
Abstract
Aim
Clinical practice guidelines (CPGs) have progressively become a popular tool for making optimal clinical decisions. The literature shows that the poor quality of CPGs can form a barrier against adhering to them, resulting in a suboptimal level of healthcare. The objective of this systematic review is to evaluate the quality of CPGs in the Middle East and North Africa (MENA) region using the Appraisal of Guidelines for Research & Evaluation II (AGREE II) Instrument.
Methods
The authors searched in the MEDLINE and EMBASE databases through the Ovid interface on May 25, 2019. Keywords relating to CPGs and MENA countries were combined using Boolean search operators. The search was not limited to specific diseases. The quality of guidelines was appraised by two reviewers independently using the AGREE II Instrument. Discrepancies within a group were resolved through the involvement of a principle investigator.
Results
A total of 61 CPGs were appraised. These guidelines were mainly from Saudi Arabia, and the most covered disease topic was cancer. Among the six domains of the AGREE II Instrument, CPGs scored the highest on clarity of presentation (mean 82%), while the lowest score was granted to the rigor of development domain (mean 28%). This indicates substantial deficiencies in reporting the developmental processes of CPGs and the resources used for the synthesis of evidence.
Conclusion
From this review, it was found that the number of retrieved guidelines published in the MENA region is limited considering the large geographical area of the MENA region. The main domains that have higher quality scores were clarity of presentation and scope and purpose, whereas domains with the lowest scores were rigor of development and applicability. The authors’ findings will help policymakers identify areas for improvement in CPGs, which can lead them to implement strategies such as the training of individuals and recruitment of international experts to ultimately develop high-quality CPGs.
Background
Clinical practice guidelines (CPGs) are defined by the Institute of Medicine (IOM) as statements that include recommendations intended to optimize patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options.Citation1 CPGs can provide several benefits to clinicians, institutions, and patients. The use of recommendations from CPGs assists clinicians in making decisions about individual patient management.Citation2 On an institutional level, the use of CPGs allows the provision of standardized care to patients with the aim of decreasing variations in clinical practice.Citation3 They also improve the quality of care and reduce preventable errors in medication.Citation3 These possible benefits can eventually promote cost-effective care.Citation4 Also, patients can benefit from some CPGs that are accompanied by “consumer” versions, which include a simple summary of the benefits and harms of available options.Citation5 Thus, it empowers patients to make more informed healthcare choices and to consider their personal needs and preferences in selecting the best option.Citation5 Nowadays, the number of published CPGs is progressively expanding.Citation6 However, the quality of those guidelines is still inconclusive.Citation7–Citation9
The AGREE II Instrument (Appraisal of Guidelines for Research & Evaluation II) is one of the widely used, validated tools for evaluating CPGs. The instrument includes specific assessment questions that cover many aspects of the quality of guidelines with a focus on methodological rigor.Citation10 It has been widely used to assess guidelines in various clinical conditions.Citation11–Citation16 High-quality clinical practice guidelines could have substantial positive impact on patients and healthcare providers. Evidence suggests that high quality could improve patients’ clinical outcomes, provide an equitable clinical recommendation that are effective, safe and appropriate to the target population.Citation17,Citation18
To our knowledge, there is no study that reviews the quality of published guidelines for clinical practice in the Middle East and North Africa (MENA) region. Several systematic reviews have been conducted to compare the quality of guidelines among high-income countries including the United statesCitation19–Citation21 and Europe.Citation22–Citation26 Similar systematic reviews were also performed for low- and middle-income countries including Turkey,Citation7 China,Citation9 and Sri Lanka.Citation8 The quality of clinical practice guidelines varies across countries. In the United States and Europe, lowest scores were assigned to “applicability” and “editorial independence”, whereas, in other developing countries including Turkey, China and Sri Lanka, the rigour of development received low scores on AGREE II Instrument.
The MENA region consists of high-, middle-, and low-income countries.Citation27,Citation28 In addition, there are variations in the financing of healthcare and the socioeconomic contexts in these countries.Citation29 Therefore, conclusions from the previously mentioned systematic reviews cannot be generalized to the MENA region. The aim of this study is to assess the quality of CPGs in the MENA region using the validated AGREE II Instrument.Citation10
Methodology
The review’s protocol is registered with the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD42019132437).
Identification of Guidelines
The sources were the MEDLINE and EMBASE databases through the Ovid interface, and the review was conducted on May 25, 2019, to identify CPGs. Additionally, gray literature has been manually searched to identify CPGs in all relevant health organization websites including those of the ministries of health and medical organizations of the MENA countries involved (Appendix 1). Keywords and terms relating to CPGs and all the MENA countries were combined using Boolean search operators (Appendix 2).
Selection of Guidelines
We used the institution of medicine (IOM) definition for clinical practice guidelines:
Statements that include recommendations intended to optimize patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options.Citation1
Therefore, the included guidelines should fulfil the following criteria:
Guidelines are developed by medical societies or governmental institutions.
Guidelines should describe the methods used to search the literature and identify eligible studies.
Guidelines should provide structured recommendations based on reviewed studies.
