
Abstract
Purpose
This study aimed to explore the relationship between white blood cells (WBCs) at admission and clinical outcomes in patients with aneurysmal subarachnoid hemorrhage (aSAH).
Patients and Methods
We analyzed data from patients with aSAH between January 2015 and September 2021 who were included in the LongTEAM (Long-term Prognosis of Emergency Aneurysmal Subarachnoid Hemorrhage) registry study. WBC is classified into four groups according to the quartile. We used the logistic model for in-hospital complications, mortality, modified Rankin scale (mRS) at discharge and 90 days to examine the relationship between WBC and clinical outcomes. We used WBC levels near odds ratio (OR) = 1 (Q1) in restricted cubic splines as the reference to evaluate whether there is a nonlinear relationship between WBC and clinical outcomes. Another Kaplan–Meier method was used to analyze the relationship between WBC levels and the risk of developing pneumonia.
Results
Of the 988 patients included, the results showed that compared with patients in the Q1 group, patients in the highest quartile (Q4) had an increased incidence of 90-day unfavorable outcomes after adjusting the confounders (adjusted OR = 1.81, 95% CI = 1.02–3.20, p = 0.042), which may be caused by the increased incidence and risk of pneumonia (adjusted OR = 2.06, 95% CI = 1.30–3.29, p = 0.002; adjusted hazard ratio [HR]=1.63, 95% CI = 1.13–2.36, p < 0.001). The restricted cubic spline indicated that the incidence of developing pneumonia and 90-day unfavorable outcomes rises with increasing WBC levels (p for nonlinear = 0.135 and 0.113).
Conclusion
Patients with higher WBC at admission were associated with an increased incidence of 90-day unfavorable outcomes, which might be related to pneumonia.
Introduction
Aneurysmal subarachnoid hemorrhage (aSAH) is a common neurological emergency with high mortality and disability.Citation1,Citation2 Researchers believe early brain injury (EBI) might be responsible for severe complications after aneurysm rupture, leading to poor patient outcomes.Citation3 Within 72 hours after aneurysm rupture, the brain will undergo various pathophysiological events such as energy failure, ionic changes, increased endothelin-1, depletion of nitric oxide, inflammation, oxidative stress, etc.Citation4,Citation5 Among these events, the inflammatory response after bleeding has always been the research hot spot.
Like many other diseases, aSAH has been demonstrated as a state of systemic inflammation and immunosuppression.Citation6 Our previous study developed a prognostic model named “TAPS” for aSAH that included white blood cells (WBCs) at admission, further emphasizing preoperative inflammation’s impact on prognosis.Citation7 WBC is the most abundant immune cell in peripheral blood and can reflect the systemic inflammatory status. Up to now, little is known about how early abnormal WBC levels contribute to unfavorable outcomes, even though three studies indicated that delayed cerebral ischemia (DCI) might be the potential cause.Citation8–10 However, considering the limited clinical evidence available, we hypothesized that other complications could also be involved in the poor prognosis of patients mediated by abnormal WBC levels. Therefore, in this study, we aimed to divide WBC at admission into four groups according to the quartile to analyze the relationship between WBC and different clinical outcomes in aSAH patients.
Materials and Methods
Study Design
All patient data between January 2015 and September 2021 were drawn from the LongTEAM registry study (Registration No. NCT 04785976), a large, single-center, observational cohort conducted at Beijing Tiantan Hospital in China. In this study, all patients had angiographically documented aneurysms with subarachnoid hemorrhage (SAH), which were confirmed by either computed tomography or lumbar puncture. We set the inclusion criteria as follows: (1) age ≥18 years old; (2) emergency admission; (3) single aneurysm; (4) treated with surgical clipping or endovascular coiling; (5) less than 72 hours from the rupture to the admission and less than 72 hours from the admission to treatment; (6) complete 90-day follow-up. The main exclusion criteria were as follows: (1) previous SAH; (2) history of neurosurgery due to any reasons; (3) physical disability due to any previous disease; (4) treatment including external ventricular drainage, lumbar puncture, angiography, intubation, and/or mechanical ventilation at other hospitals before presentation to our hospital; (5) missing data, including medical records, radiological, and laboratory information.
