
Abstract
Buerger’s disease, also known as thromboangiitis obliterans (TAO), is a segmental inflammatory disease affecting small- and medium-sized vessels, which is strongly associated with tobacco use. Although the etiology is still unknown, recent studies suggest an immunopathogenesis. Diagnosis is based on clinical and angiomorphologic criteria, including age, history of smoking, clinical presentation with distal extremity ischemia, and the absence of other risk factors for atherosclerosis, autoimmune disease, hypercoagulable states, or embolic disease. Until now, no causative therapy exists for TAO. The most important therapeutic intervention is smoking cessations and intravenous prostanoid infusions (iloprost). Furthermore, effective analgesia is crucial for the treatment of ischemic and neuropathic pain and might be expanded by spinal cord stimulation. Revascularization procedures do not play a major role in the treatment of TAO due to the distal localization of arterial occlusion. More recently, immunoadsorption has been introduced eliminating vasoconstrictive G-protein-coupled receptor and other autoantibodies. Cell-based therapies and treatment with bosentan were also advocated. Finally, a consequent prevention and treatment of wounds and infections are essential for the prevention of amputations. To achieve better clinical results, integrated care in multidisciplinary and trans-sectoral teams with emphasis on smoking cessation, pain control, wound management, and social care by professionals, social workers, and family members is necessary.
Introduction
In 1879, Winiwarter,Citation1 a young assistant physician of Theodor Billroth in Vienna, published the clinical course and pathologic examination of a lower limb amputation of a 57-year-old male describing “a peculiar kind of angiitis and endophlebitis with gangrene”. Although this is considered to be the first case report of thromboangiitis obliterans (TAO), the disease is currently more exclusively linked to the American surgeon BuergerCitation2, whose systematic work on clinical and pathological aspects of the disease constituted our modern understanding of the disease.
TAO is an inflammatory vascular pathology affecting small- and medium-sized arteries and veins leading to vessel occlusions by the formation of a mononuclear cell-rich thrombus.Citation2 Its etiology is still unknown, but it is inseparably linked to tobacco use. Due to an undulating clinical course, normal vessel segments and different stages of lesions (acute to chronic types) might be found together in the same patient.Citation2
Patients with Buerger’s disease usually present with acute ischemic or infectious acral lesions (ulcers, gangrenes, subungual infections, phlegmonous) and/or thrombophlebitic nodules. Skin discolorations such as Raynaud’s phenomenon, acrocyanosis, or livedo-like pictures are often seen.Citation3–Citation5 Rarely, a nonerosive arthritis might precede ischemia for months or years.Citation6
Epidemiology
Buerger’s disease occurs worldwide and is more prevalent in males, but an increasing prevalence in females has been reported in different countries.Citation7–Citation9 Disease characteristics and prognosis do not differ between males and females.Citation9 In contrast to North America and Western Europe, the Mediterranean, the near and far East, and the Indian subcontinent are high prevalence regions.Citation3–Citation5 Thus, prevalence rates among in-hospital treated patients with peripheral arterial occlusive disease were reported to range from 0.5% to 5.6% in Western Europe, 45%–63% in India, and 16%–66% in Korea and Japan.Citation10 In the meanwhile, the formerly often cited extremely high prevalence rate in Ashkenazi Jews was identified as a scientific error as it referred to the response rate of an invitation to participate in a study and did not reflect the true prevalence in this ethnic group.Citation11 Reported prevalence of TAO seems to decline during the past decades due to a decrease in tobacco use or – as others believe – due to an increase in socioeconomic conditions.Citation12–Citation14
Etiologic, pathologic, and pathogenetic aspects
There is a very tight correlation between the manifestation, flaring, and recurrence of Buerger’s disease (no tobacco, no Buerger’s disease).Citation3–Citation5,Citation10 Thus, tobacco must be considered to be the dominant risk factor. Besides potential differences in regional smoking habits, regional and ethnic differences in the prevalence of the disease might point toward a genetic background determining individual susceptibility. Human–leukocyte–antigen-linked factors may play a role; nevertheless, human leukocyte antigen association studies revealed heterogeneous findings.Citation15–Citation18 Published genetic polymorphisms consist of CD14 T7T polymorphism, eNOS gene 894 T/T polymorphism as a protective factor, and MyD88 rrs7744 A-G polymorphism, coding for a Toll-like receptor signaling adaptor.Citation19–Citation22
Chronic infectious disease – especially periodontal disease – was found to be associated with TAO.Citation23,Citation24 On the other hand, in a particular disease group of the disease (ie, low social status and excessive smokers), periodontal disease can be expected to be very high triggering a close correlation, which does not necessarily imply a causative linkage. Nevertheless, smoldering infections such as periodontitis might trigger autoimmune mechanisms and coagulation.Citation24
Signs of endothelial activation and proliferation as well as the presence of immunocompetent cells are seen in acute type lesions. Immunoglobulin and complement deposition as well as CD4+ and CD8+ T-lymphocytes, CD 20+ B-lymphocytes, and S-100-positive dendritic cells were found alongside the lamina elastica interna, which becomes structurally altered but is typically preserved.Citation25–Citation30 Giant cell formation and the appearance of the so-called microabscesses within the mono-nuclear cell-rich thrombus may occur.Citation2
Analysis of cytokine activation in patients with TAO revealed a pattern of elevated pro- and anti-inflammatory cytokines.Citation31,Citation32 Various kinds of autoantibodies have been identified in patients with TAO, including anti-endothelial antibodies, antibodies directed against vessel wall structures such as elastin and collagen, anticardiolipin antibodies, and antineutrophil cytoplasmic antibodies.Citation33–Citation39 More recently, agonistic autoantibodies directed against G-protein-coupled receptors were identified as potentially promoting vasospasm, compromising microcirculation, damaging vessel structures, and inducing proliferative processes.Citation40
Overall, the findings are consistent with the assumption of an immunopathogenesis of TAO. A first model of this new paradigm has recently been published by Ketha and Cooper.Citation41
Social and psychosomatic aspects
Buerger’s disease typically occurs in patients with a low social status.Citation14 Some authors even described a Buerger-type personality with manipulative and autoaggressive tendencies often matched with denial, negligence, or tendencies to minimize their illness, while others even presumed typical morphological characteristics.Citation42,Citation43 However, no systematic work has been performed in this field, and the preliminary results do not allow differentiating between premorbid traits and conditions and psychological consequences of the chronicity and severity of the disease or implications of chronic drug intake such as morphine or opioids in the affected patients.
