
Abstract
Purpose
Our study aimed to identify inflammatory biomarkers and develop a prediction model to stratify high-risk patients for hepatitis B virus-associated hepatocellular carcinoma (HBV-HCC) recurrence after curative resection.
Patients and Methods
A total of 583 eligible HBV-HCC patients with curative hepatectomy from Guangdong Provincial People’s Hospital (GDPH) and Sun Ya-sen University Cancer Centre (SYSUCC) were enrolled in our study. Cox proportional hazards regression was utilized to evaluate potential risk factors for disease-free survival (RFS). The area under the receiver operating characteristic (ROC) curve (AUC) was utilized to assess the discrimination performance. Calibration plots and decision curve analyses (DCA) were used to evaluate the calibration of the nomogram and the net benefit, respectively.
Results
Based on the systemic inflammation response index (SIRI), aspartate aminotransferase to neutrophil ratio index (ANRI), China Liver Cancer (CNLC) stage and microvascular invasion, a satisfactory nomogram was developed. The AUC of our nomogram for predicting 1-, 2-, and 3-year RFS was 0.767, 0.726, and 0.708 in the training cohort and 0.761, 0.716, and 0.715 in the validation cohort, respectively. Furthermore, our model demonstrated excellent stratification as well as clinical applicability.
Conclusion
The novel nomogram showed a higher prognostic power for the RFS of HCC patients with curative hepatectomy than the CNLC, AJCC 8th edition and BCLC staging systems and may help oncologists identify high-risk HCC patients.
Introduction
Primary liver cancer is a health threat worldwide, among which hepatocellular carcinoma accounts for more than 80% of cases.Citation1 Hepatitis B virus infection is the leading aetiology of hepatocellular carcinoma in East Asia, particularly in China.Citation2 Currently, hepatectomy is the most effective and curative treatment for select patients at early and intermediate stages.Citation3–6 Unfortunately, the high rate of tumour recurrence leads to poor 5-year overall survival.Citation7–9 At present, some studies have shown that adjuvant therapy can prolong the survival of high-risk patients. For example, our previous studies revealed that HCC patients with microvascular invasion (MVI) should receive adjuvant transhepatic arterial chemotherapy and embolization (TACE) or hepatic artery infusion chemotherapy (HAIC) treatment, which could improve their survival outcomes efficaciously and safely.Citation10,Citation11 Therefore, it is urgent to identify novel biomarkers and develop a prediction model to identify high-risk patients for HCC recurrence.
The Barcelona Clinic Liver Cancer (BCLC) staging system and American Joint Committee on Cancer (AJCC) staging system are widely applied in the clinic and can help doctors choose the best treatment.Citation3,Citation5,Citation6 An increasing number of studies have proven that the predictive effect of these staging systems is less than satisfactory.Citation12–15 Recently, Chinese experts put forward the China Liver Cancer (CNLC) staging system integrating the performance status, liver function, extrahepatic metastasis, macrovascular invasion, tumour size and tumour number.Citation16 The CNLC staging system shows good stratification abilities and prognostic accuracy, but it could be improved by integrating some critical inflammatory biomarkers.Citation14,Citation17 Meanwhile, the albumin-bilirubin score (ALBI),Citation18 neutrophil-to-lymphocyte ratio (NLR),Citation19 systemic immune-inflammation index (SII),Citation20 systemic inflammation response index (SIRI)Citation21 and aspartate aminotransferase to neutrophil ratio index (ANRI) have been reported as independent prognostic risk factors that could predict recurrence for many solid tumours. Thus, it is reasonable to construct a model combining the CNLC with these clinical blood indexes and identify which patients are at high risk of recurrence and should receive the appropriate adjuvant treatment after curative hepatectomy.
In this study, serum laboratory data and pathological information from 583 patients with HBV-related HCC were obtained from two Chinese hepatobiliary surgery centres. We aimed to develop and validate a practical and novel nomogram for RFS based on the selected significant inflammatory biomarkers and we compared the predictive power of the newly established nomogram with three common staging systems.
