
Abstract
Monocyte distribution width (MDW) is a blood monocyte morphological parameter that can be easily detected by an automated hemocyte analyzer and can provide clinicians with important information about cell volume variability in peripheral blood monocyte populations. The United States’ Food and Drug Administration and Conformite Europeenne have both been cleared for their clinical application in the detection of sepsis and developing sepsis in adult patients in the emergency department (ED). Recently, MDW has been found to have an early diagnosis and predictive value for sepsis in neonates and COVID-19 patients. Here, we summarize the findings of the studies investigating the clinical application of MDW in sepsis. Under different stimuli, especially in infectious diseases, the activation of innate immunity is the host’s first defense mechanism, and the change in monocyte volume is considered an early indicator reflecting the state of activation of innate immunity. Pivotal study data from a large multicenter patient cohort showed that abnormal MDW at presentation increases the odds of sepsis, considering the combination of MDW and White Blood Cell Count (WBC) as part of a standard sepsis assessment protocol for ED, which may increase the sensitivity and specificity of sepsis diagnosis. Meanwhile, MDW shares a diagnostic performance comparable to that of conventional biomarkers (C-reactive protein and procalcitonin) in sepsis. In addition, some evidence suggests that increased MDW, both in adults and neonates, may be associated with unfavorable short- and long-term outcomes, which indicates its prognostic value in sepsis. Taken together, MDW is a parameter of increased morphological variability of monocytes in response to infection, and numerous studies have shown that MDW could be used as a valuable diagnostic and prognostic index in patients with sepsis or suspected sepsis.
Introduction
Sepsis is a life-threatening organ dysfunction caused by the maladjustment of the body’s response to infection. Sepsis is a global public health problem that generates more than 3,000,000 hospitalizations per year. Despite advances in modern medicine, more than 5.3 million people die annually from sepsis. It remains the leading cause of death in critically ill patients in non-coronary intensive care units, with an estimated overall mortality rate of approximately 30%. It has high morbidity and mortality, especially among comorbid and hospitalized patients,Citation1,Citation2 and its incidence is continuously increasing worldwide.Citation3 Early diagnosis and treatment of sepsis and sepsis-related organ dysfunction are critical for improving patient survival and reducing healthcare costs.Citation4 To improve survival, early recognition of sepsis has become the primary healthcare goal of many societies, promoting research and the development of optimal biomarkers for rapid diagnosis and assessment of the severity of sepsis-related diseases.
Sepsis biomarkers vary with the pathogenesis of sepsis and knowledge of regarding it. In the 1980s, pro-inflammatory cytokines that produced SIRS (TNF, IL-1β, and IL-6) and C-reactive protein (CRP) were the most important indicators for the early hyperinflammatory phase. In the 1990s, the increased expression of CD64 on the cell during infection was discovered, and procalcitonin (PCT) was described as a marker of bacterial infections. In 2001, the International Conference on Sepsis included, for the first time, CRP and PCT as biomarkers of sepsis.
In addition to these biomarkers, complete blood count (CBC) and leukocyte differential (DIFF) are the most commonly used tests in clinical laboratories, and the application of CBC+DIFF in sepsis diagnosis is common.Citation5 With the introduction of new technologies and the development of analyzers capable of detecting changes in three hematopoietic cell lines, hematology analyzers have greatly improved. UniCel DxH800/900 (Beckman Coulter, Miami, Florida, USA) is used for in vitro diagnostics in clinical laboratories. The DxH800/900 system provides automated CBC, DIFF, nucleated red blood cell count, enumeration, reticulocyte analysis, and an automated method for enumeration of the total nucleated cells and red blood cells in body fluids.
The Coulter principle, under the VCSn (volume, conductivity, and scatter) technology,Citation6 could provide quantitative measurement information of the blood cell morphology (including cell size, morphology and lobulation of nucleus, intracellular granules, etc.). Monocyte distribution width (MDW), a parameter provided by the aforementioned DxH800/900 cellular analysis system, reflects the variability and heterogeneity of monocyte size in peripheral blood. This parameter has been shown to aid in the early detection of sepsis in emergency room patients, and currently, both the FDA and CE have cleared for its clinical application in the detection of sepsis and developing sepsis for adult patients in the emergency department.
As we all know, monocytes can contribute to the process of inflammation or infection by secreting cytokines;Citation7 however, there is increasing evidence that monocytes undergo morphological changes, including volume increase, during inflammatory or infectious processes and during sepsis.Citation8–11 Monocytes are important immune effector cells that protect against microbial pathogens and promote immune surveillance.Citation12 In sepsis, changes in monocytes were documented in 1993.Citation13 Monocytes perform several roles in sepsis, including antigen presentation, phagocytosis of pathogens, and production of pro- and anti-inflammatory cytokines.Citation14 Human blood monocytes are segregated into three subsets based on CD16 and CD14 expression: CD14++/CD16−classical monocytes (CM), CD14++/CD16+ intermediate monocytes (IM), and CD14+/CD16++ non-classical monocytes (NCM).Citation15 During inflammatory conditions, such as sepsis,Citation16 bacterial infection,Citation17 viral infection,Citation18–21 autoimmune diseaseCitation22 and other inflammatory diseases,Citation23,Citation24 the changes (number, volume, function, etc.) in the three subsets are different. Nowadays, MDW, a quantitative morphological parameter for monocyte activation in peripheral blood, could be used as an indicator of inflammation at an early stage.
