Abstract
Background
An intoed gait pattern is one of the most common referrals for children to an orthopedic consultation. Parental concern as to the aesthetics of the child’s gait pattern and/or its symptomatic nature will primarily drive these referrals during a child’s early developmental years. Whilst some of these referrals prove to be the result of a normal growth variant, some children will present with a symptomatic intoed gait pattern. Various treatments, both conservative and surgical, have been proposed including: braces, wedges, stretches and exercises, shoe modifications, and surgical procedures. However, which treatments are effective and justified in the management of this condition is not clear within the literature. The aim of this systematic review was to therefore identify and critique the best available evidence for the non-surgical management of an intoed gait pattern in a pediatric population.
Method
A systematic review was conducted of which only experimental studies investigating a management option for an intoeing gait pattern were included. Studies needed to be written in English, pertaining to a human pediatric population, and published within a peer reviewed journal. Electronic databases were searched: Ovid (Medline), EMBASE, AMED, PubMed, SportDiscus, CINAHL, and Cochrane Library. The National Health and Medical Research Council’s designation of levels of hierarchy and the Critical Appraisal Skills Programme cohort studies critical appraisal tool were used.
Results
Five level IV studies were found. The studies were of varied quality and with mixed results. Gait plates, physiologic/standardized shoes, and orthotic devices (with gate plate extension) were shown to produce a statistically significant improvement to an intoed gait pattern. Shoe wedges, torqheels, and a leather counter splint were not able to reduce an intoed gait pattern.
Conclusion
There is limited evidence to inform the non-surgical management of a pediatric intoed gait pattern. The body of evidence that does exist is small (n = 5) and of varied quality, which means recommendations arising from this evidence base should be interpreted with caution. There is generally weak evidence that suggests that gait plates and orthotic devices with a gait plate extension may assist in the management of a pediatric intoed gait pattern.
Background
Intoeing or “pigeon toed” is a gait pattern in which the feet, and in fact the entire leg, will point towards each other instead of functioning in a parallel alignment during ambulation. This intoed gait pattern is one of the most common referrals made to a pediatric orthopedic specialist.Citation1–Citation6 Parental concern as to the aesthetics of the child’s gait pattern will primarily drive these referrals.Citation3–Citation5,Citation7–Citation11 Whilst some of these referrals will prove to be the result of a normal growth variant,Citation2,Citation9,Citation14–Citation19 some children will present with a symptomatic intoed gait pattern. Symptoms commonly reported include frequently tripping, clumsiness during physical activities, and fatigue like pains.Citation3,Citation7,Citation13,Citation18,Citation19 Parents may also be concerned with the possibility of any long term effects on their child’s development. The long term ramifications of this gait pattern cited within the literature include patella-femoral pathology, abnormal subtalar joint pronation, hip joint arthrosis, and patella instability.Citation20
There are a collection of recognized pathologies, structural and/or postural positions that can lead to an intoed gait pattern. These include metatarsus adductus, excessive femoral antetorsion, medial tibial torsion, medial genicular bias, cerebral palsy, and weak and/or dominated lateral hip rotators.Citation4,Citation5,Citation8,Citation9,Citation14–Citation16,Citation21–Citation26 An intoed gait pattern therefore is truly the overall result of one of these underlying pathologies. It would stand to reason then, that an effective and targeted management plan requires the accurate diagnosis of one of these underlying pathologies.
Primarily the diagnosis of an intoed gait pattern is simply made by a clinical gait analysis. The degree of intoeing or outtoeing can be determined using the Foot Progression Angle (FPA).Citation2,Citation3,Citation7,Citation17,Citation24,Citation27–Citation31 This angle is formed by the line of progression (direction of gait) and the bisection of the person’s foot print. The foot bisection line used to calculate the FPA varies greatly within the literature.Citation27 Albeit only one pilot study, Milliron and colleagues, concluded that the center of the second toe be used as the anterior mark for the foot bisection line in FPA measurements. This method produced the lowest standard deviation and lowest variation values (4.47 ± 5.95), when compared to three other bisection methods (intermetatarsal space 1st and 2nd, space 2nd and 3rd, and center of the 3rd toe print).Citation27
The normal FPA ranges for children through to adults are reported to be within −3° and +20°(a minus sign denoting an intoed gait pattern).Citation30 A measurement in excess of 2 SDs (standard deviations) is said to be indicative of an abnormal FPA.Citation3,Citation7,Citation29 Whilst a measurement outside these values should suggest an abnormal gait pattern, there is no indication as to what degree of intoeing would constitute a pathological outcome. Thus the question of whether “to treat, or not to treat?” is still a pertinent question for a clinician when treating a pediatric patient, especially in the absence of pain.Citation7,Citation14,Citation32 Simply put, if a child presents to a clinician with an intoed gait pattern with no pain, should this condition be treated?
