
Abstract
Background
Theoretical domains framework (TDF) provides an integrative model for assessing barriers to behavioral changes in order to suggest interventions for improvement in behavior and ultimately outcomes. However, there are other tools that are used to assess barriers.
Objective
The objective of this study is to determine the degree of concordance between domains and constructs identified in two versions of the TDF including original (2005) and refined version (2012) and independent studies of other tools.
Methods
We searched six databases for articles that studied barriers to health-related behavior changes of health care professionals or the general public. We reviewed quantitative papers published in English which included their questionnaires in the article. A table including the TDF domains of both original and refined versions and related constructs was developed to serve as a reference to describe the barriers assessed in the independent studies; descriptive statistics were used to express the results.
Results
Out of 552 papers retrieved, 50 were eligible to review. The barrier domains explored in these articles belonged to two to eleven domains of the refined TDF. Eighteen articles (36%) used constructs outside of the refined version. The spectrum of barrier constructs of the original TDF was broader and could meet the domains studied in 48 studies (96%). Barriers in domains of “environmental context and resources”, “beliefs about consequences”, and “social influences” were the most frequently explored in 42 (84%), 37 (74%), and 33 (66%) of the 50 articles, respectively.
Conclusion
Both refined and original TDFs cataloged barriers measured by the other studies that did not use TDF as their framework. However, the original version of TDF explored a broader spectrum of barriers than the refined version. From this perspective, the original version of the TDF seems to be a more comprehensive tool for assessing barriers in practice.
Background
Knowledge translation and quality improvement (QI) efforts aimed at improving processes and outcomes in health care are plagued by many barriers.Citation1–Citation5 Indeed, barriers at the individual, team, organizational, social, economic, and political levels can dramatically reduce the effectiveness of implementation strategies and lead to suboptimal health care outcomes and increased costs.Citation1,Citation2,Citation7,Citation8 Low-quality care is estimated to account for 20%–40% of total health care industry by health care professionals.Citation8
Theoretical domains framework (TDF) has been developed for systematically identifying and assessing barriers to change interventions and is an umbrella of 33 theories of behavior change.Citation3,Citation5,Citation9,Citation10 It is considered a “ coherent theoretical framework of health-professional behaviors” modification, and its use may facilitate practice changes, knowledge translation, and QI based on sound theories.Citation9,Citation11
For performance improvement and professional development, TDF can be helpful at various levels by identifying barriers to practice change and change theories to address these barriers through a systematic approach, as well as in developing theory-informed interventions for clinical performance improvement and for evaluating and detecting effectiveness of these interventions.Citation3,Citation5,Citation9
The original TDF was developed in 2005 with 12 domains and 128 constructs; it has been used in various studies in different disciplines between 2005 and 2012.Citation5 In 2012, its validity was reevaluated, and a refined version of the TDF was proposed with 14 domains and 84 constructs.Citation3 A questionnaire was developed in 2014 to facilitate its adoption as a framework for practice change.Citation12 Several other tools however, which do not make an explicit reference to TDF as their conceptual framework, have also been developed and used for assessing barriers to change in health service research. Thus, a comparison of the barriers assessed in these questionnaires to those included in TDF is important to identify similarities and differences in order to make informed decisions in choosing a tool. Furthermore, although TDF is the single tool that has been built specifically to assess all kind of barriers systematically, it is still new (the original version was developed in 2005 and revised version in 2012). Therefore, it is important to evaluate the experience and knowledge with TDF to inform clinicians of the advantages and strengths, as well as areas that can be improved. The purpose of this study was to review the published literature on barriers to change to identify specific tools created without explicit reference to TDF and to investigate the similarities and differences of the domains and constructs between TDF (original and refined versions) and these tools. To our knowledge, this is the first review of the TDF content which compares the tools used to assess barriers (developed independently of TDF) to the TDF domains to determine if the TDF is comprehensive and addresses all barriers. Therefore, this study provides unique information that is useful for clinicians and researchers to assess barriers before implementing interventions.
Methods
Search methods for identifying studies
Using a combination of possible Medical Subject Heading terms with free text words related to the concepts derived from research question, a detailed search strategy was developed in MEDLINE-OvidSP which can be found in Table S1. This search strategy was validated by comparing the search results to a defined set of four sentinel articles that were selected by a team of two subject experts and met inclusion criteria for our review; all four sentinel studies were found among the retrieved articles. The search strategy was then translated into other databases using the appropriate controlled vocabulary and free text words in order to search appropriate studies.