Methods
This multi-institutional retrospective study was approved by the Institutional Review Board of Guangdong Provincial People’s Hospital (KY-Q-2022-086-01) and Sun Yat-Sen University Cancer Center (B2019-057-01). All procedures performed in this study involving human participants were performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Data Collection
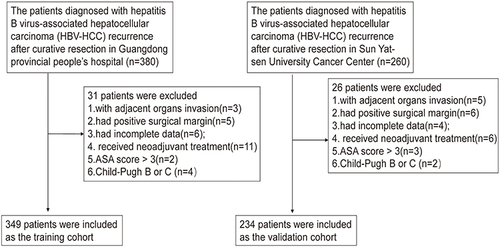
From 1 January 2014 to 1 January 2017, the clinical data of 349 patients who underwent curative hepatectomy and had pathologically confirmed HBV-related hepatocellular carcinoma (HBV-HCC) at Guangdong Provincial People’s Hospital (GDPH) were included in the present study as the training cohort. Meanwhile, the clinical data of 234 patients pathologically diagnosed with HBV-HCC at Sun Yat-sen University Cancer Centre (SYSUCC) were collected as the validation cohort. The inclusion criteria were as follows: (1) had undergone liver resection and pathologically diagnosed with HBV-HCC; (2) had liver function by the Child‒Pugh A and American Society of Anaesthesiologists (ASA) Score < III; and (3) had not received any neoadjuvant treatments before hepatectomy. Patients who (1) had incomplete baseline data and follow-up data; (2) had a positive surgical margin; (3) had distant metastasis or adjacent organ invasion; and (4) had received neoadjuvant treatments, such as TACE and HAIC, were excluded from this study. The postoperative pathologic stage of HCC was evaluated by the BCLC staging system, AJCC 8th Edition (AJCC-8) staging system and China Liver Cancer (CNLC) staging system. Recurrence-free survival (RFS) was defined as the interval from the date of surgery to tumour recurrence. HCC patients with curative resection were advised to undergo imaging examinations (contrast-enhanced CT or contrast-enhanced MRI) and peripheral blood index examinations (such as AFP, AST, ALT, and TBIL) one month after surgery to ensure that they underwent curative surgery and had good liver function. After that, they underwent imaging examinations (contrast-enhanced CT, MRI or abdominal ultrasound) and peripheral blood tests (such as AFP, HBV-DNA, AST, ALT, and TBIL) every 3 months for 5 years and every 6 months after 5 years to detect any recurrences.
Definition of Some Indicators
The definition formulas are listed as follows: (1) neutrophil-to-lymphocyte ratio (NLR = N/L); (2) platelet-to-lymphocyte ratio (PLR=P/L); (3) monocyte-to-lymphocyte ratio (MLR = M/L); (4) systemic immune-inflammation index (SII = P*[N/L]); (5) systemic inflammation response index (SIRI=(N*M)/L); (6) γ-glutamyl transferase-to-platelet ratio (GPR=GGT/P); (7) albumin-bilirubin score (ALBI= (log10(bilirubin µmol/L) × 0.66 + (albumin g/L) × (−0.085))); and (8) aspartate aminotransferase to neutrophil ratio index (ANRI=AST/N).
Statistical Analysis and Nomogram Construction
Cox proportional hazards regression was used to evaluate the potential prognostic factors and to evaluate the potential risk factors for recurrence. Tolerance and variance inflation factor (VIF) values were calculated based on SPSS software (version 20.0, IBM Statistics, Chicago, IL, USA) to estimate the multicollinearity between variables. According to previous studies, variables with tolerance <0.1 and VIF >10 were considered indicative of multicollinearity and were excluded from the multivariable Cox regression analysis.Citation22,Citation23 The nomogram based on the potential risk factors was constructed by the rms package. The concordance index (C-index) and area under the receiver operating characteristic (ROC) curve (AUC) were utilized to assess the discrimination performance. Calibration plot and decision curve analysis (DCA) were used to evaluate the calibration of the nomogram and the net benefit, respectively. Patients were divided into three groups with X-tile based on the risk score. Then, Kaplan‒Meier analyses were performed among different risk groups to assess the stratification ability of the novel nomogram. R version 4.0.0 software (http://www.r-project.org/) was used for most of the statistical analyses. A P value<0.05 was regarded as statistically significant, and all tests were two-sided.