We included English language guidelines that were produced by countries with MENA region organizations.Citation27,Citation28 Short summaries, narrative and systematic reviews, abstracts, and posters were excluded. The detailed criteria are listed in .
Table 1 Eligibility Criteria
Data Collection Process
One author (N. A.) conducted the search of electronic databases. Three authors—L. S., N. A., and W. H.—searched and screened the gray literature. Afterwards, two independent authors were involved in screening the results from the electronic databases by title, abstract, and then full text to select eligible guidelines. Conflicts and disagreements were resolved by discussion or by the involvement of an independent reviewer, if necessary. Also, two authors independently extracted and assessed the quality of the selected CPGs. Extracted data included the CPG name, specialty, year of publication, and country.
AGREE II Instrument Domain Descriptions
The AGREE II Instrument consists of six major domains that include a total of 23 different items.Citation10 The domains includes, scope and purpose, stakeholder involvement, rigor of development, clarity of presentation, applicability and editorial independence. Following these domains, there are two general rating items also known as overall assessments. The first overall assessment question requires the user to make a judgment regarding the overall quality of a guideline, taking into consideration the criteria considered in the assessment process. In the second overall assessment question, the user is asked whether she/he recommends using the CPG or not.Citation10
Each of the 23 items of the six domains and the overall assessment questions were rated as a part of the quality assessment. The AGREE II Instrument provides a rating scale from 1 to 7 with 1 indicating strong disagreement and 7 indicating strong agreement. The points between 2 and 6 can be chosen depending on the quality of reporting and its completeness. After rating the items, the score of each domain should be calculated independently. This is done by the summation of each item’s score in the domain and then calculating the total by scaling the domain’s score as percentage of the maximum possible score. The formula for calculating the scaled score is as follows:
Obtained score – Minimum possible score/Maximum possible score – Minimum possible score.
No specific score is defined as a minimum score by the AGREE II consortium. Thus, determining whether a CPG is of high or low quality is the decision of the user of the instrument. Consequently, for this review, a quality score threshold was selected considering all six domain scores to be 60% and above based on consensus among the authors. Therefore, high-quality guidelines will be those in which all domains score 60% or more.Citation10
Data Synthesis
We used descriptive statistics with mean (SD), median, and range for each domain score, calculated using Microsoft Excel (2016).Citation30
Results
Selection of CPGs
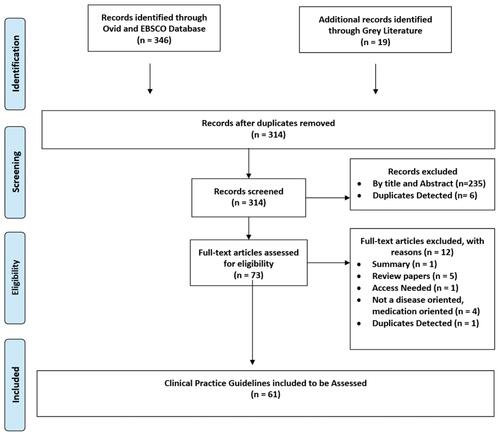
Following the authors’ systematic search strategy, a total of 346 records were identified in the previously described databases, with an additional 19 papers identified through the gray literature search. After removing duplicates, the number of guidelines was 314, of which 235 were found to be irrelevant after screening by title and abstract, and 6 were excluded as duplicates. Therefore, 73 guidelines were considered for full-text screening, and 12 of these were excluded for different reasons mentioned in the flow chart (). The final number of included guidelines was 61.
Figure 1 Flow diagram of the selection process of CPGs.
Clinical Practice Guidelines Characteristics
The description of the general characteristics of the assessed guidelines including the date and origin is illustrated in (). Among the 61 selected CPGs, 34 guidelines were from Saudi Arabia,Citation31–Citation64 12 were from multiple MENA countries,Citation65–Citation76 eight were from Lebanon,Citation77–Citation84 three were from Bahrain,Citation85–Citation87 and one was from each of the following countries: Iran,Citation88 Egypt,Citation89 and Jordan.Citation90
Table 2 Characteristics of CPGs
AGREE II Appraisal Results
The main domains that had higher scores were clarity of presentation (mean 82%, range 39–100%) and scope and purpose (mean 63%, range 3–100%); meanwhile, domains with the lowest scores were rigor of development (mean 28%, range 0–71%), applicability (mean 29%, range 0–75%), stakeholders’ involvement (mean 53%, range 14–97%), and editorial independence (mean 59%, range 0–100%).
Out of the 61 guidelines, 58 (95%) guidelines scored >60% in the clarity of presentation domain, whereas only 5 (8%) and 7 (11.5%) scored >60% in applicability and rigor of development, respectively. The summary statistics for CPG quality assessment are presented in . The detailed assessment is presented in Appendix 3.
Table 3 Summary of the Domain Scores of CPGs Using the AGREE II Instrument (N = 61)
Discussion
This study was performed to examine the quality of CPGs in the MENA region using the AGREE II Instrument. In this review, a total of 61 guidelines were suitable for inclusion, and their quality varied. Among the six domains of the AGREE II Instrument, CPGs scored the highest on clarity of presentation (mean 82%), while the lowest score was granted to the rigor of development domain (mean 28%).
