
Abstract
Purpose
The aim of this observational cross-sectional study was to determine if allied health professionals working in a large metropolitan health district were meeting the minimal physical activity (PA) recommendations and the proportion that occupational PA contributed to the recommended PA levels. A secondary aim was to determine possible relationships between self-report questionnaire measures of PA and PA measured by accelerometry.
Materials and methods
Allied health professionals, working in the Sydney Local Health District (SLHD) in 2016–2017, completed the Active Australia Survey (AAS), Occupational Sitting and Physical Activity Questionnaire (OSPAQ), International Physical Activity Questionnaire Long form (IPAQ-L), and wore the ActiGraph GT1M accelerometer for 7 days consecutively.
Results
Based on accelerometry results, allied health professionals (N=126) spent a mean (SD) of 51 (23) minutes in moderate-to-vigorous physical activity (MVPA)/day, representing 171% of the total recommended MVPA/day, with work contributing 76% to this recommendation. Participants walked a mean of 10,077 (2,766) steps/day, meeting 100% of the recommended 10,000 steps/day, with work contributing 54% to this recommendation. Sedentary behaviors were predominant throughout the entire day and work day. Compared with the ActiGraph MVPA time measurements, AAS MVPA time showed a fair level of agreement [intraclass correlation coefficient (ICC)=0.44, P<0.01], while OSPAQ and IPAQ-L MVPA time showed no agreement (ICC=0.05, P=0.27; ICC=0.13, P=0.10, respectively).
Conclusion
Allied health professionals working in a large metropolitan health district met the daily PA recommendations based on accelerometry measures but tended to overreport their MVPA on self-report questionnaires.
Introduction
Physical inactivity refers to a lack of moderate-to-vigorous physical activity (MVPA) with decreased time spent in activities involving energy expenditure of at least three metabolic equivalent tasks (METs) throughout the week.Citation1 Physical inactivity can occur as a result of a multitude of factors and has been correlated to individual (eg, age, sex, health status, self-efficacy, occupation), physical (eg, accessibility and availability of exercise facilities and equipment, seasonality), and social environmental factors (eg, urban planning, transportation systems, parks, and trails).Citation2,Citation3 Levels of physical inactivity are increasing in many countries, and this has been linked to increases in morbidity and mortality,Citation2 with major implications for the general health of populations worldwide.Citation1,Citation4–Citation6 Participation in sufficient physical activity (PA) levels throughout the day is associated with significant health benefits,Citation1 such as decreased risk of diabetes mellitus, cardiovascular disease, certain types of cancers, depression, and all-cause mortality,Citation7–Citation11 with an overall decrease in health system utilization.Citation12 PA throughout the day is accumulated through leisure time activities, transportation, domestic tasks, and occupational activities.Citation1,Citation13
To achieve the health benefits of PA, it is recommended that individuals engage in 150 minutes of moderate intensity aerobic exercise and at least 75 minutes of vigorous intensity aerobic PA (or an equivalent combination of moderate and vigorous intensity PA) each week.Citation1,Citation14 Participation in MVPA demonstrates a dose–response relationship with cardiorespiratory health (with associated risk reductions in coronary heart disease, cardiovascular disease, stroke, and hypertension),Citation1 with additional health benefits observed with up to 300 minutes of moderate-intensity PA/week.Citation15,Citation16 Therefore, it has been suggested that individuals aged 18–64 years perform at least 30 minutes of MVPA on most days of the week.Citation1,Citation14,Citation17,Citation18 The number of steps/day representative of the minimal requirement of 30 minutes of MVPA/day in healthy adults (aged 18–64 years) is 7,100–11,000 steps,Citation18,Citation19 and it is widely accepted that 10,000 steps/day is a reasonable and achievable target.Citation17,Citation18 PA levels have also been monitored using self-report questionnaires in population-based studies with varying levels of test–retest reliability and validity.Citation20,Citation21
Technological advancements and modern lifestyles (including occupational, domestic, and screen-based leisure activities) have led to increases in sedentary behaviorsCitation22–Citation28 and physical inactivity,Citation11,Citation29 which have been linked to the development of chronic disease.Citation30–Citation38 Sedentary behaviors within the workplace (eg, sitting, screen-based activities) with energy expenditure 1.0–1.5 METsCitation39,Citation40 contribute to overall physical inactivity.Citation41–Citation43 Studies have demonstrated that individuals with less PA at work are also likely to demonstrate less leisure time PA.Citation44,Citation45
Occupations in health care may be more active and health care professionals may have greater levels of health literacy, education, and clinical expertise, which may facilitate healthy lifestyle behaviors such as maintaining higher levels of daily PA.Citation46,Citation47 Although some studies have investigated PA levels in health professionals,Citation48–Citation52 few studies have investigated occupational PA levelsCitation53,Citation54 and its contribution to recommended PA levels. A study investigating occupational PA levels across various occupational sectors using accelerometry classified health sector occupations as being associated with intermediate levels of occupational PA according to the proportion of total PA spent in MVPA.Citation54 In addition, a Dutch study investigating the contribution of occupational PA levels to overall total PA levels across occupational sectors reported that occupational PA in health care sector occupations contributed ~30% to the overall total PA.Citation53 Therefore, work-related PA may be an important contributor to overall total PA levels in the health sector.Citation54 Furthermore, no studies have specifically investigated the PA levels of the allied health workforce.