There are a plethora of treatments, both conservative and surgical, that have been proposed within the literature to be effective for the management of an intoed gait pattern; including braces, wedges, stretches and exercises, shoe modifications, and various surgical osteotomies.Citation2–Citation15,Citation22–Citation26,Citation31 However, when a clinician is presented with a concerned parent and an intoed child, there are currently no best evidence based management strategies available. In the absence of established best evidence based practice, the provision of both safe and quality health care cannot be assured. The aim of this systematic review was to therefore identify and critique the best available evidence for the non- surgical management of an intoed gait pattern in a pediatric population.
Methods
Search strategy
A systematic search using the following search terms was conducted by one of the authors (HU): Intoe*, toe-in, toeing in, in-toe*, pigeon toe*, p*ediatric* within the following electronic databases from inception to August 2011: Ovid ((Medline) 1950 to August 2011), EMBASE (1996 to August 2011), AMED (1985 to August 2011), PubMed, SportDiscus, CINAHL, and Cochrane Library. “Pearling” of the retained reference lists was also conducted in an effort to identify any articles that may have been missed from the above search strategy.
Inclusion/exclusion criteria
Studies needed to be of experimental design, written in English, pertaining to a human pediatric population (<18 years of age), and published within a peer review journal. The population needed to be a pediatric population with no neurological or systemic pathologies (such as cerebral palsy) with an intoed gait pattern. Studies needed to implicitly state that the objective of their study was to manage an intoed gait pattern with a non-surgical method. All potential search “hits” were screened by both authors (HU and SK) for relevance to this review.
Data extraction
Data extraction was conducted by both authors (HU and SK) first independently with the results then compiled cohesively. Data collected was inclusive of the key characteristics of the studies (including: number of participants, population characteristics, treatment modality), outcome measures used, and the results as reported by the studies.
Methodological quality assessment
The assignment of the level of evidence of the retained studies was completed by both the authors (HU and SK) independently, with the results then compiled. The National Health and Medical Research Council’s designation of levels of evidence was used to assign the articles.Citation33 The Critical Appraisal Skills Programme critical appraisal tool, which was publicly available and widely used in systematic reviews, was used to objectively appraise the retained articles.Citation34 The tool contains twelve questions based around the following three overarching themes: are the results of the study valid?, what are the results?, and will the results help me locally? A response of “yes,” “no,” or “can’t tell” is assigned to each question. The first two questions are considered screening questions, whilst the remainders are a mix of closed and open questions. This tool can be freely accessed from the Public Health Resource Unit website.Citation34
Body of evidence
To aid in the interpretation and comprehension of the findings of this review, the National Health and Medical Research Council’s body of evidence framework was used.Citation35 This framework enables evidence based recommendations to be made despite there being a varied body of literature from which the recommendations are being drawn. The framework is composed of five components: evidence base, consistency, clinical impact, generalizability, and applicability of the research. Both authors have experience in successfully using this framework to interpret varied bodies of research.
Results
Search results
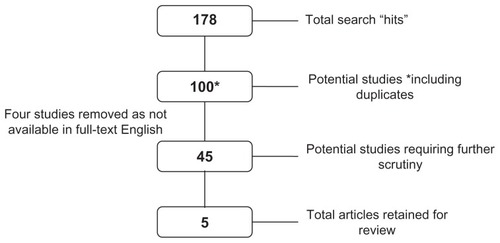
A moderate total of 178 search “hits” were found from running the above search strategy. Of these initial search “hits” only five studies met the inclusion criteria and were retained for this review. No new studies were identified through the “pearling” process. provides an overview of the literature selection process.
Figure 1 Literature selection flow chart.
Characteristics of studies
contains a summary of the study characteristics. These five studies represent the current best available level of evidence in the non-surgical management of an intoed gait pattern in a pediatric population (level IV – case series). Of note, three studies reported specific subject inclusion and exclusion criteria for their cohorts, whilst only two studies further described the presence of the underlying etiologies of their intoeing cohort.Citation3,Citation7,Citation14,Citation20 A total of four different interventions were reported: a flexible leather counter splint, shoe modifications, gait plates, and an orthotic device with a gait plate extension. The descriptions of each treatment method as described within each of the studies are as follows:
Table 1 Summary of study characteristics
Flexible leather counter splint – a leather strap which is attached to the lateral aspect of a pair of shoes and set to varying degrees of external rotation. The splint was attached to any normal, orthopedic, straight-last, prewalker, surgical, or out flare shoe.Citation26 The installation of this device was conducted within the clinician’s office. The use of this device was broadly advocated by Lanier to be for postural driven torsional abnormalities.
