
Abstract
Purpose
The fibrinogen-to-albumin ratio (FAR) is a novel inflammation marker associated with various diseases. This study aimed to investigate the correlation between FAR and early neurological deterioration (END) after intravenous thrombolysis (IVT) in patients with acute ischemic stroke (AIS).
Patients and Methods
From September 1, 2021, to March 31, 2023, continuously recruited AIS patients who received IVT within 4.5 hours were included in the study. Blood samples were collected in the emergency room before IVT. The National Institutes of Health Stroke Scale (NIHSS) score was assessed upon admission and after thrombolysis within the first 24 hours. END was defined as an increase in the NIHSS score by ≥ 4 points within 24 hours after thrombolysis. Multivariate logistic regression analysis was conducted to explore the relationship between FAR and END, and a receiver operating characteristic (ROC) curve was used to evaluate the predictive ability of FAR for END.
Results
343 participants were recruited, and 59 (17.2%) experienced END. Patients with END had higher FAR levels than those without END (P<0.001). Multivariate logistic regression analysis showed that FAR was independently associated with END, both as a continuous variable and as a tertile variable (P<0.005). After excluding patients with hemorrhagic transformation (HT), FAR remained independently associated with END (P<0.005). The area under the curve (AUC) of FAR for predicting END was 0.650 (95% CI=0.571–0.729, P<0.001), with an optimal cutoff of 72.367 mg/g, a sensitivity of 61.6%, and a specificity of 62.6%.
Conclusion
FAR upon admission was independently associated with END after IVT and can be an effective predictor.
Introduction
According to the Global Burden of Disease Study 2019, stroke remained the second-leading cause of death and the third-leading cause of death and disability combined worldwide.Citation1 Intravenous thrombolysis (IVT) with recombinant tissue plasminogen activator (rt-PA) was recommended as the standard and effective treatment for acute ischemic stroke within 4.5 hours after onset.Citation2 However, there are still some patients who will suffer early neurological deterioration (END) after IVT, with a prevalence of more than 10%.Citation3 END was defined as a National Institutes of Health Stroke Scale (NIHSS) score increase of ≥ 4 within 24 h after thrombolysis.Citation4 END is closely related to poor prognosis, so it is essential to seek early predictive markers.
Inflammatory response plays an essential role in ischemic stroke, which has an impact on the poor prognosis.Citation5 Fibrinogen is a systemic inflammatory marker critical in platelet activation and blood viscosity.Citation6 Albumin is a negative inflammation biomarker with anti-inflammatory and anti-oxidative effects.Citation7 Recently, the fibrinogen-to-albumin ratio (FAR) has been reported to be a novel inflammation marker associated with many diseases. Studies have shown that FAR has a predictive effect on the prognosis of a variety of tumors, such as breast cancer, pancreatic cancer, and gallbladder cancer.Citation8–10 Meanwhile, FAR was also reported to be closely related to the severity and prognosis of acute coronary syndrome.Citation11 In recent years, studies have reported that FAR is associated with poor prognosis of lacunar infarction, pontine infarction, and hemorrhagic transformation (HT) after IVT in ischemic stroke patients.Citation12–14 Nevertheless, the correlation between FAR and END after IVT has not been reported. Therefore, we designed this prospective study to explore the association of FAR with END and 3-month outcomes in patients receiving IVT with rt-PA.
Materials and Methods
Study Participants
This prospective observational study was conducted from January 2021 to June 2023. AIS patients undergoing IVT within 4.5h were continuously recruited from the First People’s Hospital of Yancheng. Eligible patients who met the criteria were enrolled in the final Analysis. The Inclusion criteria were: 1. admission within 4.5h after onset; 2. treated with intravenous thrombolysis with rt-PA; 3. eighteen years or older. Exclusion criteria included: 1. with severe inflammatory or infectious diseases; 2. with tumors, liver disease, autoimmune disease, and renal failure; 3. patients underwent further endovascular treatment; 4. Incomplete clinical data: The study was approved by the Ethics Committee of the First People’s Hospital of Yancheng, and written informed consent was obtained from all patients or their representatives before inclusion in the study.