The primary aim of this study was to determine if allied health professionals working in a large health district were meeting the recommended daily PA guidelines and the proportion that occupational PA contributed to this recommendation. The secondary aim of the study was to determine if there was any relationship between subjective self-report levels of PA via questionnaires and objective accelerometer measures of PA in allied health professionals.
Materials and methods
This study was a prospective observational study with cross-sectional design and was registered with the Australian and New Zealand Clinical Trials Registry (ACTRN12616000514404).
Sample
Participants were recruited from allied health professionals working in the Sydney Local Health District (SLHD). Allied health disciplines included in the study were physiotherapy, occupational therapy, psychology, nutrition and dietetics, speech pathology, pharmacy, podiatry, radiography, and social work. Allied health employees, deemed fit for work, aged 20–70 years and working in inpatient, outpatient, or community health services were invited to participate in this study. A minimum sample size of 112 participants was sufficient to demonstrate a ±1,000 step difference from the recommended 10,000 steps/day for daily PA, with P<0.05 and power of 0.80 (continuous outcome noninferiority trial).Citation55
Procedures
The study was conducted in the SLHD between April 2016 and December 2017. Staff were invited to participate via the distribution of a flyer and departmental e-mail, which provided basic information regarding the study procedures. Participation in the study was voluntary, and written informed consent was obtained from all participants. At initial assessment, demographic information, employment status, and position details were collected. Participants were asked to complete three validated questionnaires: the Active Australia Survey (AAS),Citation20,Citation56 the Occupational Sitting and Physical Activity Questionnaire (OSPAQ),Citation57–Citation59 and the long form version of the International Physical Activity Questionnaire (IPAQ-L).Citation60–Citation62
Participants wore a PA monitor (ActiGraph GT1M uni-axial accelerometer, Pensacola, Florida, USA) for 7 days consecutively. The ActiGraph GT1M detects human movement in the range of 0.05–2 gravity force with the signal filtered at a bandwidth of 0.25–2.5 HertzCitation63 and has good test–retest reliability and validity.Citation64–Citation66 Participants wore the activity monitor in the midaxillary line on their right hip via an elasticized band during waking hours and removed the monitor during bathing/showering or swimming activities. Participants were asked to continue their normal leisure and workplace activities during the data collection period. Activity counts were recorded in 1-minute epochs, which were used to calculate the relative intensity of PA performed. Adult Freedson cut points were utilized to describe the relative intensity of PA.Citation67,Citation68 For the activity data to be included in the analyses, participants had to wear the ActiGraph for a minimum of 10 hours a day (as representative of a full day’s wear) with a minimum of 4 days total wear.Citation69–Citation71 ActiLife version 6.10.4 software was used to download data and manage raw output data from the ActiGraph GT1M devices. Participants also kept a log of days and times worked during the 7-day data collection period. Participants were asked to rate the tolerability of wearing the ActiGraph device as intolerable, somewhat tolerable, neutral, tolerable, or very tolerable. Study data were collected and managed using Research Electronic Data Capture (REDCap).Citation72
Statistical analyses
Quantitative data were analyzed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corporation, Armonk, NY, USA). Normally distributed data were summarized as means and SDs, and data that were not normally distributed were summarized as medians and IQRs.
Absolute agreement between subjective questionnaire self-report measures and corresponding objective Acti-Graph measures of time spent in various categories of PA were assessed using intraclass correlation coefficients (ICC) using a two-way mixed model with absolute agreement. Subjective items within the individual questionnaires for corresponding MET levels were compared with similar ActiGraph measures of PA. Repeatability and the level of agreement were interpreted as follows: poor (<0.40), fair to good (0.40–0.75), and excellent (>0.75).Citation73 Bland–Altman plots were used to determine the level of difference between subjective questionnaire self-report and objective ActiGraph measures. Specifically, questionnaire items reflecting time spent in MVPA for the AAS, OSPAQ, and IPAQ-L were summed within each questionnaire with a daily MVPA time calculated which was compared with the ActiGraph MVPA minutes/day. Questionnaires with items reflecting time spent in work MVPA (ie, OSPAQ and IPAQ-L) were treated similarly with the calculated daily work MVPA time compared with the ActiGraph MVPA minutes/day during work hours.
Differences between key variables were analyzed via dependent samples t-tests or Wilcoxon signed rank tests and correlations were examined using Pearson’s correlations or Spearman’s rho correlations. The strength of correlation effect size was interpreted as small (0.10–0.29), medium (0.30–0.49), and large (≥0.50).Citation74 The level of statistical significance was set at P<0.05.
Ethics statement
Ethics approval was obtained from the Human Research Ethics Committee of the Sydney Local Health District (SLHD) (Protocol Number X15-0435 and HREC/15/RPAH/580). This study was conducted in accordance with the Declaration of Helsinki.
