-up. Thus, the serum KL-6 level can serve as a valuable biomarker to identify hidden ILD in patients with newly diagnosed SS patients. However, the immunoassay procedure may influence the efficacy of the prediction and its clinical association.
Introduction
Sjögren syndrome (SS) is an autoimmune disease presenting with exocrine gland inflammation and extra-glandular involvement.Citation1 Approximately one-fifth of primary SS (pSS) patients presented symptomatic pulmonary involvement with reduced quality of life and a fourfold increase in their mortality rate.Citation2 However, a high fraction of pSS patients without clinical symptoms could be identified abnormality on pulmonary high resolution computed tomography (HRCT).Citation3
Krebs von den Lungen-6 (KL-6), also called episialin, was initially identified using a murine IgG1 monoclonal antibody in a BALB/c mouse, immunized with a human pulmonary adenocarcinoma cell line.Citation4 It is a membrane-associated glycoprotein, which was classified as cluster 9 mucin-1 (MUC1), that is expressed in epithelial cells, especially type II pneumocytes, respiratory bronchiolar epithelial cells, bronchial gland serous cells, fundic gland cells, ductal epithelial cells of mammary glands, pancreas and salivary glands.Citation5,Citation6 Furthermore, it is highly expressed in regenerating pneumocytes from patients with ILD and adenocarcinoma of the lung, pancreas, or breast; whereas in healthy lung tissue, type I pneumocytes, goblet cells, and mucous cells of the bronchial glands do not express KL-6.Citation7 The concentration of KL-6 is highest in the epithelial lining fluid, followed by the serum and then the bronchoalveolar lavage fluid, which suggests a high permeability through the air-blood barrier.Citation7 KL-6 also functions as a chemotactic factor for human fibroblasts, and the high KL-6 concentration found in epithelial lining fluid may trigger intra-alveolar fibrosis.Citation8
Other biomarkers, including anti-Ro antibodies and complement 3 (C3), were reported to be associated with the development of ILD in a cohort of 315 Chinese pSS patients.Citation9 However, the serum KL-6 level is directly related to the process of recovery from pneumonitis and the following fibrosis. We aim to identify the role of the serum KL-6 level in patients with newly diagnosed SS, as well as the correlation between the latex particle-enhanced turbidimetric immunoassay (LETIA) with enzyme-linked immunosorbent assay (ELISA) and association with clinical phenotypes.
Materials and Methods
Study Subjects
In this retrospective case–control study, patients who were diagnosed with pSS between 2011 and 2018 fulfilled the American-European Consensus Group Criteria for Sjögren’s syndrome, and had an available baseline serum sample for KL-6 level evaluation, were included.Citation1 All patients received a chest high resolution computed tomography (HRCT) for clinical reason in the follow-up period. Clinical information and laboratory results on inclusion were retrieved from electronic medical records. A diagnosis of ILD was established by the pulmonologist, and the HRCT patterns were recorded according to the classification of idiopathic interstitial pneumonia.Citation10 The results of pulmonary function testing and pulmonary arterial pressure detected by transthoracic echocardiography at the end of follow-up were recorded. An experienced pulmonologist reviewed all pulmonary imaging, including a chest X-ray and HRCT.
The KL-6 level at baseline was detected with ELISA (MBS2601395; MyBioSource, CA, USA) and LETIA (Nanopia), following the manufacturer’s instructions. Immunologic assay on inclusion included antinuclear antibody (ANA), anti-Ro/La, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), complement 3 (C3) and complement 4 (C4). This study was approved by the Institutional Review Board of Tri-Service General Hospital and the National Defense Medical Center in Taiwan (1-107-05-137).
Statistical Analysis
We used the Chi-square test to compare categorical variables. The continuous variables were tested using the Wilcoxon rank sum test or t-test according to the Shapiro–Wilk normality test. Correlation between continuous variables was examined with Spearman correlation. A p-value <0.05 was considered statistically significant. Biomarker-predicted values were estimated with logistic regression, receiver-operating characteristic (ROC) curve and the area under curve (AUC). We use Youden’s J statistic to find an optimal cut-point. The effect size of independent two-sample comparison was examined in power analysis. Statistical analyses were conducted using the R software, version 3.5.2.
