Abstract
Background:
Research has shown that accurate and timely communication between multidisciplinary clinicians involved in the care of complex and chronic health conditions is often challenging. The domain knowledge for these conditions is heterogeneous, with poorly categorized, unstructured, and inconsistent clinical vocabulary. The potential of boundary object as a technique to bridge communication gaps is explored in this study.
Methods:
A standardized and controlled clinical vocabulary was developed as a boundary object in the domain of a complex and chronic health condition, namely, multiple chemical sensitivity, to improve communication among multidisciplinary clinicians. A convenience sample of 100 patients with a diagnosis of multiple chemical sensitivity, nine multidisciplinary clinicians involved in the care of patients with multiple chemical sensitivity, and 36 clinicians in the community participated in the study.
Results:
Eighty-two percent of the multidisciplinary and inconsistent vocabulary was standardized using the Systematized Nomenclature of Medicine – Clinical Terms (SNOMED® CT as a reference terminology. Over 80% of the multidisciplinary clinicians agreed on the overall usefulness of having a controlled vocabulary as a boundary object. Over 65% of clinicians in the community agreed on the overall usefulness of the vocabulary.
Conclusion:
The results from this study are promising and will be further evaluated in the domain of another complex chronic condition, ie, chronic pain. The study was conducted as a preliminary analysis for developing a boundary object in a heterogeneous domain of knowledge.
Introduction
There is growing evidence to demonstrate the importance of multidisciplinary care management of complex chronic conditions.Citation1–Citation6 Complex conditions considered in this research include those that do not have standardized treatment strategies or clinical practice guidelines.Citation7–Citation9 There is evidence to show that accurate and timely communication among multidisciplinary care teams is a key ingredient for delivering seamless care to patients with these health conditions.Citation10 Studies have established the consequences of poor communication among multidisciplinary care providers, resulting in poor care experiences for patients, repetitive medical tests, and medical errors.Citation11–Citation14 There are many challenges to effective communication among multiple disciplines. These include poorly categorized domain knowledge, and unstructured, multidisciplinary, and fragmented clinical documentation ().
Figure 1 Challenges in the management of complex and chronic conditions.
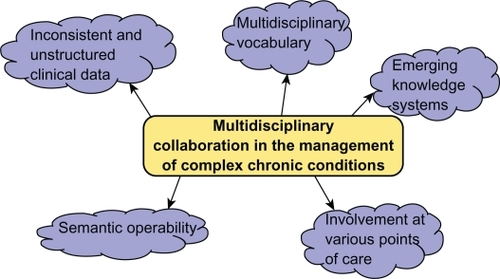
Furthermore, the domain knowledge is unstable/dynamic, with new knowledge continuing to evolve based on evidence and among domain experts. Complex health conditions can thus be viewed as heterogeneous knowledge systems. Organizing the domain knowledge, building consistency, enabling shared communication for clinicians, and semantic interoperability may be a significant challenge for these conditions. The objective of this research was to address some of these challenges and to develop a preliminary layer of consistency and standardization, with the global intent of improving collaborative work for these conditions.
Boundary objects in heterogeneous domains
Challenges related to collaborative work are poorly categorized, and unstable domains have been explored in the literature. In an observational study, Hayword and KintiCitation15,Citation16 discussed the challenges of a multidisciplinary team, working with cutting edge technology to develop a prototype for digital mammography. The authors describe the nature of the collaborative work as being characterized by high levels of uncertainty, tension, and conflict. In an extension to this work, they assessed the work of such specialized collaborations as being additionally challenging, due to the goal of activity either not being given or being poorly defined. However, they also emphasized the importance of experts continuing to work with poorly defined problems and the need for enhancing communication among experts. A study by Fong et alCitation17 in the context of designing projects for military work described the advantages of seeing a common vision in the design stages of the project to facilitate the building of the right type of knowledge. They describe the struggle of two groups that start with different visions to achieve the same goal and demonstrate how having a common vision to achieve the goal helps build the right type of bridge to close the communication gap during the design phase itself. EngeströmCitation18 stated in a study about collaborative work for communities where knowledge continues to evolve:
“There is a new generation of expertise around, not based on supreme and supposedly stable individual knowledge and ability but on the capacity of working communities to cross boundaries, negotiate and improvise ‘knots’ of collaboration in meeting constantly changing challenges and reshaping their own activities”.
In other words, experts not only have to work with changing knowledge but may have to incorporate changes in their workflow to accommodate the new knowledge.
Studies have also discussed the need to identify methods to improve communication among health care providers in order to enhance the collaborative environment.Citation19,Citation20 As stated by Hayward and Kinti,Citation15 there is a need to address communication among the care providers, who are domain experts working with constantly emerging knowledge on lesser known health conditions. There is also a need, as stated by Fong et al,Citation17 to build a common understanding at the early stages of this collaboration, so that the collective knowledge can build in a consistent and stable manner, regardless of the extent of heterogeneity that exists in the domain. However, there is a paucity of research on the exploration of methods to improve communication in poorly categorized and unstable domains.