Results
Patient Clinicopathological Characteristics
After applying the inclusion criteria, a total of 583 eligible HCC patients from GDPH and SYSUCC were enrolled in our study (). The patients in this study were all HBsAg positive, and most had well-preserved liver function at Child‒Pugh class A. Men (88.25% and 89.32%) were predominant in both cohorts. The average ages were 54.45 and 49.62 in the GDPH group and the SYSUCC group, respectively. Microvascular invasion was detected in 101 (28.94%) patients from GDPH and 91 (33.76%) patients from SYSUCC. The median follow-up time of training cohort is 37 months (36–43 months) and of validation cohort is 65.6 months (63–67.9 months). The patients’ clinicopathologic characteristics are summarized in .
Table 1 Clinicopathological Characteristics of Two Cohorts
Figure 1 The flowchart of the selection process for the training and validation cohorts.
Recurrence-Free Survival in the GDPH and SYSUCC Cohorts
The median RFS time in the GDPH cohort was 42 months (34–60 months), and 166 (47.56%) patients suffered a tumour recurrence. The 1-, 2- and 3-year RFS rates were 74.5%, 64.47% and 58.74%, respectively. Moreover, in the SYSUCC cohort, the median RFS time was not reached, and 108 (46.15%) patients had a recurrence. The 1-, 2- and 3-year RFS rates were 70.09%, 59.83% and 53.00%, respectively.
Prognostic and Stratification Capacities of the CNLC, BCLC and AJCC 8th Staging Systems
The CNLC, AJCC 8th and BCLC staging systems are widely applied in the clinic and used to guide clinical treatment decisions. The prognostic capacities of these staging systems were compared in our two cohorts. ROC curve analyses showed that the BCLC staging system had the worst AUC value for predicting 1-, 2- and 3-year RFS in both the GDPH cohort and the SYSUCC cohort. Similar AUC values for the CNLC and TNM staging systems were observed in the two cohorts ( and ).
Figure 2 The prognostic values of three staging systems: (A and B) the time-dependent ROC values of DFS in training cohort (A) and validation cohort (B); (C–E): the KM analysis of three staging system in training cohort; (F–H): the KM analysis of three staging system in validation cohort.
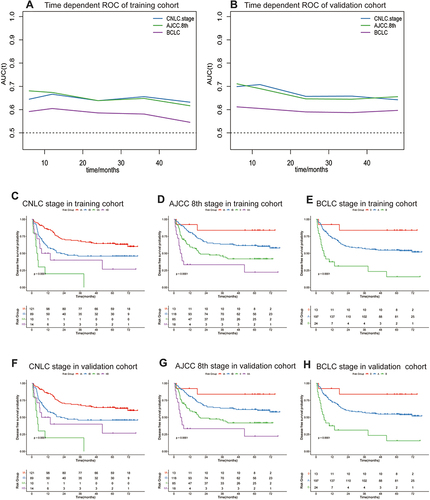
Moreover, we performed KM analysis to explore the stratification abilities of the three staging systems. The results revealed that BCLC had the best stratification ability compared with the two other staging systems ().
Identification of Independent Prognostic Factors for HBV-Related HCC
Cox proportional hazards regression analysis was utilized to identify the prognostic factors for 349 HBV-HCC patients in the GDPH cohort. The results of univariate Cox regression analysis indicated that AFP, microvascular invasion, tumour size, CNLC stage, AJCC 8th edition stage, BCLC stage, NLR, SII, SIRI, ANRI, PLR, MLR and GPR were regarded as potential risk factors (). The significant predictors were sequentially enrolled in multivariate Cox regression analysis. As Supplementary Table 1 showed, the tolerance of PLR was less than 0.1, and its VIF was larger than 10, indicating that PLR should be excluded. Considering that these three staging systems may have mutual influence, we performed multivariate Cox regression analysis. Finally, showed that microvascular invasion, CNLC stage, SIRI and ANRI were independent prognostic factors for RFS in HBV-HCC patients who underwent hepatectomy (the results of the AJCC 8th edition and BCLC staging system can be found in Supplementary Tables 2 and 3). In summary, CNLC stage, microvascular invasion, SIRI and ANRI were regarded as the key prognostic factors for HBV-related HCC.