Diagnostic criteria
Diagnosis is usually based on clinical and angiomorphologic criteria published by Olin et al and Shionoya.Citation13,Citation44 The latter is based on only five criteria and thus easy to remember (). Combined upper and lower extremity involvement is present in ~20%–25% of the cases.Citation45,Citation46 An isolated affection of only one limb strongly argues against Buerger’s disease.Citation45 Proximal arterial involvement is rarely present.Citation47,Citation48 Nevertheless, case reports of typical lesions even in cerebral, coronary, and visceral arteries have been published.Citation49–Citation53 Thrombophlebitis – if present – is often of migratory type and precedes or parallels arterial disease activity.Citation54
Table 1 Diagnostic criteria for TAO
Establishing diagnosis
Typically, a young heavy smoker presents with a more or less symmetrical distal ischemic syndrome or a crural–acral or antebrachial–acral type of arterial occlusion in two or more extremities. Distal pulses are usually absent or diminished, but can be normal in the case of exclusive acral disease manifestations. Allen’s test often reveals an upper extremity involvement.
Ankle brachial index or forearm–brachial index is usually reduced, but might be normal in cases with more distally located disease. Digital pulse recordings are characterized by low amplitudes and delayed slopes, anarchic or silent pulse curves.
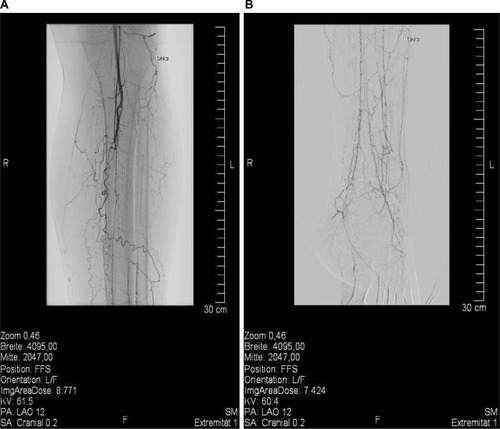
Angiographically, a typical but not pathognomonic pattern () has been described, which substantiates the diagnosis.Citation43 This pattern might also be identified by magnetic resonance imaging or a careful duplex ultrasound examination.
Figure 1 Angiographic pattern of Buerger’s disease in a young male patient.
Abbreviation: TAO, thromboangiitis obliterans.
Embolic disease – if suspected – can be ruled out by transesophageal echocardiography, computer tomography angiography, and duplex ultrasound of the proximal extremity arteries.
Capillary video microscopy is often limited by infection or hornification. It often reveals capillary loss and unspecific morphologic changes.Citation55,Citation56 Nevertheless, capillary microscopy is a useful tool in the differential diagnosis.
There are no specific biomarkers for TAO.Citation3–Citation5,Citation10 Systemic inflammatory markers such as C-reactive protein are usually absent or only slightly elevated and are therefore unsuitable for the assessment or monitoring of disease activity. Nevertheless, laboratory tests are important to exclude other entities such as diabetes, connective tissue disease, vasculitides, or congenital or acquired thrombophilia.Citation3–Citation5,Citation10
If biopsy can be performed without endangering the limb or if an amputation is performed, diagnosis should be confirmed by histopathologic examination. Fresh thrombophlebitic nodules are suitable for this purpose.
Therapy
In the past decades, therapeutic efforts concentrated on pain and infection control, revascularization, or amputation.