A promising and emerging area addressing communication gaps in collaborative work is on boundary objects.Citation21 There is some predominantly theoretical research in the literature discussing the potential of boundary objects in shared work or identifying possible boundary objects in use in collaborative work.Citation22–Citation30 There is limited research in the application of boundary objects in health care,Citation31–Citation35 and fewer still for complex chronic conditions.Citation35,Citation36 PatersonCitation35 explored the use of a boundary object in the management of chronic kidney disease. This study assumed a stable domain and developed the boundary object, which was the discharge summary based on information from a single patient. Fewer studies have explored the potential of boundary objects in a heterogeneous knowledge domain. A study by Lin et alCitation36 examines the potential of developing a boundary object to improve communication among a group of mental health professionals by using an ontology approach. This study outlines the importance and the challenges of building ontologies in heterogeneous knowledge systems. The primary interaction in that study is between a domain expert and an ontology engineer. The study highlights the challenges that exist in the knowledge capture for a domain that has obscure definitions, unstructured data, inconsistent use of vocabulary and assessment scales, and emerging knowledge with time. Despite these challenges, the authors identify the need to enable the domain knowledge in a machine retrievable format to facilitate efficient information retrieval. The study identifies the importance of developing structure and consistency in such situations as a preliminary step to developing the domain ontology.
As outlined by Lin et al, in order to develop boundary objects in heterogeneous domains, it is essential to initiate a preliminary layer of organization prior to developing boundary objects. Clinical documentation is the primary method of communication and collaboration among multidisciplinary care providers. In this study, a standardized and controlled vocabulary is explored as a boundary object to develop a preliminary layer of stabilization and understanding among care providers.
Controlled vocabulary as a boundary object
Controlled vocabularies are gaining popularity as a way of enabling shared understanding of disease concepts in collaborative care management. A controlled vocabulary can be defined as “a list of terms or phrases” that is routinely used by multiple users in a domain of knowledge. Exploration of using a controlled vocabulary as a boundary object to improve collaboration in heterogeneous or emerging knowledge systems, such as for complex health conditions, is limited. Most of the research presented in the literature has developed controlled vocabularies from well-outlined and well-defined health conditions with homogeneous or stable domain knowledge.Citation37–Citation40
There is limited research on developing boundary objects for complex health conditions. In a hypothetical study by Araújo,Citation31 the potential for use of common symptom terminologies as mediating or boundary objects to integrate the work among professionals dealing with fibromyalgia and somatic functional syndromes was discussed. The authors concluded that identifying mediating objects and using them consistently can create a shared understanding in the management of conditions such as fibromyalgia.
PatersonCitation35 studied the potential value of a controlled vocabulary as a boundary object in the management of a chronic kidney condition, whereby a text corpus was created by manually and automatically retrieving commonly used terms in a patient chart. The terms and concepts were mapped to Systematized Nomenclature of Medicine – Clinical Terms (SNOMED® CT)Citation41 using a browser. The discharge summary data were standardized to unique Unified Medical Language System® identifiers. Trainees tested the vocabulary using the information for the same patient. The trainees could insert information in three ways, ie, by typing into a text box, by choosing from a menu option, or by selecting entries from a lookup file. The discharge summary was then saved in an XML (extensible markup language) format. This study did not consider unstructured data inserted by trainees. The author advocates a proposed evaluation phase of the vocabulary by nurses, physicians, and other clinicians, but the details and results of this evaluation are not available at the present time. However, an assumption of this study was that the domain knowledge is homogeneous, and a single patient chart was used to develop the controlled vocabulary.
Methodology of development of controlled vocabulary in a heterogeneous domain
Goal and purpose
Certain methodological issues in the development of controlled vocabularies raised by MaiCitation42 and Helena and ChristophCitation43 are important for heterogeneous and emerging knowledge bases. In the discussion paper by Mai,Citation42 the author outlines the importance of the goals and usage of the pragmatic approach as being the most important aspect in the creation of vocabularies to match users’ needs. This result follows from a line of thinking that argues that a controlled vocabulary “is always required for a [specific] purpose, and why a consideration of that purpose is the most important part of the methodology of information science”.Citation44
In a study by Helena and Christoph,Citation43 knowledge integration among multiple users in data warehouse projects was examined. The challenge of nonmembers of language communities and access to the boundary object was brought to the forefront. The authors suggest that alignment of the community’s terminology to the common goal is essential for the viability of the boundary object.
Edman et alCitation45 have made a theoretical proposal for the enhancement of communication between a Swedish design company and its users in the early phases of development to ensure success of implementation. They propose three main phases in their theoretical methodology, ie, mapping out existing methods, patterns, and situations used by leading practitioners, experiments in order to develop improved design methods for user involvement in service innovation, and reflections around these two phases in order to find theoretical patterns for global level inference and transference of knowledge.
Pragmatic layer of knowledge
Carlile’s rules,Citation30 followed by boundary objects, ie, syntactic, semantic, and pragmatic, are of relevance and importance in building consistency in heterogeneous systems. The following are the four rules for boundary objects proposed by Carlile:
Establishes some shared language/syntax for representing each other’s knowledge (syntactic)
Provides individuals with a concrete means of specifying their differences and dependencies (semantic)
Facilitates individuals in negotiating and transforming their knowledge in order to create new knowledge (pragmatic)
Supports an iterative approach whereby individuals get better at representing, specifying, and transforming knowledge.
From the above discussion, we propose that in developing a controlled vocabulary in a heterogeneous and emerging knowledge domain, Carlile’s rules of syntactic, semantic, and pragmatic layers should be established, and domain users should be engaged in the process of development and evaluation of the vocabulary.