Our results were consistent with those of similar reviews assessing CPGs in Turkey, Sri Lanka, and China.Citation7–Citation9 The similarities were that the lowest scores were attributed to the rigor of development and applicability domains, whereas the highest scores were attained in the clarity of presentation followed by the scope and purpose domain. As opposed to the findings of Hu et alCitation9, editorial independence, which includes the role of funding bodies and potential conflicts of interest, was sufficiently reported in 50% of the included guidelines. This indicates the transparency of the guideline development process in the MENA region.
The impact of economic status on clinical practice and research has been widely investigated.Citation91–Citation93 Few systematic reviews have been conducted to compare and identify the gaps in several guidelines in low-income and middle-income countries compared with high-income countries.Citation94–Citation96 Since some of the MENA countries are classified as low-income and middle-income, as described in the data of the World Bank, the results of such research can be taken into consideration.Citation28 Results from those reviews found several factors in the CPGs of low- and middle-income countries that had an impact on their quality and resulted in less clear and applicable guidelines.Citation28,Citation95 These factors can be broadly classified into evidence-related and contextual-related.Citation97,Citation98 Regarding evidence-related factors, the ability to search and critique clinical evidence is limited in developing countries.Citation97,Citation98 Moreover, Baradaran-Seyed et al state that despite the awareness of health-research priorities and needs, using existing knowledge from daily practice to inform larger clinical studies is suboptimal.Citation97 Additionally, Owolabi et al found that there is a lack of compliance with the trustworthiness standards as defined in the Institute of medicine for guideline development.Citation95 One of the quality assessment items within the rigor of development domain was procedure for updating.Citation10 Some reviews showed that most of these guidelines were outdated, older than 5 years, which is an issue since medical knowledge is evolving and many updates occur regularly.Citation28,Citation95
Contextual-related factors mainly affect the applicability of guidelines.Citation10 Healthcare policies and economic and contextual factors vary among different countries of the MENA region.Citation99 For example, the access and efficient utilization of primary healthcare services in the region is suboptimal.Citation100 In addition, despite the global reduction of communicable disease and the increasing rate of non-communicable diseases, some countries in the MENA region, such as Egypt and Morocco, have an increasing trend for both types.Citation99 Workforce in the region is a major concern, and the number of physicians per 1000 people is lower than expected for middle-income countries such as Yemen, Morocco, the West Bank and Gaza, and Iraq. This factor is also superimposed with a lack of training and professional development, especially in rural regions.Citation101 Finally, out-of-pocket expenditures account for 74% of private health expenditures, a factor that negatively affects the disadvantaged population. This may explain the reasons behind the poor quality of CPGs in the MENA region, especially in the development and applicability domains.
Strengths and Limitations
To the authors’ knowledge, this is the first review performed on the assessment of the quality of CPGs in the MENA region. The search for clinical practice guidelines extends beyond medical journals, and this breadth enhances the inclusiveness of the search strategy.
A major limitation in this study is that our search strategy excludes non-English language studies, and this exclusion may result in language and publication bias. Moreover, poorly indexed studies and those not indexed in PubMed, EMBASE, databases might be missed. In addition, the included clinical practice guidelines have several weaknesses in their design and reporting that may limit the conclusions of this systematic review. The quality assessment of guidelines was assessed by two appraisers, according to the AGREE II guidance, the preferred number of appraisers is four which increases the reliability.
Finally, we could not access the hard copies published by governmental bodies and ministries of health, this could limit the comprehensiveness of grey literature search.
Implications
Identifying weaknesses and areas for improvement in CPGs of the MENA region can guide policymakers and organizations, such as the ministries of health, to implement several strategies to develop high-quality CPGs.
First, a guideline development group should consist of a multidisciplinary team including clinicians, epidemiologists and statisticians, policymakers, and patients’ advocates. These members need to receive special training in the development process for guidelines, which includes but is not limited to effective searching in medical databases, critical appraisal, and utilization of The Grading of Recommendations Assessment, Development, and Evaluation (GRADE tool).Citation102
In addition, the strengthening of collaboration between clinicians, researchers, professional societies, and stakeholders in the MENA region is urgently needed.Citation103 This can be achieved by inviting clinicians and researchers to join guideline development groups, thereby creating a healthy environment where local and international experts meet and share their experience. The involvement of patients and the general public is important in the guideline development phase as it enhances the shared decision-making process and thus improves patient outcomes.Citation104,Citation105 Despite the importance of such involvement, studies have reported suboptimal engagement. Therefore, effective utilization of patient support groups and health charity associations as a potential source for targeted patients is warranted. Tackling these issues could potentially enhance the quality of local guidelines and thus increase their implementation and potential impact.
Conclusion
From this review, it was found that the number of retrieved guidelines published in the MENA region is limited considering the large geographical area of the MENA region. The main domains with higher quality scores were clarity of presentation and scope and purpose, whereas domains with the lowest scores were rigor of development and applicability. The authors’ findings will help policymakers identify areas for improvement in CPGs, and this identification can lead them to implement strategies such as the training of individuals and the recruitment of international experts to ultimately develop high-quality CPGs.