Shoe modifications – encompass a series of sole wedges, sole and heel wedges, heel wedges, torqheels (parallel), and torqheels (circular). These modifications were made to a pair of “conventional low cut, properly fitted shoes.”Citation14
Gait plate – constructed from a piece of stiff thermoplastic material which covered the entire length of the plantar surface of the foot, finishing distally at the metatarsophalangeal heads. At the distal lateral edge, the gait plate was extended to the 5th toe and then cut at a 45°angle to sit proximal to the 1st metatarsophalangeal head at the distal medial edge. The gait plate was proposed to “block” propulsion from the lateral side of the device (intoed gait pattern) and promote propulsion from the 1st metatarsophalangeal joint. Gait plates are reported to work best in a soft soled shoe with excessive flexion.Citation7
Orthotic device (with gait plate extension) – a pair of 3 mm polypropylene (semi-rigid) custom foot orthoses produced from a positive cast of the “neutral” subtalar joint position. “An out-toeing wedge consisting of a distal extension of the material of the orthotic device that selectively overshoots the metatarsophalangeal articular line of the external rays and ends in a point in the subdigital space of the fifth toe.”Citation20
Due to the nature of the research design, only a small number of subjects were recruited into three of the five studies: 10, 20, and 20 respectively. Of note, Redmond’s research reported on data collected from the same cohort from the same application of the intervention.Citation3,Citation7 No formal conclusion can be made as to any gender bias within an intoed population from the results of these studies; however, a preliminary trend of more females than males can be seen. The age distribution ranged from <1 year of age to 6.8 years of age.
The FPA outcome measure was used in all of the studies with the exception of the Lanier study which gave no detail as to the outcome measure utilized.Citation26 Only two of the utilized outcome measures have psychometric properties published for their use; the questionnaires used by Redmond and the barefoot FPA method utilized within the Munuera et al report.Citation3,Citation20
Methodological quality assessment
provides a summation of the closed question responses from the Critical Appraisal Skills Programme cohort studies critical appraisal tool. Although this critical appraisal tool does not assign a score, it is evident that the Lanier and Knittle and Staheli studies performed poorly in comparison to the other three studies.Citation3,Citation20 None of the studies had long term follow-up, with most of the studies reporting the immediate effect of the devices being trialled.
Table 2 Critical Appraisal Skills Programme cohort critical appraisal tool
Table 3 Results of the interventions
Results of individual studies
The results as reported by the various authors are displayed in . All of the results were reported quantitatively with the exception of Lanier who reported descriptively. The Lanier study provided very little to no detail as to the treatment method, the assessment procedure, or the outcome measure used. The results were reported as three different categories: “showed improvement,” “either discontinued treatment or were not improved,” and “were lost to follow-up.” The results reported in the category “either discontinued treatment or were not improved” is flawed because each sub-category is distinctly different and not synonymous. The two outcomes represent vastly different results and should not be reported as a singular category.
The use of a gait plate produced a statistically significant improvement to an intoed gait pattern.Citation7 These findings were further supported with a significant improvement noted with the use of both a physiologic shoe and an orthotic device with a gait plate extension.Citation20 However, the use of shoe wedges and circular torqheels was not shown to have a clinically significant effect on the angle of gait of children.Citation14 One study differed from the other four by administering a questionnaire both pre and post intervention.Citation3 Redmond used this questionnaire to assess both parental satisfaction and rates of tripping amongst the participants. A reduction in the rate of tripping and positive parental satisfaction further supports the use of gait plate devices.
Body of evidence matrix
The results of the National Health and Medical Research Council’s body of evidence matrix are presented in . When assessing the current body of evidence for the non-surgical management of an intoed gait pattern, derived from the four components of evidence, it is recommended that these intervention strategies be applied with caution. The current evidence is low level (case studies) and limited (only five studies), of questionable methodological quality, and has issues with generalizability and consistency. The results from these research initiatives however provide emerging evidence which can be used to inform future research directions.
Table 4 Body of evidence matrix
Discussion
Despite intoeing being a commonly seen clinical problem, there is a significant gap on “what works” for this population. Therefore, the aim of this systematic review was to identify and critique the best available evidence for the non-surgical management of an intoed gait pattern in a pediatric population. The literature searching identified only five case studies to inform this systematic review.Citation3,Citation7,Citation14,Citation20,Citation26 Despite the limited body of research evidence, which poses unique challenges for health care professionals who routinely encounter this problem, the findings from this review provide opportunities for reflection. While recognizing its limitations, both in terms of quantity and quality, there is an emerging body of evidence which weakly supports the use of gait plates and orthotic devices with a gait plate extension in the management of a pediatric intoed gait pattern.