The following resources were searched in order to identify the studies from the beginning of indexing papers in these databases until April 2014: Ovid MEDLINE: OvidSP, PubMed, CINAHL, PsycINFO (including full text from PsycARTICLES), EBSCO databases: Academic Search Complete, and Google Scholar.
Criteria for considering studies
We included all articles reporting studies on barriers to change in health-related behavior with no limitation in terms of research methodology and study design. Participants in the studies were either individuals whose health-related knowledge, beliefs, attitudes, and behaviors were reported or health care professionals whose work-related practices were studied. Only papers published in English were included. Qualitative studies were excluded from the review. We also excluded articles that did not publish their barrier assessment questionnaire or survey, either as supplement or in the contents of the paper.
Data collection, abstraction, and analysis
Selection process of the studies
After controlling for duplicates, the titles and abstracts of all potentially relevant studies were reviewed and evaluated for possible inclusion by two reviewers (MM and HHS) working independently. Both reviewers (MM and HHS) independently agreed on including 88% of the included articles (44 out of 50), before any discussion. Disagreements on the inclusion of other 12% of included papers (six out of 50) deemed relevant by one reviewer (HHS) were resolved by discussion and referring unresolved disagreements to a content expert (JPC) after reviewing full-text paper.
Data abstraction and analysis
A table including domains of TDF and related constructs was developed, and descriptive statistics were used. Definitions of all domains and constructs were generated using TDF (2005 and 2012), professional and regular dictionaries such as American Psychological Association (APA) Dictionary of Psychology, The Cambridge Dictionary of Psychology, Dictionary of Psychology and Allied Health Sciences, Dictionary of Psychological Testing, Assessment and Treatment, Oxford English Dictionary, as well as reliable internet sources, and used as references during data abstraction (Table is available upon request).Citation13–Citation18 We developed our own list of constructs definitions in order to use the most updated resources specially APA Dictionary of Psychology (as the most important references in TDF), last version of which was released in 2015.Citation18 All barriers addressed in the articles were classified with reference to the table, using the constructs and domains definitions. Data abstraction and analyses were conducted by two reviewers (MM and HHS) working independently who are both specialized in behavior modification in health, cognitive medical anthropology, health education and health promotion, and qualitative and quantitative research. Kappa interrater reliability before agreement was 0.86 (P=0.000). Disagreements were resolved through discussion between reviewers and consulting with a third party (JPC) to get to complete agreement.
In this paper, we are defining construct as “a concept specially devised to be part of a theory”, a domain as “an area of interest; a sphere of thought, action or knowledge”, and a theoretical domain as “a group of related theoretical constructs”.Citation5
Results
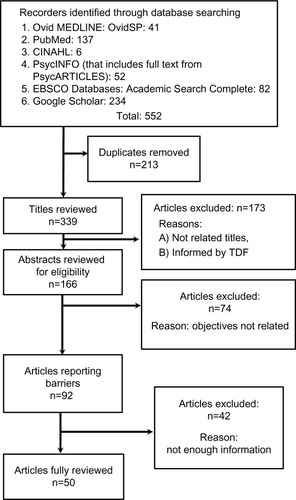
A total of 552 papers were retrieved. After removing duplicates, articles that had been informed by TDF, and articles that were not relevant or did not satisfy our inclusion criteria, 50 papers were selected for final review ().Citation2,Citation19–Citation67 In the 50 reviewed articles, 961 items were used for assessing various barriers, on average 19 items per article. Details of items in each questionnaire and for each domain are presented in Table S2.
Figure 1 Process of identifying publications.