Clinical and Laboratory Measurements
On admission, the baseline characteristics were collected, including demographic information (gender, age, body mass index [BMI]), medical history (hypertension, diabetes mellitus [DM], atrial fibrillation, prior stroke, current smoking or drinking and coronary artery disease), medication use history (previous antiplatelet, previous anticoagulation, and previous statin), clinical assessment (blood pressure, baseline National Institutes of Health Stroke Scale [NIHSS] score, stroke etiology, infarction location, onset to treatment time [OTT], proximal arterial occlusion [PAO], hemorrhagic transformation [HT]). Blood samples were collected in the emergency room before intravenous thrombolysis. All samples were processed in the hospital’s laboratory department by a technician blinded to the clinical data. Laboratory data include fibrinogen, albumin, total cholesterol (TC), triglyceride (TG), fasting plasma glucose (FPG), and glycosylated hemoglobin A1 (HbA1c).
Infarction location, HT, and PAO were evaluated by magnetic resonance, computed tomography (CT), CT angiography, or carotid ultrasound. The infarct location was divided into anterior circulation infarction and posterior circulation infarction (POCI). Stroke etiology was classified according to the Trial of Org 10,172 in Acute Stroke Treatment (TOAST) criteria.
Definitions
The NIHSS score was performed by two trained neurologists blind to our study on admission and repeated three times during the first 24 hours after thrombolysis. The END was defined as an increase in the NIHSS score by ≥ 4 points within 24 hours after thrombolysis.Citation4 In case of disagreement about the NIHSS score evaluation, a third neurologist was invited to make a final decision.
Statistical Analysis
Statistical analyses were performed using SPSS version 23.0 (IBM, New York, NY, USA). All participants were categorized into three groups based on tertiles of FAR and divided into END and non-END groups according to post-thrombolysis early neurological outcomes. Continuous variables were presented as means ± standard deviation or median (25% and 75% interquartile), while categorical variables were shown as n (%). Differences in baseline demographic and clinical characteristics between END and non-END groups were conducted using the independent Student’s t-test, one-way ANOVA or the Mann–Whitney U-test for continuous variables, and the chi-squared or Fisher’s exact test for categorical variables. Differences in baseline characteristics among tertiles of FAR were compared using analysis of variance or the Kruskal–Wallis test for continuous variables and the chi-square test for categorical variables. Univariable logistic regression analysis was conducted to investigate the risk factors of END. Multivariable logistic regression analysis adjusted for variables with a p < 0.1 in the univariable analysis was performed. An association was indicated as the odds ratio (OR) or adjusted odds ratio (aOR) with the 95% confidence interval (CI). In addition, the ROC curve was performed to assess the predictive value of FAR for post-thrombolysis END. Statistical significance was defined as a two-sided P-value of< 0.05.
Results
From September 2021 to March 2023, 484 AIS patients who received intravenous thrombolytic therapy were screened in this study. Among them, 107 patients were excluded for various reasons according to the exclusion criteria, and 34 patients did not complete the subsequent assessments during the 24 hours after thrombolysis. Finally, 343 participants with a median age of 68 were recruited, and 210 (61.2%) were male. Eventually, post-thrombolysis END was observed in 59 (17.2%) patients. The FAR was stratified by tertile, and the tertile levels were as follows: Tertile 1 (12.554≤SII<58.586), Tertile 2 (58.586≤SII<78.378), Tertile 3 (78.378≤SII≤342.213).
Baseline Characteristics Between END and Non-END Groups
In this study, 59 (17.2%) patients finally suffer from END. All participants were divided into the END group and the non-END group. shows the baseline characteristics of the patients in the two subgroups. The results suggested that patients in the END group had higher levels of age(P=0.005), NIHSS (P=0.009), fibrinogen (P=0.003), FAR (P<0.001), and higher proportions of PAO (P=0.005), HT (P<0.001) and lower levels of albumin (P<0.001). In comparison, other characteristics demonstrated no significant differences.