Disclosure
The authors report no conflicts of interest for this work.
References
- Institute of Medicine. Clinical practice guidelines we can trust [Internet]. Washington, DC: The National Academies Press; 2011. Available from: https://www.nap.edu/catalog/13058/clinical-practice-guidelines-we-can-trust. Accessed December 29, 2020.
- McCormack JP, Loewen P. Adding “value” to clinical practice guidelines. Can Fam Physician. 2007;53(8):1326–1327.
- Kredo T, Bernhardsson S, Machingaidze S, et al. Guide to clinical practice guidelines: the current state of play. Int J Qual Heal Care. 2016;28(1):122–128. doi:10.1093/intqhc/mzv115
- Pincus D, Kuhn JE, Sheth U, et al. A systematic review and appraisal of clinical practice guidelines for musculoskeletal soft tissue injuries and conditions. Am J Sports Med. 2017;45(6):1458–1464. doi:10.1177/0363546516667903
- Woolf SH, Grol R, Hutchinson A, Eccles M, Grimshaw J. Potential benefits, limitations, and harms of clinical guidelines. BMJ. 1999;318(7182):527–530. doi:10.1136/bmj.318.7182.527
- Alonso-Coello P, Irfan A, Solà I, et al. The quality of clinical practice guidelines over the last two decades: a systematic review of guideline appraisal studies. Qual Saf Heal Care. 2010;19(6):e58.
- Yaşar I, Kahveci R, Baydar Artantaş A, et al. Quality assessment of clinical practice guidelines developed by professional societies in Turkey. PLoS One. 2016;11(6):e0156483. doi:10.1371/journal.pone.0156483
- Talagala IA, Samarakoon Y, Senanayake S, Abeysena C. Sri Lankan clinical practice guidelines: a methodological quality assessment utilizing the AGREE II instrument. J Eval Clin Pract. 2019;25(4):630–636. doi:10.1111/jep.13048
- Hu J, Chen R, Wu S, et al. The quality of clinical practice guidelines in China: a systematic assessment. J Eval Clin Pract. 2013;19(5):961–967. doi:10.1111/j.1365-2753.2012.01893.x
- Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. Cmaj. 2010;182(18):E839–42. doi:10.1503/cmaj.090449
- Shallwani SM, King J, Thomas R, et al. Methodological quality of clinical practice guidelines with physical activity recommendations for people diagnosed with cancer: a systematic critical appraisal using the AGREE II tool. PLoS One. 2019;14(4):e0214846. doi:10.1371/journal.pone.0214846
- Hou XF, Li M, He W, et al. Quality assessment of kidney cancer clinical practice guidelines using AGREE II instrument: a critical review. Med (United States). 2019;98(40):e17132.
- Bragge P, Guy S, Boulet M, Ghafoori E, Goodwin D, Wright B. A systematic review of the content and quality of clinical practice guidelines for management of the neurogenic bladder following spinal cord injury. Spinal Cord. 2019;57(7):540–549. doi:10.1038/s41393-019-0278-0
- Bhatt M, Nahari A, Wang P-W, et al. The quality of clinical practice guidelines for management of pediatric type 2 diabetes mellitus: a systematic review using the AGREE II instrument. Syst Rev. 2018;7(1):193. doi:10.1186/s13643-018-0843-1
- Hayawi LM, Graham ID, Tugwell P, Abdelrazeq SY, Williams BO. Screening for osteoporosis: a systematic assessment of the quality and content of clinical practice guidelines, using the AGREE II instrument and the IOM standards for trustworthy guidelines. PLoS One. 2018;13(12):e0208251. doi:10.1371/journal.pone.0208251
- Wang Y, Li H, Wei H, et al. Assessment of the quality and content of clinical practice guidelines for post-stroke rehabilitation of aphasia. Medicine (Baltimore). 2019;98(31):e16629. doi:10.1097/MD.0000000000016629
- Barth JH, Misra S, Aakre KM, et al. Why are clinical practice guidelines not followed? Clin Chem Lab Med. 2015;54(7):1133–1139.