The four rules described by Carlile are important in the context of meeting the needs of knowledge communities that use the boundary objects. For instance, a group of experts in the management of a certain medical condition can create a repository of terms at a syntactic level to describe the profile characteristics of patients, such as fatigue, shortness of breath on exertion, or food sensitivities facilitating shared understanding in the group. The group can also create a “shared meaning” at a semantic level for the terms, facilitating translation of the terms for multidisciplinary clinicians, such as “fatigue” meaning low energy or tiredness. In addition, the group can develop a pragmatic layer facilitating knowledge transformation in the form of boundary objects using standardized terminologies, such as SNOMED CT, that can be understood and interpreted by a larger audience. The term “fatigue” can be described with a SNOMED CT concept ID of 84229001 as an energy and stamina finding, with synonyms being tiredness and weariness. This allows different groups to share, translate, and transform knowledge at the boundary level. Carlile proposed that pragmatic boundaries can facilitate interactions among social groups that goes beyond mere translation.
User involvement
Few studies have attempted to develop boundary objects with the goal of addressing specific user needs or engaged users in a feedback process. One such study is a white paperCitation34 in which improvements in the collaborative functioning of multiple departments of a hospital was investigated through the use of a boundary object. A problem response form known as the A3 report was used to integrate the operations of various departments. The A3 report was adapted from a report created for Toyota Motor Company in the problem report and solution process among various departments so they could collectively understand how they impacted each other’s work. This study used interviews with the stakeholders to evaluate the contents of the report, created a feedback tool to evaluate the usefulness of the report, and validated it in a pilot study. Feedback was obtained from the users about the usability, knowledge integration, and communicability of the tool. The feedback showed higher scores for usability and communicability subscales versus knowledge integration. This study demonstrated the importance of user engagement and feedback during the earlier phases of implementation to promote the use of new technologies or processes that are important for collaborative work.
Methods
Objectives
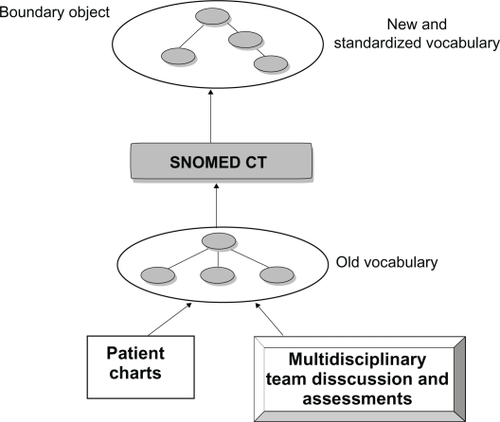
The broad objective of this research was to develop a methodology to convert an inconsistent and multidisciplinary clinical vocabulary into a standardized and controlled vocabulary that can serve as a boundary object in the collaborative care management of a complex health condition (). The more specific objective was to address the gaps in care that can occur when clinicians from various disciplines of care, such as physicians, nurses, psychologists, physiotherapists, and occupational therapists have to communicate. The clinical vocabulary was found to be inconsistent and multidisciplinary. A controlled and standardized vocabulary was explored as a mediating ground for clinicians involved in patient care. In this study, the feedback from experts in the field and other clinicians in the community who are routinely involved in the care of patients with multiple chemical sensitivity was sought to ascertain the usefulness of the vocabulary as a boundary object in collaborative work.
Figure 2 Boundary object in multidisciplinary care.

Study population
A controlled vocabulary was developed as a boundary object in the patient profile domain of a complex, chronic health condition, ie, multiple chemical sensitivity. Multiple chemical sensitivityCitation2,Citation46 is a chronic condition affecting multiple body systems, with patients experiencing symptoms in multiple areas of health focus and requiring a multidisciplinary care management approach. Many disciplines, including physicians, nurses, psychologists, and occupational therapists are typically involved in the care of patients. This health condition was selected because it fulfills the criteria for a heterogeneous domain with a poorly categorized and unstable domain of knowledge. A pragmatic approach was adopted in the development of the controlled vocabulary.Citation30 The design of the controlled vocabulary is in keeping with the users’ activities, needs, and demands.Citation42 SNOMED CT was selected as the reference terminology for standardization of concepts in the controlled vocabulary due to the availability of extensive concepts as described in the literature,Citation47–Citation53 excellent coverage of complex clinical concepts for many health conditions, and the indication of preference over other terminologies in the literature.
Study design
The methodology for the study included the following key phases: identification of the knowledge that exists in the domain by a retrospective chart audit process; standardization of vocabulary identified in the domain; user feedback on the chart audit and standardized terms; and, finally, user evaluation of the standardized and controlled vocabulary.
A convenience sample of patients and clinicians participated in the study. The study received ethical approval from the Health Authority Ethics Board. The study methodology comprised of retrieving the essential terminologies through a chart audit process and standardization using SNOMED CT. The multidisciplinary clinicians (domain experts) were involved from the initial phase of development in reviewing the chart audit terms and the standardized terms for accuracy and completeness. The domain experts and clinicians in the community (experts and nonexperts) reviewed the usefulness of the controlled vocabulary for the improvement of the collaborative care environment by facilitating a better understanding of the language and of the health condition. shows an expanded view of the schematic of methodology used in the creation of the controlled vocabulary.
