
Abstract
Background
Low-molecular-weight heparin (LMWH) is an effective means of preventing venous thromboembolism (VTE) among medical inpatients. Compared with unfractionated heparin, LMWH is equivalent or superior in efficacy and risk of bleeding. Despite its advantages, LMWH is underused in VTE prophylaxis for general-medicine patients hospitalized at our institution. Thus, a quality improvement (QI) initiative was undertaken to increase LMWH use for VTE prophylaxis among medical patients hospitalized on resident teaching services.
Methods
A QI team was formed, consisting of resident and attending physicians with pharmacy leaders. A systems analysis was performed, which showed gaps in resident knowledge as the greatest barrier to LMWH use. A knowledge translation framework was used to improve prescribing practices. Several Plan–Do–Study–Act cycles were executed, including resident-of-resident and pharmacist-of-resident education with performance audit and feedback.
Results
Pharmacist-of-resident education elicited the largest improvement and was sustained through a recurring pharmacist-led, interprofessional educational session as part of the monthly hospital orientation for incoming residents. Data analysis showed a statistically significant increase in LMWH use among treatment-eligible hospitalized medical patients, from 12.1% to 69.2%, following intervention (P<0.001). Extrapolated over 1 year, this improvement conserved 9,490 injections and nearly 791 hours of nurse time.
Conclusions
This QI project indicates that an interprofessional education intervention can lead to sustainable improvement in resident prescribing practices. This project also highlights the value of knowledge translation for the design of tailored interventions in QI initiatives.
Introduction
Venous thromboembolism (VTE) is a major cause of morbidity and death among hospitalized medical patients.Citation1 Current guidelines recommend pharmacologic prophylaxis for these patients at high risk of VTE.Citation2,Citation3 Options include unfractionated heparin (UFH) and low-molecular-weight heparins (LMWHs). Compared with UFH, LMWH offers a similar efficacy with lower risks of both bleeding and heparin-induced thrombocytopenia.Citation4,Citation5 In addition, LMWH is dosed once daily rather than the two or three times daily regimen for UFH, thereby increasing patient adherence and saving time for administration.Citation6,Citation7 Thus, LMWH should be considered the high-value choice for pharmacologic VTE prophylaxis among therapy-eligible medical inpatients.Citation8,Citation9
Despite the benefits of LMWH, many US hospitals continue to use UFH for VTE prophylaxis.Citation10 Baseline data from January to April 2015 on inpatient general medicine teaching services at our institution have shown that <20% of patients eligible for VTE prophylaxis received LMWH. Further investigation detected a lack of awareness regarding the research evidence, benefits, and cost of LMWH as the primary reason behind prescriber choice of UFH at our institution.
Changing physician behavior is challenging, and many education interventions lead to only modest or inconsistent improvement in prescribing practices.Citation11 Knowledge translation (KT) is a relatively new term to describe the process of creating awareness and increasing the use of research evidence when making clinical decisions.Citation12 Lavis et alCitation13 offer the following five-step framework for KT, which may be useful for changing physician practice patterns:
What knowledge should be transferred (ie, what is the desired message or behavior)?
To whom should the knowledge be transferred (ie, who is the target audience)?
By whom should the knowledge be transferred (ie, who is the messenger)?
How should the knowledge be transferred (ie, what is the intervention or KT process)?
With what effect should the knowledge be transferred (ie, what is the desired outcome)?
Applying this KT framework to quality improvement (QI) initiatives offers an attractive approach to improving physician prescribing practices. Indeed, a recent Cochrane systematic review found that tailored interventions prospectively designed to overcome contextual barriers to implementation are an effective method to change physician performance.Citation14 QI initiatives have successfully increased overall rates of VTE prophylaxis in multiple settings.Citation15,Citation16 However, we were unable to find a report that specifically aimed to increase the use of LMWH over UFH for medical inpatients.
Given the gap between existing research evidence and physician practice at our institution, a QI project was initiated to increase LMWH use for VTE prophylaxis among patients on wards that receive general medicine teaching services.