- Brouwers MC, Florez ID, McNair SA, Vella ET, Yao X. Clinical practice guidelines: tools to support high quality patient care. Semin Nucl Med. 2019;49(2):145–152. doi:10.1053/j.semnuclmed.2018.11.001
- Eady EA, Layton AM, Sprakel J, Arents BWM, Fedorowicz Z, van Zuuren EJ. AGREE II assessments of recent acne treatment guidelines: how well do they reveal trustworthiness as defined by the U.S. Institute of Medicine criteria? Br J Dermatol. 2017;177(6):1716–1725. doi:10.1111/bjd.15777
- Duarte-García A, Cavalcante M, Arabelovic S, Wong JB. Systematic appraisal of the American College of Rheumatology Clinical Practice Guidelines. ACR Open Rheumatol. 2019;1(3):188–193. doi:10.1002/acr2.1027
- Nelson AE, Allen KD, Golightly YM, Goode AP, Jordan JM. A systematic review of recommendations and guidelines for the management of osteoarthritis: the chronic osteoarthritis management initiative of the U.S. Bone and Joint Initiative. Semin Arthritis Rheum. 2014;43(6):701–712. doi:10.1016/j.semarthrit.2013.11.012
- Werner RN, Marinovic B, Rosumeck S, et al. The quality of European dermatological guidelines: critical appraisal of the quality of EDF guidelines using the AGREE II instrument. J Eur Acad Dermatol Venereol. 2016;30(3):395–403. doi:10.1111/jdv.13358
- Jarl G, Hellstrand Tang U, Nordén E, Johannesson A, Rusaw DF. Nordic clinical guidelines for orthotic treatment of osteoarthritis of the knee: a systematic review using the AGREE II instrument. Prosthet Orthot Int. 2019;43(5):556–563. doi:10.1177/0309364619857854
- Gamst-Jensen H, Vedel PN, Lindberg-Larsen VO, Egerod I. Acute pain management in burn patients: appraisal and thematic analysis of four clinical guidelines. Burns. 2014;40(8):1463–1469. doi:10.1016/j.burns.2014.08.020
- Ou Y, Goldberg I, Migdal C, Lee PP. A critical appraisal and comparison of the quality and recommendations of glaucoma clinical practice guidelines. Ophthalmology. 2011;118(6):1017–1023. doi:10.1016/j.ophtha.2011.03.038
- Eldin C, Raffetin A, Bouiller K, et al. Review of European and American guidelines for the diagnosis of Lyme borreliosis. Med Mal Infect. 2019;49(2):121–132. doi:10.1016/j.medmal.2018.11.011
- The World Bank. Middle East and North Africa [Internet]; 2020. Available from: https://www.worldbank.org/en/region/mena. Accessed December 29, 2020.
- World Bank Country and Lending Groups; 2020. Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups. Accessed December 29, 2020.
- Jabbour S. Public health in the Arab World: at a crossroads. J Public Health Policy. 2013;34(2):356–360. doi:10.1057/jphp.2013.2
- Microsoft Corporation. Microsoft excel [Internet]; 2020. Available from: https://www.microsoft.com/ar-ww/microsoft-365?rtc=1. Accessed December 29, 2020.
- Jazieh A, Alghamdi M, Alghanem S, et al. Saudi lung cancer prevention and screening guidelines. Ann Thorac Med. 2018;13(4):198–204. doi:10.4103/atm.ATM_147_18
- Al Amro SA, Al Aql F, Al Hajar S, et al. Practical guidelines for screening and treatment of retinopathy of prematurity in Saudi Arabia. Saudi J Ophthalmol. 2018;32(3):222–226. doi:10.1016/j.sjopt.2018.07.007
- Al-Hameed FM, Al-Dorzi HM, Abdelaal MA, et al. The Saudi clinical practice guideline for the prophylaxis of venous thromboembolism in medical and critically ill patients. Saudi Med J. 2016;37(11):1279. doi:10.15537/smj.2016.11.15268
- Alfadda AA, Al-Dhwayan MM, Alharbi AA, et al. The Saudi clinical practice guideline for the management of overweight and obesity in adults. Saudi Med J. 2016;37(10):1151. doi:10.15537/smj.2016.10.14353
- Alotaibi M, Saadeddin A, Bazarbashi S, et al. Saudi Oncology Society and Saudi Urology Association combined clinical management guidelines for testicular germ cell tumors. Urol Ann. 2016;8(2).
- Al-Moamary MS, Alhaider SA, Idrees MM, et al. The Saudi Initiative for Asthma-2016 update: guidelines for the diagnosis and management of asthma in adults and children. Ann Thorac Med. 2016;11(1):3. doi:10.4103/1817-1737.173196
- Al-Salam Z, Al-Alaiyan S, Alallah J, et al. The golden hour approach: practical guidelines of the Saudi neonatology society on managing very low birth weight infants in the first hour of life. J Clin Neonatol. 2016;5(4):222. doi:10.4103/2249-4847.194178
- Al-Mandeel HM, Sagr E, Sait K, et al. Clinical practice guidelines on the screening and treatment of precancerous lesions for cervical cancer prevention in Saudi Arabia. Ann Saudi Med. 2016;36(5):313–320. doi:10.5144/0256-4947.2016.313
- Alsanea N, Almadi MA, Abduljabbar AS, et al. National guidelines for colorectal cancer screening in Saudi Arabia with strength of recommendations and quality of evidence: tripartite task force from Saudi Society of Colon & Rectal Surgery, Saudi Gastroenterology Association and Saudi Oncology Society. Ann Saudi Med. 2015;35(3):189–195. doi:10.5144/0256-4947.2015.189
- Al-Hameed F, Al-Dorzi HM, Al Momen A, et al. Prophylaxis and treatment of venous thromboembolism in patients with cancer: the Saudi clinical practice guideline. Ann Saudi Med. 2015;35(2):95–106. doi:10.5144/0256-4947.2015.95
- Al-Hameed F, Al-Dorzi HM, Shamy A, et al. The Saudi clinical practice guideline for the diagnosis of the first deep venous thrombosis of the lower extremity. Ann Thorac Med. 2015;10(1):3. doi:10.4103/1817-1737.146849
- Al-Saleh Y, Sulimani R, Sabico S, et al. 2015 guidelines for osteoporosis in Saudi Arabia: recommendations from the Saudi Osteoporosis Society. Ann Saudi Med. 2015;35(1):1–12. doi:10.5144/0256-4947.2015.1
- Abusamra A, Murshid E, Kushi H, et al. Saudi oncology society and Saudi urology association combined clinical management guidelines for prostate cancer. Urol Ann. 2016;10(2):138–145.