Results
Demographics and ActiGraph wear
Of the 514 allied health professionals informed about the study, 126 agreed to participate in this study. The participant demographic data are presented in . ActiGraph tolerability of wear was rated as greater than or equal to tolerable by 86% (n=108) with 12% (n=15) neutral and 2% (n=3) providing no response. The mean (SD) overall number of days the ActiGraph was worn for >10 hours wear each day was 6.5 (0.8) days. Participants wore the ActiGraph for a mean of 4.2 (1.0) work days and worked a mean of 35.8 (9.0) hours/week.
Table 1 Allied health participants’ demographic data (N=126)
ActiGraph accelerometer measures of PA levels
ActiGraph PA data for the participants’ entire day and during work hours are presented in . In addition, 82% (n=103) of allied health participants met the minimum PA MVPA guidelines of ≥30 minutes/day.Citation1,Citation14 Within our sample, 46% (n=57) walked greater than the recommended 10,000 steps/day,Citation18 30% (n=38) walked between 8,000 and 10,000 steps/day, and 25% (n=31) walked <8,000 steps/day.
Table 2 Allied health participants’ ActiGraph (GT1M) PA data (N=126)
Self-report PA questionnaires and the level of agreement with ActiGraph accelerometer measurements
provides a summary of the self-report questionnaire measurement of PA levels for the AAS (), IPAQ-L (), and OSPAQ (). The level of absolute agreement between subjective questionnaire measures of PA and objective ActiGraph measures of PA are in . Bland–Altman plots for questionnaire variables which demonstrated significant agreement with ActiGraph measures are presented in .
Figure 1 Bland–Altman plots examining the agreement of statistically significant intraclass correlation coefficient data assessed with the ActiGraph and self-report questionnaires (N=126).
Abbreviations: AAS, Active Australia Survey; PA, physical activity; MVPA, moderate-to-vigorous physical activity; OSPAQ, Occupational Sitting and Physical Activity Questionnaire.
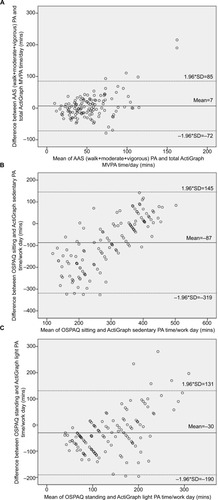
Table 3 Allied health participants’ summary of self-report PA questionnaires (N=126)
Table 4 Level of agreement between self-report PA questionnaires and ActiGraph PA measures (N=126)
Self-report AAS MVPA time and OSPAQ sitting and standing work time showed a fair level of agreement with the corresponding objective ActiGraph accelerometry measurements (, b). The calculated self-report AAS MVPA (walking + moderate + vigorous PA) when compared with the ActiGraph total MVPA [with mean (SD) values of 58 (41) and 51 (24) minutes/day, respectively] demonstrated a fair level of agreement (ICC=0.44, P<0.01) (). The self-report AAS MVPA time compared with the ActiGraph total MVPA time was overestimated by a mean (SD) of 7 (40) minutes/day (, ). The difference between these variables was not significant [t(125)=1.9, P=0.06] () but showed a medium level of correlation with Spearman’s rho (rs)=0.41, P<0.01 ().
The self-report OSPAQ work sitting time when compared with the ActiGraph work sedentary time [with mean (SD) values of 249 (146) and 336 (62) minutes/day, respectively] demonstrated a fair level of agreement (ICC=0.51, P<0.01) (). The self-reported OSPAQ work sitting time compared with the ActiGraph work sedentary time was underestimated by a mean (SD) of –87 (118) minutes/day (, ). OSPAQ self-reported work sitting time was significantly less than the objectively measured Acti-Graph work sedentary time [t(125)=−8.3, P<0.01] (). Furthermore, OSPAQ work sitting time and ActiGraph work sedentary time demonstrated a high level of correlation with rs=0.64, P<0.01 ().
Similarly, self-report OSPAQ work standing time when compared with the ActiGraph work light PA time [with mean (SD) values of 123 (91) and 153 (54) minutes/day, respectively] also demonstrated a fair level of agreement (ICC=0.54, P<0.01) (). The self-reported OSPAQ work standing time compared with the ActiGraph work light PA time was underestimated by a mean (SD) of –30 (82) minutes/day (, ). OSPAQ self-reported work standing time was significantly less than the objectively measured ActiGraph work light PA time [t(125)=−4.1, P<0.01] (). Furthermore, OSPAQ work standing time and ActiGraph work light PA time demonstrated a high level of correlation with rs=0.57, P<0.01 (). The Bland–Altman plots demonstrated that as the amount of time spent in sitting and standing increased, the overall difference between subjective self-report on the OSPAQ and objective ActiGraph time spent in sitting and standing also increased ().