This study was approved by the Institutional Review Board of Beijing Tiantan Hospital (KY 2021–008-01). Informed consent for clinical analysis was obtained from all individual participants or their authorized representatives. All the analysis was performed according to the Declaration of Helsinki and the local ethics policies. All patients were managed according to the guidelines.Citation11
Data Collection
We gathered patient baseline data on (1) demographics, including age and sex; (2) medical history, including hypertension, hyperlipidemia, diabetes mellitus, and heart disease; (3) lifestyle risk factors, including current smoking and drinking; (4) location and size of aneurysm; (5) early seizures, early loss of consciousness; (6) clinical status, including World Federation of Neurological Societies (WFNS) grade; (7) first CT-related information, including modified Fisher scale (mFS), Graeb score, Subarachnoid Hemorrhage Early Brain Edema Score (SEBES), and acute hydrocephalus; (8) laboratory examination, including WBC count (normal range: [3.5–9.5]×109/L), neutrophil-to-lymphocyte ratio (NLR); (9) treatment modality, including surgical clipping and endovascular coiling.
Besides, we collected eleven in-hospital complications such as cardiac event, DCI, intracranial infection, stress ulcer bleeding, urinary tract infection, anemia, hypoproteinemia, pneumonia, muscular calf vein thrombosis (MCVT), deep vein thrombosis (DVT), and lipid metabolism disorder. Supplementary Table 1 shows the detailed diagnostic criteria for the associated complications.
Outcome Assessment
The primary outcome was the modified Rankin scale (mRS) at 90 days after discharge (the neurosurgeon followed up with patients via telephone or an outpatient appointment). We defined the unfavorable outcome as mRS score ≥3. The secondary outcomes were the occurrence of in-hospital complications, mortality at discharge, and unfavorable outcomes at discharge.
Statistical Analysis
WBC was classified into four groups according to the quartile. Categorical variables were presented as percentages and continuous variables as mean with standard deviation (normal distribution) or median with interquartile range (IQR) (skewed distribution). One-way ANOVA with post hoc (Bonferroni correction factor) analysis was applied to compare the baseline characteristics of four groups. The relationship between baseline WBC levels and in-hospital complications, mortality, and outcomes was estimated by a logistic model, using restricted cube bar graphs of WBC levels near odds ratio (OR) = 1 (Q1) as the reference. Adjusted ORs with their 95% confidence intervals (CIs) were estimated for each quartile of the WBC level. For each outcome, two multivariable models were constructed. In Model 1, we only adjusted the variables for age, sex, and treatment modality. In Model 2, we additionally adjusted for early loss of consciousness, WFNS grade 4–5, mFS grade 3–4, Graeb score 5–12, SEBES score 3–4, acute hydrocephalus, and neutrophil-to-lymphocyte ratio.
Besides, we evaluated the pattern and magnitude of associations between the WBC levels at admission and the risk of outcome events by constructing logistic regression models with restricted cubic splines for WBC levels (continuous variable), adjusting for all potential covariates (Model 2). The Q1 of the WBC level was treated as the reference, and five knots for the spline were placed at the WBC level’s 5th, 25th, 50th, 75th, and 95th percentiles.
The hazard ratio (HR) with 95% CI for the Cox regression model was calculated to examine the relationship between WBC levels and the risk of developing in-hospital pneumonia. In addition, subgroup analysis stratified by age (>55 and ≤55 years), sex (male and female), current smoking (yes and no), hypertension (yes and no), WFNS grade (1–3 and 4–5), and treatment modality (surgical clipping and endovascular coiling) were performed to assess whether there was any significant interaction between these factors and WBC levels when analyzing pneumonia and 90-day outcomes.
The analysis was performed with SPSS Statistics 26.0 (IBM, Armonk, New York, USA), R software (Version 4.1.2), and GraphPad PRISM 8.3.0 (GraphPad Software Inc., San Diego, CA, USA). Significance was set at p <0.05.
Results
Study Patients
A total of 988 consecutive patients with aSAH enrolled in the LongTEAM study. Of the patients included, 583 (59.0%) were female patients, and the mean age was 54.8 years old.