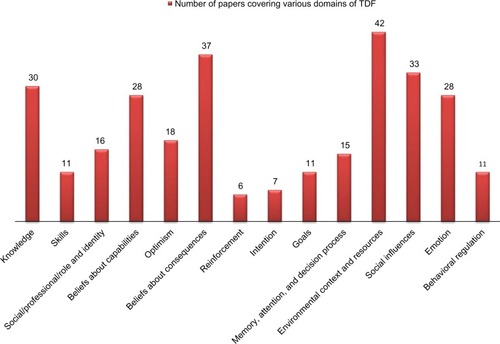
On average, the 50 articles focused on six domains (95% confidence interval: 5.1–6.6) of the refined TDF, and they covered at least two domains; 37 papers (74%) covered four domains and 27 papers (54%) covered six domains. Only two papers (4%) covered up to eleven domains (). Domains of “environmental context and resources”, “beliefs about consequences”, and “social influences” were the three domains of refined TDF assessed most frequently in the reviewed studies, so that 42, 37, and 33 out of 50 papers (84%, 74%, and 66%, respectively) had assessed barriers in these domains (). “Reinforcement” and “intention”, on the other hand, were the domains of the refined TDF that were the least assessed in the studies; “reinforcement” was studied in only six articles (12%) and “intention” in seven (14%) ().
Figure 2 Number of domains of theoretical domains framework covered by reviewed papers (N=50).
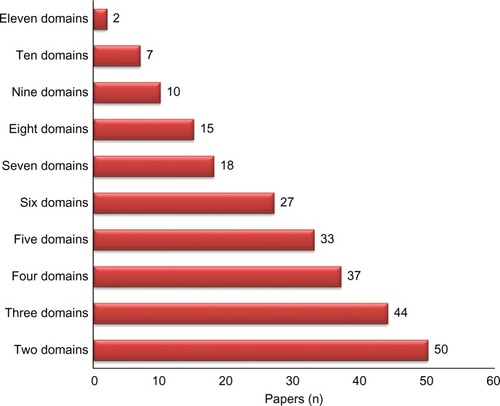
Figure 3 Frequency of papers covering various domains of TDF (N=50).
The refined version of TDF excluded barriers cited in 18 articles (36%) of papers, while the original TDF excluded only barriers cited in two articles (4%). The excluded barriers in 18 articles were mostly related to the removal of domains or constructs from the original version of TDF in the process of creating refined version in 2012 (“characteristics of the innovation/nature of behavior itself ”, “intrinsic motivation”, “attitudes”, “competitive concerns/conflicting demands”, “perceived severity and perceived susceptibility”, and “past experiences”). However, the excluded barriers in the two papers assessed barriers that were outside of domains of both versions of TDF. These barriers focused on “involvement/engagement”, “importance of the desired change”, “preferences”, and “expectations” that we did not find obvious fit with any TDF domains.
Discussion
A coherent theoretical framework of health-professional behaviors is useful to facilitate a systematic approach for identifying barriers and planning interventions aimed at practice change for QI.Citation9,Citation11,Citation68 Our finding that the barrier domains in the refined and original versions of TDF were satisfactory for covering 64% and 96% of barriers in the reviewed articles confirms the comprehensiveness of TDF, especially the original version, as a framework for assessing barriers to behavior modification and explaining practice changes.Citation10 Indeed, between 2005 and 2012, various health care research teams in different countries (Australia, UK, Denmark, and Canada) have applied TDF to inform practice; its usefulness has been confirmed in various health care systems.Citation3,Citation12
Our findings are consistent with those of Francis et al who reported that out of 133 papers from 83 scientific journals indexed in the Scopus database that cited TDF, 21 studies used TDF as an overarching framework for their work.Citation10 Francis et al concluded that TDF-related publications in 13 journals and its application in six countries implied a substantial coverage and interdisciplinary impact. They also highlighted its usefulness as a diagnostic tool to identify mediators of practice improvement and barriers to the implementation of evidence-based practice and QI which is confirmed by French et al.Citation9,Citation10
The TDF domain most often cited in the 50 articles reviewed was “environmental context and resources” in 42 papers (84%). This may imply that environmental context is an important source of barriers or that “environmental context and resources” encompasses numerous types of barriers.Citation69
“Reinforcement” and “intention”, on the other hand, were the least studied, assessed in only six (12%) and seven (14%) of all reviewed articles, respectively. This may reflect a perceived lack of significance of these domains for knowledge users and decision makers. These results were not expected in context of extensive literature supporting the importance of barriers related to “reward-punishment system”, “readiness to change”, and “stages of change”, which are related to these two domains for influencing practice change.Citation70–Citation73
