Abstract
Background
Many patients ask for advice about choosing a pillow. This research was undertaken to determine if pillow type alters cervico-thoracic spine position when resting in the side-lying position.
Aim
To investigate the effect of different pillow shape and content on the slope of cervico-thoracic spine segments when side lying.
Materials and methods
The study was a randomized blinded comparative trial set in a laboratory that replicated a bedroom. The subjects were side sleepers aged over 18 years. Exclusion criteria were history of surgery to the cervico-thoracic spine, an injury or accident to the cervico-thoracic spine in the preceding year, or currently receiving treatment for neck symptoms. Each participant rested in a standardized side-lying position for 10 minutes on each of the trial pillows: regular shaped polyester, foam, feather, and latex pillows, and a contour shaped foam pillow. Reflective markers were placed on external occipital protuberance (EOP), C2, C4, C7, and T3, and digital images were recorded of subjects at 0 and 10 minutes on each pillow. Images were digitized using each reflective marker and the slope of each spinal segment calculated. Univariate analysis of variance models were used to investigate slope differences between pillows at 0 and 10 minutes. Significance was established at P < 0.01 to take account of chance effects from repeated measures and multiple comparisons.
Results
At 0 and 10 minutes, the EOP-C2, C2-C4, and C4-C7 segmental slopes were significantly different across all pillows. Significant differences were identified when comparing the feather pillow with the latex, regular and contour foam pillows, and when comparing the polyester and foam contour pillows. The regular and contour foam pillows produced similar slopes at all spinal segments.
Conclusion
Cervico-thoracic spinal segment slope alters significantly when people change from a foam, latex, or polyester pillow to a feather pillow and vice versa. The shape of a foam pillow (contour versus regular shape) does not significantly alter cervico-thoracic spinal segment slope.
Keywords:
Introduction
Many patients present with symptoms related to the cervico-thoracic spine, such as pain, stiffness, headache, and scapular pain. Changing pillows can significantly alter waking cervical pain and stiffness, headache, and scapular pain reports.Citation1–Citation5 Many people appear to have made poor pillow choices, as low sleep quality, low pillow comfort, and waking cervico-thoracic symptoms are commonly reported.Citation6 Hence they often ask their health practitioner for advice regarding pillow selection. While it is widely believed that a pillow which holds the cervical spine in a “neutral” position prevents cervical waking symptoms, by minimizing end-range positioning of spinal segments,Citation7–Citation12 no information is available about how to achieve such a position. A range of subjective recommendations regarding pillow choice have been provided. These include use of pillows of malleable consistency such as feathers, kapok, or foam chip which provide support for the head but avoid pushing the head into flexion or lateral flexion and alter shape to the contours of the individual.Citation13 People have been advised not to use molded foam or latex pillows, which resist comfortable indentation of body contours,Citation9,Citation13 to use a cervical roll in the pillow,Citation10,Citation13,Citation14 or to use a contour pillow.Citation9,Citation15 The range of advice is confusing for consumers and health professionals and is not underpinned by published scientific evidence. There has been very limited research to understand or assess the effect of different pillow types on cervical spine posture, and appropriate recommendations cannot be made unless the manner in which the spine responds to specific pillow content and shape are better understood.
As side lying is the most common adult sleeping position,Citation16 studies investigating how pillows support the cervical spine should focus firstly on this position. Presumably, stabilization of cervical spine position in the side-lying position will occur when the pillow and mattress have compacted in response to mass and spinal creep has occurred. Previous research has identified that in the side-lying position on a firm examination plinth, 10 minutes is required for stabilization of cervical spine position when lying on pillows of various filler.Citation17
This paper reports the effect of five different pillow types on the slope of cervico-thoracic spine segments, over 10 minutes, when resting in a standardized side-lying position. Our hypotheses were that each pillow would support cervico-thoracic spine segments differently at 0 and 10 minutes and that the change in slope of cervico-thoracic spinal segments over 10 minutes would be different for each pillow type.
Materials and methods
Ethics
Ethical approval was provided by the Human Research Ethics Committee of the University of South Australia.
Study design
The study was a laboratory-based, randomized, blinded comparative trial in which subjects acted as their own control.
Participants
Sample size
Sample size was calculated for gender–age clusters using validated software, applying a repeated intervention design formula with power of 80%, alpha of 5%.Citation18 Age clusters were young (<40 years), middle (40–59 years), and old (60+ years). A minimum of 12 subjects was required in each of six age–gender clusters.