The median WBC level was 12.40×109/L ([IQR] 9.87–15.41, 109/L). Patients with higher WBC levels had a higher incidence of early loss of consciousness, higher proportions of WFNS 4–5, mFS 3–4, Graeb 5–12, and SEBES 3–4, a higher rate of acute hydrocephalus, and a higher level of NLR (Shown in ).
Table 1 Baseline Information
WBC Levels and Clinical Outcomes
shows the detailed information about association of WBC and outcomes. There were 376 (38.1%) patients with cardiac events, 268 (27.1%) patients with DCI, 125 (12.7%) patients with intracranial infection, 209 (21.2%) patients with stress ulcer bleeding, 28 (2.8%) patients with urinary tract infection, 315 (31.9%) patients with anemia, 345 (34.9%) patients with hypoproteinemia, 309 (31.3%) patients with pneumonia, 252 (25.5%) patients with MCVT, 85 (8.6%) patients with DVT, 245 (24.8%) patients with lipid metabolism disorder, 16 (1.6%) patients dead at discharge, 416 (42.1%) patients with mRS ≥3 at discharge, and 181 (18.3%) patients with mRS ≥3 at 90 days after discharge.
Table 2 Adjusted Odds Ratios of In-Hospital Complications and Functional Outcomes According to WBC Levels at Admission
After adjusting age, sex, and treatment modality (Model 1), compared with the reference group (Q1), patients in the higher WBC level categories (Q3, Q4) had a higher incidence of DCI (adjusted OR = 1.64, 95% CI = 1.08–2.50, p = 0.021; adjusted OR = 1.99, 95% CI = 1.32–3.02, p = 0.001), patients in the highest WBC level category (Q4) had a higher incidence of hypoproteinemia (adjusted OR = 2.07, 95% CI = 1.39–3.08, p < 0.001), patients in the higher WBC level categories (Q2, Q3, Q4) had a higher incidence of pneumonia (adjusted OR = 1.67, 95% CI = 1.09–2.56, p = 0.019; adjusted OR = 1.91, 95% CI = 1.25–2.91, p = 0.003; adjusted OR = 4.16, 95% CI = 2.75–6.31, p < 0.001), patients in the highest WBC level category (Q4) had a higher incidence of MCVT (adjusted OR = 1.55, 95% CI = 1.01–2.37, p = 0.043), patients in the highest WBC level category (Q4) had a higher incidence of DVT (adjusted OR = 2.01, 95% CI = 1.05–3.85, p = 0.036), patients in the highest WBC level categories (Q4) had a higher proportion of mRS ≥3 at discharge (adjusted OR = 2.72, 95% CI = 1.85–4.00, p < 0.001), and patients in the higher WBC level categories (Q3, Q4) had a higher proportion of mRS ≥3 at 90 days after discharge (adjusted OR = 2.40, 95% CI = 1.43–4.05, p = 0.001; adjusted OR = 4.30, 95% CI = 2.59–7.15, p < 0.001). After further adjustment for related risk factors (Model 2), the highest quartile of WBC level remained associated with an increased risk of pneumonia (adjusted OR = 2.06, 95% CI = 1.30–3.29, p = 0.002), and 90-day unfavorable outcomes (adjusted OR = 1.81, 95% CI = 1.02–3.20, p = 0.042) compared with patients in the Q1 group.
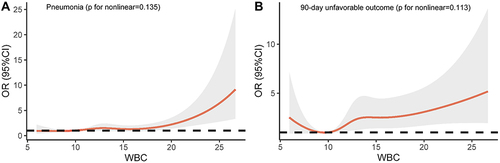
Using logistic regression models with restricted cubic spline, we found that compared with Q1 group, higher levels of WBC were associated with an increased risk of pneumonia (p for nonlinear = 0.135) and 90-day unfavorable outcomes (p for nonlinear = 0.113) (Shown in ).
Figure 1 Adjusted odds ratios of (A) pneumonia and (B) 90-day unfavorable outcomes according to baseline WBC level. The reference is the Q1 of the baseline WBC level (9.87×109/L). Data were fitted using a logistic regression model of the restricted cubic spline with five knots (the 5th, 25th, 50th, 75th, 95th percentiles) for baseline WBC level, adjusting for potential covariates.