Smoking cessation
Nevertheless, the most important therapeutic intervention in Buerger’s disease is smoking cessation.Citation3–Citation5,Citation10 Its overwhelming effect for the prevention of consecutive limb amputation was impressively shown.Citation13 Patients with TAO should be prevented not only from active smoking but also from alternative consumption mode and passive exposure.Citation57,Citation58 Tobacco dependency is usually considered to be exceptionally strong in patients with Buerger’s disease, but in the only prospective study addressing this question the degree of tobacco dependence was similar to that in patients with coronary artery disease.Citation59
Individual strategies for smoking withdrawal have to be discussed, including in- and outpatient treatment in specialized institutions with multidisciplinary teams.Citation60,Citation61 Unfortunately, the percentage of patients who maintain smoking cessation despite is low.Citation60,Citation61 In one study, the continuous abstinence rate decreased from 29% at the end of the treatment to 18.5% at the 12-month follow-up.Citation61 Best results seem to be achieved by structured and guided peer group and anti-smoking programs starting during hospital stay or shortly thereafter.Citation62,Citation63 Medication support by nicotine replacement therapy, bupropion, or varenicline might be provided. Whether replacement therapies or adjuvant therapies might prolong disease activity was – to our knowledge – not addressed, but should be examined in further studies.
As was shown by the TEMPO study, work and family circumstances, co-occurring substance use, and psychological difficulties may influence smoking cessation in the typical age groups of patients with Buerger’s disease. Factors specifically associated with a low probability of smoking cessation were job strain and symptoms of hyperactivity/inattention, while occupational grade was associated with smoking relapse.Citation64
Prostanoid therapy and antiplatelet drugs
The effectiveness of prostanoid therapy was elucidated in two older randomized trials and in two more recently published trials prospectively assessing clinical outcome in addition to smoking cessation, aspirin, or compared with sympathectomy.Citation65–Citation68 Iloprost, a prostacyclin analog, is considered the drug of choice.Citation65 Fiessinger and SchäferCitation65 randomly allocated 152 patients with Buerger’s disease and pain from critical leg ischemia to iloprost intravenously or low-dose aspirin for 28 days in a double-blind trial. Fifty-eight (85%) of 68 iloprost-treated patients showed ulcer healing or relief of ischemic pain versus eleven (17%) of 65 in the aspirin-treated group. Forty-three (63%) patients on iloprost treatment had complete relief of pain, compared with 18 (28%) on aspirin. Unfortunately, these striking results could not reproduced in the largest randomized trial, including 319 patients, when iloprost was administered orally in two dose regimes and compared with placebo.Citation66 In a study published by the Turkish Buerger’s Disease Research Group, complete ulcer healing rate was 61.9% in those receiving iloprost and 41% in the lumbar sympathectomy group at 4 weeks and 85.3% versus 52.3% at 24 weeks.Citation67 In a prospective Turkish multicenter observational trial in 158 patients with Buerger’s disease suffering from rest pain and/or ischemic lesions, complete ulcer healing without residual rest pain or major amputation was met by 60% of the patients treated with iloprost. Pain scale values decreased significantly after 4 weeks and 24 weeks. Ulcer size reduction at 4 weeks and 24 weeks, as well as clinical status, investigator, and observer grading, was also significantly improved at both time points.Citation68
A recently published Cochrane review emphasized low-quality evidence concerning medical therapy in Buerger’s disease and stated that high-quality trials assessing the effectiveness of pharmacological agents in people with Buerger’s disease are urgently needed.Citation69
Although widely used, there is no proven evidence for platelet function inhibitors such as aspirin or clopidogrel in TAO. Same is true for oral anticoagulants.Citation3–Citation5,Citation10
Analgesia
Effective analgesia is crucial as ischemic and neuropathic pain in Buerger’s disease is usually severe. Therefore, co-treatment by pain therapy specialists is essential. Combinations of morphine or opioids and peripheral analgetics are often required in high doses. Antidepressants might be of additional value. Epidural anesthesia, neuronal block, or local analgesia is often applied.Citation70–Citation72 In the selected cases, spinal cord stimulation might improve not only pain control but also perfusion by inducing sympathicolysis and via antidrome mechanisms.Citation73,Citation74
Revascularization procedures
Due to the distal localization of arterial occlusions and the absence of recipient vessels, interventional or surgical revascularization is impossible to perform in the majority of cases. Nevertheless, especially in the older literature, series of peripheral bypass procedures in Buerger’s disease have been published with acceptable results in highly selected patients (revascularization rate: 4.6%–17.7%) and highly specialized centers, reporting up to 48.8% and 62.5% at 5 years, and 43.0% and 56.3% at 10 years, respectively.Citation75–Citation78
Endovascular therapy might also be effective even in extended femorotibial occlusions, but the reported numbers are small and the role of endovascular therapy in Buerger’s disease has yet to be defined.Citation79–Citation82
Sympathectomy
As revascularization procedures are often impossible, surgical or chemical sympathectomy is often considered, despite a lack of valid data supporting this practice. In a more recent publication of a cohort of 216 Turkish patients, sympathectomy was preferred over open surgical reconstruction or bypass procedures (81% versus 19%). Clinical outcome following sympathectomy was rated “improved” in 52.3%, “stable” in 27.8%, and “worse” in 19.8% of the patients, while seven major and 36 minor amputations were performed.Citation83 On the other hand, lumbar sympathectomy was reported to be inferior to intravenous iloprost applications in a randomized trial by the same group.Citation68 Thus, currently, there is no proven indication for primary sympathectomy in Buerger’s disease despite the fact that it is still widely used in many countries.