Table 1 Characteristics Between END Group and Non-END Group
Correlation Between FAR and END
The results of logistic regression analyses for END with FAR as continuous variables and tertiles were displayed in and , respectively. The univariate logistic regression analysis suggested that age, NIHSS on admission, PAO, HT, fibrinogen, albumin, and FAR were associated with END (all P<0.05). Subsequently, multiple regression analysis was performed, and fibrinogen was eliminated due to collinearity. The multivariate regression analysis, which was adjusted for variables with P<0.1 in univariate regression analysis, demonstrated that age (OR=1.040, 95% CI=1.008–1.073, P=0.013), SBP (OR=0.987, 95% CI=0.974–1.000, P=0.044), HT (OR=7.352, 95% CI=2.103–25.700, P=0.002) as well as FAR (OR=1.016, 95% CI=1.005–1.027, P=0.001) were independently associated with END (). Furthermore, FAR was then entered as tertiles in the multiple regression analysis. The results indicated that when the first tertile of FAR was used as the reference, the third tertile was identified as an independent factor of END (OR=2.653, 95% CI=1.117–6.301, P=0.027) ().
Table 2 Univariate and Multivariate Analyses for the Potential Risk Factors Associated with END, Including FAR as Continuous Variables by Logistic Regression
Table 3 Multivariate Analyses for the Potential Risk Factors Related to END, Including FAR as Tertiles by Logistic Regression
Associations of FAR and END in Patients Without HT
Similar patterns of association between FAR and END persisted after excluding subjects with HT. The regression analysis results suggested that FAR was still an independent risk factor for END in the non-HT population, whether as a continuous variable or tertile ( and ).
Table 4 Multivariate Analyses for the Potential Risk Factors Related to END, Including FAR as Continuous Variables in Patients Without HT
Table 5 Multivariate Analyses for the Potential Risk Factors Related to END, Including FAR as Tertiles in Patients Without HT
ROC Analysis to Evaluate the Predictive Value of FAR for PSCI
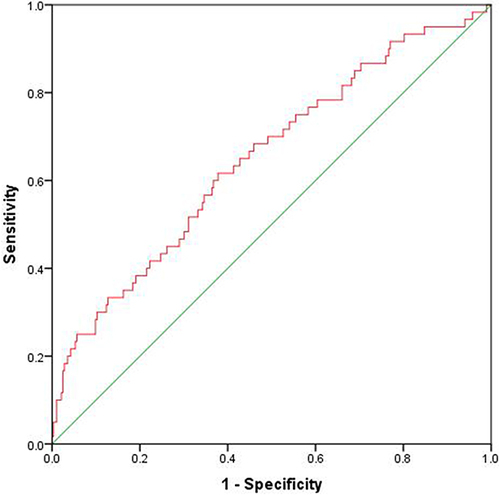
ROC analysis was conducted to assess the predictive value of FAR for END (). The AUC of FAR for predicting END was 0.650 (95% CI=0.571–0.729, P<0.001). The optimal cutoff value was ≥72.367 mg/g, with a sensitivity of 61.6% and a specificity of 62.6%.
Figure 1 ROC curve for evaluating the predictive value of FAR for END after IVT.
Discussion
This study is the first to report the association of FAR with early neurological deterioration in patients with ischemic stroke treated with intravenous thrombolysis. The current study found that FAR was independently associated with END, even when patients with HT were excluded.