Methods
This project is reported in accordance with the Standards for Quality Improvement Reporting Excellence 2.0 guidelines.Citation17 According to the policy activities that constitute research at Mayo Clinic, this work met criteria for operational improvement activities and did not require ethics review by the Institutional Review Board.
Context
This QI project involved collaboration of internal medicine residents and attending physicians with nurses and pharmacists from four general medicine teaching services at Mayo Clinic Hospital, Saint Mary’s Campus. Each of these services is composed of three interns (first-year residents), one senior resident (third-year resident), and one attending physician. Residents rotate on the service in 4- or 5-week blocks, and attending physicians rotate in 2-week blocks. Clinical pharmacists and pharmacy residents are part of the team and attend rounds with the general medical services on weekdays.
In May 2015, a team was formed to increase LMWH use for VTE prophylaxis among patients who received care from the four resident services. A systems analysis showed that VTE prophylaxis was most frequently ordered by interns as part of a computerized admission order set for newly hospitalized patients. The order set identified LMWH as the preferred option for VTE prophylaxis (for patients without renal dysfunction), but most interns continued to order UFH. Further investigation observed a lack of awareness regarding the research evidence and benefits of LMWH as the primary reason for most interns who chose UFH. For this reason, resident education was the primary focus of subsequent interventions.
Interventions
Using the Model for Improvement,Citation18 several Plan–Do–Study–Act (PDSA) cycles were performed between May and August 2015. Initial interventions consisted of resident-of-resident education in the form of didactics and posters placed in resident work areas. In addition, intern prescribing practices were audited, and resident-to-resident feedback was provided through email. Analysis of these interventions observed a small but measurable improvement in LMWH prescribing practices. Qualitative feedback from interns on the medical services indicated that some skepticism continued regarding the benefits of LMWH.
The focus of the next intervention was pharmacist-of-resident education. The decision to implement an interprofessional education intervention was based on qualitative feedback from residents during the systems analysis. Interns verbalized a strong sense of trust and respect toward the clinical expertise, judgment, and recommendations made by pharmacists on the medical unit.
At the start of each new resident rotation, a supervising clinical pharmacist (JGO) presented a 10-minute lecture about the QI project to residents, with specific data regarding safety, efficacy, costs, dosing, and periprocedural management of LMWH for VTE prophylaxis. Prescribing practices reflected a prompt and substantial improvement in LMWH use after the presentation. Subsequent PDSA cycles focused on sustainability by incorporating a standard pharmacist-led educational lecture into new-resident orientation on the first day of each clinical rotation. The benefits of this intervention appeared to reach a maximum effect by September 2015, at which time the project entered the sustainability phase, which consisted of a monthly, recurring pharmacist-led interprofessional education lecture during the new-resident rotation orientation.
From November 2015 to March 2016, the intervention was interrupted because of several competing pharmacy initiatives and relocation of the primary ward for the resident teaching services. In April 2016, the pharmacist-of-resident monthly didactic was restarted and was augmented by informal audit and feedback of interns’ prescribing practices by clinical pharmacists during rounds.
Study of the intervention and outcome measures
To measure this QI project’s effect on LMWH use, data were obtained from the hospital pharmacy database regarding the use of heparin (LMWH or UFH) for patients hospitalized on the wards of general medicine teaching services between January 1, 2015, and June 30, 2016. Given stakeholder concerns about the potential increased risk of bleeding among patients receiving LMWH compared with UFH, we also evaluated the balancing measure of major bleeding among patients hospitalized during the project timeline. Our definition of major bleeding, which is based on existing literature,Citation19 is a decrease in hemoglobin of ≥2.0 g/dL in a 48-hour period.