Immunosuppressive drugs
Although widely used in former times, there is no proven evidence for the use of steroids or cyclophosphamide therapy.Citation43,Citation84,Citation85
Progenitor cell therapy
In the past decade, cell-based therapies with autologous progenitor cells harvested from bone marrow or peripheral blood have been advocated in critical limb ischemia, including Buerger’s disease. The cell suspensions are usually applied by intramuscular injections alongside the vascular bed of the limbs or by intra-arterial injection.Citation86–Citation90
Meta-analyses confirmed practicability and safety as well as positive therapeutic effects (including pain control, ulcer healing, pain-free walking ability, amputations-free survival) of cell-derived therapies in critical limb ischemia.Citation88,Citation91,Citation92 Patients with Buerger’s disease responded better than patients with atherosclerotic peripheral arterieal disease in some, but not all studies.Citation93–Citation95 There seems to be a significant time lag of 4–8 weeks until an improvement of microcirculation becomes evident in responders after bone marrow cell transplantation.Citation96 This lag might be especially problematic in case of severe ischemia demanding a more urgent improvement of perfusion. Results of randomized double-blinded studies are awaited, but the hype about progenitor cell therapy already seems to be over.
Intramuscular or intra-arterial progenitor cell therapies compete against surgical concepts of stimulating angio-genesis and arterialization in patients with TAO based on tibia bone distraction or fenestration, or implantation of a Kirschner wire in the tibial intramedullary canal. These procedures were also reported to result in improved outcomes including pain scores, ulcer healing, and walking distances.Citation97–Citation99 Nevertheless, they might be hampered by side effects as the operation takes place in an ischemic environment. Controlled and comparative studies are missing.
Immunoadsorption
Immunoadsorption (IA) is an extracorporeal procedure clearing plasma from immunoglobulins and circulating immuno-complexes approved in many immune-mediated diseases. Based on the hypothesis that Buerger’s disease is immune-mediated with humoral factors playing a major role, IA was successfully introduced in a pilot study conducted by Baumann et alCitation100 and later introduced in clinical routine care.Citation101 More recently, a possible effective mechanism of IA was elucidated as IA eliminates vasoconstrictive α- and endothelin receptor agonistic autoantibodies that seem to cluster in patients with Buerger’s disease.Citation102 The pilot study revealed a fast improvement of pain, a steep increase in tcpO2-levels and decrease in tcCO2-levels, an improvement in ulcer healing, and a high return-to-work rate of the patients.Citation100 Overall, these positive results were reproduced in a clinical routine setting.Citation101 IA is being performed on five consecutive days for 5–6 hours per session aiming for a clearance of ~2.5-fold of patient’s plasma volume.Citation100–Citation102 It might be followed by the substitution of polyvalent immunoglobulin to ameliorate infectious risks in patients with active gangrene or ulcers.Citation100
Bosentan
Referring to a first positive case report, another Spanish group published their results of a pilot study introducing the endothelin-receptor-blocking agent, bosentan, in the treatment of digital ulcers in patients with Buerger’s disease.Citation103,Citation104 Dosing was derived from the approved application for prophylaxis of digital ulcers in patients with scleroderma. Despite the promising results, ~1/6 of the patients had to undergo minor digital amputations: a finding, not necessarily arguing against the effectiveness of bosentan as minor amputations might have already been inevitable at presentation or might even have been made successfully possible by the treatment, and a finding that was also observed in our IA patients.Citation101
Wound management and infection
Local wound management in ischemic lesions in Buerger’s disease is based on modern wound care standards with surgical debridement and selected wound dressings according to the wound’s stage and condition. As ischemic wounds – if at all – tend to heal very slowly, a cross-sectional and multidisciplinary concept is crucial. Wound, soft tissue, and bone infections might cause serious clinical problems and relapses as they occur in often highly ischemic states. Bacterial species and resistance spectra vary widely with gram-positive species dominating our own series (unpublished data). Starting calculated antibiotic therapy, one has to take anaerobic species and multiple resistances into account.
Outcome and social consequences
According to an older literature survey conducted by Börner and Heidrich,Citation105 amputations were performed in 6.9%–75% of patients with TAO within 3–10 years of follow-up. Minor amputations predominated; nevertheless, major amputation rate was reported as high as 31%. The high amputation rates in the relatively young patients significantly contribute to the financial and social burden of the disease, which additionally includes job loss, early retirements, divorces, and subsequent social isolation.Citation105
Perspective
Many decades from Buerger’s landmark report the disease he dedicated himself to remains an important health issue not only in high prevalence regions as it affects young people and induces a high social and financial burden. Hopefully, the new paradigm of an immunopathogenesis of Buerger’s disease might improve knowledge and prognosis in the future. To achieve better clinical results, integrated care in multidisciplinary and trans-sectoral teams with emphasis on lifestyle changes such as smoking cessation, pain control, wound management, and social care by professionals, social workers, and family members is necessary.Citation106,Citation107
Disclosure
The authors report no conflicts of interest in this work.