Results
Of the 39 patients with pSS, 21 (53.85%) had developed ILD by the end of the follow-up period, with a median of 2 years (IQR 4.47–0.91). The median age of the participants was 59 years (IQR 53–63). Women comprised 87.2% of the participants. The median time to diagnosis of ILD was 2.24 years (IQR 1.15–4.34) in the ILD group. There were coexisting malignancies in seven patients, including two patients with breast cancer and one patient with lung adenocarcinoma in the non-ILD group and one with breast cancer, one with lymphoplasmacytic lymphoma, one with pancreatic adenocarcinoma, and one with gastric mucosa-associated lymphoid tissue lymphoma in the ILD group. Five patients had non-productive cough lasting for at least 3 months at baseline, including two in the ILD group and three in the non-ILD group. Other baseline characteristics including European League Against Rheumatism Sjögren’s syndrome disease activity index (ESSDAI), immunomodulators, and comorbidities did not show a difference between the ILD and non-ILD groups (). Five patients received labial minor salivary gland biopsy with a focus score 1, three of whom were in the ILD group and two of whom were in the non-ILD group.
Table 1 Patient Characteristics
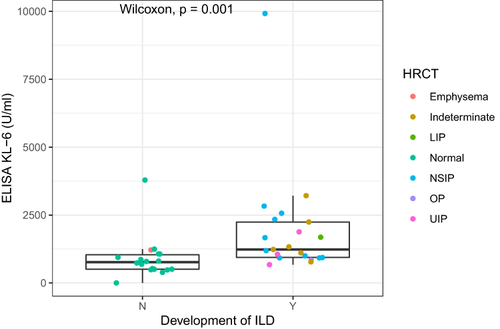
Baseline serum and clinical markers are summarized in . Missing data for clinical laboratory examinations are listed in . Two patients were not arranged pulmonary function test, and echocardiogram was not available in 16 patients. The median serum KL-6 level, measured using ELISA, was 1232 U/mL (IQR 937–2242) and 764.5 U/mL (IQR 503.25–1035.75) in the ILD group and the non-ILD group, respectively (p = 0.001). () The median serum KL-6 in LETIA was 329 U/mL (IQR 235–619) and 245 U/mL (IQR 215.25–291) in the ILD group and the non-ILD group, respectively (p = 0.074). The effect size was 0.528 for ELISA KL-6 and 0.289 for LETIA KL-6. Serum KL-6 did not differ between patients with and without coexisting malignancy (p = 0.770 for ELISA and 0.985 for LETIA). Serum KL-6 level did not differ between patients with and without positive anti-Ro, including ELISA (p = 0.529) and the LETIA (p = 0.867). The correlation between ELISA and LETIA for serum KL-6 was 0.40 (p = 0.012). The correlation between ESSDAI and KL-6 was insignificant in ELISA (r = 0.01, p = 0.929) and low in LETIA (r = 0.32, p = 0.048).
Table 2 Baseline Serum and Clinical Markers
Figure 1 The KL-6 level, measured using enzyme-linked immunosorbent assay, in patients with and without interstitial lung disease (ILD) development, shows significantly higher values in patients with the development of ILD. Colors discriminated against different CT patterns. N and Y represent the non-ILD and ILD groups, respectively. ILD not meeting the above-mentioned patterns was recorded as indeterminate.
