Abstract
Aim:
The aim was to describe how a multidisciplinary medical assessment changed the distribution of long-term sickness absentees between three different forms of social security support during a period of eleven years.
Methods:
The study group (n = 1002) consisted of persons on long-term sickness absence who were referred to a multidisciplinary medical assessment by the Social Insurance Office in Stockholm, Sweden between 1998 and 2007. Register data from the years 1993–2008 were linked to the study group. A calculation was provided for the number of days per person and year on unemployment benefits, sickness benefits, and disability pension, five years before, during, and five years after the assessment. Also, differences in the average number of days per person and year were calculated with one-way analysis of variance.
Results:
The number of days on sickness benefits increased up to the time of multidisciplinary medical assessment, from 69 to 218 days on average. After the assessment there was a decrease in the average number of days on sickness benefits, from 218 to 16 days. Before the assessment the number of days on disability pension was 21, but this increased after the assessment from 104 days to an average of 272 days five years after the assessment. There were age differences regarding number of compensated days, and these were particularly pronounced for disability days after the assessment. Further, there were significant differences between types of diagnosis in relation to average days on disability pension after the assessment.
Conclusion:
The study shows that after a multidisciplinary medical assessment there is a rapid increase in disability pension and a dramatic decrease in sickness benefits. The results indicate that for a large number of persons, a Social Insurance Office referral to an assessment does not improve their chances of returning to work, but rather seems to justify disability pension.
Introduction
Long-term sickness absence (SA) and disability pension (DP) are seen as major public health and socioeconomic problems in many Western countries.Citation1,Citation2 Research during recent decades has mainly focused on the reasons why individuals and groups of individuals become sick-listed or take early retirement due to sickness and incapacity, but also on why the numbers have varied over time.Citation3–Citation5
Less research has been published on the effects of SA or having been granted DP. However, there are a few studies on the short- or long-term effects of having been on different forms of social security support.Citation6,Citation7 It has been shown that long periods of SA reduce the likelihood of returning to work and increase the risk of DP.Citation4,Citation8–Citation13 AndrenCitation14 found that SA is a strong predictor for exit from the labor market through full or partial DP, unemployment, or emigration. Although other factors such as age and educational level affect the risk of DP after long spells of SA, the length of SA remains an important factor.Citation15 Wallman et alCitation16 found that the number of annual days of SA had the best prognostic precision for DP compared with other predictors such as age, length of education, and geographical area. Several other studies have also found that previous SA increases the risk of long-term SA and DP.Citation11,Citation17–Citation21
Also, a number of studies have indicated that factors other than health are important in association with return-to-work (RTW) or DP.Citation7,Citation22–Citation26 Low socioeconomic position, exposures to physical, psychosocial, or organizational factors at work, and high age increased the risk of DP.Citation27
In Sweden, a correlation between the number of long-term SA cases and trends in numbers of new DPs has been reported.Citation28 Both DP and compensation for long-term SA are granted on the basis of reduction of work capacity due to a disease or an injury.Citation29 The individual’s social or labor market conditions are not formally assumed to affect the decision. For this reason, the assessment of medical conditions related to the individual’s work capacity is crucial. This is particularly important in relation to prolonged cases of SA and in deciding about permanent DP. However, in many cases of long-term SA the severity of the disease, its prognosis, and the rehabilitation potential of the individual are not well known by the Social Insurance Office (SIO). In the Swedish social security administration, different forms of intensified medical examinations are used to meet the need for a systematic assessment of health conditions, work capacity, and useful medical and vocational rehabilitation measures. The results of such examinations are assumed to improve the decision about whether the individual can RTW with or without rehabilitation measures. As DP is in most cases irreversible, it involves severe financial and social consequences for the individual and high costs for society.
Thus, the idea behind the SIO’s referral of an individual to a systematic multidisciplinary medical assessment (MMA) is to get better information about the individual’s health and work capacity. The primary assumption is that MMA provides a valid foundation for the insurance officials to decide on the sickness absentee’s right to benefits and need for further work-related rehabilitation. However, it is known that the MMA is in most cases conducted at a relatively late stage of an SA process and that a large number of individuals will not return to work after the MMA.Citation10,Citation11,Citation30 What is not known is the mobility between different forms of social security compensation that takes place after an MMA, and to what degree the selection in this mobility is primarily due to health conditions or to other factors such as age, education, or sex.