Setting and sampling
All subjects came from a large South Australian regional city, whose population was similar to the South Australian demographic profile at the time.Citation19,Citation20 Subjects were initially invited in the six gender–age clusters from subjects randomly selected from the register of an earlier population study on pillows.Citation21 Where clusters remained incomplete after this invitation, volunteers were recruited via local newspaper advertisements.
Inclusion criteria
Side-sleepers aged over 18 years were recruited. Exclusion criteria were history of cervico-thoracic spine surgery, an injury or accident to the cervico-thoracic spine in the preceding year, or currently receiving treatment for neck symptoms.
Intervention
Five pillows were tested, these being the most commonly reported in our earlier community telephone survey.Citation1 New pillows were procured for the trial: polyester, synthetic fiber fill provided by the Tontine Group (Brunswick East, VIC, Australia); foam regular shape (Comfort Classic) and foam contour shape (Medi Rest), both supplied by Dentons Pty Ltd (Wantirna South, VIC, Australia) and molded from the same high density foam; Dunlopillo® (Hilding Anders, Huntingdon, England, UK) latex pillows provided by the University of South Australia; and feather pillows purchased by the principal author from Target Australia Pty, Ltd. Pillow suppliers were independent of the study conduct and interpretation and reporting of results.
The depth of the foam regular pillow was 120 mm, the foam contour pillow varied between 120 and 142 mm across the contour, the latex pillow was 115 mm, the feather pillow was 120 mm, and the polyester pillow was 118 mm.
De-identification
To assist blinding of measurers and subjects, the trial pillows were de-identified as much as possible by removing pillow labels and covering pillows with pillowcases of the same brand and color.
Procedures
The laboratory consisted of four measurement cubicles, each containing an identical single bed innerspring ensemble (Aussie Mate ensemble; Adriatic Slumber Bedding, Dry Creek, South Australia), and a digital camera mounted on a tripod placed parallel to, and 1 m from, the participant’s neck. A spirit level was used to align the camera to neutral in both the vertical and horizontal planes before taking each photograph. Pillow order was randomized by ballot for each participant.
Instructions and test position
Preparation
Participants agreed not to perform any unusual exercise/activities in the days prior to testing. No “limbering up” exercises were given prior to testing, and the pillow position was standard for everyone. Participants were permitted to sit up briefly to stretch and move their neck between each pillow trial.
Test position
Participants assumed a standardized right-side-lying position with their head resting on the pillow, both arms placed at 45° in front of the trunk with their knees flexed together at 90°, and the hips bent at 60° to the trunk. A self-adhesive reflective marker of 5 mm diameter (made with a standard paper hole punch) was placed on a headband placed over the external occipital protuberance (EOP) and on the spinous processes of C2, C4, C7, and T3.
Intervention administration
Subjects attended for one 90-minute session, and tested every trial pillow. Administration order was randomized by ballot for every subject by a nonblinded research assistant, who then administered the trial.
Test time
Subjects lay on each trial pillow for 10 minutes. They could sit up briefly to stretch between each pillow trial.
Validity and accuracy of marker placement
A preliminary test established the accuracy of the principal researcher’s external placement of markers on spinous processes in side-lying. Two experienced physiotherapists (SJG, PHT) palpated the spinous processes of C4, C7, and T3 on six participants, and marked each anatomical point by felt-tip pen (total 18 points). The accuracy of the marker positions was then verified by an experienced sonographer using portable diagnostic ultrasonography. The preliminary data were analyzed before commencing the trial, by calculating the percentage agreement between the 18 ultrasonographic positions and the marker placements.
Outcome measure
A digital image was recorded at the start and end of the pillow trial (0 and 10 minutes). The position of each landmark was digitized from each image using ImageTool software (Department of Dental Diagnostic Science, The University of Texas Health Science Center, San Antonio, TX). To ensure inter-assessor reliability of digitized coordinates, 30 landmarks were digitized by the two assessors. The correlation coefficient for the x-coordinate digitization was 0.92 and for the y-coordinate digitization, 0.94. The linear coordinates from each landmark were used to calculate intersegmental slopes relative to horizontal using the formula: (y2 − y1)/(x2 − x1).
For example, using the EOP-C2 segment, slope was calculated as (yC2 − yEOP)/(xC2 − xEOP). The direction of slope was indicated by a positive or negative sign (+ or −). A negative value indicated that the more proximal landmark of the segment (eg, EOP in the example above) was higher than the distal landmark (eg, C2 spinous process). Conversely, a positive value indicated that the distal landmark of the segment was higher than the proximal landmark.