Figure 3 Schematic of the methodology for the creation of the boundary object.
The development of the controlled vocabulary included the following phases: a retrospective audit of patient charts, interviews with experts, standardization of vocabulary, testing, and evaluation of the vocabulary by users and end users, as shown in .
Syntactic layer: retrieving terminologies in use by retrospective chart audit
A sample size of 100 patient charts was selected to account for the heterogeneity in the knowledge base. One hundred patients with a diagnosis of multiple chemical sensitivity were approached for participation. Patient charts were audited to create a text corpus of commonly occurring clinical terminologies and themes used by the multidisciplinary team of clinicians in describing the profile of a patient. The key intake documents in the patient charts used by the multidisciplinary clinicians were reviewed in the categorization of patient profiles. A database of commonly occurring terminologies was created. The frequency of occurrence of a term in the 100 patient charts was compiled in the form of a percentage and its importance in patient profile categorization was determined. The terminologies were grouped by areas of health focus, medical, psychosocial, physical, rehabilitation, and nutrition.
Semantic layer of knowledge: standardizing terminologies using SNOMED CT
SNOMED CT was used as the reference terminology to standardize the chart audit terms. A manual mapping process was used in this study in which each source term (chart audit term) was searched using a SNOMED CT browser, ie, CLINICLUE.Citation54 The terms were grouped under exact match, synonyms, or no match terms.
The multidisciplinary clinicians involved in the management of multiple chemical sensitivity participated in reviewing the concepts retrieved in the patient profile domain during the chart audit process and following the standardization of the chart audit terms. Involvement of the clinicians was important to ascertain the accuracy and relevancy of concepts found in the domain of multiple chemical sensitivity.
Pragmatic layer of knowledge: usability of vocabulary in clinical care
The controlled vocabulary was used by the multidisciplinary clinicians to recode three patient profiles. A representative sample of charts that was a prototypical representation of the patient population was selected by a key member (a physician) of the multidisciplinary care team. The three patient charts were different from the 100 patient charts used to develop the controlled vocabulary.
The clinicians were randomly assigned to coding Group A and coding Group B. Each coding group comprised a physician, nurse, physiotherapist, rehabilitation coordinator, dietician, and psychologist (or psychotherapist). The clinicians used information from the patient charts in the recoding process.
A web-based form containing the terminologies from the controlled vocabulary was created to help the clinicians recode the patient profiles. Each terminology in the web-based form had a link to the hierarchical classification of the term as it exists in SNOMED CT. This provided an opportunity for the clinician to view the parent concepts, the concept ID, and synonyms for the clinical terminology in order to determine the accuracy of the concepts in SNOMED CT to represent the intended clinical concepts of the source terms correctly. Through the recoding process, the clinicians had an additional opportunity to explore the accuracy of terms in the controlled vocabulary. Cohen’s kappa was used to analyze the interrater reliability of the coding disciplines, with the same area of health focus, such as a psychologist and psychotherapist, for the area of psychosocial factors. The kappa score was used to determine reliability in the number of terms identified as missing terms in the new vocabulary.
Evaluation of controlled vocabulary
Clinicians (multidisciplinary clinicians and clinicians in the community) then provided feedback on the usefulness of the controlled vocabulary in building a common platform for communication. The evaluation format proposed by ToewsCitation55 was used to determine the usefulness of the controlled vocabulary by users and end users of the vocabulary. An evaluation questionnaire on a five-point Likert scale validated in another study,Citation55 with questions about the scope, specificity, structure, and usability of the clinical vocabulary, was used to obtain feedback. The evaluation was conducted under the categories provided below.
Scope
Is the vocabulary capable of representing all of the concepts found in the complete patient record? Does the vocabulary have the terms necessary to represent the full range of health? Does the vocabulary encompass the terminology used to describe the procedures performed by care providers? Does the vocabulary use terms that are commonly used by care providers?
Specificity
Is the vocabulary specific enough to represent accurately the many aspects of health care reality? Is there minimal loss of clinical detail when data are encoded in the vocabulary?
Structure
Are the vocabulary hierarchies logical and complete? Does the vocabulary contain redundant terms?
Usability
Does the vocabulary meet the needs of a range of end users?
Each response category was assigned a numeric value. The greatest negative response (strongly disagree) was scored as “1” and the highest positive response (strongly agree) was scored as “5”. Responses to each item were analyzed as the percentage of reviewers who agreed/disagreed (strongly or not). The reliability (internal consistency) of the questionnaire was determined using Cronbach’s alpha,Citation56 which is a widely accepted reliability measure of internal consistency in survey research.
Evaluation by multidisciplinary clinicians
Clinicians involved in using the controlled vocabulary in the recoding process offered their feedback on the usefulness of the new vocabulary.
Evaluation of controlled vocabulary by clinicians in the community
Clinicians in the community, such as general physicians and other care providers, who may have to treat patients with these conditions, were approached to obtain their feedback on the usefulness of the patient profiles generated using the controlled vocabulary. A convenience sample of clinicians from the community was recruited through an email invitation to participate that was sent to the department heads and managers. The information package sent to participants included an overview of the study, the consent form, the three patient profiles in the old and new vocabularies, and the survey questionnaire. Usefulness was evaluated on the basis of the scope, specificity, structure, and usefulness of standardization on a five-point Likert scale.