Analysis
For analysis purposes, LMWH use was quantified weekly as a proportion of all patients receiving thromboprophylaxis. To calculate this proportion, the sum of the number of patients receiving LMWH for the days of the given calendar week was the numerator, and the sum of the number of patients receiving LMWH or UFH for the days of the same week was the denominator. The process improvement efforts were implemented through multiple iterations of PDSA cycles undertaken from May through August 2015. Therefore, when evaluating the effectiveness of the overall improvement effort, we divided the study period into three phases: January through April 2015 (preintervention), May through August 2015 (intervention), and September 2015 through June 2016 (postintervention). Patients with renal failure (defined as creatinine >2 g/dL) were excluded from the analysis.
To account for potential underlying trends in LMWH use, we performed segmented regression.Citation20 The segmented regression model included terms to assess a linear trend in LMWH use before the initiation of the process improvement efforts, a step-change when the intervention was completed, and a potential change following intervention. As we were not interested specifically in modeling the changes in LMWH use during the intervention phase, the LMWH use data for this transition period were excluded rather than modeled as a separate segment.
The segmented regression analysis was performed with ordinary least-squares regression. The Durbin–Watson test was used to assess the assumption that the error terms associated with the weekly data points were uncorrelated. To supplement the segmented regression analysis, we compared demographic characteristics, heparin use, and bleeding complications among hospitalized patients who received LMWH vs UFH during the preintervention vs postintervention periods. In all cases, analyses were performed using SAS software (version 9.3; SAS Institute Inc).
Results
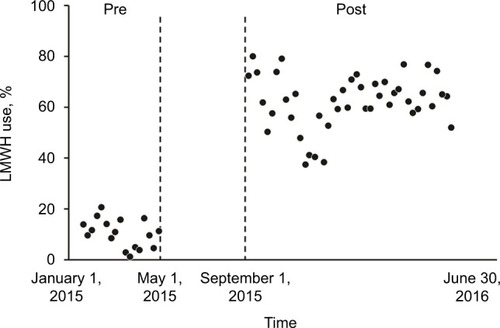
LMWH use over the study period is summarized in . The segmented regression analysis detected a significant increase (P<0.001) in the use of LMWH following the intervention, with no evidence of a trend over time during the preintervention period (P=0.34) or following intervention (P=0.26). The median (interquartile range) weekly LMWH use increased from 11% (5%–15%) during preintervention to 64% (58%–70%) during the postintervention phase.
Figure 1 Weekly LMWH use before and after the knowledge translation intervention.
Demographic characteristics of patients who received heparin were similar for preintervention and postintervention periods (). Among patients receiving some form of heparin during the preintervention, 90.5% received UFH on at least 1 day and 43.5% received UFH for 4 or more days. These percentages were significantly reduced (P<0.001) in the postintervention period, with 34.5% of patients receiving UFH on at least 1 day and 14.5% on 4 or more days (). The percentage of patients who had major bleeding did not differ significantly between the periods (3.6% preintervention vs 3.4% postintervention, P=0.82).
Table 1 Patient demographic characteristics, heparin use, and bleeding complications
To assess the effect of the intervention on institutional costs and resource use, we performed a post hoc analysis comparing number of injections and nursing medication administration time pre and postintervention. Assuming an average census of 24 patients per day who require VTE prophylaxis injections, we estimate that our intervention, sustained over 1 year, would directly save 9,490 injections. Assuming an average medication administration time of 5 minutes per UFH or LMWH injection, the direct saving of 9,490 injections would lead to an indirect saving of 790.8 hours of nurse time (equivalent to 0.38 full-time employment).
Discussion
A brief interprofessional educational intervention correlated with a significant change in resident prescribing practices. A monthly pharmacist-led didactic for each new group of residents resulted in a sustained increase in LMWH use for VTE prophylaxis in treatment-eligible patients, with a corresponding decrease in UFH prescribing and no change in the rate of major bleeding. In particular, this study showed that the use of KT principles to design a relatively simple low-cost QI intervention can lead to sustained change in resident prescribing in a clinical setting where frequent turnover occurs among physician learners.