Table 2 Univariate Cox Regression Analysis of Disease-Free Survival in the Training Cohort
Table 3 Multivariate Cox Regression Analysis of Disease-Free Survival Based on CNLC Staging System in the Training Cohort
Construction and Validation of a Novel Prognostic Nomogram for RFS
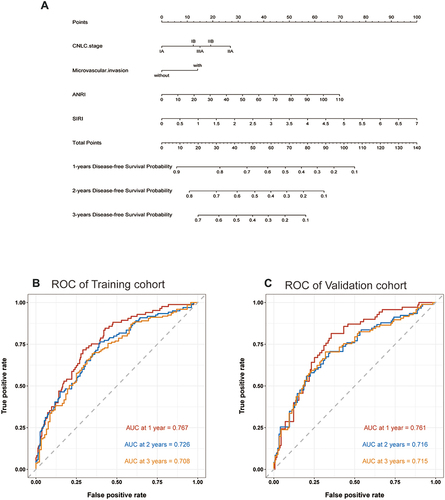
A satisfactory nomogram for predicting the 1-, 2- and 3-year RFS of HBV-HCC was established based on microvascular invasion, CNLC stage, SIRI and ANRI (). According to the formula of our nomogram, the recurrence risk score for each patient in these two cohorts could be calculated conveniently. A higher total score indicated a worse prognosis. The AUC values for our nomogram for predicting 1-, 2-, and 3-year RFS were 0.767, 0.726, and 0.708 in the training cohort and 0.761, 0.716, and 0.715 in the validation cohort, respectively ( and ).
Figure 3 (A) the nomogram for predicting the 1-, 2-, and 3-year DFS of HBV-HCC patients after curative hepatectomy. (B and C): the 1-year, 2-year and 3-year ROC values of DFS in training cohort (B) and validation cohort (C).
The time-dependent AUC further showed that our nomogram was also better than the CNLC, AJCC-8th and BCLC staging systems and the other predictive factors alone ( and ).
Figure 4 (A and B) the time-dependent ROC values of our nomogram, three staging systems and other clinicopathological characteristics in training cohort (A) and validation cohort (B); (C): the KM analysis of our nomogram in training cohort; (D): the KM analysis of our nomogram in validation cohort; (E–G): Calibration plots of the nomogram for 1-year (E), 2-year (F), and 3-year (G) survival prediction of training cohort; (H–J): Calibration plots of the nomogram for 1-year (H), 2-year (I), and 3-year (J) survival prediction of validation cohort.
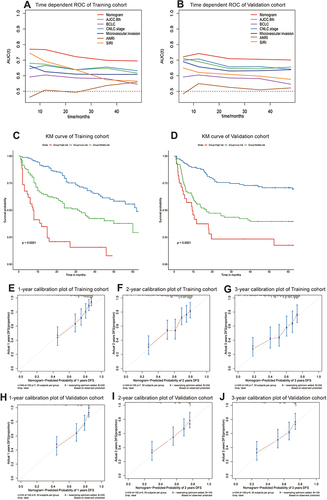
To further explore the prognostic and stratification capacities of the nomogram, the GDPH cohort was divided into high-, medium- and low-recurrence risk subgroups based on an optimal cut-off value determined by X-tile: low-risk group<32.90; 32.90 ≤middle-risk group<65.54; high-risk group≥65.54. As shown in , patients in the low-risk group had the best RFS, while those in the high-risk group had the worst RFS. We applied the same cut-off value to divide the SYSUCC cohort into high-, middle- and low-recurrence-risk subgroups. As shown in , patients in different risk subgroups had different RFS. This indicated that our nomogram had outstanding stratification ability.