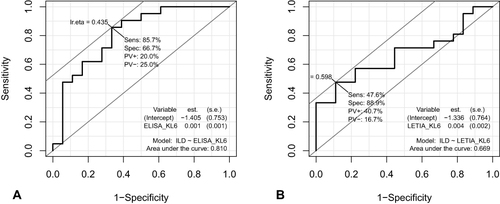
The AUC of the ROC curve was 0.810 and 0.669 on ELISA and LETIA of serum KL-6, respectively (). The optimal cut-point was 922 U/mL and 402 U/mL for ELISA and LETIA of serum KL-6, respectively. The risk factors for ILD are summarized in . Serum KL-6 level higher than the cut-point revealed an increased risk of ILD, odds ratio 12 (95% CI 2.51, 57.48) in ELISA and 7.27 (95% CI 1.33, 39.86) in LETIA. The rest of the biomarkers did meet the significance level to incorporate into multivariable adjustment.Citation11
Table 3 Predictors for Interstitial Lung Disease in Patients with Sjögren Syndrome
Figure 2 Receiver-operating characteristic curve analysis of two methodologies of serum KL-6. Investigation of the ability of KL-6 level to identify the development of ILD in patients with Sjögren syndrome revealed an area under the curve of 0.810 and 0.669 on enzyme-linked immunosorbent assay (ELISA) (A) and latex particle-enhanced turbidimetric immunoassay (LETIA) (B) of serum KL-6, respectively.
At the end of follow-up, the median percentage of predicted forced vital capacity (FVC) was 84.00 (IQR 74.30–88.00) and 86.00 (IQR 74.80–90.40) in the ILD and non-ILD groups, respectively (p-value 0.798); the median diffusing capacity for carbon monoxide (DLCO) was 72.55 (IQR 59.80–84.28) and 90.35 (IQR 83.15–101.50) in the ILD and non-ILD groups, respectively (p-value <0.001). The median pulmonary artery pressure measured by transthoracic echocardiography was 36.00 (IQR 28.50–40.50) mmHg in patients with ILD and 28.00 (IQR 27.00–36.00) in patients without ILD (p = 0.292).
Discussion
KL-6 is a mucin-like high-molecular-weight glycoprotein expressed in regenerating type II pneumocytes.Citation12 Serum KL-6, measured with various immunoassays, has shown diagnostic and prognostic value in ILD. Immunoassays with ELISA, LETIA, and chemiluminescent enzyme immunoassay (CLEIA) have been reported in studies. Its levels are highly associated with ILD activity in patients with radiation pneumonitis, idiopathic pulmonary fibrosis (IPF), nonspecific interstitial pneumonia (NSIP), hypersensitivity pneumonitis, sarcoidosis, rheumatoid arthritis (RA), polymyositis, dermatomyositis, systemic sclerosis (SSc), and a combination of autoimmune diseases, which were primarily measured by ELISA.Citation5,Citation13–22 LETIA KL-6 has demonstrated higher levels in patients with CTD-ILD and provided an independent prognostic prediction for the mortality of patients with RA-associated ILD.Citation23,Citation24 Moreover, serial change in serum KL-6, measured in CLEIA, was associated with the improvement of lung function and HRCT in patients with IPAF.Citation25,Citation26 In a recent trial with newly diagnosed CTD patients, serum KL-6 was higher in CTD-LID patients than patients with non-ILD CTD, pneumonia, and healthy population; there was also a correlation between serum KL-6 and extent of HRCT involvement.Citation22 Serum KL-6 increased mortality hazard with a cutoff value greater than 800 U/mL in a Japanese cohort.Citation27 An increase in the levels of KL-6 in the serum might reflect an increase in the number of regenerating type II pneumocytes, secondary to pulmonary damage.Citation21 Our data also suggested that serum KL-6 level is higher in pSS patients with insubstantial chest X-ray changes (non-radiographic) and developing ILD. Furthermore, KL-6 tended to induce chemotaxis, proliferation and inhibit apoptosis of human fibroblast.Citation8,Citation28 However, the predictivity of KL-6 may vary according to the immunoassay methodology. Serum KL-6 in both immunoassays was elevated in patients with pSS who developed ILD during follow-up, but the LETIA did not achieve significance. Other markers, such as autoimmunity markers (ANA, anti-Ro/La, C3, and C4), inflammation markers (ESR and CRP), and LDH, did not exhibit a significant difference.Citation29–31 Although LETIA is much more efficient than ELISA, only requiring approximately 10 minutes with an automated clinical chemistry analyzer versus 4 hours, respectively, the implication regarding clinical association needs to be carefully taken into consideration.