Statistical analysis
The reliability (internal consistency) of the questionnaire was determined using Cronbach’s alpha.Citation56 Cohen’s KappaCitation57 was calculated to assess agreement between the various disciplines. Kendall’s TauCitation58 was calculated to determine agreement among multiple raters.
Results
Syntactic layer of knowledge
A total of 100 patient charts were audited to retrieve key concepts and terminologies relevant to the patient profile categorization of multiple chemical sensitivity, as shown in . Five hundred and twelve concepts/terminologies in use were retrieved in the multidisciplinary areas of health focus, including physical, psychosocial, nutrition, rehabilitation, and medical. In the top one-third consortium, symptoms in the various body systems included blood and gland symptoms (fatigue), nervous system symptoms (such as light-headedness, cold fingertips, cold extremities and irritability), eye symptoms (eye irritation, itchy eyes), and nasal symptoms (sinus congestion). Along with symptoms in the body systems, such as pain (multiple body systems), nonrestorative sleep (nervous system), poor memory (nervous system), and food sensitivity and bloating (stomach and bowel), there is a manifestation of other determinants of health such as psychosocial factors (nonassertiveness, self-criticism, and overly accommodative) that add to the patient profile. In the middle-third grouping, there is further evidence of the influence of multidimensional health factors in the patient profile characteristics for multiple chemical sensitivity. There are additional manifestations of stomach and bowel symptoms (reflux, diarrhea, abdominal cramps), nervous system symptoms such as depressed mood; rehabilitation elements such as the “not working” status, work-related onset of illness, and characteristics of home environment; sign of diminished physical capacity, such as a low step count (measured using a pedometer over a two-week period) and more psychosocial characteristics, such as withdrawal, stifled emotions, and somatization. Psychosocial characteristics that have an impact also include childhood abuse, seen in 47% of the study sample. Poor balance and chest pain add to other clinical features of this illness. Psychosocial characteristics, such as emotional eating along with other nutritional symptoms, such as nausea, are prevalent in the bottom-third grouping.
Table 1 Concepts retrieved from the chart audit process
Semantic layer of knowledge
Four hundred and twenty-two (82%) of these concepts were available in SNOMED CT.
shows examples of inconsistent concepts retrieved from various areas of health focus and standardized using SNOMED CT. The number of concepts in each field were 356 (medical), 136 (physical), 122 (psychosocial), 118 (rehabilitation), and 80 (nutrition). shows an expanded view of the controlled vocabulary under the nutrition area of health focus. The top level concepts that occur in the nutrition profile are shown in this view.
Figure 4 Sample view of the controlled vocabulary - nutrition profile.
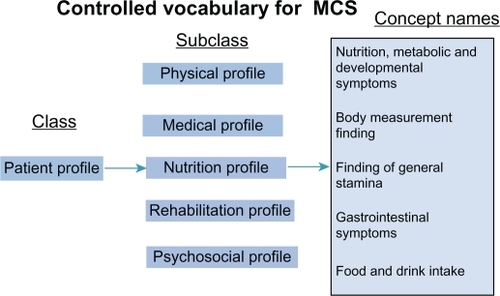
Table 2 Standardization of multidisciplinary clinical vocabulary (semantic) using SNOMED CT
Pragmatic layer of knowledge
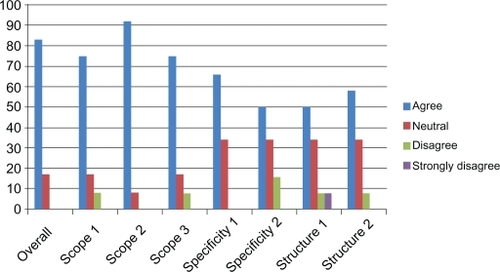
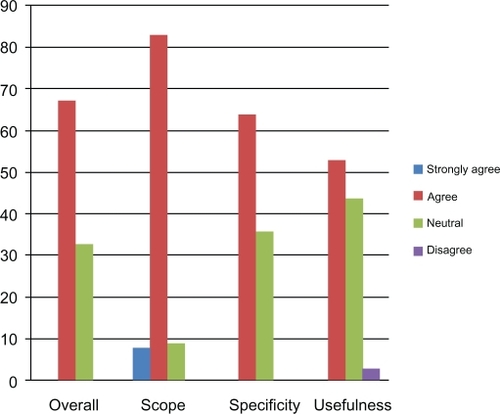
Ten of the twelve clinicians participating in the recoding process completed their evaluation of the vocabulary using a five-point Likert scale that measured the usefulness of the vocabulary under an overall category and under subcategories of scope, specificity, and structure.
Eighty percent of the multidisciplinary clinicians (experts in the domain) agreed on the overall usefulness of the controlled vocabulary (). The subcategories also had an overall high level of agreement, with the question on the use of terms familiar to the clinicians under the scope category getting the maximum level of agreement from the clinicians (90%). Questions under structure and specificity brought a level of disagreement from a small percentage of the clinicians. Cronbach’s alpha analysis was conducted to determine the internal reliability of the survey questionnaire. A moderate level of agreement was obtained with an alpha score of 0.61 (score interpretation).
Figure 5 Response to the survey questionnaire in the multidisciplinary group of clinicians (%).