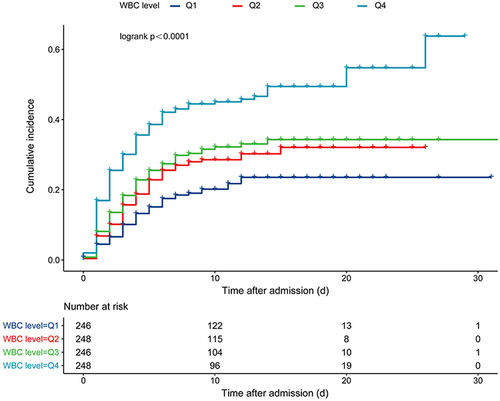
depicts the cumulative incidence of pneumonia by WBC levels. Compared with Q1 group, the adjusted regression model (model 2) suggested that Q4 (adjusted HR = 1.63, 95% CI = 1.13–2.36, p < 0.001) was associated with a higher risk of pneumonia.
Figure 2 Kaplan–Meier curves for in-hospital pneumonia.
Subgroup Analysis
After adjusting for all potential confounding variables according to model 2, subgroup analysis only showed a significant interaction between WBC levels and age when analyzing pneumonia. The effect of WBC levels on the prevalence of pneumonia was stronger in patients with age ≤55 than in those patients with age >55 in the fully adjusted model (p for interaction = 0.040) (Shown in ).
Table 3 Subgroup Analysis of Association Between WBC Groups and In-Hospital Pneumonia
Table 4 Subgroup Analysis of Association Between WBC Groups and 90-Day Outcomes
Time of Developing Pneumonia in Different Groups, and the Relationship Between Pneumonia and Length of Hospital Stay, Number of Complications, and Total Hospital Charges
The median time after admission of developing pneumonia did not differ between patients in the Q1, Q2, Q3, Q4, and overall groups (2.0 [4.0–6.0] vs 3.0 [1.0–5.0] vs 3.0 [1.0–5.0] vs 2.0 [1.0–4.8] vs 3.0 [1.0–5.0], p = 0.223). Compared with patients without pneumonia, patients with pneumonia had longer hospital length of stays (14.0 [11.0–19.0] vs 11.0 [8.0–14.0], p < 0.001), more complications (3.0 [2.0–4.0] vs 2.0 [1.0–3.0], p < 0.001), and more hospital charges (21237 [14759–29501] vs 16094 [11372–23935], p < 0.001) (shown in ).
Figure 3 (A) The timing of pneumonia formation. (B) Relationship between the length of stays and pneumonia. (C) Relationship between the number of complications and pneumonia. (D) Relationship between the total hospital charges and pneumonia (US dollar = 7.11 renminbi [updated on October 10, 2022]).
![Figure 3 (A) The timing of pneumonia formation. (B) Relationship between the length of stays and pneumonia. (C) Relationship between the number of complications and pneumonia. (D) Relationship between the total hospital charges and pneumonia (US dollar = 7.11 renminbi [updated on October 10, 2022]).](/cms/asset/e2a2be68-8058-4e61-a2b7-51bef1845ee4/djir_a_12150264_f0003_c.jpg)
Discussion
The earliest reports describing WBC and outcomes in patients with hemorrhagic stroke can date back to 1987, with two clinical studies illustrating the relationship between WBC and vasospasm and death, respectively.Citation12,Citation13 However, in the following decades, reports on WBC came more frequently from patients with ischemic stroke.Citation14–18 One meta-analysis in 2021 indicated although confirms the association between WBC and unfavorable outcomes in aSAH patients, a strong conclusion cannot be made due to the limitation of the small study number, between-study heterogeneity, and suspicion of uncontrolled factors.Citation19 Therefore, whether WBC at admission can be regarded as a prognostic marker needs more investigation.
In this large observational cohort study conducted in China, we divided WBC levels at admission according to the quartile. We found that the preoperative WBC levels were associated with an increased risk of in-hospital pneumonia and 90-day unfavorable outcomes for aSAH patients. Moreover, such risk rises with increasing WBC levels.