Early opening of the occluded vessels was the main treatment for acute ischemic stroke (AIS), and IVT with rt-PA is an effective treatment option for AIS within 4.5h.Citation2,Citation15 Although IVT reduces mortality and improves functional outcomes in AIS patients, about one in seven thrombolysis patients still suffer from END.Citation16 Therefore, early prediction and intervention of END are critical to improve the prognosis of these patients. The causes of END include symptomatic intracranial hemorrhage (sICH), malignant edema, early recurrent ischemic stroke (ERIS), and early seizures.Citation3,Citation17 In addition to the above causes, about half of END after IVT occurred without clear cause.Citation18 Inflammation plays an essential role in the pathological process of AIS and is considered to be associated with END and poor prognosis of stroke.Citation19,Citation20 Ischemic stroke can induce a robust inflammatory response, which in turn aggravates secondary brain damage by exacerbating blood-brain barrier damage, microvascular injury, oxidative stress, brain edema, and by directly evoking neurocyte death.Citation5,Citation19
Fibrinogen, a plasmatic coagulation factor synthesized by the liver, is an essential determinant of blood viscosity and platelet activation. Meanwhile, it is also an acute-phase protein that plays a role in the pathophysiological process of inflammation.Citation21 Many studies have shown that fibrinogen is an inflammatory marker closely related to ischemic stroke.Citation21,Citation22 High levels of fibrinogen can increase the risk of ischemic stroke, and a recent meta-analysis reported that the risk of ischemic stroke increased by 1.47 times in patients with higher fibrinogen levels.Citation23 Fibrinogen is also regarded as a predictor of poor prognosis in ischemic stroke. According to a large sample clinical study in China, both increased baseline and 90-day fibrinogen levels were associated with poor outcomes in patients with ischemic stroke or transient ischemic attack (TIA).Citation24 Elevated plasma fibrinogen could indicate short-term poor outcomes for patients with AIS receiving IVT, but decreased fibrinogen level was independently associated with HT.Citation25 Furthermore, a few studies have also demonstrated that the higher plasma fibrinogen level at admission could be used as an effective predictor of post-stroke depression and cognitive impairment.Citation26–28 Recently, A clinical study on the Indian population showed that fibrinogen was independently associated with END and poor hospital outcomes in patients with AIS.Citation28
Albumin is the most abundant plasma protein with many physiological functions. As a negative inflammation biomarker, It can also play an important role in antioxidant, antithrombotic, and protecting vascular endothelium.Citation29,Citation30 Many studies have demonstrated a close association between serum albumin levels and ischemic stroke.Citation31,Citation32 Xu et al have reported that low serum albumin was a risk factor for ischemic stroke.Citation33 In recent years, a growing body of research has revealed that albumin could predict poor functional outcomes and mortality in patients with AIS.Citation32 A large-sample prospective study recently confirmed that low serum albumin levels in patients with AIS or TIA were closely associated with poor functional outcomes and mortality at three months and one year.Citation31 In addition, several pre-clinical studies have reported that albumin could exert neuroprotective effects by reducing infarct volume and brain swelling.Citation34,Citation35 This suggests that albumin might have a potential therapeutic value for ischemic stroke. In this study, patients with END had a lower albumin level, but low albumin was not an independent risk factor for END.
Both plasma fibrinogen and albumin are effective inflammatory biomarkers closely related to ischemic stroke. The new parameter FAR, consisting of fibrinogen and albumin, is a better indicator of an inflammatory state than fibrinogen and albumin alone.Citation36 As a promising inflammatory biomarker, FAR has been reported to be a valid predictor of the prognosis of a variety of tumors, such as esophagus cancer, gallbladder cancer, breast cancer, and pancreatic cancer.Citation8–10 Furthermore, FAR has also been proven to be independently associated with the severity and prognosis of coronary artery disease (CAD).Citation37 Karahan O et al reported that FAR was strongly related to the severity of CAD in patients with ST-segment elevation myocardial infarction (STEMI).Citation38 Recently, a large observational study with a 5-year follow-up found that a higher FAR combined with DM was associated with worse 5-year outcomes in patients with CAD undergoing percutaneous coronary intervention (PCI).Citation36 In addition, growing evidence has confirmed the correlation between FAR and ischemic stroke. Ruan Y et al reported that high FAR could significantly increase the risk of HT in AIS patients.Citation13 Further, Yang M et al found that FAR was also independently associated with HT after IVT in AIS patients.Citation39 In addition, some studies have demonstrated that FAR could be used as a predictor of the prognosis of certain ischemic stroke types. For example, a clinical study by Zheng L et al showed that high FAR on admission independently correlated with clinical outcomes three months after lacunar stroke.Citation14 Another recent survey of patients with acute pontine infarction proved that high FAR was a valid predictor of a poor outcome at three months.Citation12
However, there are insufficient publications on the relationship between FAR and END. In this study, we confirmed the association of FAR with END after IVT. Interestingly, we found that HT was independently associated with END, but FAR remained an independent risk factor for END in patients without HT. This indicated that the positive effect of FAR on END might not be due to its ability to increase the risk of HT. The underlying mechanisms between FAR and END after IVT remain unclear. We suspected this might result from an interaction between the higher fibrinogen and lower albumin levels, and the following mechanisms might play a role. First, as a composite index combining coagulation and nutritional information, FAR can effectively reflect systemic inflammation and hypercoagulable state, leading to END and AIS progression.Citation8,Citation13 Second, as mentioned above, fibrinogen is associated with oxidative stress. At the same time, albumin has an anti-oxidative stress effect, so FAR can indirectly reflect oxidative stress and endothelial dysfunction, contributing to the END of AIS.Citation6,Citation7 Third, high fibrinogen levels may increase blood viscosity, aggravate microcirculation disturbance in ischemic penumbra, and lead to END.Citation6,Citation14,Citation18 Furthermore, albumin plays an important role in maintaining the integrity of the blood-brain barrier. Low albumin levels can increase the risk of brain edema and HT after IVT, thereby inducing END.Citation31,Citation33 To further understand the mechanisms underlying the association between FAR and END after IVT in ischemic stroke patients, more research is needed.