Overall, the methodological quality of the included studies was poor. Many studies failed to account for selection bias, measurement bias, confounders, and loss to follow-up. The study by Redmond was an exception among this cohort of studies, controlling for selection and measurement bias but failing to control confounders.Citation3 Selection of participants in these research initiatives was poorly reported by the majority of the studies (four out of five). The study by Munuera and colleagues was the exception which clearly defined an inclusion and exclusion criteria.Citation20 Whilst Munuera and colleagues did not have a minimum level of intoeing required, they did exclude children with motor alterations or serious deformities of the lower limb that would affect gait, a history of surgical management of the lower limb, or children presenting requiring surgical management.
As previously acknowledged, intoeing is the resultant gait pattern caused by the presence of a number of different underlying pathologies, be they structural or postural. Two studies described the presence of the underlying pathologies within their cohort of children but did not complete any sub-group analysis.Citation7,Citation14 It is a significant design flaw that these sub-group analyses have not been acknowledged and systematically accounted for in the results. An adequate clinical assessment of an intoed gait pattern should include an extensive assessment as to what underlying pathology is driving this resultant gait pattern. Without this accurate diagnosis, a targeted management plan cannot be implemented. The absence of these sub-group analyses greatly reduces the application of these results to the clinical population.
Measurement bias was poorly controlled within the five studies reviewed. All of the FPA measurements were collected with a mixture of both barefoot and shod conditions and by using different footprint bisection lines. The results within the studies of both before and after the intervention and between the studies are not wholly comparable with the differing barefoot and shod conditions. As previously stated, Milliron and colleagues demonstrated with their pilot study that a footprint (barefoot) bisection line through the middle of the second toe was the most reliable point for measurement.Citation27 This point of bisection was not used consistently within the five studies reviewed. The lack of measurement consistency both within and between the studies once again reduces the relevance of these results to the clinical population.
The only study to utilize an outcome measure other than the FPA was Redmond.Citation3 The questionnaires initiated at pre and post intervention demonstrated both parental satisfaction and a reduction in the rate of tripping amongst the intoeing cohort. Investigating parental satisfaction is a significant inclusion as parental concern as to the aesthetics of the child’s gait pattern will primarily drive these referrals.Citation3–Citation5,Citation7–Citation11 Although the results as a whole have been clouded by the aforementioned measurement biases, the results from the Redmond study show promising trends for the use of gait plates, both for the parent and the child.Citation3
Limitations of this review
The very nature of a systematic review ensures a very specific, targeted body of literature is identified, accessed, evaluated, and synthesized. As the review only included published, English language literature, the potential for publication and language bias should be acknowledged. While the authors made all attempts to identify and access all relevant studies, it is possible, due to differing terminologies, and access to databases and journals, some may have been missed. Finally, this review is based on a small body of evidence (five studies) which were underpinned by several methodological flaws. While the number and quality of primary research is beyond the authors’ control, it must be acknowledged when considering the findings from this review.
Conclusion
Implications for clinical practice
There is a lack of published high level, methodologically sound evidence for the non-surgical management of a pediatric intoed gait pattern. The body of evidence that does exist is small (n = 5) and of varied quality. There is generally weak evidence that suggests that gait plates and orthotic devices with a gait plate extension may assist in the management of a pediatric intoed gait pattern. However, due to concerns with the methodological quality of the evidence base, this recommendation must be applied with caution. Intoeing may be the resultant gait pattern from the presence of one or multiple underlying pathologies. Although the current evidence base is flawed in not considering the assessment and/or sub-group analysis of any of these pathologies, good clinical practice should not exclude a thorough clinical assessment for the diagnosis of one of these underlying pathologies.
Due to this limited and weak evidence base, clinical practice continues to be guided by clinician’s expertize and experiential knowledge. It is imperative that interpretation and implementation of these findings in clinical practice is underpinned by clinical reasoning and regular monitoring of patient outcomes.
Implications for future research
Future research needs to specifically address the underlying pathologies driving the intoed gait pattern, for without this consideration the results are neither specific nor applicable to current clinical practice. Future research should endeavor to use well described samples with adequate sample size, robust methodological design to control for bias, and outcome measures with strong psychometric properties with data collected over a long period of time.
Disclosure
The authors report no conflicts of interest in this work.