- Al-Hameed FM, Al-Dorzi HM, Al-Momen AM, et al. The Saudi Clinical Practice Guideline for the treatment of venous thromboembolism: outpatient versus inpatient management. Saudi Med J. 2015;36(8):1004. doi:10.15537/smj.2015.8.12024
- Khan J, Idrees MM. Saudi guidelines on the diagnosis and treatment of pulmonary hypertension: pregnancy in pulmonary hypertension. Ann Thorac Med. 2014;9(Suppl 5):S108. doi:10.4103/1817-1737.134050
- Idrees MM, Saleemi S, Azem MA, et al. Saudi guidelines on the diagnosis and treatment of pulmonary hypertension: 2014 updates. Ann Thorac Med. 2014;9(Suppl 1):S1. doi:10.4103/1817-1737.134006
- Khan JH, Lababidi HMS, Al-Moamary MS, et al. The Saudi guidelines for the diagnosis and management of COPD. Ann Thorac Med. 2014;9(2):55. doi:10.4103/1817-1737.128843
- Abdo AA, Hassanain M, AlJumah A, et al. Saudi guidelines for the diagnosis and management of hepatocellular carcinoma: technical review and practice guidelines: created and endorsed by the Saudi Association for the Study of Liver Diseases and Transplantation and the Saudi Oncology Society. Ann Saudi Med. 2012;32(2):174–199. doi:10.5144/0256-4947.2012.174
- Al Jahdali HH, Baharoon S, Abba AA, et al. Saudi guidelines for testing and treatment of latent tuberculosis infection. Ann Saudi Med. 2010;30(1):38–49. doi:10.4103/0256-4947.59373
- The Saudi Center for Evidence Based Health Care. Clinical practice guideline on the timing of initiation of dialysis. 2015.
- The Saudi Center for Evidence Based Health Care. Clinical practice guideline on prevention of venous thromboembolism in patients with stroke. 2014.
- The Saudi Center for Evidence Based Health Care. Clinical practice guideline on allergic rhinitis in asthma. 2014.
- The Saudi Center for Evidence Based Health Care. Clinical practice guideline on the use of thrombolytic therapy in acute stroke. 2014.
- Alharbi H, Alkhateeb S, Murshid E, et al. Saudi Oncology Society and Saudi Urology Association combined clinical management guidelines for urothelial cell carcinoma of the urinary bladder 2017. Urol Ann. 2018;10(2):133. doi:10.4103/UA.UA_176_17
- The Saudi Center for Evidence Based Health Care. Clinical practice guideline on the role of vitamin D, calcium and exercise in fracture prevention in elderly. 2014.
- The Saudi Center for Evidence Based Health Care. Clinical practice guideline on antithrombotic treatment of patients with non-valvular atrial fibrillation. 2014.
- The Saudi Center for Evidence Based Health Care. Clinical practice guideline on the treatment of venous thromboembolism. 2014.
- The Saudi Center for Evidence Based Health Care. Clinical practice guideline on the use of screening strategies for the detection of breast cancer. 2014.
- Alsharm A, Bazarbashi S, Alghamdi A, et al. Saudi Oncology Society and Saudi Urology Association combined clinical management guidelines for renal cell carcinoma 2017. Urol Ann. 2018;10(2):123. doi:10.4103/UA.UA_175_17
- Jazieh AR, Al Kattan K, Bamousa A, et al. Saudi lung cancer management guidelines 2017. Ann Thorac Med. 2017;12(4):221. doi:10.4103/atm.ATM_92_17
- Al-Hameed FM, Al-Dorzi HM, Abdelaal MA, et al. The saudi clinical practice guideline for the prophylaxis of venous thromboembolism in long-distance travelers. Saudi Med J. 2017;38(1):101–107. doi:10.15537/smj.2017.1.15738
- Al-Jahdali H, Alshimemeri A, Mobeireek A, et al. The Saudi Thoracic Society guidelines for diagnosis and management of noncystic fibrosis bronchiectasis. Ann Thorac Med. 2017;12(3):135. doi:10.4103/atm.ATM_171_17
- Bashiri FA, Hamad MH, Amer YS, et al. Management of convulsive status epilepticus in children: an adapted clinical practice guideline for pediatricians in Saudi Arabia. Neurosciences. 2017;22(2):146. doi:10.17712/nsj.2017.2.20170093
- Al-Jazairi A, Al-Jaser R, Al-Halees Z, et al. Guidelines for the secondary prevention of rheumatic heart disease: endorsed by Saudi Pediatric Infectious Diseases Society (SPIDS). Int J Pediatr Adolesc Med. 2017;4(1):47–50. doi:10.1016/j.ijpam.2017.02.002
- Abulkhair O, Saghir N, Sedky L, et al. Modification and implementation of NCCN guidelinesTM on breast cancer in the Middle East and North Africa region. J Natl Compr Cancer Netw. 2010;8(Suppl_3):S–8.