Discussion
The main findings of the study were that allied health professionals spent a mean (SD) of 51 (23) minutes in MVPA/day and walked a mean (SD) of 10,077 (2,766) steps/day (). PA during work hours contributed 76% of the overall recommended total PA requirement for MVPA of 30 minutes/dayCitation1,Citation14 and 54% of the daily recommended 10,000 steps/dayCitation18 (). Self-report PA questionnaires for time spent in MVPA when compared with ActiGraph measures of time spent in MVPA revealed only poor to fair levels of agreement between corresponding measurement tools, with higher MVPA on self-report questionnaires compared with ActiGraph measures ().
Are allied health professionals meeting the recommended guidelines for PA?
The main findings of the study were that allied health professionals spent the majority of their day in sedentary behaviors but were meeting the overall total PA recommendations for MVPA and number of steps/day. Participants spent a mean (SD) of 51 (23) minutes in MVPA/day, which represented 171% of the recommended total PA requirements for MVPA/dayCitation1,Citation14 (). For the group, MVPA/day during work hours contributed a mean of 23 (11) minutes to the overall daily PA, which was 76% of the overall recommended total PA requirements for MVPA/dayCitation1,Citation14 (). Furthermore, 82% (n=103) of allied health participants met the minimum PA MVPA guidelines of ≥30 minutes/day.Citation1,Citation14 A previous study of physiotherapists found that 91% of participants exceeded the minimum recommended PA guidelines reporting greater amounts of time spent in vigorous and walking PA/week.Citation50 Participants in our study walked a mean (SD) of 10,077 (2766) steps/day, which was 100% of the recommended 10,000 steps/dayCitation18 (). The recommended 10,000 steps/dayCitation18 was achieved by 46% (n=57) of our sample, with 30% (n=38) walking between 8,000 and 10,000 steps and 25% (n=31) walking <8,000 steps/day. A recent study examining activity levels of healthcare professionals in New Zealand found that 65% of staff were achieving 10,000 steps/day, which was greater than the overall percentage reported in the general population.Citation52
Our study also demonstrated that participants generally exceeded the recommended PA guidelines based on self-report questionnaires (AAS and IPAQ-L) with overall PA levels reported as a mean (SD) of 1,878 (1,436) and 4,311 (3,632) MET minutes/week (METmins/week), respectively ( and b). Self-reported data from both these questionnaires exceeded the recommended weekly PA levels of ≥600 METmins/week and indicated that the PA levels in our sample were high (ie, ≥1,200 METmins/week).Citation56 This agrees with previous studies using self-report PA questionnaires, which showed that health professionals overall are a physically active group,Citation48,Citation51 with one study reporting that 60% of health professionals reported their PA levels at ≥600 METmins/week.Citation51 Our study demonstrated that 86% and 94% of allied health participants met the minimum PA of ≥600 METmins/weekCitation56 on the AAS and IPAQ-L, respectively. Various studies have reported a wide range in the percentage of the general population meeting the recommended PA guidelines with values ranging from 5% to 75%,Citation28,Citation70,Citation75–Citation77 which may reflect differences between the self-report and objective measurement tools. When objective measures using accelerometry were used to evaluate PA, some studies reported that only 5%–10% met the recommended PA guidelines.Citation70,Citation78 Respondents often overestimated their PA levels on self-report questionnaires when compared with objective accelerometry, and this self-reporting bias may be due to social desirability bias where respondents want to appear as if they are adopting healthy lifestyle behaviors.Citation70 Self-report questionnaires are also prone to misreport due to issues with respondent recall and comprehension of questionnaire items.Citation21,Citation79
Contribution of work PA to overall PA levels in allied health professionals
Our results demonstrated that MVPA during work hours contributed to 76% of the overall recommended daily total PA requirement for MVPA and that steps/day during work accounted for 54% of the daily recommended 10,000 steps/day (). Our results demonstrated that work contributed to a greater amount of the total recommended MVPA and total steps/day in allied health professionals compared with studies examining different occupational sectors.Citation41,Citation53,Citation54 A study conducted in Dutch workers utilizing a cross-sectional survey across various occupational sectors found that the work occupational activity in the health care sector accounted for ~30% of the contribution of work to total PA.Citation53 Studies have demonstrated marked differences in occupational PA across differing occupations and sectorsCitation41,Citation53,Citation54,Citation80,Citation81 and the contribution of PA at work to total levels of PA.Citation41,Citation53,Citation54 Occupations that appear to be relatively active may contribute to a greater degree to the overall total PA levels of individuals.Citation54
Sedentary behavior in allied health professionals
Our study found that allied health professionals engaged on average in a mean (SD) 1,117 (61) minutes (18.6 hours) of sedentary time/day (), which equates to ~10.6 hours of sedentary behavior during waking hours (assuming an average of 8 hours of sleep/night). These results are similar to those of previous studies, which have reported that on average adults spend between 55% and 70% of their day (~9–11 hours/day) in sedentary behaviors.Citation33,Citation34 Furthermore, sedentary time during work hours in our study participants accounted for 336 (61) minutes (5.6 hours)/work day (). A study examining sedentary time in office workers demonstrated that ~77% of working hours (ie, 6.6 hours) were spent in sedentary behaviors,Citation26 which is similar to the sedentary time at work observed in our study participants. These findings suggest that allied health professionals working in a large health district spend the majority of their time at work in sedentary behaviors despite achieving PA recommendations. This is an important consideration as the detrimental effects of sedentary workplace behaviors have been demonstrated even in adults engaging in MVPA throughout the week.Citation32–Citation34
Use of self-report questionnaires in assessing PA levels in allied health professionals
The self-reported MVPA time in the AAS showed only a fair level of agreement with the total ActiGraph measured MVPA time (). The AAS as a tool investigating PA levels has been shown to be subject to less overreport compared with other PA questionnaires such as the IPAQ-L.Citation82 Furthermore, the AAS has been found to have moderate correlation with MVPA levels as measured by accelerometry.Citation82 This is similar to our results () and may reflect that fewer items in this questionnaire may lead to less self-reporting error compared with longer questionnaires such as the IPAQ-L.