References
- WiniwarterFUeber eine eigenthümliche Form von Endarteriitis und Endophlebitis mit Gangrän des Fußes [About a strange kind of endarteriitis and endophlebitis with gangrene of the foot]Arch Klin Chir187923202226 quoted according to ref. 39
- BuergerLLandmark publication from the American Journal of the Medical Sciences,’ Thrombo-angiitis obliterans: a study of the vascular lesions leading to presenile spontaneous gangrene’. 1908Am J Med Sci2009337427428419365174
- DargonPTLandryGJBuerger’s diseaseAnn Vasc Surg201226687188022284771
- OlinJWThromboangiitis obliterans (Buerger’s disease)N Engl J Med20003431286486910995867
- PiazzaGCreagerMAThromboangiitis obliteransCirculation2010121161858186120421527
- PuéchalXFiessingerJNThromboangiitis obliterans or Buerger’s disease: challenges for the rheumatologistRheumatology (Oxford)200746219219917116654
- HidaNOhtaTCurrent status of patients with Buerger disease in JapanAnn Vasc Dis20136361762324130618
- LieJTThe rise and fall and resurgence of thromboangiitis obliterans (Buerger’s disease)Acta Pathol Jpn19893931531582662703
- SasakiSSakumaMKuniharaTYasudaKCurrent trends in thromboangiitis obliterans (Buerger’s disease) in womenAm J Surg1999177431632010326851
- ArkkilaPEThromboangiitis obliterans (Buerger’s disease)Orphanet J Rare Dis200611416722538
- AdarREpidemiology of TAO – correction of an errorAtherosclerosis201021112420167322
- MatsushitaMNishikimiNSakuraiTNimuraYDecrease in prevalence of Buerger’s disease in JapanSurgery199812434985029736901
- OlinJWYoungJRGraorRARuschhauptWFBartholomewJRThe changing clinical spectrum of thromboangiitis obliterans (Buerger’s disease)Circulation1990825 supplIV3IV82225420
- FazeliBBuerger’s disease as an indicator of socioeconomic development in different societies, a cross-sectional descriptive study in the North-East of IranArch Med Sci20106334334722371769
- McLoughlinGAHelsbyCREvansCCChapmanDMAssociation of HLA-A9 and HLA-B5 with Buerger’s diseaseBr Med J19762604511651166990826
- AerbajinaiWTsuchiyaTKimuraAYasukochiYNumanoFHLA class II DNA typing in Buerger’s diseaseInt J Cardiol199654supplS197S2029119524
- OtawaTJugiTKawanoNMishimaYToyamaHLetter: HL-A antigens in thromboangiitis obliteransJAMA1974230811284479437
- NumanoFSasazukiTKoyamaTHLA in Buerger’s diseaseExp Clin Immunogenet1986341952003274054
- KimuraAKobayashiYTakahashiMMICA gene polymorphism in Takayasu’s arteritis and Buerger’s diseaseInt J Cardiol199866suppl 1S107S1139951809
- MehraNKJainiRImmunogenetics of peripheral arteriopathiesClin Hemorheol Microcirc2000232–422523211321444
- AdigüzelYYilmazEAkarNEffect of eNOS and ET-1 polymorphisms in thromboangiitis obliteransClin Appl Thromb Hemost201016110310619520685
- ChenZNakajimaTInoueYA single nucleotide polymorphism in the 3′-untranslated region of MyD88 gene is associated with Buerger disease but not with Takayasu arteritis in JapaneseJ Hum Genet201156754554721525878
- PavlicVVujic-AleksicVZubovicNGojkov-VukelicMPeriodontitis and Buerger’s disease: recent advancesActa Inform Med201321425025224554799
- IwaiTPeriodontal bacteremia and various vascular diseasesJ Periodontal Res200944668969419874452
- FazeliBRafatpanahHRavariHHosseiniRFRezaeeSAInvestigation of the expression of mediators of neovascularization from mononuclear leukocytes in thromboangiitis obliteransVascular201422317418023567329
- GulatiSMAgarwalVSharmaVSahaKC3 complement components & their breakdown product (C3d) in patients of thromboangiitis obliteransIndian J Med Res1986846076113494676
- HalachevaKGulubovaMVManolovaIPetkovDExpression of ICAM-1, VCAM-1, E-selectin and TNF-alpha on the endothelium of femoral and iliac arteries in thromboangiitis obliteransActa Histochem2002104217718412086338
- KimEJChoBSLeeTSKimSJSeoJWMorphologic change of the internal elastic lamina in Buerger’s diseaseJ Korean Med Sci2000151444810719807
- KobayashiMItoMNakagawaANishikimiNNimuraYImmunohistochemical analysis of arterial wall cellular infiltration in Buerger’s disease (endarteritis obliterans)J Vasc Surg199929345145810069909
- LeeTSeoJWSumpioBEKimSJImmunobiologic analysis of arterial tissue in Buerger’s diseaseEur J Vasc Endovasc Surg200325545145712713785
- Dellalibera-JovilianoRJovilianoEESilvaJSEvoraPRActivation of cytokines corroborate with development of inflammation and autoimmunity in thromboangiitis obliterans patientsClin Exp Immunol20121701283522943198