Three previous studies showed that elevated WBC might be associated with the development of DCI during hospitalization, leading to unfavorable outcomes.Citation8–10 There are several mechanisms by which WBC contributes to cerebral injury. On the one hand, the brain will experience early hypoperfusion after an aneurysm rupture, in this period, the capillaries may behave like a sieve and trap the leukocytes to increase the WBC count. Aggregates of WBC adherent to each other can occlude the microcirculation, aggravating tissue hypoperfusion and ischemia injury.Citation20 On the other hand, WBC could release cytotoxic mediators such as some interleukins to increase WBC-endothelial interactions and damage the vessel wall or other viable tissues.Citation21 In our study, when adjusting for age, sex, and treatment modality, the elevated WBC correlates with the development of DCI, but when adjusting for more preoperative confounders, the results showed that elevated WBC appears to be associated only with pneumonia, not DCI. The similar conclusion was addressed in a 2018 study where they considered NLR (also an inflammatory biomarker thought to be associated with the development of DCI) only to be associated with pneumonia rather than DCI after adjusting preoperative confounders.Citation22
We suppose there are several reasons leading to this controversial conclusion. First, is the study population the same? Is there any consideration given to the effect of preoperative grading on DCI? In other words, patients with high-grade aSAH have a higher level of inflammation and a higher probability of developing DCI, and the effect of confounding factors on DCI should be appropriately adjusted. Second, there may be differences in the sensitivity of WBC levels in peripheral blood for predicting DCI compared with local (cerebrospinal fluid), and how the consistency of WBC levels in peripheral blood and cerebrospinal fluid remains to be explored. Third, the time at which WBC was collected may influence the results.
Our previous study indicated that pneumonia might have a long-lasting impact on the prognosis of aSAH patients and is even more devastating than DCI since some DCI is asymptomatic, whereas the development of pneumonia can cause damage to multiple systems throughout the body.Citation23 Another study in 2011 similarly pointed out that pneumonia is a leading cause of poor prognosis in patients with aSAH.Citation24 Fortunately, there are increasing studies focusing on preventing and treating postoperative pneumonia. One study in 2022 revealed that age, WFNS 4–5, heart disease, higher WBC levels, and mFS 3–4 were independent risk factors for pneumonia, and the reason for WBC leading to pneumonia might be due to its ability to reflect the disease severity (patients with high WBC levels had higher WFNS grade and mFS grade at admission, which can prolong the bedridden time and increase the risk of hypostatic pneumonia and aspiration pneumonia).Citation25 Another study in 2022 developed a novel risk score for predicting pneumonia containing WFNS grade, high neutrophil, the need for RBC transfusion, and tracheostomy.Citation26 Besides, NLR, lactate dehydrogenase, and neutrophil-to-albumin ratio were also reported to be associated with pneumonia.Citation27–29
Interestingly, in addition to DCI and pneumonia, the inflammatory response following aSAH can induce hypoproteinemia, leading to muscle dystrophy, of which temporal muscle thickness has been reported to predict patient outcomes, further highlighting the importance of controlling inflammation.Citation30–32 Up to now, we have found many ongoing clinical trials on inflammation, and the interventions used in these clinical trials include dexamethasone, dexmedetomidine, lycopene, hydrogen gas, etc. We look forward to the results of these clinical trials. After all, there are currently very limited measures to improve outcomes in patients with aSAH.
Our study provides evidence for the involvement of WBC after aSAH and highlights the significance of preoperative inflammatory biomarkers for predicting prognosis and complications. As we know, WBC is the most accessible inflammatory indicator regardless of the hospital level. Exploring the relationship between WBC and outcomes can help clinicians better understand the role of inflammatory response in the early brain injury stage.
Limitation
There are several limitations of our study. First, it is unclear whether the patient had a preoperative infection. Second, the conclusions from this study are only based on WBC levels in peripheral blood. Third, the population we studied came from northern China, and it is unclear whether racial differences exist in this phenomenon. Fourth, we did not collect data for daily WBC count in the early hospital course. Fifth, the data used for analysis only include patients with single aneurysms.
Conclusion
In this large, single-center, observational cohort in China, WBC levels at admission were associated with an increased risk of in-hospital pneumonia and 90-day unfavorable outcomes in patients with aSAH. Moreover, such risk rises with increasing WBC levels. Our findings can help clinicians better understand the role of inflammatory response in early brain injury.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
This study has obtained approval from the Institutional Review Board of Beijing Tiantan Hospital (KY 2021-008-01). Informed consent for clinical analysis was obtained from all individual participants or their authorized representatives. All the analysis was performed according to the Declaration of Helsinki and the local ethics policies.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have no personal, financial, or institutional interest in any of the materials or methods used in this study or the findings specified in this paper.