Our finding that barriers in some of the reviewed articles were not cataloged by TDF is interesting and supported by literature. Thirty-six percent of the articles had barriers not captured in the refined TDF and 4% in the original version of TDF. Barriers in the cited 36% tried to assess “characteristics of the innovation/nature of behavior itself ”, “intrinsic motivation”, “attitudes”, and “competitive concerns/conflicting demands”, which had been covered in the original TDF either as a domain (“nature of behavior/characteristics of innovation”) or as constructs under other domains (“intrinsic motivation”, for instance, was covered under the domain “motivation and goals”, “attitudes” was covered under “beliefs about consequences” domain, and “conflict—competing demands, conflicting roles” was covered under the domain “social influences”). Furthermore, “perceived severity” and “perceived susceptibility” had been covered in the original TDF under the domain “beliefs about consequences” as “perceived risk/threat”. The structure of the original TDF and its changes are described briefly in Table S3.Citation3,Citation5 Our finding that the original TDF with a broader range of constructs was more comprehensive than the refined version and compatible with the researchers’ needs is supported by other researchers.Citation12 In the process of developing and validating a user-friendly questionnaire based on TDF, Huijg et al concluded that the original (2005) version of TDF with 12 domains and 128 constructs is more applicable for assessing barriers in practice, while they partially supported the refined TDF.Citation12 In addition, authors of a recent study that has tried to use refined TDF in QI have used the original TDF for informing their interview and focus group questions, implying more practicality for the original version of TDF.Citation74
There were also a few barriers (“involvement/engagement”, “importance of the desired change”, “preferences”, “expectations”) identified in two articles (4%) that could not be found in any TDF versions. Besides a possible shift in behavior change theories over time, another reason for this discrepancy may lie on the difference in definitions of some constructs as we developed our own definition list with the last edition of APA dictionary (2015).Citation5,Citation18 A possible misclassification due to varying scopes of subjective definitions may also be considered; for instance, other researchers may have classified “engagement/involvement” into the construct “team working” that was part of the “social influences” domain in the original TDF; however, any decision to classify constructs in one category or another is subject to critics, given the numerous assumptions in the absence of clear operational definitions.
We also found that there is a need for more clarification about assigning items into the domain of “emotion”. For instance, when a person is saying “I am scared of side effects of medication” or when a practitioner is saying “I fear that this approach may lead to more issues in complex patients”, should these be categorized in the domain of emotion (construct of fear) or are they making references to the consequences, or both? This confirms Wilkinson et al’s finding that more clarification regarding operationalization of TDF would streamline its application.Citation75
Findings of this study should be considered in light of several limitations that may affect some of our results. Non-English papers and qualitative researches were excluded. We also eliminated the articles that did not include their questionnaires in the publication. In addition, the findings are based on the questionnaires developed by the authors of the reviewed articles, and not empirical data. Furthermore, we added the term guidelines in the search strategy since we were aiming to include articles studying barriers to health-related behavior of public people, as well as barriers to clinical practice of health care professionals. Therefore, we may have missed some papers. Like original TDF itself, some constructs were defined using general resources, although we have tried to keep these as low as possible. Finally, we did not assess the quality of the original studies. We do not think, however, that these limitations invalidate our conclusions.
Conclusion
Both refined and original versions of TDF covered well barriers measured by the studies that did not make references to TDF. This result reinforces the idea that TDF is a coherent theoretical framework for measuring barriers to improve or change health-related behaviors among public people or health care professionals. In practice, however, the original version of TDF showed a broader scope of barrier constructs that better fit the researchers’ comprehensive needs. More research may need to see if our findings are supported.
Author contributions
MM contributed to the conception and design of the study, and the acquisition, analysis, and interpretation of data. HHS contributed to acquisition, analysis, and interpretation of data. NK and JPC contributed to conception and design of the study. All authors contributed toward drafting and critically revising the paper, read and approved the final manuscript, and agree to be accountable for all aspects of the work. This project was not supported by any funding.
Disclosure
The authors report no conflicts of interest in this work.