Statistical analysis
The mean, range, and standard deviation of each segmental slope at 0 and 10 minutes, and change in slope over this time, were calculated. Differences in change in segmental slope between pillows at 0 and 10 minutes, and over the 10-minute pillow trial were assessed using univariate analysis of variance (ANOVA) models. Significance was established at P < 0.01 to take account of chance effects from repeated measures and multiple comparisons.
Results
Pilot study
There was 94% overall agreement between researcher palpated spinous processes and their ultrasonographic identification in side lying. Agreement was similar for each anatomical point. This confirmed the validity of external palpation to mark landmarks on spinous processes of the cervical spine in side lying by the researchers (SJG, PT).
Photographic study
Participants
A total of 95 subjects participated (86 from the earlier study register, and nine from newspaper advertisements).
Slope at 0 minutes
The ANOVA models identified significant differences in EOP-C2, C2-C4, and C4-C7 segmental slopes when comparing individuals lying on each pillow (see and ). Generally, the extremes of mean slope measure occurred when resting on the feather and foam contour pillows.
Figure 1 Mean slope at zero minutes, for each spinal segment.
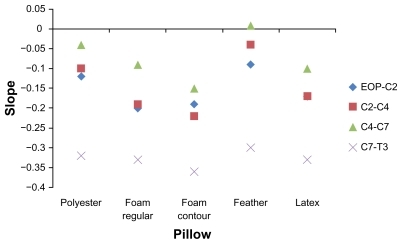
Table 1 Mean, standard deviation, and minimum and maximum values of slope at 0 and 10 minutes and the change in slope over 10 minutes, for each segment on each pillow
Slope at 10 minutes
The ANOVA models also identified significant differences in EOP-C2, C2-C4, and C4-C7 segmental slopes when comparing individuals lying on each pillow at 10 minutes (see and ). The slopes were similar for the regular foam and latex pillows, indicating similar support provided to spinal segments by these pillows. The extremes of mean slope measure again occurred when resting on the feather and foam contour pillows.
Figure 2 Mean slope at 10 minutes for each spinal segment, for each pillow.
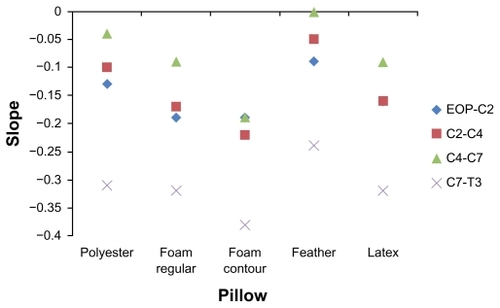
Table 2 T-test confidence limits and P values comparing spinal segment slopes for pairs of pillows at 10 minutes
At 0 and 10 minutes, for all segments, pillows filled with particulate matter (polyester and feather) (“soft” pillows), produced spinal slope distributions which were more positive (the distal landmark was higher than the proximal landmark) than the other pillows, which had more solid filler (foam and latex).
Slope change
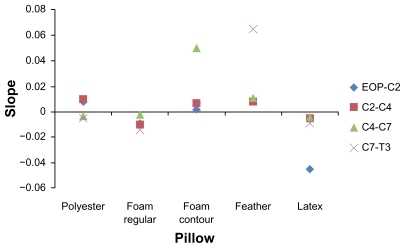
Most segmental slopes changed less than 0.01 units over 10 minutes (see and ). However overall, there was no significant difference in slope change at any spinal segment over 10 minutes when comparing pillows.
Figure 3 Mean change in slope over 10 minutes for each spinal segment, for each pillow.
Comparing the segmental slopes between pairs of pillows at 10 minutes
Side lying on the feather pillow resulted in significantly different slopes at C2-C4, C4-C7, and C7-T3 when compared with the foam contour pillow, at EOP-C2 and C2-C4 when compared with the regular foam pillow, and at C2-C4 when compared with the latex pillow. Side lying on the polyester pillow resulted in significantly different slopes at C2-C4 and C4-C7 when compared with the contour foam pillow. The slope of the C2-C4 spinal segment appears to be the most sensitive to change in pillow type. The foam regular, foam contour, and latex pillows support each segment of the spine in a similar manner as do the polyester and feather pillows.
Discussion
This paper reports the largest known study of the effect of pillow shape and filler on cervico-thoracic posture in the side-lying position. Pillows of different content and shape supported each spinal segment in a significantly different manner at 0 and 10 minutes. However, no significant difference was found in the change in slope over 10 minutes between pillows included in this study. This suggested that all pillows in this study, irrespective of content and shape, altered in the support they provided to the head and neck in a similar manner over 10 minutes. Slope changes over 10 minutes were small on every pillow, suggesting that spinal creep, mattress, and pillow deformation were negligible.