Evaluation of boundary object by expert and nonexpert community-based clinicians
Thirty-six clinicians from various disciplines in health care participated in the study, comprising six physicians, six psychologists, six physiotherapists, six dietitians, and six occupational therapists. They reviewed the patient charts in the old vocabulary and the new vocabulary. An overall agreement on the usefulness of the vocabulary was reached among the experts in most categories ().
Figure 6 Response to the survey questionnaire from clinicians in the community (%).
Internal validity of the questionnaire was tested using Cronbach’s alpha analysis, and this demonstrated a good level of validity, with a value of 0.73 for the 36 raters. The mean value for the various disciplines had a better level of validity, with Cronbach’s alpha being 0.89 ().
Table 3 Cronbach’s alpha by the discipline of care
Kendall’s tau was calculated at 0.5, with a moderate level of concordance among the 36 (multiple) raters with a P-value of 0.04. Cohen’s kappa for the dieticians showed the highest level of agreement, with a score of 0.84. Cohen’s kappa for agreement across disciplines showed low agreement between physicians and dieticians (0.2) and a moderate level of agreement between physicians and physiotherapists (0.5). Qualitative feedback was obtained from the clinicians in the community through open-ended questions. Presented in are some comments that were presented by clinicians from various health disciplines. The emerging themes show that clinicians are receptive of this move towards bringing consistency and standardization to the clinical vocabulary to build a better understanding of complex health conditions.
Table 4 Feedback from clinicians in the community
Discussion
In this study, a boundary object in the form of a controlled vocabulary was developed, tested, and evaluated in a heterogeneous knowledge domain. Research on boundary objects to date has predominantly focused on theoretical concepts.Citation22–Citation30 There is limited exploration of the potential of boundary objects in health care.Citation31–Citation36 Furthermore, the challenges of developing boundary objects in heterogeneous knowledge systems are well recognized.Citation36
The methodology in the study adapted steps outlined in the combined works of Helena and Christoph,Citation43 Mai,Citation42 and EdmanCitation45 related to emerging and heterogenous knowledge systems. The premise of the assumption included complex and chronic conditions being unstable/dynamic and with poorly categorized knowledge systems. The study used approaches that allowed exploration of heterogeneity of the knowledge (retrospective audit of 100 patient charts and feedback of clinicians) in the design and involvement of clinicians in the exploration of concepts in SNOMED CT, leading to standardization of concepts. This was done to ensure user interest in the subsequent use of the new technology.Citation34,Citation59,Citation60 The study involved testing of the usefulness of the vocabulary in a clinical setting in the form of recoding of patient profiles. This step is often a limitation in the studies to date where proposed advances in health care were not tested in the clinical process, leading to a general level of discontent among clinicians.Citation61–Citation63 The study further included the feedback of clinicians involved in the patient’s care (domain experts) on the usefulness of creating boundary objects.Citation55 Furthermore, the usefulness of the boundary object in enhancing understanding of the domain knowledge among nonexperts was explored by obtaining feedback from clinicians in the community.
The controlled vocabulary was created using SNOMED CT as the reference terminology. SNOMED CT was shown to capture 82% of the concepts necessary to categorize the patient profile in the domain of a complex health condition. The excellent availability of concepts is similar to those found in other studies.Citation47–Citation52 The scope and extent of coverage of the terms in SNOMED CT for multiple chemical sensitivity is of importance, given that the nature of the profile characteristics for complex conditions, such as multiple chemical sensitivity, go beyond the conventional problem list that is well recognized in the medical field.Citation60 The clinical vocabulary includes multifaceted characteristics under physical, psychosocial, rehabilitation, and nutrition areas of health focus. This study has shown that there can be a reasonable expectation for standardizing multidisciplinary vocabulary for other complex conditions through the review of one complex health condition, ie, multiple chemical sensitivity. However, there were terms and concepts of direct relevance and importance to multiple chemical sensitivity that could not be found in SNOMED CT. The term “multiple chemical sensitivity” itself is not available in SNOMED CT. Other terms of relevance to the condition not available in SNOMED CT included “heightened reactivity to the environment”, “increasing sensitivity to chemicals”, symptoms related to exposures, such as “shortness of breath with exposure”, “dizziness with exposure”, “metallic taste in mouth with exposure”, and other terms related to cognitive abilities, such as brain fog and trouble finding the right words. PostcoordinationCitation64 was applied to such terms in an attempt to improve coverage for this condition. For forty-five (75%) of the terms with direct relevance to multiple chemical sensitivity, postcoordination was possible with some level of complexity, and a few attribute value pairs were required for the process. However, these terms were not reviewed by the experts for accuracy and completeness in this study.
The boundary object developed in this study has the potential not only to allow knowledge sharing but also to enable knowledge expansion. Using a well recognized terminology, such as SNOMED CT, allows multiple expert groups in the domain to build knowledge together in a consistent manner.Citation25 The usage of this terminology has grown to a great extent in recent years as a reference terminology to represent many disease concepts and is well accepted in the medical community. Using this terminology in lesser known conditions will ensure that a clinician from any discipline of care, whether expert or nonexpert in the domain of the complex chronic condition, can explore the syntactic and semantic aspects of a specific terminology used to categorize the patient. This boundary object thus has the potential to grow as clinicians in the community or specialized groups use the information in the shared knowledge space and contribute their own knowledge to the shared space. This can be viewed as a dynamic boundary object.Citation27
Limitations and future work
While the study was overall successful in exploring the potential for creating controlled vocabulary as a boundary object for a complex health condition, the study used a convenience sample approach. Knowledge about multiple chemical sensitivity was explored from the perspective of one expert group. There is a possibility that other expert groups may have additional terms, which may lower the expectation for finding multidisciplinary terms in SNOMED CT. The postcoordination terms developed in the study were not reviewed by the experts for accuracy and completeness. This can be viewed as another important step in the methodology for developing standardization for complex conditions by improving coverage of terms and concepts that are relevant and important to these conditions in SNOMED CT.