- SlavovESStanilovaSAPetkovDPDobrevaZGCytokine production in thromboangiitis obliterans patients: new evidence for an immune-mediated inflammatory disorderClin Exp Rheumatol200523221922615895893
- De GodoyJMBraileDMGodoyMFBuerger’s disease and anticardiolipin antibodies: a worse prognosis?Clin Appl Thromb Hemost200281858611991245
- EichhornJSimaDLindschauCAntiendothelial cell antibodies in thromboangiitis obliteransAm J Med Sci1998315117239427570
- GulatiSMMadhraKThusooTKNairSKSahaKAutoantibodies in thromboangiitis obliterans (Buerger’s disease)Angiology198233106426516751163
- HalachevaKSManolovaIMPetkovDPAndreevAPStudy of anti-neutrophil cytoplasmic antibodies in patients with thromboangiitis obliterans (Buerger’s disease)Scand J Immunol19984855445509822265
- OlinJWAre anticardiolipin antibodies really important in thromboangiitis obliterans (Buerger’s disease)?Vasc Med20027425725812710839
- Pereira de GodoyJMBraileDMBuerger’s disease and anticardiolipin antibodiesJ Cardiovasc Med (Hagerstown)2009101079279419455050
- SmolenJSYoungchaiyudUWeidingerPAutoimmunological aspects of thromboangiitis obliterans (Buerger’s disease)Clin Immunol Immunopathol1978112168177367656
- Klein-WeigelPFBimmlerMHempelPPattern of G-protein coupled receptor auto-antibodies in thromboangiitis obliterans (Buerger’s disease) and their removal by immunoadsorptionVasa201443534735225147011
- KethaSSCooperLTThe role of autoimmunity in thromboangiitis obliterans (Buerger’s disease)Ann N Y Acad Sci20131285152523510296
- FarberowNLNehemkisAMIndirect self-destructive behavior in patients with Buerger’s diseaseJ Pers Assess19794318696430334
- DiehmCSchäferMDas Buerger-Syndrom (Thrombangiitis obliterans) Geschichte, Epidemiologie, Pathologie, Klinik, Diagnostik und Therapie [The Buerger’s syndrome (thrombangiitis obliterans) History, epidemiology, pathology, clinic, diagnostic, and therapy]Berlin; Heidelberg; New YorkSpringer Verlag1993
- ShionoyaSDiagnostic criteria of Buerger’s diseaseInt J Cardiol198866suppl 1S243S245
- Klein-WeigelPFRichterJGThromboangiitis obliterans (Buerger’s disease)Vasa201443533734625147010
- SasakiSSakumaMKuniharaTYasudaKDistribution of arterial involvement in thromboangiitis obliterans (Buerger’s disease): results of a study conducted by the Intractable Vasculitis Syndromes Research Group in JapanSurg Today200030760060510930225
- ShionoyaSBanINakataYMatsubaraJHiraiMKawaiSInvolvement of the iliac artery in Buerger’s disease (pathogenesis and arterial reconstruction)J Cardiovasc Surg (Torino)19781916976
- WysokinskiWEKwiatkowskaWMaslowskiLWitkiewiczWKowal-GierczakBBuerger’s disease in two brothers: iliac artery occlusion by thromboangiitis obliterans-case reportsAngiology19984954094149591534
- BecitNUnlüYKoçakHCevizMInvolvement of the coronary artery in a patient with thromboangiitis obliterans. A case reportHeart Vessels200216520120312181595
- CalgüneriMOztürkMAAyHBuerger’s disease with multisystem involvement. A case report and a review of the literatureAngiology200455332532815156267
- DrakeMEJrWiniwarter-Buerger disease (‘thromboangiitis obliterans’) with cerebral involvementJAMA198224815187018727120607
- HartenPMüller-HuelsbeckSRegensburgerDLoefflerHMultiple organ manifestations in thromboangiitis obliterans (Buerger’s disease). A case reportAngiology19964744194258619517
- SiddiquiMZReisEDSoundararajanKKersteinMDBuerger’s disease affecting mesenteric arteries: a rare cause of intestinal ischemia – a case reportVasc Surg200135323523811452353
- FazeliBModagheghHRavraiHKazemzadehGThrombophlebitis migrans as a footprint of Buerger’s disease: a prospective-descriptive study in north-east of IranClin Rheumatol2008271555717554578
- FagrellBLundbergGA simplified evaluation of vital capillary microscopy for predicting skin viability in patients with severe arterial insufficiencyClin Physiol1984454034116541549
- RanftJLammersenTHeidrichHIn-vivo capillary-microscopical findings in patients with thromboangiitis obliterans, progressive systemic scleroderma, and rheumatoid arthritis, respectivelyKlin Wochenschr198664199469503784444
- LawrencePFLundOIJimenezJCMuttalibRSubstitution of smokeless tobacco for cigarettes in Buerger’s disease does not prevent limb lossJ Vasc Surg200848121021218589234
- LieJTThromboangiitis obliterans (Buerger’s disease) and smokeless tobaccoArthritis Rheum19883168128133382454