Pulmonary symptoms are present in 6–15% of the patients with pSS; among these, dyspnea and cough are the most common.Citation29,Citation30 Although most patients with pulmonary involvement are non-symptomatic, they present with functional decline.Citation32 There was a lower DLCO in patients with ILD. FEV1, FVC, FEV1/FVE, or pulmonary arterial pressure, upon transthoracic echocardiography, did not reveal a significant difference. The decline in DLCO was most likely the result of an ILD other than restrictive lung disease, obstructive lung disease, or pulmonary hypertension.
ILD may be highly misdiagnosed or delay-diagnosed in patients with pSS,Citation3 although the progression of ILD is relatively less frequent in patients with pSS than other CTD.Citation33 The pSS patients who developed ILD exhibited increased morbidity and mortality, and required additional medical resources. Our data support that KL-6 is a valuable biomarker in identifying hidden ILD in patients with pSS.
This study was a retrospective case–control study with small sample size and possible selection bias. The effect size in power analysis was large enough for ELISA KL-6 but small for LETIA KL-6. The HRCT was performed at the end of follow-up, but not on inclusion. There might be hidden ILD patients on inclusion until they received HRCT. Except for KL-6 level, other serum biomarker levels were measured clinically with existing missing data. Moreover, although the serum KL-6 level was associated with ILD and adenocarcinoma in the literature review, the coexisting malignancy did not significantly affect the serum KL-6 level in both ELISA and LETIA.
Conclusion
Serum KL-6 levels were significantly higher in SS patients with developing ILD and might denote early pulmonary damage. Serum KL-6 level can serve as a valuable biomarker for identifying hidden ILD in patients with newly diagnosed SS, and regular screening may be warranted. However, the methodology of immunoassay may influence the efficacy of the prediction and clinical association.
Data Sharing Statement
Raw data were generated at Tri-Service General Hospital. Derived data supporting the findings of this study are available from the corresponding author on request.
Ethics Approval
All patients provided written informed consents in this study. This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Tri-Service General Hospital and the National Defense Medical Center in Taiwan (1-107-05-137).
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We thank the health professionals in the Division of Rheumatology/Immunology/Allergies, NDMC, Taiwan and all patients participating in this study. The authors thank Kuo’s Yuan In Enterprise co., LTD, for supporting LETIA KL-6 exam. The abstract of this paper was presented at the 2019 European Congress of Rheumatology as a poster presentation and the 2020 European Congress of Rheumatology as scientific abstracts with interim findings. The poster’s abstract was published in “Poster Presentations” in Annals of the Rheumatic Diseases (https://ard.bmj.com/content/78/Suppl_2/793.2) and “Scientific Abstracts” in Annals of the Rheumatic Diseases (https://ard.bmj.com/content/79/Suppl_1/1908.1).
Additional information
Funding
References
- Vitali C, Bombardieri S, Jonsson R, et al. Classification criteria for Sjogren’s syndrome: a revised version of the European criteria proposed by the American-European Consensus Group. Ann Rheum Dis. 2002;61(6):554–558. doi:10.1136/ard.61.6.554
- Palm O, Garen T, Berge Enger T, et al. Clinical pulmonary involvement in primary Sjogren’s syndrome: prevalence, quality of life and mortality–a retrospective study based on registry data. Rheumatology. 2013;52(1):173–179. doi:10.1093/rheumatology/kes311
- Uffmann M, Kiener HP, Bankier AA, Baldt MM, Zontsich T, Herold CJ. Lung manifestation in asymptomatic patients with primary Sjogren syndrome: assessment with high resolution CT and pulmonary function tests. J Thorac Imaging. 2001;16(4):282–289. doi:10.1097/00005382-200110000-00009
- Kohno N, Akiyama M, Kyoizumi S, Hakoda M, Kobuke K, Yamakido M. Detection of soluble tumor-associated antigens in sera and effusions using novel monoclonal antibodies, KL-3 and KL-6, against lung adenocarcinoma. Jpn J Clin Oncol. 1988;18(3):203–216.