References
- CabanaMDRandCSPoweNRWhy don’t physicians follow clinical practice guidelines? A framework for improvementJAMA1999282151458146510535437
- LarsonEA tool to assess barriers to adherence to hand hygiene guidelineAm J Infect Control2004321485114755236
- CaneJO’ConnorDMichieSValidation of the theoretical domains framework for use in behaviour change and implementation researchImplement Sci201273722530986
- LugtenbergMZegers-van SchaickJMWestertGPBurgersJSWhy don’t physicians adhere to guideline recommendations in practice? An analysis of barriers among Dutch general practitionersImplement Sci200945419674440
- MichieSJohnstonMAbrahamCLawtonRParkerDWalkerAMaking psychological theory useful for implementing evidence based practice: a consensus approachQual Saf Health Care2005141263315692000
- CabanaMDRushtonJLRushAJImplementing practice guidelines for depression: applying a new framework to an old problemGen Hosp Psychiatry2002241354211814532
- Della PennaRMartelHNeuwirthEBRapid spread of complex change: a case study in inpatient palliative careBMC Health Serv Res2009924520040099
- SollecitoWAJohnsonJThe global evolution of continuous quality improvement: from Japanese manufacturing to global health servicesMcLaughlin and KalCuzny’s Continuous Quality Improvement in Health Care4th edBurlington, MAJones and Bartlett Learning2013
- FrenchSDGreenSEO’ConnorDADeveloping theory-informed behaviour change interventions to implement evidence into practice: a systematic approach using the Theoretical Domains FrameworkImplement Sci2012713822531013
- FrancisJJO’ConnorDCurranJTheories of behaviour change synthesised into a set of theoretical groupings: introducing a thematic series on the theoretical domains frameworkImplement Sci201273522531601
- SudsawadPKnowledge Translation: Introduction to Models, Strategies, and MeasuresThe National Center for the Dissemination of Disability Research2007 Available from: http://www.ncddr.org/kt/products/ktintro/ktintro.pdfAccessed February 5, 2016
- HuijgJMGebhardtWACroneMRDusseldorpEPresseauJDiscriminant content validity of a theoretical domains framework questionnaire for use in implementation researchImplement Sci201491124423394
- VandenBosGAPA Dictionary of PsychologyWashington, DCAmerican Psychological Association (APA)2007
- MatsumotoDThe Cambridge Dictionary of PsychologyNew York, NYCambridge University Press2009
- Stuart-HamiltonIDictionary of Psychological Testing, Assessment and Treatment2nd edLondon, UKJessica Kingsley Publishers2007
- RoeckeleinJElsevier’s Dictionary of Psychological TheoriesAmsterdamElsevier2006
- BhatiaMDictionary of Psychology and Allied Health SciencesNew DelhiNew Age International (P) Ltd., Publishers2009
- VandenBosGRAPA Dictionary of Psychology2nd edWashington, DCAmerican Psychological Association (APA)2015
- MollemEDSnoekFJHeineRJAssessment of perceived barriers in self-care of insulin-requiring diabetic patientsPatient Educ Couns19962932772819006243
- YoungMReadJBarker-ColloSHarrisonREvaluating and overcoming barriers to taking abuse historiesProf Psychol Res Pract2001324407414
- O’CarrollREFosterCMcGeechanGSandfordKFergusonEThe “ick” factor, anticipated regret, and willingness to become an organ donorHealth Psychol201130223624521401258
- HeinowitzAEBrownKRLangsamLCIdentifying perceived personal barriers to public policy advocacy within psychologyProf Psychol Res Pract2012434372378
- SudomKZamorskiMGarberBStigma and barriers to mental health care in deployed Canadian forces personnelMil Psychol2012244414431
- PidanoAEKimmelblattCANeaceWPBehavioral health in the pediatric primary care setting: needs, barriers, and implications for psychologistsPsychol Serv201183151165
- OuimettePVogtDWadeMPerceived barriers to care among veterans health administration patients with posttraumatic stress disorderPsychol Serv201183212223
- GordonAJKavanaghGKrummMFacilitators and barriers in implementing buprenorphine in the Veterans Health AdministrationPsychol Addict Behav201125221522421480679
- PerepletchikovaFHiltLMCherejiEKazdinAEBarriers to implementing treatment integrity procedures: survey of treatment outcome researchersJ Consult Clin Psychol200977221221819309181