- CooperLTHendersonSSBallmanKVA prospective, case-control study of tobacco dependence in thromboangiitis obliterans (Buerger’s Disease)Angiology2006571737816444459
- HootenWMBrunsHKHaysJTInpatient treatment of severe nicotine dependence in a patient with thromboangiitis obliterans (Buerger’s disease)Mayo Clin Proc19987365295329621859
- Jiménez-RuizCADaleLCAstray MochalesJVelázquez BuendíaLde Granda OriveIGuirao GarcíaASmoking characteristics and cessation in patients with thromboangiitis obliteransMonaldi Arch Chest Dis200665421722117393667
- BalmfordJLeifertJASchulzCElzeMJaehneAImplementation and effectiveness of a hospital smoking cessation service in GermanyPatient Educ Couns201494110310924176610
- RigottiNAMunafoMRSteadLFInterventions for smoking cessation in hospitalized patientsCochrane Database Syst Rev20073CD00183717636688
- KhatiIMenvielleGCholletAYounèsNMetadieuBMelchiorMWhat distinguishes successful from unsuccessful tobacco smoking cessation? Data from a study of young adults (TEMPO)Prev Med Rep2015267968526844137
- FiessingerJNSchäferMTrial of iloprost versus aspirin treatment for critical limb ischaemia of thromboangiitis obliterans. The TAO StudyLancet199033586895555571689791
- The European TAO Study GroupOral iloprost in the treatment of thromboangiitis obliterans (Buerger’s disease): a double-blind, randomised, placebo-controlled trialEur J Vasc Endovasc Surg19981543003079610341
- BozkurtAKKöksalCDemirbasMYA randomized trial of intravenous iloprost (a stable prostacyclin analogue) versus lumbar sympathectomy in the management of Buerger’s diseaseInt Angiol200625216216816763533
- BozkurtAKCengizKArslanCA stable prostacyclin analogue (iloprost) in the treatment of Buerger’s disease: a prospective analysis of 150 patientsAnn Thorac Cardiovasc Surg201319212012522971807
- CacioneDGBaptista-SilvaJCMacedoCRPharmacological treatment for Buerger’s diseaseCochrane Database Syst Rev20162CD011033 Update in: Cochrane Database Syst Rev. 2016;3:CD01103326828199
- HashimotoAItoHSatoYFujiwaraYAutomated intermittent bolus infusion for continuous sciatic nerve block: a case reportMasui201160787387521800674
- ParaskevasKITrigkaAASamaraMSuccessful intravenous regional sympathetic blockade (Bier’s Block) with guanethidine and lidocaine in a patient with advanced Buerger’s Disease (thromboangiitis obliterans)-a case reportAngiology200556449349616079935
- SaddlerJMCrosseMMIschaemic pain in Buerger’s disease. Report of a female patient receiving long-term local analgesiaAnaesthesia19884343053062454039
- DonasKPSchulteSKtenidisKHorschSThe role of epidural spinal cord stimulation in the treatment of Buerger’s diseaseJ Vasc Surg200541583083615886668
- Vaquer QuillsLBlasco GonzálezLAsensio SamperJVillanueva PérezVLLópez AlarcónMDDe Andrés IbáñezJEpidural neuro-stimulation of posterior funiculi for the treatment of Buerger’s diseaseNeuromodulation200912215616022151290
- InadaKIwashimaYOkadaAMatsumotoKNonatherosclerotic segmental arterial occlusion of the extremityArch Surg197410856636674829784
- SayinABozkurtAKTüzünHVuralFSErdogGOzerMSurgical treatment of Buerger’s disease: experience with 216 patientsCardiovasc Surg1993143773808076063
- ShionoyaSBanINakataYMatsubaraJHiraiMKawaiSSurgical treatment of Buerger’s diseaseJ Cardiovasc Surg (Torino)19802117784
- SasajimaTKuboYInabaMGohKAzumaNRole of infrainguinal bypass in Buerger’s disease: an eighteen-year experienceEur J Vasc Endovasc Surg19971321861929091153
- KawaradaOAyabeSYotsukuraHSubintimal angioplasty of lengthy femorotibial total occlusion in Buerger’s diseaseJ Endovasc Ther201320457858123914872
- GrazianiLMorelliLPariniFClinical outcome after extended endovascular recanalization in Buerger’s disease in 20 consecutive casesAnn Vasc Surg201226338739522285343
- SandnerTADegenhartCBecker-LienauJReiserMFTreitlMTherapie peripherer Gefäßstenosen und –verschlüsse bei Thrombangiitis obliterans [Therapy of peripheral vessel stenosis and occlusion in patients with thromboangiitis obliterans]Radiologe20105010887893 German20717643
- HodgsonTJGainesPABeardJDThrombolysis and angioplasty for acute lower limb ischemia in Buerger’s diseaseCardiovasc Intervent Radiol19941763333357882401
- BozkurtAKBeşirliKKöksalCSurgical treatment of Buerger’s diseaseVascular200412319219715586528
- SahaKChabraNGulatiSMTreatment of patients with thromboangiitis obliterans with cyclophosphamideAngiology200152639940711437030