In a Danish study (page 300),Citation25 RTW was measured in terms of “whether one received public transfer income or not in a given time period” and some 7,800 individuals who had been on SA for more than 8 weeks were followed over 2–3 years (page 300). After one year, the majority had no public transfer income, and was thus assumed to have returned to work, and within 2 years almost 60% received no public transfer. After that there was no increase and about 40% remained in some form of public compensation. RTW decreased with increasing age, low education, low income, female sex, and immigrant status.
The present study describes how the use of different kinds of social security benefits has developed over a period of eleven years among long-term sickness absentees that have undergone an MMA. The individuals are followed five years before the MMA and five years after. The main aim was to investigate the number of days of different forms of social security compensation among long-term sickness absentees, five years before, during, and five years after MMA. Specific aims were to analyse the shifts in the number of days on social security benefits per person and year with respect to three forms of compensation: unemployment benefits, sickness benefits, and DP. Further objectives were to study differences in the average number of days for each form of compensation related to sex, age, education, country of birth, and diagnosis.
Methods
Participants and procedure
The study group consisted of persons on long-term SA who underwent an MMA at the Diagnostic Center (DC), Karolinska University Hospital, Stockholm, Sweden, from 1998 to 2007 (see earlier studiesCitation31–Citation33). At the MMA, all individuals completed a comprehensive questionnaire before medical examinations. The questionnaire included items about socio-demographics, social life, lifestyle, health, and symptoms. Each individual was examined on three different occasions within three weeks by three board-certified specialists in psychiatry, orthopedic surgery, and rehabilitation medicine, respectively. For each individual, the three specialists thereafter agreed on a joint statement with respect to diagnoses, level of work capacity, prognosis of return to work, and recommendation of medical and vocational rehabilitation measures. Most of the persons had been on SA for more than one year and had been referred to a MMA by the SIO. A total of 1,006 persons were examined over the period from 1998 to 2007, and the number of persons referred varied between 25 and 181 for the individual year.
Exclusion criteria
Persons who were entitled to old age pension when they turned 65 years of age (n = 14) or died (n = 20) during the follow-up period were excluded from the study group for the years post these events. Immigrants (n = 14) and emigrants (n = 10) were excluded for the years they were not resident in Sweden.
Study design
presents a description of the longitudinal study design. The persons were followed five years before, during, and five years after the year of the MMA. Information about the individuals was collected during the MMA. The follow-up data originate from databases from Statistics Sweden (LISA) and the Swedish Social Insurance Agency (MiDAS) about the annual numbers of days on different kinds of social security compensation for each individual during the period 1993–2008, linked to the study group. Individuals who underwent MMA after 2004 could not be followed during all five years. Thus the number of cases was reduced for each year after 2004 by 25, 144, 235, and 351.
Figure 1 Design of the study. Number of years and participating individuals before (t-5 to t-1), during (t0), and after (t1 to t5) a multidisciplinary medical assessment at the diagnostic center.

Background variables
The background factors used were sex, age, education, country of birth, and diagnoses, categorized as follows: age categories (21–39, 40–49, 50–63 years), educational level (elementary, high school, university), country of birth (Sweden, other than Sweden), type of diagnosis (psychiatric, somatic, psychiatric and somatic, or none).
Outcome variables
Unemployment benefits: number of days per person and year with unemployment compensation, labor market education, sheltered employment. Days with part-time compensation were added to make full days.
Sickness benefits: number of days per person and year on sickness benefits, rehabilitation allowance, occupational injury allowance, preventive sick leave allowance, disease carrier’s allowance. Days on part-time compensation were added to make full days.
Disability pension: number of days per person and year with permanent or temporary DP. Days on part-time compensation were added to make full days.
Statistical analyses
Descriptive statistics were used to illustrate how the average number of days on different kinds of social security benefits had developed. The data were computed in two steps. In the first step, a calculation was provided for the number of days per person and year on unemployment benefits, sickness benefits, and DP. This was done for each year over the eleven-year period, ie, five years before the MMA, during the MMA year, and five years after the MMA. The information was based on register data for the period 1993–2008. In the second step, differences in the average number of days per person and year were calculated with one-way analysis of variance (ANOVA) for each form of compensation related to sex, age, education, country of birth, and diagnosis (F-values and df were computed but not presented in ). Also, cross-tabulation of sex by background variables was analyzed using the Chi-square test (). All P-values reported are statistically significant at the 5% level. Data were analysed using SPSS/PASW statistical programme package (version 17; SPSS Inc, Chicago, IL).
Table 1 Distribution of women and men by age, education, country of birth, and type of diagnosis at MMA (n = 1002)
Table 2 Number of days on disability pension, sickness benefits, and unemployment related to sex, age, education, country of birth, and diagnosis
Ethics
The study was approved by the Regional Ethical Review Board in Stockholm, Sweden (1995-149, 2006/1281-31, 2008/71-31/5, 2008/1051-31/12, and 2010/448-32).