The correlation between FAR and END and the predictive effect of FAR on END after IVT proved significant, but the sensitivity and specificity were low in this study. This low sensitivity and specificity might be due to the limited sample size and strict enrollment criteria. Moreover, the heterogeneity of the patient population and the difference between FAR measurement time and stroke onset time might also play a role. We supposed that the study design of multi-center and large samples and the dynamic detection of FAR at multiple time points might help to improve the sensitivity and specificity. If the validity of FAR in predicting END could be sufficiently confirmed, it may open the door to consider various cerebral protective measures. This could include the development of new therapeutic approaches designed to modify FAR levels treatments aimed at reducing fibrinogen levels or strategies to increase albumin levels. Furthermore, Due to the close association between FAR and inflammation, appropriate treatment to reduce inflammatory response can be considered for high-risk patients. However, at this stage, the correlation between FAR and END after IVT does not seem strong enough to redirect treatment.
Our study provides epidemiological evidence that FAR is a valid predictor of END after IVT for the first time. However, some limitations should be pointed out. First, Our study was a single-center study with a small sample size, which multi-center studies with large samples must further confirm. Second, only the baseline FAR was collected, and the dynamic FAR was not continuously recorded. Third, because of the limited sample size, we did not subgroup END according to the underlying causes, which would have helped to explore potential mechanisms further. Fourth, the correlation between FAR and END and its predictive value were significant but weak in this study, and more studies were needed to verify it.
Conclusion
Our study showed that a high level of FAR was independently associated with END and could be used as a potential predictor. Further exploration of its potential mechanism might help to provide new targets for the early prevention and intervention of END.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of The First People’s Hospital of Yancheng. This study was in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants or their families before this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We express our gratitude to all the patients who participated in this study.
Data Sharing Statement
We declare that all the data in this article are authentic, valid, and available from Yongjun Cao for reasonable request.
Additional information
Funding
References
- Islam SMS, Uddin R, Ball K, et al. The burden and trend of diseases and their risk factors in Australia, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2023;8(8):e585–99. doi:10.1016/S2468-2667(23)00123-8
- Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359(13):1317–1329. doi:10.1056/NEJMoa0804656
- Seners P, Turc G, Oppenheim C, Baron JC. Incidence, causes and predictors of neurological deterioration occurring within 24 h following acute ischaemic stroke: a systematic review with pathophysiological implications. J Neurol Neurosurg Psychiatry. 2015;86(1):87–94. doi:10.1136/jnnp-2014-308327
- Siegler JE, Martin-Schild S. Early Neurological Deterioration (END) after stroke: the END depends on the definition. Int J Stroke. 2011;6:211–212. doi:10.1111/j.1747-4949.2011.00596.x
- Shi K, Tian D, Li Z, Ducruet AF, Lawton MT, Shi F. Global brain inflammation in stroke. Lancet Neurol. 2019;18:1058–1066. doi:10.1016/S14744422(19)30078-X