Interpretation
Selecting the target audience is an essential step in the process of KT.Citation12,Citation13 Health care providers often work in large teams with member rotation in the hospital, which may make this process challenging. Using stakeholder interviews, we were able to identify the important role that the intern has in the selection of VTE prophylaxis on our general medicine teaching services. This finding not only enabled us to identify the target audience for KT, but also showed the specific knowledge gaps and barriers to LMWH use among these providers. The educational intervention was then tailored to address these gaps and facilitate effective KT.
Observations from the initial PDSA cycles suggested that pharmacist-based education had a greater effect on residents’ prescribing practices than peer-based education. Again, this determination fits into the framework of KT, which identifies the importance of the person from whom knowledge should be transferred. Although the content of the education was similar, informal feedback showed that residents tended to view information about the benefits of LMWH as more credible when it came from a content expert (ie, a pharmacist) rather than a peer. This finding is also consistent with existing research that has shown a positive correlation between teacher credibility and learner outcomes.Citation21
Clinical pharmacists have an important role in the care of hospitalized patients in medical wards. Pharmacist-led interventions can substantially alter physician prescribing habits and improve patient outcomes.Citation22,Citation23 However, the quality of the physician–pharmacist relationship appears to be a major determinant to the adoption of pharmacist recommendations by physicians.Citation24 Interprofessional education has been proposed as a method to improve the working relationships between doctors and pharmacists.Citation25 The present project establishes the positive effect that pharmacist educators can have on the behavior of physician learners. Additionally, although we did not formally measure the effect of the intervention on interprofessional teamwork, informal feedback from project participants indicated improved collaboration between pharmacists and residents on the medicine services. Institutions aiming to improve physicians’ prescribing practices should consider mechanisms to incorporate pharmacists into the education of medical trainees.
Limitations
Although we have demonstrated that a QI project designed within the KT framework can succeed to improve inpatient LMWH use, our project has limitations. First, this was a single-institution study involving residents at a large academic center, which limits the generalizability to nonresident prescribers and other settings such as nonacademic hospitals. Yet, application of a similar KT approach that focuses on identifying the relevant prescribers, reasons for their prescribing habits, and whom they view as a credible source of information should be effective in other settings. Second, this was not a randomized study, which opens the possibility of confounding. However, we used segmented regression to attempt to identify any hospital-wide phenomenon that may have influenced LMWH use. Third, the intervention phase involved multiple PDSA cycles, making it difficult to know with certainty that the final pharmacist-of-resident education directly caused the observed changes in prescribing practice. However, when the sustainability phase of the intervention was temporarily interrupted because of relocation of the hospital unit, a corresponding decrease in LMWH prescriptions was observed. Use of LMWH subsequently increased when the intervention was reinstated, strongly suggesting that the educational intervention had a causal relationship with the increased LMWH use. This finding also emphasizes that continuity of the education intervention was important for achieving sustainable results. Finally, although research evidence suggests clinical benefits of LMWH over UFH, we did not measure the effect of the intervention on patient outcomes.
Conclusion
This report demonstrates that a relatively low-effort, inter-professional education intervention can produce sustainable improvement in resident physicians’ prescribing practices. This initiative also highlights the value of KT framework application to QI methods. With accurate identification of knowledge gaps and misconceptions underlying current practice, similar QI endeavors may lead to educational interventions that apply across a wide range of clinical settings and specialties. Future work is needed to clarify the effect of pharmacist-of-resident education on pharmacist–doctor teamwork and collaboration.