Results
shows the distribution of women and men in the study population with respect to age, educational level, country of birth, and diagnostic category. All persons had been long-term sickness absent, all for at least one year.Citation31 There was a significant difference between the type of diagnosis with respect to sex. However, there were no significant differences between the sexes with respect to age, education, or country of birth. further shows that most persons had both a psychiatric and a somatic diagnosis.
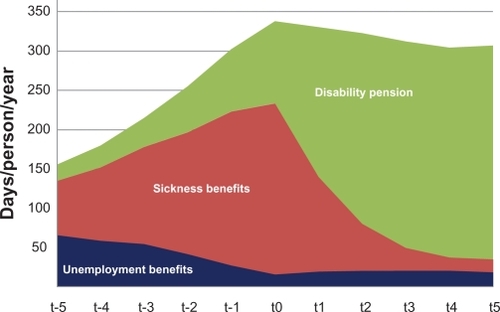
shows the results of a cumulative description of how the average number of days on different kinds of social security benefits had developed during the period of eleven years. Five years before the MMA, about 208 days in a year were not compensated through SA, DP, or unemployment benefits. Five years after the MMA, the group had on average only 64 days without compensation. The average number of days on unemployment benefits decreased from 66 to 16 days per person and year until the time of the MAA, but after the MMA there was no change. The number of days on sickness benefits increased until the time of MMA from 69 to 218 days on average. After the MMA there was a rapid decrease in the number of days on sickness benefits, from 218 to 16 days on average. Before the MMA, the average number of days on DP was 21. Only one individual had a permanent DP before the MMA, but a few individuals had different forms of temporary DP. The average number of days on DP increased gradually after the MMA, from an average of 104 days in the first year, to an average of 272 days five years after the MMA. There is a general shift from high numbers of days on sickness compensation in the years before the MMA, to high numbers of days on DP after the MMA. Five years after the MMA, about 20% had returned to work. Fewer elderly persons, persons not born in Sweden, and persons with both somatic and psychiatric diagnoses returned to work compared to other groups.
Figure 2 Number of benefit days based on the average value per person and year on unemployment benefit, sickness benefit, disability pension, 5 to 1 years before multidisciplinary medical assessment (MMA) (t-5 to t-1), and after MMA (t1 to t5) for individuals diagnosed in the period 1998–2007.
presents the differences in average number of days on the three different types of social security benefits, with respect to sex, age, educational level, country of birth, and type of diagnosis over time. There were no significant differences between the sexes in relation to average days on sickness benefits, disability benefits, or unemployment benefits, neither before nor after the MMA. Age differences in the number of compensated days occurred more frequently, and were particularly pronounced for disability days after the MMA. A tendency towards fewer days on unemployment benefits before and after the MMA was also observed in the oldest age group (50–63 years). There were no significant differences between different levels of education and sickness benefit or unemployment benefits. However, it emerges from the data that individuals with a low level of education had significantly lower numbers of days on DP during the years after the MMA.
also shows that there were no clear associations between the country of birth and sickness benefit, but individuals from countries other than Sweden had a significantly higher rate of number of days with DP after the MMA. Further, there were no significant differences between types of diagnosis in relation to average days on DP before the MMA, but there were significant differences between types of diagnosis after the MMA. There were no clear patterns in relation to sickness benefit before or after the MMA. As expected, individuals who had psychiatric diagnoses, as well as individuals with a combination of psychiatric and somatic diagnoses, also had on average a larger number of days on DP after the MMA.
Discussion
The study describes how the use of different kinds of social security benefits developed five years before and five years after MMA. The results show that the average number of days on DP increased rapidly after the MMA, and that the number of days on sickness benefits decreased concurrently. The average number of days on unemployment benefits decreased until the MMA, but remained constant after the MMA.
The results indicate that a referral of the SIO to an MMA did not improve the chances of RTW for large numbers of individuals. Furthermore, the results of this study illustrate that the selection between different forms of social security compensation that takes place after an MMA, and the degree to which it takes place, is partly due to background factors such as age, education, and country of birth, but also related to diagnosis. Age and country of birth are strongly associated with a higher number of days on disability benefits as older individuals and individuals born outside Sweden had a significantly higher number of benefits after MMA. Persons with psychiatric diagnoses as well as those with combinations of somatic and psychiatric diagnoses had a higher average number of days on DP. This may imply that modern working life is less adjustable to psychiatric disorders such as cognitive malfunctioning, phobias, anxieties, or unstable moods compared to somatic disabilities.Citation34,Citation35 To some degree these psychiatric disorders may also have workplace-related grounds.Citation36–Citation39
The results of this study confirm the findings of two previous Swedish studies of transition from SA to DP.Citation14,Citation15 This is also in line with a Danish follow-up of long-term sick-listed individuals,Citation25 and is also in concordance with a recent review of factors affecting the risk of DP.Citation27 However, the fact that conducting an MMA does reduce the numbers who were granted DP and stability in the distribution of factors affecting such as a decision has not previously been studied.