- Oyama T, Kohno N, Yokoyama A, et al. Detection of interstitial pneumonitis in patients with rheumatoid arthritis by measuring circulating levels of KL-6, a human MUC1 mucin. Lung. 1997;175(6):379–385. doi:10.1007/PL00007584
- Castro I, Albornoz N, Aguilera S, et al. Aberrant MUC1 accumulation in salivary glands of Sjogren’s syndrome patients is reversed by TUDCA in vitro. Rheumatology. 2020;59(4):742–753. doi:10.1093/rheumatology/kez316
- Kohno N. Serum marker KL-6/MUC1 for the diagnosis and management of interstitial pneumonitis. J Med Invest. 1999;46(3–4):151–158.
- Hirasawa Y, Kohno N, Yokoyama A, Inoue Y, Abe M, Hiwada K. KL-6, a human MUC1 mucin, is chemotactic for human fibroblasts. Am J Respir Cell Mol Biol. 1997;17(4):501–507. doi:10.1165/ajrcmb.17.4.2253
- Li X, Xu B, Ma Y, et al. Clinical and laboratory profiles of primary Sjogren’s syndrome in a Chinese population: a retrospective analysis of 315 patients. Int J Rheum Dis. 2015;18(4):439–446. doi:10.1111/1756-185X.12583
- Lynch DA, Sverzellati N, Travis WD, et al. Diagnostic criteria for idiopathic pulmonary fibrosis: a Fleischner Society white paper. Lancet Respir Med. 2018;6(2):138–153. doi:10.1016/S2213-2600(17)30433-2
- Heinze G, Wallisch C, Dunkler D. Variable selection - A review and recommendations for the practicing statistician. Biom J. 2018;60(3):431–449. doi:10.1002/bimj.201700067
- Kohno N, Kyoizumi S, Awaya Y, Fukuhara H, Yamakido M, Akiyama M. New serum indicator of interstitial pneumonitis activity. Sialylated carbohydrate antigen KL-6. Chest. 1989;96(1):68–73. doi:10.1378/chest.96.1.68
- Hamada H, Kohno N, Akiyama M, Hiwada K. Monitoring of serum KL-6 antigen in a patient with radiation pneumonia. Chest. 1992;101(3):858–860. doi:10.1378/chest.101.3.858
- Kohno N, Hamada H, Fujioka S, Hiwada K, Yamakido M, Akiyama M. Circulating antigen KL-6 and lactate dehydrogenase for monitoring irradiated patients with lung cancer. Chest. 1992;102(1):117–122. doi:10.1378/chest.102.1.117
- Kohno N, Awaya Y, Oyama T, et al. KL-6, a mucin-like glycoprotein, in bronchoalveolar lavage fluid from patients with interstitial lung disease. Am Rev Respir Dis. 1993;148(3):637–642. doi:10.1164/ajrccm/148.3.637
- Kobayashi J, Kitamura S. Serum KL-6 for the evaluation of active pneumonitis in pulmonary sarcoidosis. Chest. 1996;109(5):1276–1282. doi:10.1378/chest.109.5.1276
- Kubo M, Ihn H, Yamane K, et al. Serum KL-6 in adult patients with polymyositis and dermatomyositis. Rheumatology. 2000;39(6):632–636. doi:10.1093/rheumatology/39.6.632
- Yamane K, Ihn H, Kubo M, et al. Serum levels of KL-6 as a useful marker for evaluating pulmonary fibrosis in patients with systemic sclerosis. J Rheumatol. 2000;27(4):930–934.