The Role of MDW in Sepsis
The Role of MDW for Emergency Department (ED) Patients
In ED patients, the prevalence of sepsis is approximately 1.2%.Citation25 Rhee et alCitation26 reported that the vast majority of sepsis patients (86.8% [95% CI, 86.7–87.0%]) had sepsis upon admission. In ED patients, non-severe sepsis without organ failure or shock has a significant difference in mortality compared to severe sepsis. Therefore, the early diagnosis of sepsis may improve patient prognosis.Citation27 Unfortunately, in the ED, the early diagnosis of sepsis has some difficulties, including the overlap of various patient symptoms, limitations of medical conditions, and time constraints.
Owing to the increasing incidence and mortality of sepsis, there is an urgent need for new and effective biomarkers for the diagnosis and monitoring of sepsis in the ED. Many studies have shown that MDW improves the early detection of sepsis during initial ED visits. Based on morphological changes in monocytes during inflammation, the sepsis index ((SI), based on MDW and mean monocyte volume (MMV)) significantly improves the accuracy of early sepsis screening and diagnosis.Citation28,Citation29 A blind, prospective cohort study was conducted in two different emergency departments at Ohio State University by Crouser et al,Citation30 1320 subjects were enrolled in the ED consecutively. Those patients were grouped into systemic inflammatory response syndrome (SIRS), infection, and sepsis (including sepsis, severe sepsis, and septic shock) groups, and MDW was measured using a UniCel DxH 800 analyzer. The results showed that MDW can distinguish sepsis from other conditions (AUC, 0.79; 95% CI, 0.73–0.84); moreover, it was associated with the severity of sepsis, increased with progression from mild infection to sepsis, and was highest in patients with more organ dysfunction in sepsis. A subsequent study also showed that MDW could be used as a screening tool for early identification of patients at risk of sepsis in the ED (AUC, 0.964; 95% CI, 0.945–0.984).Citation31 In a study regarding health and economics,Citation32 approximately 67% of patients benefited from MDW results due to early recognition of sepsis, resulting in a reduction in the average duration of antibiotic use from 3.98 to 2.07 hours and a reduction in the average hospital cost of $3046. At the hospital level, the early diagnosis of sepsis with MDW is expected to reduce the total cost by $712,783 per hospital per year.
Sepsis 3.0 is defined as a life-threatening organ dysfunction caused by a dysregulated host response to infection. For clinical operationalization, organ dysfunction can be represented by an increase in the Sequential [Sepsis-related] Organ Failure Assessment (SOFA) score by 2 points or more. However, the SOFA score can take time to obtain; thus, SIRS criteria [abnormal white blood cell count (WBC), tachycardia, tachypnea, and fever (or hypothermia)] and quick sepsis-related organ failure assessment (qSOFA) score (tachypnea, altered mental state, and hypotension) are used as surrogate methods to assist in the quick diagnosis of sepsis in the ED. Crouser et alCitation33 found that regardless of SIRS or qSOFA variables, an initial MDW >20.0% (vs. <20.0) significantly increased the incidence of sepsis; Meanwhile, according to Agnello et alCitation34 meta-analysis data, MDW plays an important role in Sepsis screening regardless of the Sepsis-2 and Sepsis-3 standard groups; therefore, MDW improved the early detection of sepsis in the initial ED and was a good complement to SIRS and qSOFA parameters. Similarly, the combination of MDW and white blood cell count (WBC),Citation35 neutrophil-to-lymphocyte ratio (NLR), and platelet-to-lymphocyte ratio (PLR)Citation36 significantly improved the early diagnosis of sepsis. It has been proved that the diagnostic performance of MDW was comparable to that of traditional diagnostic biomarkers (PCT, CRP), and the combined diagnosis could enhance the effect to some extent, but not significantly.Citation37,Citation38
The Role of MDW for ICU Patients
Patients in intensive care units (ICUs) are considered at high risk for sepsis because of surgical and invasive procedures.Citation3 Globally, sepsis leading to shock and/or end-organ failure has been identified as the most common indication for ICU admission and the leading cause of ICU death.Citation39 A pilot study in the ICUCitation40 showed that MDW levels at admission were significantly higher in patients with sepsis than in those without sepsis and those with sepsis during hospitalization. Interestingly, the MDW values were significantly higher at the time of clinical sepsis diagnosis than at admission. In addition, Polilli et alCitation41 compared patients with no sepsis, sepsis, and septic shock and found that MDW values were significantly higher in patients with sepsis or septic shock than in the no sepsis group [median 26.23 (IQR: 23.48–29.83); 28.97 (IQR: 21.27–37.21); 21.99 (IQR: 19.86–24.36)]. Moreover, the elevation of MDW was independent of the type of sepsis-causing pathogen. Therefore, MDW can be used as a diagnostic indicator of early sepsis in ICU patients and has a strong ability to resist the interference of infectious organisms. Moreover, MDW is a good predictor of disease progression and associated prognosis.