It should be noted, however, that the present study is not a controlled clinical trial. Generally, a high proportion of individuals who have been long-term sickness absent stand a high risk for DP. Conducting MMA earlier during a sick-leave spell might lead to more adequate interventions, promoting RTW.
Methodological considerations
The strength of this study was its longitudinal design, and that the MMAs were carried out in the same manner for all persons. There was also good quality of register data over 16 years (1993–2008) and few missing cases over these years. However, the study has some limitations: with regard to referral of individuals from the SIO, the selection process might have changed over the years (1998–2007), or might differ between SIO officials, and the criteria for SIO selection are unknown.Citation31 Some variables that can impact on the selection process are probably health status, education, economic and labor market situation of the individual, and changes in the insurance system. Not all of the individuals included in this study (n = 1002) could be followed up for a full 5-year period. A total of 39% were lost to follow-up in the fifth year due to a short follow-up period (36%), due to death (2%), or emigration (1%).
Conclusion
The study shows that after a multidisciplinary medical assessment, there was a rapid increase in DP and a corresponding dramatic decrease in sickness benefits. The fact that the multidisciplinary medical assessment was conducted at a late stage of the process of sickness absence seems to lead to a decision to grant DP in a large number of cases. This may be connected with a number of factors such as deterioration of health, labor market difficulties, or lack of efficient vocational rehabilitation. Those factors need to be further researched.
Acknowledgements
This study was financially supported by the County Council of Stockholm and the Swedish Council for Working Life and Social Research.
Disclosure
No conflicts of interest were declared in relation to this paper.
References
- IlmarinenJEAging workersOccup Environ Med200158854655211452053
- OECDSickness, disability and work, breaking the barriers, Sweden: will the recent reforms make it? Directive for employment, labor and social affairs, organization for economic co-operation and development. OECD;2009
- LidwallULong-term sickness absence Aspects of society, work, and family PhD thesis, Stockholm: Karolinska Institutet, Sweden;2010
- HansenAEdlundCBranholmIBSignificant resources needed for return to work after sick leaveWork200525323124016179772
- LidwallUMarklundSTrends in long-term sickness absence in Sweden 1992–2008: the role of economic conditions, legislation, demography, work environment, and alcohol consumptionInt J Soc Welfare201010.1111/j.1468-2397.2010.00744.x
- KarlssonNECarstensenJMGjesdalSAlexandersonKARisk factors for disability pension in a population-based cohort of men and women on long-term sick leave in SwedenEur J Public Health200818322423118245150
- KrokstadSJohnsenRWestinSSocial determinants of disability pension: a 10-year follow-up of 62000 people in a Norwegian county populationInt J Epidemiol20023161183119112540720
- AdamsHEllisTStanishWDSullivanMJPsychosocial factors related to return to work following rehabilitation of whiplash injuriesJ Occup Rehabil200717230531517486435
- WaddellGSawneyPBack pain, incapacity for work, and social security benefits: an international review and analysisPress RSoMLondon, United Kingdom2002
- AhlgrenABergrothAEkholmJSchuldtKWork resumption after vocational rehabilitation: a follow-up two years after completed rehabilitationWork200728434335417522455
- AhlgrenABromanLBergrothAEkholmJDisability pension despite vocational rehabilitation? A study from six social insurance offices of a countyInt J Rehabil Res2005281334215729095
- EdenLAnderssonIHEjlertssonReturn to work still possible after several years as a disability pensioner due to musculoskeletal disorders: a population-based study after new legislation in Sweden permitting “resting disability pension”Work200626214715516477107
- BurstromBNylenLClaytonSWhiteheadMHow equitable is vocational rehabilitation in Sweden? A review of evidence on the implementation of a national policy frameworkDisabil Rehabil201133645346620528191
- AndrenDLong-term absenteeism due to sickness in Sweden. How long does it take and what happens after?Eur J Health Econ200781415017225127
- AndrenDFirst exits from the Swedish labor market due to disabilityPopul Res Policy Rev200827227238