- Han L, Wang Z, Yuan J, et al. Circulating leukocyte as an inflammatory biomarker: association with fibrinogen and neuronal damage in acute ischemic stroke. J Inflamm Res. 2023;16:1213–1226. doi:10.2147/JIR.S399021
- Xu T, Xia L, Wu Y, et al. High ratio of c-reactive protein to albumin is associated with hemorrhagic transformation and poor functional outcomes in acute ischemic stroke patients after thrombolysis. Front Aging Neurosci. 2023;15:1109144. doi:10.3389/fnagi.2023.1109144
- Fang L, Yan FH, Liu C, et al. Systemic inflammatory biomarkers, especially fibrinogen to albumin ratio, predict prognosis in patients with pancreatic cancer. Cancer Res Treat. 2021;53(1):131–139. doi:10.4143/crt.2020.330
- Xu WY, Zhang HH, Xiong JP, et al. Prognostic significance of the fibrinogen-to-albumin ratio in gallbladder cancer patients. World J Gastroenterol. 2018;24(29):3281–3292. doi:10.3748/wjg.v24.i29.3281
- Hwang KT, Chung JK, Roh EY, et al. Prognostic influence of preoperative fibrinogen to albumin ratio for breast cancer. J Breast Cancer. 2017;20(3):254–263. doi:10.4048/jbc.2017.20.3.254
- Chen C, Lu C, Liu W, et al. Association between fibrinogen/albumin ratio and arterial stiffness in patients with type 2 diabetes: a cross-sectional study. Front Pharmacol. 2023:13. doi:10.3389/fphar.2022.1120043
- Zhai M, Cao S, Lu J, Xu H, Xia M, Li Z. The relationship between the fibrinogen to albumin ratio and early outcomes in patients with acute pontine infarction. Clin Appl Thromb Hemost. 2022;28:1319718532. doi:10.1177/10760296211067260
- Ruan Y, Yuan C, Liu Y, et al. High fibrinogen-to-albumin ratio is associated with hemorrhagic transformation in acute ischemic stroke patients. Brain Behav. 2021;11(1):e1855. doi:10.1002/brb3.1855
- Zheng L, Wang Z, Liu J, et al. Association between admission blood fibrinogen-to-albumin ratio and clinical outcomes after acute lacunar stroke. Biomarker Med. 2021;15(2):87–96. doi:10.2217/bmm-2019-0537
- Berge E, Whiteley W, Audebert H, et al. European stroke organisation (eso) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur Stroke J. 2021;6(1):I–LXII. doi:10.1177/2396987321989865
- Seners P, Ben Hassen W, Lapergue B, et al. Prediction of early neurological deterioration in individuals with minor stroke and large vessel occlusion intended for intravenous thrombolysis alone. JAMA Neurol. 2021;78(3):321–328. doi:10.1001/jamaneurol.2020.4557
- Seners P, Turc G, Tisserand M, et al. Unexplained early neurological deterioration after intravenous thrombolysis. Stroke. 2014;45(7):2004–2009. doi:10.1161/STROKEAHA.114.005426
- Tisserand M, Seners P, Turc G, et al. Mechanisms of unexplained neurological deterioration after intravenous thrombolysis. Stroke. 2014;45(12):3527–3534. doi:10.1161/STROKEAHA.114.006745
- Esenwa CC, Elkind MS. Inflammatory risk factors, biomarkers and associated therapy in ischaemic stroke. Neurology. 2016;12(10):594–604. doi:10.1038/nrneurol.2016.125
- Parikh NS, Merkler AE, Iadecola C. Inflammation, autoimmunity, infection, and stroke. Stroke. 2020;51(3):711–718. doi:10.1161/STROKEAHA.119.024157
- Barakzie A, Jansen AJG, Ten Cate H, de Maat MPM. Coagulation biomarkers for ischemic stroke. Res Pract Thromb Haemost. 2023;7(4):100160. doi:10.1016/j.rpth.2023.100160
- Swarowska M, Polczak A, Pera J, Klimkowicz-Mrowiec A, Slowik A, Dziedzic T. Hyperfibrinogenemia predicts long-term risk of death after ischemic stroke. J Thromb Thrombolysis. 2014;38(4):517–521. doi:10.1007/s11239-014-1122-1
- Prasad MK, Marandi S, Mishra B, et al. Association of fibrinogen with ischemic stroke: a systematic review and meta-analysis. Cureus. 2023;15(1):e34335. doi:10.7759/cureus.34335