While the controlled vocabulary received an overall level of agreement from the clinicians, it is not known whether using the vocabulary will in fact improve communication or enhance patient care. However, it must be stated that this study conducted an evaluation of the boundary object through clinicians using it to recode patient profiles. The methodology will be validated by developing a controlled vocabulary as a boundary object for chronic pain.
Disclosure
The authors report no conflicts of interest in this work.
References
- KuzmaAMMeliYMeldrumCMultidisciplinary care of the patient with chronic obstructive pulmonary diseaseProc Am Thorac Soc2008556757118453373
- Removed for review process.
- ClarkTInterdisciplinary treatment for chronic pain: Is it worth the money?Proc (Bayl Univ Med Cent)20001324024316389389
- KolstandHASilberschmidtMNielsenJBMultiple chemical sensitivity, a well-defined illness?Ugeskr Laeger20061681116111916545215
- DysvikENatvigGKEikelandOJBrattbergGResults of a multidisciplinary pain management program: A 6- and 12-month follow-up studyRehabil Nurs20053019820616175925
- DobschaSCorsonKPerrinNACollaborative care for chronic pain in primary careJAMA20093011242125219318652
- RichardsonREngelCEvaluation and management of medically unexplained physical symptomsNeurologist200461183014720312
- HenningsenPZimmermanTSattelHMedically unexplained physical symptoms, anxiety, and depression; A meta-analytic reviewPsychosom Med20036552853312883101
- VerhaakPFMeijerSAVisserAPWoltersGPersistent presentation of medically unexplained symptoms in general practiceFam Pract20062341442016632487
- MarchibrodaJMThe impact of health information technology on collaborative chronic care managementJ Manag Care Pharm2008142 SupplS3S1118331114
- SchoenCOsbornRHowSKHDotyMMPeughJChronic conditions: Experiences of patients with complex health care needs, in eight countries, 2008Health Aff (Millwood)2008271235124518780906
- KennedyClinical documentation improvement in MS-DRGs as a strategy for compliance: Facilities may consider clinical documentation audits to look for coding errorsJ Healthcare Compliance2008
- PaceWDDickinsonLMStatonEWSeasonal variation in diagnoses and visits to family physiciansAnn Fam Med2004241141715506572
- StangeKCNuttingPABursting the bubble on chronic disease management, the meaning of healingAnn Fam Med20053194196
- HaywardGKintiIConflicting values in collaborative organisingPresented at: The Seventh International Conference on Social ValuesOxford UKJuly 14–15, 2004
- KintiILloydSSimpsonACHaywardGManaging collaborative expertise: Issues and challengesProceedings of the Sixth European Organizational Knowledge and Learning ConferenceMarch 17–19, 2005Boston, MA
- FongAValerdiRSrinivasanSBoundary objects as a framework to understand the role of systems integratorsPresented at the Fifth Annual Conference on Systems Engineering ResearchHoboken, NJMarch 14–16, 2007
- EngeströmYThe new generation of expertise: Seven thesesRainbirdHFullerAMunroAWorkplace Learning in ContextLondon, UKRoutledge2004
- RuhstallerTRoeHThurlimannBThe multidisciplinary meeting: An indispensable aid to communication between different specialtiesEur J Cancer2006422459246216934974
- BrooksPThe impact of chronic illness: Partnerships with other health-care professionalsMed J Aust200317926026212924975
- StarSLGriesemerJRInstitutional ecology, translations and boundary objects: Amateurs and professionals in Berkeley’s Museum of Vertebrate Zoology 1907–1939Soc Stud Sci198919387420
- BechkyBASharing meaning across occupational communities: The transformation of understanding on a production floorOrgan Sci200314312330
- YakuraEKCharting time: Timeliness as temporal boundary objectsAcad Manage J200245956970
- EdmanKWDesign method for design service innovation. Engaging Artifacts, 2009 Available at: http://www.hgu.gu.se/Files/gothenburg_research_institute/business/2009_Wetter_Nordes.pdf. Accessed February 16, 2011.
- FongAValerdiRSrinivasanSBoundary objects as a framework to understand the role of systems integratorsPresented at the Fifth Annual Conference on Systems Engineering ResearchHoboken, NJMarch 14–16, 2007
- ForguesDKoskelaLLejeuneAInformation technology as boundary object for transformational learning, ITcon Vol 14, Special Issue Technology Strategies for Collaborative Working; 2009
- GalUYooYBolandRThe dynamics of boundary objects, social infrastructures and social identitiesSprouts: Working Papers on Information SystemsCleveland, OHCase Western Reserve University2004
- HendersonKFlexible sketches and inflexible databases: Visual communication, conscription devices, and boundary object in design engineeringSci Technol Hum Values199116448473
- HendersonKThe role of material objects in the design process: A comparison of two design cultures and how they contend with automationSci Technol Hum Values199823139174
- CarlilePRA pragmatic view of knowledge and boundaries: Boundary objects in new product developmentOrgan Sci200213442455
- AraújoRejaneFibromyalgy: Construction and reality in medical formationRev Bras Reumatol2006465660 Spanish.