- Gur’evaMSBaranovAABagrakovaSVKurdiukovAAPul’s-terapiia gliukokortikoidami i tsiklofosfamidom v lechenii obliteriruiushchego trombangiita [Pulse-therapy with glucocorticoids and cyclophosphamide in the treatment of thromboangiitis obliterans]Klin Med (Mosk)200381105357 Russian
- BodaZUdvardyMRázsóKStem cell therapy: a promising and prospective approach in the treatment of patients with severe Buerger’s diseaseClin Appl Thromb Hemost200915555256018818231
- DurduSAkarARAratMSancakTErenNTOzyurdaUAutologous bone-marrow mononuclear cell implantation for patients with Rutherford grade II–III thromboangiitis obliteransJ Vasc Surg200644473273916926085
- LawallHBramlagePAmannBTreatment of peripheral arterial disease using stem and progenitor cell therapyJ Vasc Surg201153244545321030198
- LeeKBKangESKimAKStem cell therapy in patients with thromboangiitis obliterans: assessment of the long-term clinical outcome and analysis of the prognostic factorsInt J Stem Cells201142889824298340
- MotukuruVSureshKRVivekanandVRajSGirijaKRTherapeutic angiogenesis in Buerger’s disease (thromboangiitis obliterans) patients with critical limb ischemia by autologous transplantation of bone marrow mononuclear cellsJ Vasc Surg2008486 suppl53S60S19084740
- TeraaMSprengersRWvan der GraafYPetersCEMollFLVerhaarMCAutologous bone marrow-derived cell therapy in patients with critical limb ischemia: a meta-analysis of randomized controlled clinical trialsAnn Surg2013258692292923426345
- BenoitEO’DonnellTFPatelANSafety and efficacy of autologous cell therapy in critical limb ischemia: a systematic reviewCell Transplant201322354556222490340
- KinoshitaMFujitaYKatayamaMLong-term clinical outcome after intramuscular transplantation of granulocyte colony stimulating factor-mobilized CD34 positive cells in patients with critical limb ischemiaAtherosclerosis2012224244044522877866
- MatobaSTatsumiTMuroharaTLong-term clinical outcome after intramuscular implantation of bone marrow mononuclear cells (Therapeutic Angiogenesis by Cell Transplantation [TACT] trial) in patients with chronic limb ischemiaAm Heart J200815651010101819061721
- MoriyaJMinaminoTTatenoKLong-term outcome of therapeutic neovascularization using peripheral blood mononuclear cells for limb ischemiaCirc Cardiovasc Interv20092324525420031722
- AmannBLuedemannCRateiRSchmidt-LuckeJAAutologous bone marrow cell transplantation increases leg perfusion and reduces amputations in patients with advanced critical limb ischemia due to peripheral artery diseaseCell Transplant200918337138019500466
- InanMAlatIKutluRHarmaAGermenBSuccessful treatment of Buerger’s Disease with intramedullary K-wire: the results of the first 11 extremitiesEur J Vasc Endovasc Surg200529327728015694801
- KimDIKimMJJohJHAngiogenesis facilitated by autologous whole bone marrow stem cell transplantation for Buerger’s diseaseStem Cells20062451194120016439614
- PatwaJJKrishnanABuerger’s disease (thromboangiitis obliterans)-management by ilizarov’s technique of horizontal distraction. A retrospective study of 60 casesIndian J Surg2011731404722211037
- BaumannGStanglVKlein-WeigelPStanglKLauleMEnke-MelzerKSuccessful treatment of thromboangiitis obliterans (Buerger’s disease) with immunoadsorption: results of a pilot studyClin Res Cardiol2011100868369021380608
- Klein-WeigelPKöningCHärtwigAImmunadsorption bei Thrombangiitis obliterans – eine vielversprechende therapeutische Option. Behandlungsergebnisse einer konsekutiven Patientenkohorte in der klinischen Routineversorgung [Immunoadsorption in thromboangiitis obliterans: a promising therapeutic option: results of a consecutive patient cohort treated in clinical routine care]Zentralbl Chir20121375460465 German23136105
- Klein-WeigelPFBimmlerMHempelPPattern of G-protein coupled receptor auto-antibodies in thromboangiitis obliterans (Buerger’s disease) and their removal by immunoadsorptionVasa201443534735225147011
- Todoli ParraJAHernándezMMArrébola LópezMAEfficacy of bosentan in digital ischemic ulcersAnn Vasc Surg2010245690.e1690.e4
- De HaroJAcinFBledaSVarelaCEsparzaLTreatment of thromboangiitis obliterans (Buerger’s disease) with bosentanBMC Cardiovasc Disord201212522333218
- BörnerCHeidrichHLong-term follow-up of thromboangiitis obliteransVasa199827280869612110
- MyerSACase studies: what a difference a nurse makesAACN Clin Issues1995645765877493261
- Frost-RudeJANunneleeJDSpanerSBuerger’s diseaseJ Vasc Nurs200018412813011995294