Reports on the early diagnosis and detection of ICU sepsis using MDW combined with other indicators or compared with other indicators are gradually increasing. In a prospective study in Italy,Citation42 the AUC of MDW (0.785; 95% CI: 0.767–0.801) was comparable to that of PCT (0.759; 95% CI: 0.740–0.778), and superior to CRP (0.667; 95% CI: 0.646–0.688) and WBC (0.570; 95% CI: 0.547–0.592) in the diagnosis of sepsis in the ICU. The combination of MDW > 23 and PCT > 0.5 ng/mL had high specificity (92.6%), Youden index (0.61) and PPV (92.6%).Citation41 Therefore, the combination of MDW with other inflammatory indicators (PCT, CRP, interleukin, and leukocyte-related indicators) indicates a great potential for early diagnosis and prediction of sepsis prognosis.
The Role of MDW in Pediatric Patients
Neonatal sepsis is a clinical syndrome caused by pathogen invasion, with nonspecific signs and symptoms, high morbidity and mortality, and difficult diagnosis.Citation43,Citation44 The incidence of neonatal sepsis is significantly higher in low-income countries than in high-income countries,Citation45,Citation46 and exposure time, dose, infant immune status, and pathogen virulence may affect the incidence and clinical manifestations of neonatal sepsis.Citation43 Early diagnosis of neonatal sepsis is difficult because the symptoms are non-specific, blood culture results are time-consuming, and the positive rate is low. However, using antibiotics to treat culture-negative sepsis or clinical sepsis is controversial.Citation47 Prolonged or unnecessary use of antibiotics increases the risk of other diseases (obesity, necrotizing enterocolitis, fungal infections, bronchopulmonary dysplasia, and death) in newborns.Citation48 Therefore, it is important to identify fast and effective biomarkers for the early detection and diagnosis of neonatal sepsis.
There has been very little literature on the role of MDW in neonatal sepsis. Celik et alCitation49 investigated 227 newborns [sepsis group: 116 (proven sepsis, n = 40; clinical sepsis, n = 76) and control group: 111] and found MDW was higher in septic patients in comparison with control group. The MDW of infants with late-onset sepsis was significantly higher than that of those with early onset sepsis. Moreover, there was no significant difference in the MDW values between gram-positive and gram-negative bacteria grown in blood cultures. An experiment was conducted by Nam et al.Citation50 In pediatric septic patients, the levels of MDW gradually increased from the control, SIRS without infection, to sepsis. In addition, MDW (AUC, 0.77; 95% CI, 0.72–0.83) showed higher AUC values than CRP (AUC, 0.74; 95% CI, 0.68–0.80), and MDW was also a valuable marker for predicting mortality.
CRP,Citation51 PCT,Citation52 IL-6Citation53 are the most widely studied inflammatory markers for the diagnosis of newborn sepsis. Although the CRP concentration correlates with disease severity, early diagnosis of neonatal sepsis is unreliable because of delayed elevation.Citation54 In addition, other non-infectious mother-to-child diseases may lead to elevated CRP levels, making it a nonspecific biomarker.Citation55 Meanwhile, the sensitivity and PPV of CRP are considered low in early-onset sepsis.Citation56 PCT increases more rapidly than CRP, which makes PCT more sensitive than CRP in the early diagnosis of neonatal sepsis,Citation54 and this increase is often associated with disease severity and mortality.Citation57 IL-6 may not be a strong predictor of neonatal sepsis owing to its high measurement cost, low sensitivity, and specificity.Citation49 Although MDW is inferior to PCT and CRP in the diagnosis of neonatal sepsis,Citation49 MDW still has certain advantages in the application of neonatal sepsis diagnosis, owing to its ease of use, fast TAT, micro blood volume requirement, and low cost.
The Role of MDW in COVID-19 Patients
Coronavirus disease 2019 (COVID-19) is caused by SARS-CoV-2 infection, most COVID-19 patients have mild or no symptoms, while some develop symptoms such as severe pneumonia, acute respiratory distress syndrome (ARDS) or multiple organ failure. Lymphocytopenia and inflammatory storms are typical in critically ill patients. Inflammatory storms occur when patients have high levels of inflammatory mediators including IL-6, IL-10, tumor necrosis factor (TNF)-α, and immunosuppressors.Citation58–60 Peripheral circulating monocytes participate in inflammatory storms by producing inflammatory cytokines and mediators.Citation7,Citation61 Interestingly, significant differences were found in the function and morphology of monocytes between COVID-19 patients and healthy individuals.Citation62 Therefore, activation and morphological changes in monocytes may be used to predict changes in the condition of COVID-19 patients.