- Bazarbachi A, Azim HA, Alizadeh H, et al. Modification and implementation of NCCN guidelinesTM on lymphomas in the Middle East and North Africa Region. J Natl Compr Cancer Netw. 2010;8(Suppl_3):S–29.
- Okasha A, Alkhadhari S, Al Sharqi A, et al. Arab treatment guidelines for the management of major depressive disorder. Arab J Psychiatry. 2017;44(5487):1–21.
- Jassim NA, Adib G, Rahman YAA, et al. Pan Arab Osteoporosis Society guidelines for osteoporosis management. Mediterr J Rheumatol. 2017;28(1):27.
- İçli F, Akbulut H, Bazarbashi S, et al. Modification and implementation of NCCN guidelinesTM on colon cancer in the Middle East and North Africa Region. J Natl Compr Cancer Netw. 2010;8(Suppl_3):S–22.
- Hassen WA, Karsan FA, Abbas F, et al. Modification and implementation of NCCN guidelinesTM on prostate cancer in the Middle East and North Africa Region. J Natl Compr Cancer Netw. 2010;8(Suppl_3):S–26.
- Yusuf MA, Kapoor VK, Kamel RR, et al. Modification and implementation of NCCN guidelinesTM on hepatobiliary cancers in the Middle East and North Africa Region. J Natl Compr Cancer Netw. 2010;8(Suppl_3):S–36.
- Bohlega S, Alsaadi T, Amir A, et al. Guidelines for the pharmacological treatment of peripheral neuropathic pain: expert panel recommendations for the Middle East region. J Int Med Res. 2010;38(2):295–317. doi:10.1177/147323001003800201
- Al-Abdely HM, Alothman AF, Al Salman J, et al. Clinical practice guidelines for the treatment of invasive Aspergillus infections in adults in the Middle East region: expert panel recommendations. J Infect Public Health. 2014;7(1):20–31. doi:10.1016/j.jiph.2013.08.003
- Alothman AF, Al-Musawi T, Al-Abdely HM, et al. Clinical practice guidelines for the management of invasive Candida infections in adults in the Middle East region: expert panel recommendations. J Infect Public Health. 2014;7(1):6–19. doi:10.1016/j.jiph.2013.08.002
- Alfadhel M, Al Mutairi F, Makhseed N, et al. Guidelines for acute management of hyperammonemia in the Middle East region. Ther Clin Risk Manag. 2016;12:479. doi:10.2147/TCRM.S93144
- Jazieh A-R, Bamefleh H, Demirkazik A, et al. Modification and implementation of NCCN guidelinesTM on non–small cell lung cancer in the Middle East and North Africa Region. J Natl Compr Cancer Netw. 2010;8(Suppl_3):S–16.
- Husni R, Atoui R, Choucair J, et al. The Lebanese Society of Infectious Diseases and Clinical Microbiology: guidelines for the treatment of urinary tract infections. Leban Med J. 2017;103(5521):1–12.
- Moghnieh R, Sakr NY, Kanj SS, Musharrafieh U, Husni R. The Lebanese Society for Infectious Diseases and Clinical Microbiology (LSIDCM) guidelines for adult community-acquired pneumonia (CAP) in Lebanon. Leban Med J. 2014;103(1006):1–8.
- Shatila AR, Koussa S, Jabbour R, et al. LSN MS guidelines for the management of multiple sclerosis. Rev Neurol (Paris). 2013;169(12):950–955. doi:10.1016/j.neurol.2012.12.002
- Ministry of public health. National guidelines for tuberculosis prevention, care and elimination in Lebanon. 2017.
- Ziadé N, Menassa J, Saliba G, Baraliakos X, Ramiro S, Chatzidionysiou K Protocol for prescription and follow up of biologics and targeted synthetic disease modifying anti-rheumatic drugs (b/tsDMARDS) in the management of chronic inflammatory rheumatic diseases (RA, axSpA, PsA). 2018.
- Mokhbat JE. National Guidelines for diagnosis and management of HIV infected adults. Antiretroviral Ther Manag. 2012.
- Fuleihan GEH. FRAX based Lebanese osteoporosis guidelines [Internet]; 2013. Available from: https://www.moph.gov.lb/userfiles/files/Quality%26Safety/OsteoporosisAssessment%26Treatment/FRAX-guidelines.pdf. Accessed December 29, 2020.
- Ministry of Health Kingdom of Bahrain. Guideline on Middle East respiratory syndrome coronavirus (MERS-CoV). 2014.
- Ministry of Health Kingdom of Bahrain. Guideline for management of suspected or confirmed cholera. 2015.
- Ministry of Health Kingdom of Bahrain. Management of Influenza A (H1N1) and Influenza like Illness (ILI). 2015.