References
- MolonyDHeffermanGDoddsMMcCormackDNormal variants in the paediatric orthopaedic populationIr Med J2006991131416506683
- BriggsRGCarlsonWOThe management of intoeing: a reviewS D J Med199043213162406900
- RedmondACThe effectiveness of gait plates in controlling in- toeing symptoms in young childrenJ Am Podiatr Med Assoc2000902707610697970
- RyanDJIntoeing. A developmental normOrthop Nurs2001202131812024629
- MaloneMRotational deformities of the lower limb in children – a primary cause of intoeingPodiatry Now200710102936
- KillamPEOrthopedic assessment of young children: developmental variationsNurse Pract198914727362664594
- RedmondACAn evaluation of the use of gait plate inlays in the short-term management of the intoeing childFoot Ankle Int19981931441489542984
- LiYHLeongJCIntoeing gait in childrenHong Kong Med J19995436036610870163
- WilliamsPFIntoeing in ChildrenMed J Aust1960472161913844916
- SharrardWJIntoeing and flat feetBr Med J1976160148888891260395
- GulanGMatovinovićDNemecBRubinićDRavlić-GulanJFemoral neck anteversion: values, development, measurement, common problemsColl Antropol200024252152711216420
- SvenningsonSTerjesenTApalsetKAndaSOsteotomy for femoral anteversion: A prospective 9-year study of 52 childrenActa Orthop Scand19906143603632402992
- PayneLZDeLucaPAIntertrochanteric versus supracondylar osteotomy for severe femoral anteversionJ Pediatr Orthop199414139448113370
- KnittleGStaheliLTThe effectiveness of shoe modifications for intoeingOrthop Clin North Am19767410191025980415
- StaheliLTIntoeing in ChildrenPrim Care19785197110247529
- StaheliLTLower positional deformity in infants and children: a reviewJ Pediatr Orthop19901045595632193037
- LöselSBurgess-MillironJMicheliLJEdingtonCJA simplified technique for determining foot progression angle in children 4 to 16 years of ageJ Pediatr Orthop19961655705748865038
- MatovinovićDNemecBGulanGŠestanBRavlić-GulanJComparison in regression of femoral neck anteversion in children with normal, intoeing and outtoeing gait – prospective studyColl Antropol19982225255329887609
- SvenningsonSApalsetKTerjesenTAndaSRegression of femoral anteversion: A prospective study of intoeing childrenActa Orthop Scand19896021701732728876
- MunueraPVCastilloJMDominguezGLafuenteGOrthotic devices with out-toeing wedge as treatment for in-toes gait in childrenJ Am Podiatr Med Assoc2010100647247821084533
- FabryGChengLXMolenaersGNormal and abnormal torsional development in childrenClin Orthop Relat Res199430222268168306
- KarolLARotational deformities in the lower extremitiesCurr Opin Pediatr19979177809088759
- RosmanMAIntoeing. Easing parents’ concernsPatient Care19872112173179
- StrickerSJSamaAAAssessment of angulation and torsion of lower limbs in childrenInt Pediatr2001163138143
- ScherlSACommon lower extremity problems in childrenPediatr Rev2004252526114754927
- LanierJCThe intoeing child. Treament with a simple orthopedic applianceJ Fla Med Assoc1971581219235121861
- MillironMLoeselSMicheliLEdingtonCComparison of methods for calculation of foot progression angleJ Am Coll Sports Med1992245S173
- YngveDAFoot-progression angle in clubfeetJ Pediatr Orthop19901044674722358483
- StaheliLTReport of the Pediatric Orthopaedic Society (POS) Subcommittee on Torsional DeformityOrthop Trans198046465
- StaheliLTCorbettMWyssCKingHLower-extremity rotational problems in children. Normal values to guide managementJ Bone Joint Surg Am198567139473968103
- SassPHassanGLower extremity abnormalities in childrenAm Fam Physician200368346146812924829
- EvansAMThe flat-footed child – to treat or not to treat: what is the clinician to do?J Am Podiatr Med Assoc200898538639318820042
- National Health and Medical Research Council (NHMRC)A guide to the development, implementation and evaluation of clinical practice guidelines1998Australia Available from: http://www.nhmrc.gov.au/_files_nhmrc/file/publications/synopses/cp30.pdfAccessed December 19, 2011
- The Critical Appraisal Skills ProgrammeCohort Studies Critical Appraisal Tool2004Oxford Available from: http://www.phru.nhs.uk/Doc_Links/cohort%2012%20questions.pdfAccessed December 19, 2011
- NHMRC levels of evidence and grades for recommendations for developers of guidelines2009Australia Available from: http://www.nhmrc.gov.au/_files_nhmrc/file/guidelines/evidence_statement_form.pdfAccessed December 19, 2011