Ognibene et alCitation63 proved that in COVID-19 positive patients, MDW (mean: 27.3 ± 4.9) was significantly higher than that of COVID-19 negative patients (mean: 20.3 ± 3.3), and the MDW value of severe patients was also higher than that of mild patients, indicating that MDW can be used as an indicator of the prognosis or treatment effect of COVID-19. Recent studies have also shown significant increases in both the lymphoid index and MDW in COVID-19 patients, with good diagnostic performance in combination (AUC: 0.89).Citation64,Citation65 MDW >20 and NLR <3.2 or NLR >5 could independently distinguish COVID-19 from common upper respiratory tract infections or influenza.Citation66 Using random forest classifier, the algorithm developed based on the combination of four monocyte CPD (cellular population data, including MDW) to distinguish positive and negative COVID-19 patients also achieved good results (specificity 89.7%, sensitivity 60.5%), and it was also found that patients with sepsis often had false positives.Citation67 A recent study performed by Riva et alCitation68 showed that MDW is strongly correlated with CRP, fibrinogen, ferritin, and body temperature in COVID-19 patients, that MDW values are significantly correlated with final clinical outcome (survival/discharge vs death), and that the risk of fatal outcomes increased significantly when MDW values were higher than 26.4 (RR = 4.91, 95% CI: 1.73–13.96; OR = 7.14, 95% CI: 2.06–24.71).
Discussion
This review summarizes the current major studies on MDW application in sepsis, suggesting that MDW serves as a new inflammatory marker and can be used as an early diagnosis and prognostic indicator of sepsis in emergency departments, ICU, neonates, children, and patients with COVID-19, and can be used to predict the progression of sepsis ().
Table 1 Researches About Monocyte Distribution Width (MDW) and Sepsis
MDW can be easily measured using an automated hemocyte analyzer (Unicel DxH800/900) together with routine blood tests. Since there is no need for additional technical requirements, the cost of each test is low and affordable (ie, a full blood cell count). Furthermore, TAT is fast, and it may be considered to be of high value in the diagnosis of fast-progressing sepsis. Moreover, it requires simple equipment for MDW detection, which is particularly important in areas where medical facilities may be limited. Compared with other inflammatory indicators, MDW has comparable efficacy to PCT and CRP, and the combined diagnosis can also improve the diagnostic efficacy of sepsis to a certain extent. The cutoff value of MDW is heterogeneous in various studies, where the reference interval of MDW is reported to be 20–25.Citation30,Citation31,Citation33,Citation37,Citation42,Citation69 This may be due to the type and clinical condition of the patients admitted as well as technical problems. The FDACitation70 approved the use of whole blood vein samples of K2EDTA to detect MDW, and many laboratories use K3EDTA, which has been shown to yield higher values for MDW than K2EDTA.Citation71 The influence of anticoagulants has been reported by the manufacturer, with a 1.5 offset between K2 and K3.Citation72 Due to the demographic characteristics of the population and testing technology, a single cut-off point for MDW cannot be determined until a greater degree of standardization is achieved; hence, it is not feasible to adopt a universal cut-off point.
As shown in , as a new inflammatory indicator, MDW can reflect the morphological changes in monocytes during inflammation, which has a positive effect on the early diagnosis of sepsis. MDW is also positively correlated with disease development and can predict disease progression. At the same time, there are also morphological changes in monocytes in some other disease processes (hepatitis B,Citation73 hepatitis C,Citation19 HIV infection,Citation18 Mycobacterium tuberculosis infection,Citation10,Citation17,Citation74 coronary heart diseases, andCitation75 rheumatoid arthritisCitation22); therefore, we can speculate that MDW may also have potential application value in these diseases. In addition, peripheral blood monocytes are an important source of macrophages, and MDW can also reflect some macrophage-related functions (pathogen infection, tumor immunity, immune monitoring, etc.).
Figure 1 MDW and the role of MDW in various diseases. The morphological changes of monocytes can be indicated by MDW values. Under the action of various stimuli, monocytes undergo morphological changes, which can reflect the state of host immune function and the state and process of disease.