Acknowledgments
We acknowledge the contribution of all staff who participated in the present study.
Additional information
Funding
References
- Uhl C, Huscher D, Sommerfeld J, Schönberg B, Vajkoczy P, Dengler N. Aneurysmal subarachnoid hemorrhage in Germany between 2005 and 2018: a nationwide observational study. Eur J Neurol. 2022;29:3009–3016. doi:10.1111/ene.15457
- Lovelock C, Rinkel G, Rothwell P. Time trends in outcome of subarachnoid hemorrhage: population-based study and systematic review. Neurology. 2010;74(19):1494–1501. doi:10.1212/WNL.0b013e3181dd42b3
- Fujii M, Yan J, Rolland W, Soejima Y, Caner B, Zhang J. Early brain injury, an evolving frontier in subarachnoid hemorrhage research. Transl Stroke Res. 2013;4(4):432–446. doi:10.1007/s12975-013-0257-2
- Sehba F, Friedrich V. Early events after aneurysmal subarachnoid hemorrhage. Acta Neurochir Suppl. 2015;120:23–28. doi:10.1007/978-3-319-04981-6_4
- Suzuki H. What is early brain injury? Transl Stroke Res. 2015;6(1):1–3. doi:10.1007/s12975-014-0380-8
- Saand AR, Yu F, Chen J, Chou SH. Systemic inflammation in hemorrhagic strokes - A novel neurological sign and therapeutic target? J Cereb Blood Flow Metab. 2019;39(6):959–988. doi:10.1177/0271678X19841443
- Li R, Lin F, Chen Y, et al. A 90-day prognostic model based on the early brain injury indicators after aneurysmal subarachnoid hemorrhage: the TAPS Score. Transl Stroke Res. 2022. doi:10.1007/s12975-022-01033-4
- Al-Mufti F, Misiolek K, Roh D, et al. White blood cell count improves prediction of delayed cerebral ischemia following aneurysmal subarachnoid hemorrhage. Neurosurgery. 2019;84(2):397–403. doi:10.1093/neuros/nyy045
- Kasius K, Frijns C, Algra A, Rinkel G. Association of platelet and leukocyte counts with delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage. Cerebrovasc Dis. 2010;29(6):576–583. doi:10.1159/000306645
- Mahta A, Azher A, Moody S, et al. Association of early white blood cell trend with outcomes in aneurysmal subarachnoid hemorrhage. World Neurosurg. 2021;151:e803–e809. doi:10.1016/j.wneu.2021.04.124
- Connolly E, Rabinstein A, Carhuapoma J, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012;43(6):1711–1737. doi:10.1161/STR.0b013e3182587839
- Maiuri F, Gallicchio B, Donati P, Carandente M. The blood leukocyte count and its prognostic significance in subarachnoid hemorrhage. J Neurosurg Sci. 1987;31(2):45–48.
- Di Piero V, Bastianello S. Prognostic value of peripheral white blood cell count in intracerebral hemorrhage. Stroke. 1987;18(5):957. doi:10.1161/str.18.5.957a
- Zimmermann L, Pham M, März A, Kollikowski A, Stoll G, Schuhmann M. Defining cerebral leukocyte populations in local ischemic blood samples from patients with hyperacute stroke. J Cereb Blood Flow Metab. 2022;42(5):901–904. doi:10.1177/0271678x221078617
- Tarkanyi G, Karadi Z, Szabo Z, Szegedi I, Csiba L, Szapary L. Relationship between leukocyte counts and large vessel occlusion in acute ischemic stroke. BMC Neurol. 2020;20(1):440. doi:10.1186/s12883-020-02017-3
- Chen J, Zhang F, Lv S, et al. Association of admission leukocyte count with clinical outcomes in acute ischemic stroke patients undergoing intravenous thrombolysis with recombinant tissue plasminogen activator. Curr Neurovasc Res. 2020;17(5):660–666. doi:10.2174/1567202617999201125201616
- Semerano A, Strambo D, Martino G, et al. Leukocyte counts and ratios are predictive of stroke outcome and hemorrhagic complications independently of infections. Front Neurol. 2020;11:201. doi:10.3389/fneur.2020.00201
- Malhotra K, Goyal N, Chang J, et al. Differential leukocyte counts on admission predict outcomes in patients with acute ischaemic stroke treated with intravenous thrombolysis. Eur J Neurol. 2018;25(12):1417–1424. doi:10.1111/ene.13741
- Ma X, Lan F, Zhang Y. Associations between C-reactive protein and white blood cell count, occurrence of delayed cerebral ischemia and poor outcome following aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis. Acta Neurol Belg. 2021;121(5):1311–1324. doi:10.1007/s13760-020-01496-y
- Schmid-Schnbein GW. Capillary hugging by granulocytes and the no-reflow phenomenon in the microcirculation. Fed Proc. 1987;46(7):2397–2401.