We drew calibration curves to illustrate the probability of 1-, 2- and 3-year RFS between the prediction by the novel nomogram and the actual observation. The calibration curves matched well in the training and validation cohorts, which showed that they could accurately predict the 1-, 2-, and 3-year RFS ().
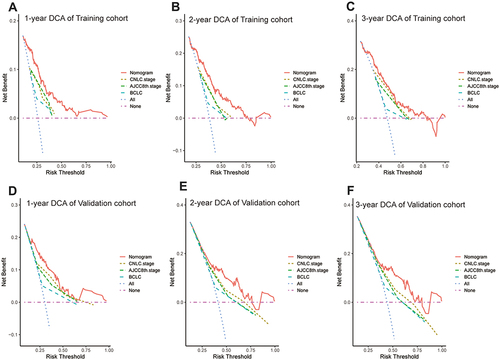
Decision curve analysis (DCA) was performed to evaluate the clinical performance and the net benefit of our nomogram. Compared to the CNLC, AJCC-8th and BCLC staging systems, our nomogram could provide a better clinical benefit and had significant clinical application in the GDPH cohort and the SYSUCC cohort ().
Figure 5 Decision curve analysis of the nomogram. (A–C) Decision curve analysis of the nomogram for 1-year (A), 2-year (B), and 3-year (C) DFS prediction in training cohort; (D–F) Decision curve analysis of the nomogram for 1-year (D), 2-year (E), and 3-year (F) DFS prediction in validation cohort.
Discussion
It is well known that a high risk of recurrence is the main problem for HCC patients after curative liver resection. At present, it is of great clinical significance to identify the independent prognostic factors of RFS, build a reliable model to predict tumour recurrence and provide a strategy for adjuvant therapy for high-risk patients. In this study, SIRI, ANRI, and CNLC stage and microvascular invasion were regarded as the key prognostic factors for HBV-related HCC. A novel nomogram was constructed based on 349 patients from the hepatobiliary surgery centre of GDPH and validated by 234 patients from the hepatobiliary surgery centre of SYSUCC. The novel nomogram showed higher ROC values and stratification ability, better calibrations and more net benefits than the three widely used staging systems.
Microvascular invasion is a nest of malignant cells in endothelial-lined vessels visible only under a microscope.Citation24 Increasing numbers of studies have demonstrated that MVI is an occult micrometastasis of HCC and it has a great negative impact on the survival of HCC patients after hepatectomy.Citation24 We confirmed that MVI was an independent risk factor in this study, which is consistent with our previous findings.Citation25,Citation26 Our previous studies have demonstrated that receiving adjuvant TACE or HAIC with FOLFOX after hepatectomy might improve the RFS and OS for HCC patients with MVI, and the adverse events were evaluated as mild and manageable.Citation10,Citation11
SIRI and ANRI are both comprehensive haematological indices of inflammation.Citation27 Their effective prediction capacities for survival and tumour recurrence have been extensively validated in many solid tumours, such as lung cancer,Citation28 gallbladder cancerCitation27 and pancreatic cancer.Citation21 In our research, the performance of these inflammatory indicators was indeed outstanding in predicting recurrence-free survival of HBV-HCC with curative resection.Cancer-associated inflammation plays a crucial role in the tumorigenesis, progression and survival of patients with HCC.Citation29–31 Cancer-associated inflammation can promote the generation of active oxygen and reactive oxygen and nitrogen, resulting in DNA damage and creating inflammatory tumour microenvironments.Citation32 Eventually, the activation of tumour-related transcription factors and the production of cytokines further promote tumorigenesis and tumour progression.Citation33 Neutrophils and lymphocytes in the primary tumour microenvironment are closely related to local inflammation and immune responses, respectively.Citation34 Thus, they play important regulatory roles in tumour progression. Studies have shown that neutrophils can promote tumour invasion, metastasis and angiogenesis by releasing tumour suppression M, hepatocyte growth factor, neutrophil elastase, and matrix metalloproteins.Citation35 CD4+ T cells and CD8+ T cells are the main components of tumour-infiltrating lymphocytes, which play an important role in the immune response to anticancer activity.Citation36 It is well known that as a routine indicator for evaluating liver function, AST is an enzyme that reflects liver damage and is also used to evaluate the progression of liver disease. Therefore, most scientists believe that the potential mechanism by which these inflammatory markers could predict tumour patient outcomes is that these inflammatory indices could represent the status of systemic inflammation and immune activity in the tumour microenvironment.Citation37
Our research has some advantages. 1) In previous studies on inflammatory biomarkers, continuous values were often converted into categorical variables lacking standard cut-off values.Citation19,Citation38,Citation39 This heterogeneity not only limited the statistical power but also led to incorrect causality, reducing its prognostic predictive ability.Citation40,Citation41 In our study, the continuous variables SIRI and ANRI were used to construct the predictive model to ensure a correct conclusion. 2) Most previous studies focused on one or two inflammatory biomarkers. However, our study explored most of the reported inflammatory biomarkers. 3) Previous studies only explored the prognostic values of inflammatory biomarkers. They did not assess their prognostic capacity in comparison to the current tumour staging systems.Citation20,Citation42,Citation43 In our study, by incorporating inflammatory biomarkers and other clinicopathological factors, we built a simple but reproducible model that had higher prognostic power than common staging systems.