The self-report IPAQ-L total MVPA time showed no agreement with the total ActiGraph measure of MVPA time (ICC=0.13, P=0.10) (). The IPAQ-L has been found to be subject to overreport as assessed against reference accelerometry,Citation83–Citation85 with only a low to moderate level of correlation with corresponding MVPA levels as measured by accelerometry.Citation61,Citation82,Citation86 This is similar to the results observed in our study () and may be the result of the large number of questions that rely on recall of a diverse range of activities over a 1-week period.Citation62 Activities in the IPAQ-L such as walking and other moderate activities tend to occur in small bouts throughout the day making these activities difficult to recall,Citation61,Citation62 with individuals finding it easier to recall more structured forms of activity such as planned, high-intensity activities (eg, organized sports, fitness classes).Citation20,Citation61
Our study demonstrated that allied health professionals underestimated their work sitting and standing when assessed against work sedentary behavior and light PA ActiGraph measurements, respectively (), and overestimated the time they spent in occupational walking and heavy labor as assessed against ActiGraph work moderate PA and work ≥ vigorous PA ActiGraph measures, respectively (). This has been described in other studiesCitation57,Citation59 and highlights respondents’ inability to correctly classify their work activi ties on self-report questionnaires in relation to the intensity of PA. Workers often perceived they were performing higher levels of PA at work when compared with objective accelerometry measurements.Citation57 The OSPAQ items sitting and standing demonstrated fair levels of agreement with ActiGraph measurements of work sedentary behavior and work light PA time, respectively (ICC=0.51, P<0.01; ICC=0.54, P<0.01, respectively) (). There was a very good correlation between self-reported OSPAQ sitting and standing time with corresponding ActiGraph measurements of work sedentary behavior and work light PA time (). These results have also been demonstrated in previous studies involving desk-based workers and government/nongovernment organizations and have found moderate validity for estimating time spent sitting and standing at work with lower validity for measuring occupational walking and heavy labor.Citation58,Citation59 This may be because sitting and standing time account for a greater proportion of an individual’s time at work, which may mean less error in recall.Citation57,Citation59 Our study also demonstrated poor levels of agreement between OSPAQ self-reported MVPA and ActiGraph measurements of MVPA at work, and these results may reflect the difficulties of respondents recalling occupational walking and heavy labor tasks, which contribute to MVPA as described in previous studies.Citation58,Citation59
The practical implications of these findings suggest that PA measurements in allied health professionals need to be assessed by accelerometry as self-report PA questionnaires only provide a poor to fair level of agreement when compared with objective measurements. Although allied health professionals are meeting PA recommendations, initiatives to reduce sedentary behavior at work may be of value in facilitating higher levels of PA.
Limitations
There were a number of limitations associated with this study. First, our study may have attracted participation by allied health professionals who were physically active. However, all allied health professionals were encouraged to participate in this study. Furthermore, the use of the ActiGraph may have stimulated participants to be more physically active than usual. Second, the ActiGraph GT1M was a uniaxial accelerometer, which may not have been able to detect movement in all planes and may not have detected some types of activities, eg, upper limb activities, weight training activities, cycling, or swimming activities. Therefore, in some instances, the Acti-Graph GT1M may have underrepresented some participant’s PA levels,Citation61,Citation86 which were reported in the IPAQ-L introducing a possible source of measurement error.Citation61
Conclusion
This study demonstrated that allied health professionals working in a large metropolitan health district met the overall total PA recommendations for MVPA and number of steps/day. When measured objectively, PA during work contributed more than half of the recommended steps/day and greater than three-quarters of the recommended daily MVPA. PA questionnaires demonstrated that allied health professionals surpassed the recommended PA levels; however, they should be interpreted with caution due to poor to fair levels of agreement with accelerometry.
Data sharing statement
Due to ethics requirements participant data from this study cannot be shared unless individual ethics approval is obtained from the relevant human research ethics committees.