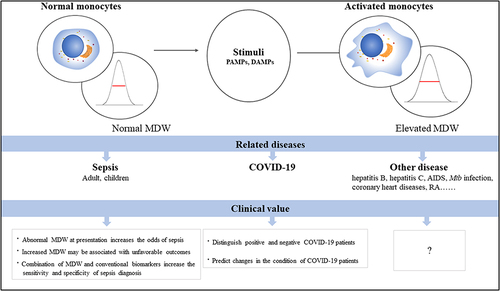
We know the activation of monocyte is an early event of pathogen infection and with no distinction between bacterial, viral or fungal infections. Upon activation, these cells undergo structural and functional modifications, enabling a broad set of immunomodulatory activities. From the studies related to the application of MDW in COVID-19, some inspiring results are obtained. Besides the diagnosis application of MDW in COVID-19 infection, the severity prediction value of MDW in these patients may indicate the pathological mechanism behind it. The dysregulation of monocytes contributes to the systemic hyper-inflammatory response, coagulopathy and organ damage, which could be presented as cytokine storms, cardiac injury, respiratory failure and so on, characterizing the severe form of COVID-19. Interestingly, the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) has clearly defined sepsis as life-threatening organ dysfunction caused by a dysregulated host response to infection. The abnormal activation and dysregulation of monocyte may be serve as the key factor of the sepsis onset and progression. Thus, the application of MDW in sepsis diagnosis and prognosis works from both theoretical and practical aspects. It naturally links the thought of comparison with the exploration of internal mechanism connections between sepsis and COVID-19 infection (especially in severe patients). In addition to MDW, other biomarkers related to monocyte dysregulation or abnormal excessive activation may be investigated to be used in both sepsis and COVID-19. Overall, there is no doubt that more studies are warranted to explore these hypotheses.
Conclusion
Significant progress has been made in the treatment of patients with sepsis; however, the disease remains associated with high mortality and disability. In this review, MDW serves as an important indicator of the activation state of the immune system, is readily and rapidly obtained, plays a key role in infectious disease (sepsis, COVID-19, etc.) diagnosis and prognosis, and plays a non-negligible role in guiding the clinical diagnosis and treatment of the disease. As mentioned before, MDW serves as a morphological indicator of monocyte abnormal activation, and we speculate that MDW could be used in more niches related to dysregulation of monocyte, such as cytokine storm prediction, infection differentiation in immune compromised patients, hematopoietic stem cell transplantation monitoring and so on.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no potential competing interests.
Additional information
Funding
References
- Hotchkiss RS, Moldawer LL, Opal SM, Reinhart K, Turnbull IR, Vincent JL. Sepsis and septic shock. Nat Rev Dis. 2016;2(1):16046. doi:10.1038/nrdp.2016.46
- Grande E, Grippo F, Frova L, et al. The increase of sepsis-related mortality in Italy: a nationwide study, 2003–2015. Eur J Clin Microbiol Infect Dis. 2019;38(9):1701–1708. doi:10.1007/s10096-019-03601-3
- Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the global burden of disease study. Lancet. 2020;395(10219):200–211. doi:10.1016/S0140-6736(19)32989-7
- Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637. doi:10.1097/CCM.0b013e31827e83af
- Spaeth B, Shephard M, Kokcinar R, et al. Impact of point-of-care testing for white blood cell count on triage of patients with infection in the remote Northern Territory of Australia. Pathology. 2019;51(5):512–517. doi:10.1016/j.pathol.2019.04.003
- Martinez-Iribarren A, Tejedor X, Sala Sanjaume À, et al. Performance evaluation of the new hematology analyzer UniCel DxH 900. Int J Lab Hematol. 2021;43(4):623–631. doi:10.1111/ijlh.13448
- Fajgenbaum DC, June CH, Longo DL. Cytokine storm. N Engl J Med. 2020;383(23):2255–2273. doi:10.1056/NEJMra2026131
- Goasguen JE, Bennett JM, Bain BJ, et al. Morphological evaluation of monocytes and their precursors. Haematologica. 2009;94(7):994–997. doi:10.3324/haematol.2008.005421
- Bomans K, Schenz J, Sztwiertnia I, et al. Sepsis induces a long-lasting state of trained immunity in bone marrow monocytes. Front Immunol. 2018;9:2685. doi:10.3389/fimmu.2018.02685