- WallmanTWedelHPalmerESick-leave track record and other potential predictors of a disability pension. A population based study of 8,218 men and women followed for 16 yearsBMC Public Health2009910419368715
- VaezMRylanderGNygrenAAsbergMAlexandersonKSickness absence and disability pension in a cohort of employees initially on long-term sick leave due to psychiatric disorders in SwedenSoc Psychiatry Psychiatr Epidemiol200742538138817450454
- LindbergPVingardEJosephsonMAlfredssonLRetaining the ability to work-associated factors at workEur J Public Health200616547047516162597
- HansenAEdlundCHenningssonMFactors relevant to a return to work: a multivariate approachWork200626217919016477110
- GjesdalSRingdalPRHaugKMaelandJGPredictors of disability pension in long-term sickness absence: results from a population-based and prospective study in Norway 1994–1999Eur J Public Health200414439840515542877
- KivimakiMFerrieJEHagbergJDiagnosis-specific sick leave as a risk marker for disability pension in a Swedish populationJ Epidemiol Community Health2007611091592017873230
- ManssonNOMerloJThe relation between self-rated health, socioeconomic status, body mass index and disability pension among middle-aged menEur J Epidemiol2001171656911523578
- MelchiorMNiedhammerIBerkmanLFGoldbergMDo psychosocial work factors and social relations exert independent effects on sickness absence? A six year prospective study of the GAZEL cohortJ Epidemiol Community Health200357428529312646546
- Sjogren-RonkaTOjanenMTLeskinenEKTmustalampiSMalkiaEAPhysical and psychosocial prerequisites of functioning in relation to work ability and general subjective well-being among office workersScand J Work Environ Health200228318419012109558
- StoltenbergCDSkovPGDeterminants of return to work after long-term sickness absence in six Danish municipalitiesScand J Public Health201038329930820056786
- VirtanenMKivimakiMVahteraSickness absence as a risk factor for job termination, unemployment, and disability pension among temporary and permanent employeesOccup Environ Med200663321221716497865
- BjorngaardJHKrokstadSJohnsenEpidemiologisk forkning om uförepensjon i NordenNorsk Epidemiologi200919103114 [Epidemiological research about disability pension in the Nordic countries, in Norwegian, abstract in English].
- Skogman ThoursiePLidwallPMarklundSTrends in new disability pensionsGustafssonRLundbergIWorklife and health in Sweden 2004Stockholm, SwedenNational Institute for Working Life2005205222
- SFS 1962:381Lagen om allmän försäkring (AFL)Stockholm, Sweden1962 [The National Insurance Act, Government Offices of Sweden, in Swedish].
- AhlgrenABergrothAEkholmJWork resumption or not after rehabilitation? A descriptive study from six social insurance officesInt J Rehabil Res200427317118015319686
- SvedbergPSalmiPHagbergJLundhGLinderJAlexandersonKDoes multidisciplinary assessment of long-term sickness absentees result in modification of sick-listing diagnoses?Scand J Public Health201038665766320534634
- SalmiPSvedbergPHagbergJLundhGLinderJAlexandersonKMultidisciplinary investigations recognize high prevalence of co-morbidity of psychiatric and somatic diagnoses in long-term sickness absenteesScand J Public Health2009371354219141553
- SalmiPSvedbergPHagbergJLundhGLinderJAlexandersonKOutcome of multidisciplinary investigations of long-term sickness absenteesDisabil Rehabil200931213113718608401
- MuschallaBLindenMOlbrichDThe relationship between job-anxiety and trait-anxiety–a differential diagnostic investigation with the Job-Anxiety-Scale and the State-Trait-Anxiety-InventoryJ Anxiety Disord201024336637120207103
- LindenMMuschallaBAnxiety disorders and workplace-related anxietiesJ Anxiety Disord200721346747416890399
- HensingGAnderssonLBrageSIncrease in sickness absence with psychiatric diagnosis in Norway: a general population-based epidemiologic study of age, gender and regional distributionBMC Med200641916923198
- GjesdalSRingdalPRHaugKMaelandJGLong-term sickness absence and disability pension with psychiatric diagnoses: a population-based cohort studyNord J Psychiatry200862429430118622882
- LinderJEkholmKSJansenGBLundhGEkholmJLong-term sick leavers with difficulty in resuming work: comparisons between psychiatric-somatic comorbidity and monodiagnosisInt J Rehabil Res2009321203519648800
- AnderssonLNymanCSSpakFHensingGHigh incidence of disability pension with a psychiatric diagnosis in western Sweden. A population-based study from 1980 to 1998Work200626434335316788254