Acknowledgments
This study used the REDCap data management system, which is supported by NIH/NCRR Colorado CTSI grant number UL1 RR025780. The contents of the study are the authors’ sole responsibility and do not necessarily represent official National Institutes of Health views. We would also like to acknowledge the following people who assisted with this research project: Associate Professor Emmanuel Stamatakis (The University of Sydney), Emalynne So (Psychology CRGH), Anne Tunks (Dementia Advisory Service, SLHD), Amanda Piggott (Physiotherapy RPAH), Avindu Vithanage, Caitlin Mackenzie (Physiotherapy RPAH), Catherine Wickson, Melissa Cain, Lara Fernandez (Occupational Therapy, Home Based Therapy SLHD), Clare Ferguson, Kiah Witney-Cochrane (Nutrition and Dietetics RPAH), Samantha Tkac (Occupational Therapy, Canterbury Hospital), Garry Jones, Sze Chun Ng (Balmain Hospital), Kylie Draper, Sarah Coventry (Speech Pathology, RPAH), June Hee Choi, Ying Lian (Honors students, The University of Sydney).
Disclosure
The authors report no conflicts of interest in this work.
References
- World Health OrganizationGlobal recommendations on physical activity for health2010 Available from: http://apps.who.int/iris/bitstream/10665/44399/1/9789241599979_eng.pdf158Accessed January 28, 2018
- BaumanAEReisRSSallisJFCorrelates of physical activity: why are some people physically active and others not?Lancet2012380983825827122818938
- HeathGWParraDCSarmientoOLEvidence-based intervention in physical activity: lessons from around the worldLancet2012380983827228122818939
- HaskellWLBlairSNHillJOPhysical activity: health outcomes and importance for public health policyPrev Med200949428028219463850
- LeeIMShiromaEJLobeloFEffect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancyLancet2012380983821922922818936
- DingDLawsonKDKolbe-AlexanderTLThe economic burden of physical inactivity: a global analysis of major non-communicable diseasesLancet2016388100511311132427475266
- JonsdottirIHRödjerLHadzibajramovicEBörjessonMAhlborgGA prospective study of leisure-time physical activity and mental health in Swedish health care workers and social insurance officersPrev Med201051537337720691721
- WenCPWaiJPTsaiMKMinimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort studyLancet201137897981244125321846575
- SattelmairJPertmanJDingELKohlHWHaskellWLeeIMDose response between physical activity and risk of coronary heart disease: a meta-analysisCirculation2011124778979521810663
- SchoenbornCAStommelMAdherence to the 2008 adult physical activity guidelines and mortality riskAm J Prev Med201140551452121496750
- CoombesJSLawJLancashireBFassettRG“Exercise is Medicine”: curbing the burden of chronic disease and physical inactivityAsia Pac J Public Health2015272NP600NP60523572372
- Medibank PrivateThe Cost of Physical Inactivity102008 Available from: https://www.medibank.com.au/client/documents/pdfs/the_cost_of_physical_inactivity_08.pdfAccessed January 24, 2018
- OwenNSugiyamaTEakinEEGardinerPATremblayMSSallisJFAdults’ sedentary behavior determinants and interventionsAm J Prev Med201141218919621767727
- HaskellWLLeeIMPateRRPhysical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart AssociationMed Sci Sports Exerc20073981423143417762377
- MooreSCPatelAVMatthewsCELeisure time physical activity of moderate to vigorous intensity and mortality: a large pooled cohort analysisPLoS Med2012911e100133523139642
- AremHMooreSCPatelALeisure time physical activity and mortality: a detailed pooled analysis of the dose-response relationshipJAMA Intern Med2015175695996725844730
- MarshallSJLevySSTudor-LockeCETranslating physical activity recommendations into a pedometer-based step goal: 3000 steps in 30 minutesAm J Prev Med200936541041519362695
- Tudor-LockeCCraigCLBrownWJHow many steps/day are enough? For adultsInt J Behav Nutr Phys Act201181797921798015
- Tudor-LockeCJohnsonWDKatzmarzykPTRelationship between accelerometer-determined steps/day and other accelerometer outputs in US adultsJ Phys Act Health20118341041921487141
- BrownWJTrostSGBaumanAMummeryKOwenNTest-retest reliability of four physical activity measures used in population surveysJ Sci Med Sport20047220521515362316
- HelmerhorstHJBrageSWarrenJBessonHEkelundUA systematic review of reliability and objective criterion-related validity of physical activity questionnairesInt J Behav Nutr Phys Act20129110310322938557
- MatthewsCEChenKYFreedsonPSAmount of time spent in sedentary behaviors in the United States, 2003-2004Am J Epidemiol2008167787588118303006
- BrownWJBaumanAEOwenNStand up, sit down, keep moving: turning circles in physical activity research?Br J Sports Med2009432868819001015
- ChauJYvan der PloegHPMeromDCheyTBaumanAECross-sectional associations between occupational and leisure-time sitting, physical activity and obesity in working adultsPrev Med2012543–419520022227284
- ThorpAAOwenNNeuhausMDunstanDWSedentary behaviors and subsequent health outcomes in adults a systematic review of longitudinal studies, 1996-2011Am J Prev Med201141220721521767729