- Shen T, Cao X, Shi J, et al. The morphological changes of monocytes in peripheral blood as a potential indicator for predicting active pulmonary tuberculosis. Clin Chim Acta. 2018;481:189–192. doi:10.1016/j.cca.2018.03.015
- Schulz M, Zambrano F, Schuppe H-C, et al. Monocyte-derived extracellular trap (MET) formation induces aggregation and affects motility of human spermatozoa in vitro. Syst Biol Reprod Med. 2019;65(5):357–366. doi:10.1080/19396368.2019.1624873
- Shi C, Pamer EG. Monocyte recruitment during infection and inflammation. Nat Rev Immunol. 2011;11(11):762–774. doi:10.1038/nri3070
- Fingerle G, Pforte A, Passlick B, et al. The novel subset of CD14+/CD16+ blood monocytes is expanded in sepsis patients. Blood. 1993;82(10):3170–3176. doi:10.1182/blood.V82.10.3170.3170
- Wong KL, Yeap WH, Tai JJY, et al. The three human monocyte subsets: implications for health and disease. Immunol Res. 2012;53(1–3):41–57. doi:10.1007/s12026-012-8297-3
- Ziegler-Heitbrock L, Ancuta P, Crowe S, et al. Nomenclature of monocytes and dendritic cells in blood. Blood. 2010;116(16):e74–80. doi:10.1182/blood-2010-02-258558
- Skrzeczyñska J, Kobylarz K, Hartwich Z, et al. CD14 + CD16 + monocytes in the course of sepsis in neonates and small children: monitoring and functional studies. Scand J Immunol. 2002;55(6):629–638. doi:10.1046/j.1365-3083.2002.01092.x
- Castano D, Garcia LF, Rojas M. Increased frequency and cell death of CD16+ monocytes with Mycobacterium tuberculosis infection. Tuberculosis. 2011;91(5):348–360. doi:10.1016/j.tube.2011.04.002
- Han J, Wang B, Han N, et al. CD14(high)CD16(+) rather than CD14(low)CD16(+) monocytes correlate with disease progression in chronic HIV-infected patients. J Acquir Immune Defic Syndr. 2009;52(5):553–559. doi:10.1097/QAI.0b013e3181c1d4fe
- Rodriguez-Munoz Y, Martín-Vílchez S, López-Rodríguez R, et al. Peripheral blood monocyte subsets predict antiviral response in chronic hepatitis C. Aliment Pharmacol Ther. 2011;34(8):960–971. doi:10.1111/j.1365-2036.2011.04807.x
- Jones JR, Ireland R. Morphological changes in a case of SARS-CoV-2 infection. Blood. 2020;135(25):2324. doi:10.1182/blood.2020006665
- Zhang JY, Zou Z-S, Huang A, et al. Hyper-activated pro-inflammatory CD16 monocytes correlate with the severity of liver injury and fibrosis in patients with chronic hepatitis B. PLoS One. 2011;6(3):e17484. doi:10.1371/journal.pone.0017484
- Rossol M, Kraus S, Pierer M, et al. The CD14 bright CD16+ monocyte subset is expanded in rheumatoid arthritis and promotes expansion of the Th17 cell population. Arthritis Rheum. 2012;64(3):671–677. doi:10.1002/art.33418
- Heine GH, Ulrich C, Seibert E, et al. CD14(++)CD16+ monocytes but not total monocyte numbers predict cardiovascular events in dialysis patients. Kidney Int. 2008;73(5):622–629. doi:10.1038/sj.ki.5002744
- Urra X, Cervera A, Obach V, et al. Monocytes are major players in the prognosis and risk of infection after acute stroke. Stroke. 2009;40(4):1262–1268. doi:10.1161/STROKEAHA.108.532085
- Reinhart K, Daniels R, Kissoon N, et al. Recognizing sepsis as a global health priority – a WHO resolution. N Engl J Med. 2017;377(5):414–417. doi:10.1056/NEJMp1707170
- Rhee C, Dantes R, Epstein L, et al. Incidence and trends of sepsis in US hospitals using clinical vs claims data, 2009–2014. JAMA. 2017;318(13):1241–1249. doi:10.1001/jama.2017.13836
- Holder AL, Gupta N, Lulaj E, et al. Predictors of early progression to severe sepsis or shock among emergency department patients with nonsevere sepsis. Int J Emerg Med. 2016;9(1):10. doi:10.1186/s12245-016-0106-7
- Agnello L, Iacona A, Maestri S, et al. Independent validation of sepsis index for sepsis screening in the emergency department. Diagnostics. 2021;11(7):1292
- Agnello L, Iacona A, Lo Sasso B, et al. A new tool for sepsis screening in the Emergency Department. Clin Chem Lab Med. 2021;59(9):1600–1605. doi:10.1515/cclm-2021-0208
- Crouser ED, Parrillo JE, Seymour C, et al. Improved early detection of sepsis in the ED with a novel monocyte distribution width biomarker. Chest. 2017;152(3):518–526. doi:10.1016/j.chest.2017.05.039