- BergMBowkerGThe multiple bodies of the medical record: Toward a sociology of an artefactSociol Q199738513537
- PatelVIBranchTArochaJFErrors in interpreting quantities as procedures: The case of pharmaceutical labelsInt J Med Inform20026519321112414018
- White Paper 2006. Test of a boundary object for process improvement.
- PatersonGIBoundary Infostructures for Chronic Diseases: Constructing Infostructures to Bridge Communities of PracticeSaarbrücken, GermanyVDM Verlag2008
- LinYPoschenMProcterROntology as a social-technical process: A case studyPresented at: the Oxford eResearch Conference 2008Oxford, UKSeptember 11–13, 2008
- RosenfeldLMorvillePInformation Architecture for the World Wide Web3rd edCambridge, UKO’Reilly2007
- LancasterFWVocabulary Control for Information Retrieval2nd edArlington, VAInformation Resources Press1986
- American National Standards Committee, National Information Standards OrganizationGuidelines for the construction, format, and management of monolingual controlled vocabularies. Z39.19–2005Bethesda, MANational Information Standards Organization Press2005
- CiminoJJHripcsakGJohnsonSBClaytonPDDesigning an introspective multipurpose medical vocabularyProceedings of the Thirteenth Annual Symposium on Computer Applications in Medical CareWashington, DCIEEE Press1989
- College of American PathologistsSNOMED CT® clinical terms technical reference guideNorthfield, ILCollege of American Pathologists2005
- MaiJEActors, domains, and constraints in the design and construction of controlled vocabulariesKnowledge Organization2008351621
- HelenaVChristophRThe role of boundary objects and boundary spanning in data warehousingPresented at the 17th European Conference on Information SystemsVerona, ItalyJune 8–10, 2009
- HjørlandBPedersenKNA substantive theory of classification for information retrievalJ Doc200561582597
- EdmanKWDesign method for design service innovation. Engaging Artifacts, The Oslo School of Architecture and Design, Norway August 30–September 1, 2009. Available at: http://www.hgu.gu.se/Files/gothenburg_research_institute/business/2009_Wetter_Nordes.pdf. Accessed February 16, 2011.
- Multiple chemical sensitivity: A 1999 consensusArch Environ Health19995414714910444033
- OsornioALLunaDGambarteMLGomezAReynosoGde QuirósFGCreation of a local interface terminology to SNOMED CTStud Health Technol Inform2007129Pt 176576917911820
- StenzhornHPachecoEJNohamaPSchulzSAutomatic mapping of clinical documentation to SNOMED CT. Medical Informatics in a United and Healthy EuropeStud Health Technol Inform200922823219745302
- JamesAGSpackmanKARepresentation of the disorders of the newborn infant by SNOMED CTStud Health Technol Inform200813683383818487835
- RichessonRLAndrewJEJeffreyPKUse of SNOMED CT® to represent clinical research data: A semantic characterization of data items on case report forms in vasculitis researchJ Am Med Inform Assoc20061353654616799121
- AsbehNPelegMSchertzMKuflikTCreating consistent diagnoses list for developmental disorders using UMLSLect Notes Comput Sci20064032333336
- ElevitchFRSNOMED CT: Electronic health record enhances anesthesia patient safetyAANA J20057336136616261852
- ElkinPBrownSHusserCAn evaluation of the content coverage of SNOMED-CT for clinical problem listsMayo Clin Proc20068174174816770974
- CliniClue 2006. Clinical terminology services from the clinical information consultancy. Available at: www.cliniclue.com. Accessed November 6, 2006.
- ToewsLAn evaluation methodology for clinical vocabularies and evaluation of the read codes. Health Sciences Library Available at: http://www.ualberta.ca/dept/slis/cais/toews.htm. Accessed February 16, 2011.
- CronbachLJShavelsonRJMy current thoughts on coefficient alpha and successor proceduresEduc Psychol Meas200464391418
- CohenJWeighed kappa: Nominal scale agreement with provision for scaled disagreement or partial creditPsychol Bull19687021322019673146
- KendallMGRank Correlation Methods4th edLondon, UKCharles Griffin and Co1970
- WalshSThe clinician’s perspectives on electronic health records and how they can affect patient careBMJ20043281184118715142929
- HamCLearning from Kaiser Permanente: A Progress Report Unpublished paperLondon, UKDepartment of Health2003
- TsasisPBainsJManagement of complex chronic disease: facing the challenges in the Canadian health-care systemHealth Serv Manage Res20082122823518957400
- WalshSHThe clinician’s perspective on electronic health records and how they can affect patient careBMJ20043281184118715142929
- BlaserRSchnabelMHegerOImproving pathway compliance and clinician performance by using information technologyProceedings of MIE2005116199204
- RichessonRLAndrewJEJeffreyPKUse of SNOMED CT® to represent clinical research data: A semantic characterization of data items on case report forms in vasculitis researchJ Am Med Inform Assoc20061353654616799121