It is undeniable that our research has some limitations. First, our predictive model may not be suitable for all HCC patients. Only patients with HBV-HCC who received curative hepatectomy would fit this model. In addition, this study was based on the experience of large public hospitals in China, so it might not be applicable in all clinical circumstances. Moreover, selection bias was unavoidable because this was a retrospective study with relatively small samples. Larger samples and a prospective study are required in the future to verify our prognostic models and stratification strategies.
In summary, SIRI, ANRI, CNLC stage and microvascular invasion were identified as independent prognostic factors of HBV-HCC after curative surgical resection. A comprehensive and useful nomogram was established and validated, and it could be applied in clinical practice to accurately evaluate RFS and identify high-risk patients.
Conclusion
The novel nomogram incorporating the SIRI and ANRI showed a higher prognostic power for RFS of HCC patients with curative hepatectomy than the CNLC, AJCC 8th edition and BCLC staging systems and may help oncologists identify high-risk HCC patients.
Open Access Statement
The raw data supporting the conclusions of this article will be made available by the corresponding author, without undue reservation.
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation. They took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; had agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors have completed the ICMJE uniform disclosure form and declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Funding
References
- Villanueva A, Longo DL. Hepatocellular Carcinoma. N Engl J Med. 2019;380(15):1450–1462. doi:10.1056/NEJMra1713263
- Choo SP, Tan WL, Goh BKP, Tai WM, Zhu AX. Comparison of hepatocellular carcinoma in Eastern versus Western populations. Cancer. 2016;122(22):3430–3446. doi:10.1002/cncr.30237
- Benson AB, D’Angelica MI, Abbott DE, et al. Hepatobiliary cancers, version 2. 2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19(5):541–565. doi:10.6004/jnccn.2021.0022
- Zhou J, Sun H, Wang Z, et al. Guidelines for the diagnosis and treatment of hepatocellular carcinoma (2019 edition). Liver Cancer. 2020;9(6):682–720. doi:10.1159/000509424
- Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
- European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
- Bruix J, Reig M, Sherman M. Evidence-based diagnosis, staging, and treatment of patients with hepatocellular carcinoma. Gastroenterology. 2016;150(4):835–853. doi:10.1053/j.gastro.2015.12.041
- Ikeda M, Kudo M, Aikata H, et al. Transarterial chemoembolization with miriplatin vs. epirubicin for unresectable hepatocellular carcinoma: a Phase III randomized trial. J Gastroenterol. 2018;53(2):281–290. doi:10.1007/s00535-017-1374-6
- Ishizawa T, Hasegawa K, Aoki T, et al. Neither multiple tumors nor portal hypertension are surgical contraindications for hepatocellular carcinoma. Gastroenterology. 2008;134(7):1908–1916. doi:10.1053/j.gastro.2008.02.091
- Li S, Mei J, Wang Q, et al. Postoperative adjuvant transarterial infusion chemotherapy with FOLFOX could improve outcomes of hepatocellular carcinoma patients with microvascular invasion: a preliminary report of a Phase III, randomized controlled clinical trial. Ann Surg Oncol. 2020;27(13):5183–5190. doi:10.1245/s10434-020-08601-8