- Hou HQ, Xiang XL, Pan YS, et al. Baseline or 90-day fibrinogen levels and long-term outcomes after ischemic stroke or tia: results from the China national stroke registry iii. Atherosclerosis. 2021;337:35–41. doi:10.1016/j.atherosclerosis.2021.10.002
- Li D, Xing C, Li Y, Zhu X. Elevated plasma fibrinogen indicates short-term poor outcome in patients with acute ischemic stroke after intravenous thrombolysis. J Stroke Cerebrovascular Dis. 2020;29(8):104991. doi:10.1016/j.jstrokecerebrovasdis.2020.104991
- Liu Y, Chen H, Zhao K, He W, Lin S, He J. High levels of plasma fibrinogen are related to post‐stroke cognitive impairment. Brain Behav. 2019;9(10). doi:10.1002/brb3.1391
- Zhu J, Wang L, Shao H, et al. Higher plasma fibrinogen level at admission is associated with post-stroke depression at discharge. Brain Sci. 2022;12(8):1032. doi:10.3390/brainsci12081032
- Mehta V, Sharma A, Jyoti D, et al. Fibrinogen as a predictor of early neurological deterioration in acute ischemic stroke – evidence from the Indian population. J Cent Nerv Syst Dis. 2023;15:370494219. doi:10.1177/11795735231156349
- Huang Y, Xiao Z. Albumin therapy for acute ischemic stroke: a meta-analysis. Neurol Sci. 2021;42(7):2713–2719. doi:10.1007/s10072-021-05244-9
- Cabrerizo S, Cuadras D, Gomez-Busto F, Artaza-Artabe I, Marín-Ciancas F, Malafarina V. Serum albumin and health in older people: review and meta-analysis. Maturitas. 2015;81(1):17–27. doi:10.1016/j.maturitas.2015.02.009
- Zhou H, Wang A, Meng X, et al. Low serum albumin levels predict poor outcome in patients with acute ischaemic stroke or transient ischaemic attack. Stroke Vasc Neurol. 2021;6(3):458–466. doi:10.1136/svn-2020-000676
- Mangoni AA, Zinellu A. A systematic review and meta-analysis of serum concentrations of ischaemia-modified albumin in acute ischaemic stroke, intracerebral haemorrhage, and subarachnoid haemorrhage. Biomolecules. 2022;12(5):653. doi:10.3390/biom12050653
- Xu WH, Dong C, Rundek T, Elkind MS, Sacco RL. Serum albumin levels are associated with cardioembolic and cryptogenic ischemic strokes: northern Manhattan study. Stroke. 2014;45(4):973–978. doi:10.1161/STROKEAHA.113.003835
- Soeters PB, Wolfe RR, Shenkin A. Hypoalbuminemia: pathogenesis and clinical significance. Jpen J Parenter Enteral Nutr. 2019;43(2):181–193. doi:10.1002/jpen.1451
- Prajapati KD, Sharma SS, Roy N. Current perspectives on potential role of albumin in neuroprotection. Rev Neurosci. 2011;22(3):355–363. doi:10.1515/RNS.2011.028
- Wang P, Yuan D, Zhang C, et al. High fibrinogen-to-albumin ratio with type 2 diabetes mellitus is associated with poor prognosis in patients undergoing percutaneous coronary intervention: 5-year findings from a large cohort. Cardiovasc Diabetol. 2022;21(1):46. doi:10.1186/s12933-022-01477-w
- Desai R, Fadah K, Srikanth S, Neha N, Jain A. Fibrinogen-albumin ratio predicting major adverse cardiovascular outcomes post-percutaneous coronary intervention: a systematic review and exploratory meta-analysis. Clin Cardiol. 2023;46:455–458. doi:10.1002/clc.23981
- Li M, Tang C, Luo E, Qin Y, Wang D, Yan G. Relation of Fibrinogen-to-Albumin Ratio to Severity of Coronary Artery Disease and Long-Term Prognosis in Patients with Non-ST Elevation Acute Coronary Syndrome. Biomed Res Int. 2020;2020:1860268. doi:10.1155/2020/1860268
- Yang M, Tang L, Bing S, Tang X. Association between fibrinogen-to-albumin ratio and hemorrhagic transformation after intravenous thrombolysis in ischemic stroke patients. Neurol Sci. 2023;44:1281–1288. doi:10.1007/s10072-022-06544-4