As both foam pillows were made of the same foam (differing only in shape), any variation in the support provided to the cervico-thoracic spine could be attributed to shape alone. The foam contour pillow produced steeper (although nonsignificant) slopes at each spinal segment compared with the foam regular pillow. Thus there is no evidence to support the recommendation of a foam contour pillow over a foam regular pillow to achieve a neutral cervico-thoracic spine posture in side sleepers. Further research using different depths of contour is indicated.
The widest slope range at 10 minutes occurred at the C2-C4 and C4-C7 spinal segments, highlighting the vulnerability of these segments to slope change, and their usefulness in assessing the form of the cervical spine related to pillow performance. This may be explained by the kinematics of the cervical spine, where the EOP-C2 and C7-T3 segments are relatively inflexible in frontal plane movements compared with the C2-C4 and C4-C7 spinal segments.
The more positive slope distributions produced by the “soft” pillows, compared with the more negative distributions of the pillows with more solid filler (foam and latex) resulted in the “soft” pillows generally supporting the distal landmark of any segment in a higher position than the proximal landmark, whereas the firmer pillows supported the proximal landmark in a higher position than the distal one of the segment. This difference should be investigated with respect to waking symptom production, pillow comfort, and sleep quality on different pillows.
The strengths of this study included the replication of a real-life sleeping environment by using a common ensemble mattress as the base. By having a large sample of subjects acting as their own controls, the study has identified robust within-subject changes on different pillows over time. Limitations include that subjects were resting rather than sleeping, and no information is currently available regarding differences in cervico-thoracic muscle function between resting and sleeping on a pillow. The study period (10 minutes) was based on previous research which assessed the stabilization of spinal segments when lying on a firm examination couch.Citation17 The use of a less firm innerspring mattress in this study may have altered the time required for stabilization of spinal position on each pillow. While the starting position of participants was standardized, the scapular position over the 10 minutes was not controlled, and this should be considered in future studies. Further research considering anthropometry, pillow type, support surfaces, and spinal slope is required. Future research should explore methods to allow assessment of movement and posture of the cervico-thoracic spine in other planes.
A previous report of cervico-thoracic spine posture on x-ray in relation to contour pillow use in the supine position used a sample of one.Citation9 All other identified pillow studies have used subjective measures to investigate the relationship between contour-shaped pillows and pillow comfort and neck symptomsCitation4,Citation22–Citation25 or compared contour and regular-shaped pillows.Citation4,Citation5,Citation22 No previous research has quantified or described the effect of pillow type on cervico-thoracic spine posture.
Conclusion
The pillow is only one factor which contributes to sleep quality and waking symptoms.Citation26,Citation27 This research, however, indicates that if people are using a similar foam, latex, or polyester pillow as used in this research, the support provided by the pillow will alter significantly if they change to a feather pillow and vice versa. Many health practitioners are asked specifically about contour pillow use, and the results of this study do not indicate that the contour foam pillow supports the cervico-thoracic spine any differently to a regular shaped foam pillow when side lying. Further research is required to assess the effect of different contour pillow depth and their use in the supine position.
Acknowledgments
The authors would like to thank both Dentons Pty Ltd and the Tontine Group for supplying pillows for this research, David Forbes of Forbes Furniture for supplying the mattresses, and Bob Edmonds and Kym Hosking for assistance with the slope measures.
Disclosure
The authors report no conflicts of interest in this work. Apart from the supply of some pillows by Dentons Pty Ltd and the Tontine Group, this research was unfunded.