- Wei W, Jian PE, Li SH, et al. Adjuvant transcatheter arterial chemoembolization after curative resection for hepatocellular carcinoma patients with solitary tumor and microvascular invasion: a randomized clinical trial of efficacy and safety. Cancer Commun. 2018;38(1):61. doi:10.1186/s40880-018-0331-y
- Kamarajah SK, Frankel TL, Sonnenday C, Cho CS, Nathan H. Critical evaluation of the American Joint Commission on Cancer (AJCC) 8th edition staging system for patients with Hepatocellular Carcinoma (HCC): a Surveillance, Epidemiology, End Results (SEER) analysis. J Surg Oncol. 2018;117(4):644–650. doi:10.1002/jso.24908
- Park S, Choi S, Cho YA, et al. Evaluation of the American Joint Committee on Cancer (AJCC) 8th edition staging system for hepatocellular carcinoma in 1008 patients with curative resection. Cancer Res Treat. 2020;52(4):1145–1152. doi:10.4143/crt.2020.208
- Liao R, Wei XF, Che P, Yin KL, Liu L. Nomograms incorporating the CNLC staging system predict the outcome of hepatocellular carcinoma after curative resection. Front Oncol. 2021;11:755920. doi:10.3389/fonc.2021.755920
- Otto G, Pitton MB, Hoppe-Lotichius M, Weinmann A. Liver transplantation and BCLC classification: limitations impede optimum treatment. Hepatobiliary Pancreat Dis Int. 2021;20(1):6–12. doi:10.1016/j.hbpd.2020.12.009
- Zhou J, Sun HC, Wang Z, et al. Guidelines for diagnosis and treatment of primary liver cancer in China (2017 edition). Liver Cancer. 2018;7(3):235–260. doi:10.1159/000488035
- Vitale A, Farinati F, Finotti M, et al. Overview of prognostic systems for hepatocellular carcinoma and ITA.LI.CA external validation of MESH and CNLC classifications. Cancers. 2021;13(7):1673. doi:10.3390/cancers13071673
- Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-The ALBI grade. J Clin Oncol. 2015;33(6):550–558. doi:10.1200/JCO.2014.57.9151
- Wu Y, Tu C, Shao C. Inflammatory indexes in preoperative blood routine to predict early recurrence of hepatocellular carcinoma after curative hepatectomy. BMC Surg. 2021;21(1):178. doi:10.1186/s12893-021-01180-9
- Wang D, Hu X, Xiao L, et al. Prognostic nutritional index and systemic immune-inflammation index predict the prognosis of patients with HCC. J Gastrointest Surg. 2020;25(2):421–427. doi:10.1007/s11605-019-04492-7
- Qi Q, Zhuang L, Shen Y, et al. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122(14):2158–2167. doi:10.1002/cncr.30057
- Marcoulides KM, Raykov T. Evaluation of variance inflation factors in regression models using latent variable modeling methods. Educ Psychol Meas. 2019;79(5):874–882. doi:10.1177/0013164418817803
- Liao Y, Yin G, Fan X. The Positive lymph node ratio predicts survival in T1-4N1-3M0 non-small cell lung cancer: a nomogram using the SEER database. Front Oncol. 2020;10:1356. doi:10.3389/fonc.2020.01356
- Zheng Z, Guan R, Jianxi W, et al. Microvascular invasion in hepatocellular carcinoma: a review of its definition, clinical significance, and comprehensive management. J Oncol. 2022;2022:9567041. doi:10.1155/2022/9567041
- Zou Y, Chen Z, Lou Q, et al. A novel blood index-based model to predict Hepatitis B virus-associated hepatocellular carcinoma recurrence after curative hepatectomy: guidance on adjuvant transcatheter arterial chemoembolization choice. Front Oncol. 2021;11:755235. doi:10.3389/fonc.2021.755235