- ThorpAAHealyGNWinklerEProlonged sedentary time and physical activity in workplace and non-work contexts: a cross-sectional study of office, customer service and call centre employeesInt J Behav Nutr Phys Act2012912823101767
- MenaiMCharreireHKesse-GuyotEDetermining the association between types of sedentary behaviours and cardiometabolic risk factors: a 6-year longitudinal study of French adultsDiabetes Metab201642211212126404651
- LoyenAClarke-CornwellAMAnderssenSASedentary time and physical activity surveillance through accelerometer pooling in four European countriesSports Med20174771421143527943147
- HallalPCAndersenLBBullFCGlobal physical activity levels: surveillance progress, pitfalls, and prospectsLancet2012380983824725722818937
- MummeryWKSchofieldGMSteeleREakinEGBrownWJOccupational sitting time and overweight and obesity in Australian workersAm J Prev Med2005292919716005804
- van UffelenJGWongJChauJYOccupational sitting and health risks: a systematic reviewAm J Prev Med201039437938820837291
- van der PloegHPCheyTKordaRJBanksEBaumanASitting time and all-cause mortality risk in 222 497 Australian adultsArch Intern Med2012172649450022450936
- MatthewsCEGeorgeSMMooreSCAmount of time spent in sedentary behaviors and cause-specific mortality in US adultsAm J Clin Nutr201295243744522218159
- ChauJYGrunseitACCheyTDaily sitting time and all-cause mortality: a meta-analysisPLoS One2013811e8000024236168
- ChomistekAKMansonJEStefanickMLRelationship of sedentary behavior and physical activity to incident cardiovascular disease: results from the Women’s Health InitiativeJ Am Coll Cardiol201361232346235423583242
- StamatakisEChauJYPedisicZAre sitting occupations associated with increased all-cause, cancer, and cardiovascular disease mortality risk? A pooled analysis of seven British population cohortsPLoS One201389e7375324086292
- GarciaLMda SilvaKSdel DucaGFda CostaFFNahasMVSedentary behaviors, leisure-time physical inactivity, and chronic diseases in Brazilian workers: a cross sectional studyJ Phys Act Health20141181622163424732950
- Bjørk PetersenCBaumanAGrønbækMWulff HelgeJThygesenLCTolstrupJSTotal sitting time and risk of myocardial infarction, coronary heart disease and all-cause mortality in a prospective cohort of Danish adultsInt J Behav Nutr Phys Act20141111324498933
- BiddleSJSedentary behaviorAm J Prev Med200733650250418022068
- ProperKISinghASvan MechelenWChinapawMJSedentary behaviors and health outcomes among adults: a systematic review of prospective studiesAm J Prev Med201140217418221238866
- JansMPProperKIHildebrandtVHSedentary behavior in Dutch workers: differences between occupations and business sectorsAm J Prev Med200733645045418022060
- OwenNHealyGNMatthewsCEDunstanDWToo much sitting: the population health science of sedentary behaviorExerc Sport Sci Rev201038310511320577058
- LoyenAvan der PloegHPBaumanABrugJLakerveldJEuropean sitting championship: prevalence and correlates of self-reported sitting time in the 28 European Union member statesPLoS One2016113e014932026934701
- KirkMARhodesREOccupation correlates of adults’ participation in leisure-time physical activity: a systematic reviewAm J Prev Med201140447648521406284
- JakaMMHaapalaJLWolfsonJFrenchSADescribing the relationship between occupational and non-occupational physical activity using objective measurementPrev Med Rep2015221321726000235
- DayoubEJenaABChronic disease prevalence and healthy lifestyle behaviors among US health care professionalsMayo Clin Proc201590121659166226422242
- FlorindoAABrownsonRCMielkeGIAssociation of knowledge, preventive counseling and personal health behaviors on physical activity and consumption of fruits or vegetables in community health workersBMC Public Health20151534425885709
- AtanTTuralEImamogluOCicekGTuralSPhysical activity levels of teachers and health professionals in TurkeyHealthMED20126619351942
- ArvidsonEBörjessonMAhlborgGLindegårdAJonsdottirIHThe level of leisure time physical activity is associated with work ability-a cross sectional and prospective study of health care workersBMC Public Health20131385524044699
- McphailSMWaiteMCPhysical activity and health-related quality of life among physiotherapists: a cross sectional survey in an Australian hospital and health serviceJ Occup Med Toxicol201491124405934
- KuneneSHTaukobongNPLevel of physical activity of health professionals in a district hospital in KwaZulu-Natal, South AfricaS Afr J Physiother20157116
- ChanLMcnaughtonHWeatherallMAre physical activity levels of health care professionals consistent with activity guidelines? A prospective cohort study in New ZealandJRSM Cardiovasc Dis20187204800401774901
- ProperKIHildebrandtVHPhysical activity among Dutch workers–differences between occupationsPrev Med2006431424516684560
- SteevesJATudor-LockeCMurphyRAKingGAFitzhughECHarrisTBClassification of occupational activity categories using accelerometry: NHANES 2003-2004Int J Behav Nutr Phys Act2015128926122724