References
- GordonSGrimmerKTrottPPillow use: the behaviour of cervical pain, sleep quality and pillow comfort in side sleepersMan Ther200914667167819427257
- GordonSJGrimmerKATrottPHPillow use: the behaviour of cervical stiffness, headache and scapular painJ Pain Res2010313714521197317
- BernateckMKarstMMerkesdalSSustained effects of comprehensive inpatient rehabilitative treatment and sleeping neck support in patients with chronic cervicobrachialgia: a prospective and randomized clinical trialInt J Rehabil Res200831434234619008684
- PerssonLNeck pain and pillows – a blinded study of the effect of pillows on non-specific neck pain, headache and sleepAdv Physiother200683122127
- HaginoCBoscariolJDoverLBefore/after study to determine the effectiveness of the align-right cylindrical cervical pillow in reducing chronic neck pain severityJ Manipulative Physiol Ther19982189939502063
- GordonSJGrimmer-SomersKYour pillow may not guarantee a good night’s sleep or symptom-free wakingPhysiother Can2011632183190
- BlandJHBousheyDRDisorders of the cervical spinePhiladelphia, PAsaunders1987
- GrieveGPCommon vertebral joint problems2nd edEdinburghChurchill Livingstone1988
- JacksonRThe cervical spine3rd edSpringfield IllinoisCharles C Thomas1976
- KramerJIntervertebral disk diseases: causes, diagnosis, treatment and prophylaxis2nd edNew York, NYThieme Medical Publishers Inc1990
- LansamRPillow talkingCare in the Home19921215
- McDonnellJSleep posture: its implicationsBr J Phys Med19469465221028552
- McKenzieRMaySWThe cervical and thoracic spine: mechanical diagnosis and therapy2New ZealandSpinal Publications2006
- ElkindAHMuscle contraction headachePostgrad Med1987832032183588462
- EmbersonMWSupport pillowPhysiotherapy198571498
- DeKoninckJLorrainDGagnonPSleep positions and position shifts in five age groups: an ontogenetic pictureSleep1992151431491579788
- PuntumetakulRCervical pillows: the relationship between the pillow content and contact pressure, alignment of the cervical spine, and participant ratings of support and comfort under the head and neck [MA thesis]AdelaideSchool of Physiotherapy, University of South Australia1993
- SchoenfeldDAStatistical considerations for clinical trials and scientific experiments [webpage on the Internet; updated May 14, 2010]Sample size calculation developed with support from the Massachusetts General Hospital Mallinckrodt General Clinical Research Center, Research Resources Division, National Institutes of Health, General Clinical Research Center Program2010 Available from: http://hedwig.mgh.harvard.edu/sample_size/size.htmlAccessed July 11, 2011
- Australian Bureau of Statistics2001 Census of Population and Housing Australia (Australia): Age by SexCanberra. CanberraAustralian Bureau of Statistics2001 Available from http://www.censusdata.abs.gov.au/ABSNavigation/prenav/ViewData?action=404&documentproductno=0&documenttype=Details&order=1&tabname=Details&areacode=0&issue=2001&producttype=Census%20Tables&javascript=true&textversion=false&navmapdisplayed=true&breadcrumb=TLPD&&collection=Census&period=2001&productlabel=Age%20by%20Sex&producttype=Census%20Tables&method=Location%20on%20Census%20Night&topic=Population%20Size%20&%20Growth&Accessed March 10, 2009
- Australian Bureau of Statistics2001Census quickstats: Port Lincoln (C) (local government area) [webpage on the Internet]CanberraAustralian Bureau of Statistics2006 Available from: http://www.censusdata.abs.gov.au/ABSNavigation/prenav/LocationSearch?locationLastSearchTerm=port+lincoln&locationSearchTerm=port+lincoln&newarea=LGA46300&submitbutton=View+QuickStats+%3E&mapdisplay=on&collection=Census&period=2001&areacode=LGA46300&geography=&method=Location+on+Census+Night&productlabel=&producttype=QuickStats&topic=&navmapdisplayed=true&javascript=true&breadcrumb=PL&topholder=0&leftholder=0¤taction=104&action=401&textversion=false&subaction=1Accessed July 15, 2011
- GordonSGrimmerKTrottPSleep position, age, gender, sleep quality and waking cervico-thoracic symptomsInternet J Allied Health Sci Pract [journal on the Internet]200751 Available from: http://ijahsp.nova.edu/articles/vol5num1/gordon2.pdfAccessed 2011 Jun 26
- LavinRAPappagalloMKuhlemeierKVCervical pain: a comparison of three pillowsArch Phys Med Rehabil1997781931989041902
- ErfanianPHaginoCGuerrieroRA preliminary study assessing adverse effects of a semi-customized cervical pillow on asymptomatic adultsJ Can Chiropr Assoc199842156162
- PerssonLMoritzUNeck support pillows: a comparative studyJ Manipulative Physiol Ther1998212372409608378
- ErfanianPTenzifSGuerrieroRCAssessing effects of a semi-customized experimental cervical pillow on symptomatic adults with chronic neck pain with and without headacheJ Can Chiropr Assoc200448202917549216
- GordonSGrimmerKTrottPUnderstanding sleep quality and waking cervico-thoracic symptomsInternet J Allied Health Sci Pract [journal on the Internet]200752 http://ijahsp.nova.edu/articles/vol5num2/gordon.pdfAccessed 2011 Jun 26
- VersterJCPandi-PerumalSRStreinerDLSleep and quality of life in clinical medicineTotowa, NJHumana Press2008