Acknowledgments
This study was supported in part by the Mayo Clinic Hospital Internal Medicine Small Grants Program. The funder had no involvement in study design, data acquisition, data analysis, manuscript preparation, or submission of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- BarbarSNoventaFRossettoVA risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: the Padua Prediction ScoreJ Thromb Haemost20108112450245720738765
- KahnSRLimWDunnASPrevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice GuidelinesChest20121412 Supple195Se226S22315261
- QaseemAChouRHumphreyLLVenous thromboembolism prophylaxis in hospitalized patients: a clinical practice guideline from the American College of PhysiciansAnn Intern Med2011155962563222041951
- AlikhanRCohenATHeparin for the prevention of venous thromboembolism in general medical patients (excluding stroke and myocardial infarctionCochrane Database Syst Rev20093CD003747
- LaporteSLiotierJBertolettiLIndividual patient data meta-analysis of enoxaparin vs. unfractionated heparin for venous thromboembolism prevention in medical patientsJ Thromb Haemost20119346447221232002
- FanikosJStevensLALabrecheMAdherence to pharmacological thromboprophylaxis orders in hospitalized patientsAm J Med2010123653654120569760
- LloydACAndersonPMQuinlanDJBearneAEconomic evaluation of the use of enoxaparin for thromboprophylaxis in acutely ill medical patientsJ Med Econ200141–499113
- AminANLinJLenhartGSchulmanKLClinical and economic outcomes in patients at risk of venous thromboembolism receiving appropriate enoxaparin or unfractionated heparin prophylaxisThromb Haemost2009102232132619652883
- BurleighEWangCFosterDThromboprophylaxis in medically ill patients at risk for venous thromboembolismAm J Health Syst Pharm20066320 Suppl 6S23S2917032931
- TiryakiFNutescuEAHennenfentJAAnticoagulation therapy for hospitalized patients: patterns of use, compliance with national guidelines, and performance on quality measuresAm J Health Syst Pharm201168131239124421690430
- CerveroRMGainesJKThe impact of CME on physician performance and patient health outcomes: an updated synthesis of systematic reviewsJ Contin Educ Health Prof201535213113826115113
- GrimshawJMEcclesMPLavisJNHillSJSquiresJEKnowledge translation of research findingsImplement Sci201275022651257
- LavisJNRobertsonDWoodsideJMHow can research organizations more effectively transfer research knowledge to decision makers?Milbank Q200381222124817117212841049
- BakerRCamosso-StefinovicJGilliesCTailored interventions to address determinants of practiceCochrane Database Syst Rev20154CD00547025923419
- StreiffMBLauBDHobsonDBThe Johns Hopkins Venous Thromboembolism Collaborative: multidisciplinary team approach to achieve perfect prophylaxisJ Hosp Med201611Suppl 2S8S1427925423
- JenkinsIHWhiteRHAminANReducing the incidence of hospital-associated venous thromboembolism within a network of academic hospitals: findings from five University of California medical centersJ Hosp Med201611Suppl 2S22S2827925421
- OgrincGDaviesLGoodmanDSQUIRE 2.0 (Standards for Quality Improvement Reporting Excellence): revised publication guidelines from a detailed consensus processContin Educ Nurs20154611501507
- LangleyGJMoenRNolanKMThe Improvement Guide: A Practical Approach to Enhancing Organizational PerformanceCaliforniaJossey-Bass2009
- SchulmanSKearonCSubcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and HaemostasisDefinition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patientsJ Thromb Haemost20053469269415842354
- WagnerAKSoumeraiSBZhangFRoss-DegnanDSegmented regression analysis of interrupted time series studies in medication use researchJ Clin Pharm Ther200227429930912174032
- FinnANSchrodtPWittPLA meta-analytical review of teacher credibility and its associations with teacher behaviors and student outcomesCommun Educ2009584516537
- McmullinSTHennenfentJARitchieDJA prospective, randomized trial to assess the cost impact of pharmacist-initiated interventionsArch Intern Med1999159192306230910547170
- MekonnenABMclachlanAJBrienJ-AnneeBrienJAEffectiveness of pharmacist-led medication reconciliation programmes on clinical outcomes at hospital transitions: a systematic review and meta-analysisBMJ Open201662e010003
- BéchetCPichonRGiordanABonnabryPHospital pharmacists seen through the eyes of physicians: qualitative semi-structured interviewsInt J Clin Pharm20163861483149627817170
- GallagherRMGallagherHCImproving the working relationship between doctors and pharmacists: is inter-professional education the answer?Adv Health Sci Educ Theory Pract201217224725721088991