- Harlan JM. Leukocyte-endothelial interactions. Blood. 1985;65(3):513–525. doi:10.1182/blood.V65.3.513.513
- Giede-Jeppe A, Reichl J, Sprügel M, et al. Neutrophil-to-lymphocyte ratio as an independent predictor for unfavorable functional outcome in aneurysmal subarachnoid hemorrhage. J Neurosurg. 2019;132(2):400–407. doi:10.3171/2018.9.Jns181975
- Li R, Lin F, Chen Y, et al. In-hospital complication-related risk factors for discharge and 90-day outcomes in patients with aneurysmal subarachnoid hemorrhage after surgical clipping and endovascular coiling: a propensity score-matched analysis. J Neurosurg. 2021:1–12. doi:10.3171/2021.10.Jns211484
- Vergouwen M, Fang J, Casaubon L, et al. Higher incidence of in-hospital complications in patients with clipped versus coiled ruptured intracranial aneurysms. Stroke. 2011;42(11):3093–3098. doi:10.1161/strokeaha.111.619510
- Yuan K, Li R, Zhao Y, et al. Pre-operative predictors for post-operative pneumonia in aneurysmal subarachnoid hemorrhage after surgical clipping and endovascular coiling: a single-center retrospective study. Front Neurol. 2022;13:893516. doi:10.3389/fneur.2022.893516
- Wang R, Zhang J, He M, Xu J. A novel risk score for predicting hospital acquired pneumonia in aneurysmal subarachnoid hemorrhage patients. Int Immunopharmacol. 2022;108:108845. doi:10.1016/j.intimp.2022.108845
- Chen Y, Lian B, Peng L, et al. Neutrophil to lymphocyte ratio is a prognosis factor for post-operative pneumonia in aneurysmal subarachnoid hemorrhage patients. Chin Med J. 2020;134(6):682–689. doi:10.1097/cm9.0000000000001304
- Ding C, Peng L, Lin Y, Yu L, Wang D, Kang D. Elevated lactate dehydrogenase level predicts postoperative pneumonia in patients with aneurysmal subarachnoid hemorrhage. World Neurosurg. 2019;129:e821–e830. doi:10.1016/j.wneu.2019.06.041
- Zhang X, Zhang S, Wang C, Liu R, Li A. High neutrophil-to-albumin ratio predicts postoperative pneumonia in aneurysmal subarachnoid hemorrhage. Front Neurol. 2022;13:840858. doi:10.3389/fneur.2022.840858
- Onodera H, Mogamiya T, Matsushima S, et al. High protein intake after subarachnoid hemorrhage improves oral intake and temporal muscle volume. Clin Nutr. 2021;40(6):4187–4191. doi:10.1016/j.clnu.2021.01.040
- Katsuki M, Kakizawa Y, Nishikawa A, et al. Temporal muscle and stroke-A narrative review on current meaning and clinical applications of temporal muscle thickness, area, and volume. Nutrients. 2022;14(3):687. doi:10.3390/nu14030687
- Katsuki M, Yamamoto Y, Uchiyama T, Wada N, Kakizawa Y. Clinical characteristics of aneurysmal subarachnoid hemorrhage in the elderly over 75; would temporal muscle be a potential prognostic factor as an indicator of sarcopenia? Clin Neurol Neurosurg. 2019;186:105535. doi:10.1016/j.clineuro.2019.105535