- Sakamoto K, Taniguchi H, Kondoh Y, et al. Serum KL-6 in fibrotic NSIP: correlations with physiologic and radiologic parameters. Respir Med. 2010;104(1):127–133. doi:10.1016/j.rmed.2009.08.011
- Takanashi S, Nishina N, Nakazawa M, Kaneko Y, Takeuchi T. Usefulness of serum Krebs von den Lungen-6 for the management of myositis-associated interstitial lung disease. Rheumatology. 2019;58(6):1034–1039. doi:10.1093/rheumatology/key420
- Elhai M, Hoffmann-Vold AM, Avouac J, et al. Performance of candidate serum biomarkers for systemic sclerosis-associated interstitial lung disease. Arthritis Rheumatol. 2019;71(6):972–982. doi:10.1002/art.40815
- Ma H, Lu J, Song Y, Wang H, Yin S. The value of serum Krebs von den lungen-6 as a diagnostic marker in connective tissue disease associated with interstitial lung disease. BMC Pulm Med. 2020;20(1):6. doi:10.1186/s12890-019-1043-z
- Kim HC, Choi KH, Jacob J, Song JW, Kuwana M. Prognostic role of blood KL-6 in rheumatoid arthritis-associated interstitial lung disease. PLoS One. 2020;15(3):e0229997. doi:10.1371/journal.pone.0229997
- Lee JS, Lee EY, Ha YJ, Kang EH, Lee YJ, Song YW. Serum KL-6 levels reflect the severity of interstitial lung disease associated with connective tissue disease. Arthritis Res Ther. 2019;21(1):58. doi:10.1186/s13075-019-1835-9
- Wang J, Zheng P, Huang Z, et al. Serum SP-A and KL-6 levels can predict the improvement and deterioration of patients with interstitial pneumonia with autoimmune features. BMC Pulm Med. 2020;20(1):315. doi:10.1186/s12890-020-01336-y
- Xue M, Cai C, Zeng Y, et al. Krebs von den Lungen-6 and surfactant protein-A in interstitial pneumonia with autoimmune features. Medicine. 2021;100(4):e24260. doi:10.1097/MD.0000000000024260
- Kamiya Y, Fujisawa T, Kono M, et al. Prognostic factors for primary Sjogren’s syndrome-associated interstitial lung diseases. Respir Med. 2019;159:105811. doi:10.1016/j.rmed.2019.105811
- Ohshimo S, Yokoyama A, Hattori N, Ishikawa N, Hirasawa Y, Kohno N. KL-6, a human MUC1 mucin, promotes proliferation and survival of lung fibroblasts. Biochem Biophys Res Commun. 2005;338(4):1845–1852. doi:10.1016/j.bbrc.2005.10.144
- Roca F, Dominique S, Schmidt J, et al. Interstitial lung disease in primary Sjogren’s syndrome. Autoimmun Rev. 2017;16(1):48–54. doi:10.1016/j.autrev.2016.09.017
- Kampolis CF, Fragkioudaki S, Mavragani CP, Zormpala A, Samakovli A, Moutsopoulos HM. Prevalence and spectrum of symptomatic pulmonary involvement in primary Sjogren’s syndrome. Clin Exp Rheumatol. 2018;36(Suppl 112):94–101.
- Elhai M, Avouac J, Allanore Y. Circulating lung biomarkers in idiopathic lung fibrosis and interstitial lung diseases associated with connective tissue diseases: where do we stand? Semin Arthritis Rheum. 2020;50(3):480–491. doi:10.1016/j.semarthrit.2020.01.006
- Flament T, Bigot A, Chaigne B, Henique H, Diot E, Marchand-Adam S. Pulmonary manifestations of Sjogren’s syndrome. Eur Respir Rev. 2016;25(140):110–123. doi:10.1183/16000617.0011-2016
- Chiu YH, Spierings J, de Jong PA, et al. Predictors for progressive fibrosis in patients with connective tissue disease associated interstitial lung diseases. Respir Med. 2021;187:106579. doi:10.1016/j.rmed.2021.106579