- Sealed Envelope LtdPower calculator for continuous outcome non-inferiority trial. [Online]2012 Available from: https://www.sealedenvelope.com/power/continuous-noninferior/Accessed April 20, 2016
- BrownWJBurtonNWMarshallALMillerYDReliability and validity of a modified self-administered version of the Active Australia physical activity survey in a sample of mid-age womenAust N Z J Public Health200832653554119076744
- ReisJPDuboseKDAinsworthBEMaceraCAYoreMMReliability and validity of the occupational physical activity questionnaireMed Sci Sports Exerc200537122075208316331132
- ChauJYvan der PloegHPDunnSKurkoJBaumanAEValidity of the occupational sitting and physical activity questionnaireMed Sci Sports Exerc201244111812521659903
- PedersenSJKiticCMBirdMLMainsbridgeCPCooleyPDIs self-reporting workplace activity worthwhile? Validity and reliability of occupational sitting and physical activity questionnaire in desk-based workersBMC Public Health201616183627542603
- CraigCLMarshallALSjöströmMInternational physical activity questionnaire: 12-country reliability and validityMed Sci Sports Exerc20033581381139512900694
- HagströmerMOjaPSjöströmMThe International Physical Activity Questionnaire (IPAQ): a study of concurrent and construct validityPublic Health Nutr20069675576216925881
- KimYParkIKangMConvergent validity of the International Physical Activity Questionnaire (IPAQ): meta-analysisPublic Health Nutr201316344045222874087
- JohnDFreedsonPActiGraph and Actical physical activity monitors: a peek under the hoodMed Sci Sports Exerc2012441 Suppl 1S868922157779
- KozeySLStaudenmayerJWTroianoRPFreedsonPSComparison of the ActiGraph 7164 and the ActiGraph GT1M during self-paced locomotionMed Sci Sports Exerc201042597197619997000
- SilvaPMotaJEsligerDWelkGTechnical reliability assessment of the actigraph GT1M accelerometerMeas Phys Educ Exerc Sci20101427991
- LeeKYMacfarlaneDJCerinEComparison of three models of actigraph accelerometers during free living and controlled laboratory conditionsEur J Sport Sci201313333233923679150
- FreedsonPSMelansonESirardJCalibration of the computer science and applications, inc. accelerometerMed Sci Sports Exerc19983057777819588623
- NortonKNortonLSadgroveDPosition statement on physical activity and exercise intensity terminologyJ Sci Med Sport201013549650220005170
- MâsseLCFuemmelerBFAndersonCBAccelerometer data reduction: a comparison of four reduction algorithms on select outcome variablesMed Sci Sports Exerc20053711 SupplS544S55416294117
- TroianoRPBerriganDDoddKWMâsseLCTilertTMcdowellMPhysical activity in the United States measured by accelerometerMed Sci Sports Exerc200840118118818091006
- HartTLSwartzAMCashinSEStrathSJHow many days of monitoring predict physical activity and sedentary behaviour in older adults?Int J Behav Nutr Phys Act201186221679426
- HarrisPATaylorRThielkeRPayneJGonzalezNCondeJGResearch electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics supportJ Biomed Inform200942237738118929686
- StreinerDLNormanGRCairneyJHealth Measurement Scales: A Practical Guide to Their Development and Use5th edOxfordOxford University Press2014
- CohenJA power primerPsychol Bull1992112115515919565683
- GerovasiliVAgakuITVardavasCIFilippidisFTLevels of physical activity among adults 18-64 years old in 28 European countriesPrev Med201581879126299619
- MarquesASarmentoHMartinsJSaboga NunesLPrevalence of physical activity in European adults - compliance with the World Health Organization’s physical activity guidelinesPrev Med20158133333826449407
- KatzmarzykPTLeeIMMartinCKBlairSNEpidemiology of physical activity and exercise training in the United StatesProg Cardiovasc Dis201760131028089610
- TuckerJMWelkGJBeylerNKPhysical activity in U.S.: adults compliance with the physical activity guidelines for AmericansAm J Prev Med201140445446121406280
- SkenderSOseJChang-ClaudeJAccelerometry and physical activity questionnaires - a systematic reviewBMC Public Health201616151527306667
- Brighenti-ZoggSMundwilerJSchüpbachUPhysical workload and work capacity across occupational groupsPLoS One2016115e015407327136206
- DeyaertJHarmsTWeenasDGershunyJGlorieuxIAttaching metabolic expenditures to standard occupational classification systems: perspectives from time-use researchBMC Public Health201717162028673271
- TimperioASalmonJRosenbergMBullFCDo logbooks influence recall of physical activity in validation studies?Med Sci Sports Exerc20043671181118615235322
- MacfarlaneDJLeeCCHoEYChanKLChanDConvergent validity of six methods to assess physical activity in daily lifeJ Appl Physiol200610151328133416825525
- CerinECainKLOyeyemiALCorrelates of agreement between accelerometry and self-reported physical activityMed Sci Sports Exerc20164861075108426784274
- WannerMProbst-HenschNKriemlerSMeierFAutenriethCMartinBWValidation of the long international physical activity questionnaire: influence of age and language regionPrev Med Rep2016325025627419023
- HagstromerMAinsworthBEOjaPSjostromMComparison of a subjective and an objective measure of physical activity in a population sampleJ Phys Act Health20107454155020683097