- Li SH, Guo ZX, Xiao CZ, et al. Risk factors for early and late intrahepatic recurrence in patients with single hepatocellular carcinoma without macrovascular invasion after curative resection. Asian Pac J Cancer Prev. 2013;14(8):4759–4763. doi:10.7314/APJCP.2013.14.8.4759
- Xu B, Chen Z, Zhang J, et al. Prognostic value of peripheral whole blood cell counts derived indexes in gallbladder carcinoma: a systematic review and meta-analysis. Front Oncol. 2021;11:707742. doi:10.3389/fonc.2021.707742
- Jiang S, Wang S, Wang Q, et al. Systemic Inflammation Response Index (SIRI) independently predicts survival in advanced lung adenocarcinoma patients treated with first-generation EGFR-TKIs. Cancer Manag Res. 2021;13:1315–1322. doi:10.2147/CMAR.S287897
- Colotta F, Allavena P, Sica A, Garlanda C, Mantovani A. Cancer-related inflammation, the seventh hallmark of cancer: links to genetic instability. Carcinogenesis. 2009;30(7):1073–1081. doi:10.1093/carcin/bgp127
- Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–e503. doi:10.1016/S1470-2045(14)70263-3
- Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
- Maeda H, Akaike T. Nitric oxide and oxygen radicals in infection, inflammation, and cancer. Biochemistry. 1998;63(7):854–865.
- Digifico E, Balinzo S, Belgiovine C. The dark side of the force: when the immune system is the fuel of tumor onset. Int J Mol Sci. 2021;22(3):1224. doi:10.3390/ijms22031224
- Qian BZ. Inflammation fires up cancer metastasis. Semin Cancer Biol. 2017;47:170–176. doi:10.1016/j.semcancer.2017.08.006
- Rawat K, Syeda S, Shrivastava A. Neutrophil-derived granule cargoes: paving the way for tumor growth and progression. Cancer Metastasis Rev. 2021;40(1):221–244. doi:10.1007/s10555-020-09951-1
- Klein S, Mauch C, Brinker K, et al. Tumor infiltrating lymphocyte clusters are associated with response to immune checkpoint inhibition in BRAF V600(E/K) mutated malignant melanomas. Sci Rep. 2021;11(1):1834. doi:10.1038/s41598-021-81330-4
- Xie D, Marks R, Zhang M, et al. Nomograms predict overall survival for patients with small-cell lung cancer incorporating pretreatment peripheral blood markers. J Thorac Oncol. 2015;10(8):1213–1220. doi:10.1097/JTO.0000000000000585
- Kim EY, Song KY. The preoperative and the postoperative neutrophil-to-lymphocyte ratios both predict prognosis in gastric cancer patients. World J Surg Oncol. 2020;18(1):293. doi:10.1186/s12957-020-02059-4
- Sun L, Jin Y, Hu W, et al. The impacts of systemic immune-inflammation index on clinical outcomes in gallbladder carcinoma. Front Oncol. 2020;10:554521. doi:10.3389/fonc.2020.554521
- Naggara O, Raymond J, Guilbert F, Roy D, Weill A, Altman DG. Analysis by categorizing or dichotomizing continuous variables is inadvisable: an example from the natural history of unruptured aneurysms. AJNR Am J Neuroradiol. 2011;32(3):437–440. doi:10.3174/ajnr.A2425
- Royston P, Altman DG, Sauerbrei W. Dichotomizing continuous predictors in multiple regression: a bad idea. Stat Med. 2006;25(1):127–141. doi:10.1002/sim.2331
- Shi X, Li F, Xu Y, Nyalali AMK, Li F. The prognostic value of the preoperative inflammatory index on the survival of glioblastoma patients. Neurol Sci. 2022;43(9):5523–5531. doi:10.1007/s10072-022-06158-w
- Liu L, Wang W, Zhang Y, et al. Declined preoperative aspartate aminotransferase to neutrophil ratio index predicts poor prognosis in patients with intrahepatic cholangiocarcinoma after hepatectomy. Cancer Res Treat. 2018;50(2):538–550. doi:10.4143/crt.2017.106