- VincentNLewyckySFinneganHBarriers to engagement in sleep restriction and stimulus control in chronic insomniaJ Consult Clin Psychol200876582082818837599
- MansfieldAKAddisMECourtenayWMeasurement of men’s help seeking: development and evaluation of the barriers to help seeking scalePsychol Men Masc20056295108
- MartinDJBrooksRAOrtizDJVeniegasRCPerceived employment barriers and their relation to workforce-entry intent among people with HIV/AIDSJ Occup Health Psychol20038318119412872956
- CatzSLKellyJABogartLMBenotschEGMcauliffeTLPatterns, correlates, and barriers to medication adherence among persons prescribed new treatments for HIV diseaseHealth Psychol200019212413310762096
- de VosMLvan der VeerSNGraafmansWCImplementing quality indicators in intensive care units: exploring barriers to and facilitators of behaviour changeImplement Sci201055220594312
- MillsEWilsonKRachlisBBarriers to participation in HIV drug trials: a systematic reviewLancet Infect Dis200661323816377532
- BryarRMClossSJBaumGThe Yorkshire BARRIERS project: diagnostic analysis of barriers to research utilisationInt J Nurs Stud2003401738412550152
- TuckerCMRiceKGDesmondFFHouWKayeLBSmithTMThe youth form of the Motivators of and Barriers to Health-Smart Behaviors InventoryPsychol Assess201224249050222103550
- TuVPHussonFSutanAHaDTValentinDFor me the taste of soy is not a barrier to its consumption. And how about you?Appetite201258391492122329946
- ColletJ-PKissoonNSkippenPEngaging pediatric intensive care unit (PICU) clinical staff to lead practice improvement: the PICU participatory action research project (PICU-PAR)Implement Sci20149624401288
- SeidMOpipari-ArriganLGelhardLRVarniJWDriscollKBarriers to care questionnaire: reliability, validity, and responsiveness to change among parents of children with asthmaAcad Pediatr20099210611319329101
- CahillNEMurchLCookDHeylandDKBarriers to feeding critically ill patients: a multicenter survey of critical care nursesJ Crit Care201227672773422981532
- WelshEMJefferyRWLevyRLMeasuring perceived barriers to healthful eating in obese, treatment-seeking adultsJ Nutr Educ Behav201244650751221665549
- VennerKLGreenfieldBLVicuñaBMuñozRBhattSO’KeefeV“I’m not one of them”: barriers to help-seeking among American Indians with alcohol dependenceCultur Divers Ethnic Minor Psychol201218435236222985245
- TimenAHulscherMEJLRustLBarriers to implementing infection prevention and control guidelines during crises: experiences of health care professionalsAm J Infect Control201038972673320605262
- WilliamsMTDomanicoJMarquesLLeblancNJTurkheimerEBarriers to treatment among African Americans with obsessive-compulsive disorderJ Anxiety Disord201226455556322410094
- SimonSLDuncanCLJanickeDMWagnerMHBarriers to treatment of paediatric obstructive sleep apnoea: development of the adherence barriers to continuous positive airway pressure (CPAP) questionnaireSleep Med201213217217722172967
- AikenAMGoldMAParkerAMChanges in young women’s awareness, attitudes, and perceived barriers to using emergency contraceptionJ Pediatr Adolesc Gynecol2005181253215749581
- ParkESongMCommunication barriers perceived by older patients and nursesInt J Nurs Stud200542215916615680614
- ChouP-LRauK-MLinC-CDevelopment and psychometric testing of a short version of the Barriers Questionnaire-Taiwan form for cancer patientsInt J Nurs Stud20114891071107921396643
- PassikSDKirshKLDonaghyKPatient-related barriers to fatigue communication: initial validation of the fatigue management barriers questionnaireJ Pain Symptom Manage200224548149312547048
- ThompsonJLDavisSMGittelsohnJPatterns of physical activity among American Indian children: an assessment of barriers and supportJ Community Health200126642344511759094
- CigularovKChenPYThurberBWStallonesLWhat prevents adolescents from seeking help after a suicide education program?Suicide Life Threat Behav2008381748618355110
- CranneyMBartonSWalleyTAddressing barriers to change: an RCT of practice-based education to improve the management of hypertension in the elderlyBr J Gen Pract19994944452252610621984