- Alavian SM, Hajarizadeh B, Lankarani KB, et al. Recommendations for the clinical management of hepatitis C in Iran: a consensus-based national guideline. Hepat Mon. 2016;16(8). doi:10.5812/hepatmon.guideline.
- Ibrahim MM. Egyptian hypertension guidelines. Egypt Heart J. 2014;66:79–132.
- Jordanian Osteoporosis Prevention Society. The practical guide for management of osteoporosis. 2016.
- Alemayehu C, Mitchell G, Nikles J. Barriers for conducting clinical trials in developing countries- a systematic review. Int J Equity Health. 2018;17(1):37. doi:10.1186/s12939-018-0748-6
- Mcmichael C, Waters E, Volmink J. Evidence-based public health: what does it offer developing countries? J Public Health (Oxf). 2005;27:215–221. doi:10.1093/pubmed/fdi024
- Røttingen JA, Chamas C, Goyal LC, Harb H, Lagradae L, Mayosi BM. Securing the public good of health research and development for developing countries. Bull World Health Organ. 2012;90(5):398–400. doi:10.2471/BLT.12.105460
- Owolabi M, Olowoyo P, Miranda J, et al. Gaps in hypertension guidelines in low- and middle-income versus high-income countries: a systematic review. Hypertension. 2016;68(6):1328–1337. doi:10.1161/HYPERTENSIONAHA.116.08290
- Owolabi MO, Yaria JO, Daivadanam M, et al. Gaps in guidelines for the management of diabetes in low- and middle-income versus high-income countries—a systematic review. Diabetes Care. 2018;41(5):1097–1105. doi:10.2337/dc17-1795
- Bayona H, Owolabi M, Feng W, et al. A systematic comparison of key features of ischemic stroke prevention guidelines in low- and middle-income vs. high-income countries. J Neurol Sci. 2017;375:360–366. doi:10.1016/j.jns.2017.02.040
- Baradaran-Seyed Z, Nedjat S, Yazdizadeh B, Nedjat S, Majdzadeh R. Barriers of clinical practice guidelines development and implementation in developing countries: a case study in Iran. Int J Prev Med. 2013;4(3):340–348.
- Dizon JM, Grimmer K, Louw Q, Machingaidze S, Parker H, Pillen H. Barriers and enablers for the development and implementation of allied health clinical practice guidelines in South African primary healthcare settings: a qualitative study. Heal Res Policy Syst. 2017;15(1):79. doi:10.1186/s12961-017-0243-3
- Mate K, Bryan C, Deen N, McCall J. Review of health systems of the Middle East and North Africa Region. Int Encycl Public Health. 2017;347–356.
- Fadlallah R, Bou-Karroum L, El-Jardali F, et al. Quality, safety and performance management in primary health care: from scoping review to research priority setting and implementation plan in the Eastern Mediterranean Region. BMJ Global Health. 2020;4:e001477. doi:10.1136/bmjgh-2019-001477
- Pierre-Louis AM, Akala FA, Karam HS. Public Health in the Middle East and North Africa: Meeting the Challenges of the Twenty-First Century. World Bank; 2004.
- GRADE HOME; 2020. Available from: https://www.gradeworkinggroup.org/. Accessed December 29, 2020.
- El-Jardali F, Lavis JN, Ataya N, Jamal D. Use of health systems and policy research evidence in the health policymaking in eastern Mediterranean countries: views and practices of researchers. Implement Sci. 2012;7:2. doi:10.1186/1748-5908-7-2
- Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4(4):CD001431. doi:10.1002/14651858.CD001431.pub5
- Hack TF, Degner LF, Watson P, Sinha L. Do patients benefit from participating in medical decision making? Longitudinal follow-up of women with breast cancer. Psychooncology. 2006;15(1):9–19. doi:10.1002/pon.907
- Boivin A, Légaré F, Gagnon MP. Competing norms: Canadian rural family physicians’ perceptions of clinical practice guidelines and shared decision-making. J Heal Serv Res Policy. 2008;13(2):79–84. doi:10.1258/jhsrp.2007.007052
- Schünemann HJ, Fretheim A, Oxman AD. Improving the use of research evidence in guideline development 10. Integrating values and consumer involvement. Heal Res Policy Syst. 2006;5(4):22. doi:10.1186/1478-4505-4-22
- Haddad N, Kanj SS, Awad LS, Abdallah DI, Moghnieh RA. The 2018 Lebanese Society of Infectious Diseases and Clinical Microbiology Guidelines for the use of antimicrobial therapy in complicated intra-abdominal infections in the era of antimicrobial resistance. BMC Infect Dis. 2019;19(1):293. doi:10.1186/s12879-019-3829-2
- World Bank Country and Lending Groups [Internet]; 2020. Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups. Accessed December 29, 2020.
- Bazarbashi S, Alkhateeb S, Abusamra A, et al. Saudi Oncology Society and Saudi Urology Association combined clinical management guidelines for renal cell carcinoma. Urol Ann. 2014;6(4):286. doi:10.4103/0974-7796.140974
- Saudi Ministry of Health (MOH). Clinical practice guideline on the diagnosis of suspected first deep vein thrombosis of lower extremity: Saudi Center for Evidence based Healthcare. 2014.