- Agnello L, Bivona G, Vidali M, et al. Monocyte distribution width (MDW) as a screening tool for sepsis in the emergency department. Clin Chem Lab Med. 2020;58(11):1951–1957. doi:10.1515/cclm-2020-0417
- Paoli CJ, Reynolds MA, Coles C, et al. Predicted economic benefits of a novel biomarker for earlier sepsis identification and treatment: a counterfactual analysis. Crit Care Explor. 2019;1(8):e0029. doi:10.1097/CCE.0000000000000029
- Crouser ED, Parrillo JE, Martin GS, et al. Monocyte distribution width enhances early sepsis detection in the emergency department beyond SIRS and qSOFA. J Intensive Care. 2020;8:33. doi:10.1186/s40560-020-00446-3
- Agnello L, Vidali M, Sasso BL, et al. Monocyte distribution width (MDW) as a screening tool for early detecting sepsis: a systematic review and meta-analysis. Clin Chem Lab Med. 2022;60(5):786–792. doi:10.1515/cclm-2021-1331
- Crouser ED, Parrillo JE, Seymour CW, et al. Monocyte distribution width: a novel indicator of sepsis-2 and sepsis-3 in high-risk emergency department patients. Crit Care Med. 2019;47(8):1018–1025. doi:10.1097/CCM.0000000000003799
- Hou SK, Lin HA, Chen SC, Lin CF, Lin SF. Monocyte distribution width, neutrophil-to-lymphocyte ratio, and platelet-to-lymphocyte ratio improves early prediction for sepsis at the emergency. J Pers Med. 2021;11(8):732. doi:10.3390/jpm11080732
- Woo A, Oh DK, Park C-J, et al. Monocyte distribution width compared with C-reactive protein and procalcitonin for early sepsis detection in the emergency department. PLoS One. 2021;16(4):e0250101. doi:10.1371/journal.pone.0250101
- Hausfater P, Robert Boter N, Morales Indiano C, et al. Monocyte distribution width (MDW) performance as an early sepsis indicator in the emergency department: comparison with CRP and procalcitonin in a multicenter international European prospective study. Crit Care. 2021;25(1):227. doi:10.1186/s13054-021-03622-5
- Raman V, Laupland K. Challenges to reporting the global trends in the epidemiology of ICU-treated sepsis and septic shock. Curr Infect Dis Rep. 2021;23:23. doi:10.1007/s11908-021-00767-w
- Agnello L, Sasso BL, Giglio RV, et al. Monocyte distribution width as a biomarker of sepsis in the intensive care unit: a pilot study. Ann Clin Biochem. 2021;58(1):70–73. doi:10.1177/0004563220970447
- Polilli E, Frattari A, Esposito JE, et al. Monocyte distribution width (MDW) as a new tool for the prediction of sepsis in critically ill patients: a preliminary investigation in an intensive care unit. BMC Emerg Med. 2021;21(1):147. doi:10.1186/s12873-021-00521-4
- Piva E, Zuin J, Pelloso M, et al. Monocyte distribution width (MDW) parameter as a sepsis indicator in intensive care units. Clin Chem Lab Med. 2021;59(7):1307–1314. doi:10.1515/cclm-2021-0192
- Shane AL, Sánchez PJ, Stoll BJ. Neonatal sepsis. Lancet. 2017;390(10104):1770–1780. doi:10.1016/S0140-6736(17)31002-4
- Celik IH, Hanna M, Canpolat FE, Pammi M. Diagnosis of neonatal sepsis: the past, present and future. Pediatr Res. 2021;91:337–350.
- Weston EJ, Pondo T, Lewis MM, et al. The burden of invasive early-onset neonatal sepsis in the United States, 2005–2008. Pediatr Infect Dis J. 2011;30(11):937–941. doi:10.1097/INF.0b013e318223bad2
- Oza S, Lawn JE, Hogan DR, et al. Neonatal cause-of-death estimates for the early and late neonatal periods for 194 countries: 2000–2013. Bull World Health Organ. 2015;93(1):19–28. doi:10.2471/BLT.14.139790
- Cantey JB, Baird SD. Ending the culture of culture-negative sepsis in the neonatal ICU. Pediatrics. 2017;140(4). doi:10.1542/peds.2017-0044
- Ting JY, Synnes A, Roberts A, et al. Association between antibiotic use and neonatal mortality and morbidities in very low-birth-weight infants without culture-proven sepsis or necrotizing enterocolitis. JAMA Pediatr. 2016;170(12):1181–1187. doi:10.1001/jamapediatrics.2016.2132
- Celik HT, Portakal O, Yiğit Ş, et al. Efficacy of new leukocyte parameters versus serum C-reactive protein, procalcitonin, and interleukin-6 in the diagnosis of neonatal sepsis. Pediatr Int. 2016;58(2):119–125. doi:10.1111/ped.12754
- Nam M, Son BH, Seo JE, et al. Improved diagnostic and prognostic power of combined delta neutrophil index and mean platelet volume in pediatric sepsis. Ann Clin Lab Sci. 2018;48(2):223–230.