- LetiziaMCreechSNortonEShanahanMHedgesLBarriers to caregiver administration of pain medication in hospice careJ Pain Symptom Manage200427211412415157035
- ChanWKKongHWaiKSumRLauKOBarriers to the implementation of physical education (PE) assessment in Hong KongInt J Learn2006134165170
- McKennaHPAshtonSKeeneySBarriers to evidence-based practice in primary careJ Adv Nurs200445217818914706003
- ChiuYa-WenWengYi-HaoLoHeng-LienHsuChih-ChengYa-Hui ShihKKComparison of evidence-based practice between physicians and nurses: a national survey of regional hospitals in TaiwanJ Contin Educ Health Prof201030213213820564703
- MorinagaKOhtsuboYYamauchiKShimadaYDoctors’ traits perceived by Japanese nurses as communication barriers: a questionnaire surveyInt J Nurs Stud200845574074917280673
- SimmAlannaLiLindaGeddesLynneBrooksDianaAlisson HoensDRImpact of a behavioral-based intervention on inspiratory muscle training prescription by a multidisciplinary teamJ Contin Educ Health Prof201232211612522733639
- LeeCOryMGYoonJForjuohSNNeighborhood walking among overweight and obese adults: age variations in barriers and motivatorsJ Community Health2013381122222811072
- GunnarsdottirSDonovanHSSerlinRCVogeCWardSPatient-related barriers to pain management: the Barriers Questionnaire II (BQ-II)Pain200299338539612406513
- DobkinPLde CivitaMBernatskySFilipskiMSitaABaronMPreliminary validity of the barriers to treatment adherence questionnaire in fibromyalgia: combining quantitative and focus group dataPsychol Rep2009105244746019928606
- BearseJLMcMinnMRSeegobinWFreeKBarriers to psychologists seeking mental health careProf Psychol Res Pract2013443150157
- TurconiGCelsaMRezzaniCBiinoGSartiranaMARoggiCReliability of a dietary questionnaire on food habits, eating behaviour and nutritional knowledge of adolescentsEur J Clin Nutr200357675376312792659
- CCNCritical Care Nutrition: barriers questionnaire2013 Available from: http://www.criticalcarenutrition.com/index.php?option=com_content&view=article&id=171%3Ains-barriers-questionnaire&catid=16%3Anewsroom&Itemid=1Accessed May 1, 2014
- McCluskeyALovariniMProviding education on evidence-based practice improved knowledge but did not change behaviour: a before and after studyBMC Med Educ200554016364181
- GravelKLégaréFGrahamIBarriers and facilitators to implementing shared decision-making in clinical practice: a systematic review of health professionals’ perceptionsImplement Sci200611616899124
- SalbachNMJaglalSBKorner-bitenskyNRappoltSDavisDPractitioner and organizational barriers to evidence-based practice of physical therapists for people with strokePhys Ther200787101284130317684088
- StichlerJFFieldsWKimSCBrownCEFaculty knowledge, attitudes, and perceived barriers to teaching evidence-based nursingJ Prof Nurs20112729210021420041
- GrimshawJMShirranLThomasRChanging provider behavior: an overview of systematic reviews of interventionsMed Care2001398 Suppl 2II2II4511583120
- DamschroderLJAronDCKeithREKirshSRAlexanderJALoweryJCFostering implementation of health services research findings into practice: a consolidated framework for advancing implementation scienceImplement Sci200945019664226
- Di NoiaJProchaskaJODietary stages of change and decisional balance: a meta-analytic reviewAm J Health Behav201034561863220524891
- NorcrossJCKrebsPMProchaskaJOStages of changeJ Clin Psychol201167214315421157930
- LamCSWileyAHSiuAEmmettJAssessing readiness to work from a stages of change perspective: implications for return to workWork201037332132920978339
- ReddingCARossiJSRossiSRVelicerWFProchaskaJOHealth behavior modelsInt Electron J Health Educ20003Special Issue180193
- SteinmoSHMichieSFullerCStanleySStapletonCStoneSPBridging the gap between pragmatic intervention design and theory: using behavioural science tools to modify an existing quality improvement programme to implement “Sepsis Six”Implement Sci2016111426841877
- WilkinsonSThomasSPhillipsCJExperiences of using the Theoretical Domains Framework across diverse clinical environments: a qualitative studyJ Multidiscip Healthc2015813914625834455