- McWilliam S, Riordan A. How to use: C-reactive protein. Arch Dis Child Educ Pract Ed. 2010;95(2):55–58. doi:10.1136/adc.2009.174367
- Irwin AD, Carrol ED. Procalcitonin. Arch Dis Child Educ Pract Ed. 2011;96(6):228–233. doi:10.1136/archdischild-2011-300178
- Silveira RC, Procianoy RS. Evaluation of interleukin-6, tumour necrosis factor-alpha and interleukin-1 beta for early diagnosis of neonatal sepsis. Acta Paediatr. 1999;88(6):647–650. doi:10.1080/08035259950169314
- Brown JVE, Meader N, Wright K, et al. Assessment of C-reactive protein diagnostic test accuracy for late-onset infection in newborn infants: a systematic review and meta-analysis. JAMA Pediatr. 2020;174(3):260–268. doi:10.1001/jamapediatrics.2019.5669
- Celik IH, Demirel G, Canpolat FE, Erdeve O, Dilmen U. Inflammatory responses to hepatitis B virus vaccine in healthy term infants. Eur J Pediatr. 2013;172(6):839–842. doi:10.1007/s00431-013-1946-2
- Lacaze-Masmonteil T, Rosychuk RJ, Robinson JL. Value of a single C-reactive protein measurement at 18 h of age. Arch Dis Child Fetal Neonatal Ed. 2014;99(1):F76–9. doi:10.1136/archdischild-2013-303984
- Altunhan H, Annagür A, Örs R, Mehmetoğlu I. Procalcitonin measurement at 24 hours of age may be helpful in the prompt diagnosis of early-onset neonatal sepsis. Int J Infect Dis. 2011;15(12):e854–8. doi:10.1016/j.ijid.2011.09.007
- Liu J, Li S, Liu J, et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. EBioMedicine. 2020;55:102763. doi:10.1016/j.ebiom.2020.102763
- Mehta P, McAuley DF, Brown M, et al. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. 2020;395(10229):1033–1034. doi:10.1016/S0140-6736(20)30628-0
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
- Chousterman BG, Swirski FK, Weber GF. Cytokine storm and sepsis disease pathogenesis. Semin Immunopathol. 2017;39(5):517–528. doi:10.1007/s00281-017-0639-8
- Karimi Shahri M, Niazkar HR, Rad F. COVID-19 and hematology findings based on the current evidences: a puzzle with many missing pieces. Int J Lab Hematol. 2021;43(2):160–168. doi:10.1111/ijlh.13412
- Ognibene A, Lorubbio M, Magliocca P, et al. Elevated monocyte distribution width in COVID-19 patients: the contribution of the novel sepsis indicator. Clin Chim Acta. 2020;509:22–24. doi:10.1016/j.cca.2020.06.002
- Zeng X, Xing H, Wei Y, et al. Monocyte volumetric parameters and lymph index are increased in SARS-CoV-2 infection. Int J Lab Hematol. 2020;42(6):e266–e269. doi:10.1111/ijlh.13323
- Lippi G, Sanchis-Gomar F, Henry BM. Pooled analysis of monocyte distribution width in subjects with SARS-CoV-2 infection. Int J Lab Hematol. 2021;43(4):O161–o163. doi:10.1111/ijlh.13482
- Lin HA, Lin S-F, Chang H-W, et al. Clinical impact of monocyte distribution width and neutrophil-to-lymphocyte ratio for distinguishing COVID-19 and influenza from other upper respiratory tract infections: a pilot study. PLoS One. 2020;15(11):e0241262. doi:10.1371/journal.pone.0241262
- Vasse M, Ballester M-C, Ayaka D, et al. Interest of the cellular population data analysis as an aid in the early diagnosis of SARS-CoV-2 infection. Int J Lab Hematol. 2021;43(1):116–122. doi:10.1111/ijlh.13312
- Riva G, Castellano S, Nasillo V, et al. Monocyte distribution width (MDW) as novel inflammatory marker with prognostic significance in COVID-19 patients. Sci Rep. 2021;11(1):12716. doi:10.1038/s41598-021-92236-6
- Polilli E, Sozio F, Frattari A, et al. Comparison of monocyte distribution width (MDW) and procalcitonin for early recognition of sepsis. PLoS One. 2020;15(1):e0227300. doi:10.1371/journal.pone.0227300
- Lopez-Molina M, Ganduxé XT, Iribarren AM, et al. Influence of K2-EDTA and K3-EDTA tubes for monocyte distribution width measurement. Clinica Chimica Acta. 2019;493:S384. doi:10.1016/j.cca.2019.03.819
- Agnello L, Lo Sasso B, Bivona G, et al. Reference interval of monocyte distribution width (MDW) in healthy blood donors. Clin Chim Acta. 2020;510:272–277. doi:10.1016/j.cca.2020.07.036
- Agnello L, Lo Sasso B, Vidali M, et al. Validation of monocyte distribution width decisional cutoff for sepsis detection in the acute setting. Int J Lab Hematol. 2021;43(4):O183–O185. doi:10.1111/ijlh.13496
- Lu Y, Wang G, Li C. Expression of peripheral monocytic programmed death ligand-1 in severe sepsis combined with HBV-related cirrhosis. A pilot observational study. Cent Eur J Immunol. 2021;46(2):217–224. doi:10.5114/ceji.2021.108179
- Sun T, Wu B, Wang J, Yuan T, Huang H, Xu D. Evaluation of the diagnostic efficacy of monocyte parameters and MCP-1 to distinguishing active tuberculosis from latent tuberculosis. Clin Lab. 2019;65(7):2411–2502
- Li HZ, Wang Q, Zhang YY, et al. Onset of coronary heart disease is associated with HCMV infection and increased CD14 (+)CD16 (+) monocytes in a population of Weifang, China. Biomed Environ Sci. 2020;33(8):573–582. doi:10.3967/bes2020.076