
Abstract
Introduction
COVID-19 is a current health concern in the world. People applying the prevention methods of COVID-19 are vital determinants of curbing the spread of the coronavirus. This study aimed to assess the practices and associated factors of the COVID-19 preventive measures among Dire Dawa residents.
Methods
A community-based, cross-sectional mixed method was used. We conducted the study between June 15th and July 15th, 2020. The subjects of the study were selected by using systematic random sampling. We collected data through face-to-face and in-depth interviews. Both bivariate and multiple logistic regression were employed to determine the predictor variables with the practice of COVID-19 prevention measures. Thematic content analysis analyzed qualitative data.
Results
The practice of COVID-19 preventive measures was 40.7% (95% CI: 37–44.4%). Being female [AOR= 1.8; 95% CI: 1.17–2.72], married [AOR=2.75; 95% CI: 1.68–4.48], family income >10,000 Ethiopia birr [AOR=7.3; 95% CI: 3.8–13.9], having history of a chronic disease [AOR=3.46 (1.69, 7.08)], not chewing khat [AOR= 2.15; 95% CI: 1.1–4.2], had a good knowledge about COVID-19 [AOR=5.23; 95% CI: 3–9], and had a favorable attitude about COVID-19 [AOR=3.87; 95% CI: 2.4–6.14] were significantly associated with practice of COVID-19 preventive measures. The qualitative result revealed the communities are not willingly practicing prevention measures because of carelessness and ignorant of the consequences of COVID-19, and some communities believed that COVID-19 is not a real pandemic rather government uses it merely to gain political profit.
Conclusion
The proportion of practice of COVID-19 preventive measures was low. Sex, marital status, income, history of chronic disease, history of khat chewing, knowledge, and attitude about COVID-19 were associated factors with COVID-19 preventive practices. The communities were not practicing the COVID-19 prevention method because of poor knowledge and a negative attitude.
Introduction
The novel coronavirus COVID-19 outbreak was declared as a global public health problem for the sixth time in history.Citation1 Globally on January 15, 2021, 93,536,554 coronavirus cases and 2,002,465 deaths, and in Ethiopia 129,922 cases and 2008 deaths were reported.Citation2 COVID-19 is transmitted through contact between humans mainly through droplets of an infected person during coughing, sneezing, or speaking, and as well infected by touching of contaminated surface, and then touching eyes, nose, or mouth without washing hands.Citation3 COVID-19 is often more severe in people aged 60+years, with respiratory or heart disease, diabetes, a condition that leads to immune-compromised, and infants. The clinical manifestation of COVID-19 includes coughing, sneezing, febrile to touch, headache, and difficulty of breathing, within 2–14 days of incubation period.Citation4,Citation5
WHO recommended COVID-19 prevention measures such as hand washing, wearing a face mask, keeping distance, make the room ventilated, avoid going to a crowded area, and covering nose and mouth during coughing or sneezing, avoiding close contact with animals and suspected area with coronavirus infections, and avoiding the consumption and handling of raw meat to prevent cross-contamination.Citation6,Citation7
Many countries have planned to decrease or prevent the spread of the virus. The plan aimed to reduce and end the transmission, avert outbreaks and give optimized care for every infected person, also critical sick; ease the impact of COVID-19 on the health care system, social services, and financial activities.Citation8 An international experts and African governments have articulated their concern regarding the transmission of COVID-19 and predicted that over 2 million deaths might happen in sub-Saharan Africa if action is not implemented.Citation9 Ethiopia, the second populated country in Africa, reinforced COVID-19 prevention and methods with the support of WHO and other partners. The country’s health authorities are focusing on surveillance, diagnosis, infection prevention, and control, epidemic response coordination, and community health education to swiftly identify cases and minimize the spread of the disease. The World Health Organization considered Ethiopia as the highest priority, along with 13 African countries for COVID-19 preparedness because of its continued flight to China.Citation10
Experts believed the pandemic can affect seriously African countries because of the weak health care system, crowded situations, poor sanitation in the cities, and the random movement of people can make the outbreak out of control.Citation11,Citation12 The restriction of travel because of COVID-19 also significantly influenced the economy and interrupt the efforts towards achieving sustainable development goals (SDGs) in SSA, including Ethiopia that depends on foreign aid.Citation13 In Ethiopia, with the poor public health systems, deprived public health sectors, and an insufficient number of specialized hospitals, there is little capacity for tracing, testing, confirmation, isolation, and treatment of those infected. By taking experience from previously affected countries, the preparedness, and the current Intensive Care Unit hospitalization capacities in Africa pales compared to the oncoming infections.Citation14
The World Health Organization identified community transmission in several African countries, including Ethiopia, March 2020, and the rate of spread of the virus is rising for lack of practicing and implementing the principle of social distance, unable to frequent hand washing, unable to stay at home, and the pandemic itself its different symptom of COVID-19 across individual and unclear and contradicting (eg WHO) information about the case among countries and scientist and other factors make pandemic the challenge of controlling and preventing.Citation15
Ethiopia similar to other developed countries had its own emergency practice project guideline intended for COVID-19-virus. The aim of developing the guideline is to strengthen the government’s capacity to prepare and respond to the COVID-19 outbreak.Citation16 Nowadays, no any recommended treatments or vaccines for COVID-19. Studies are limited to this issue in the current study area. Hence, this study aimed to determine the practice of COVID-19 preventive measures and associated factors among Dire Dawa City residents.
Materials and Methods
Study Area and Period
We conducted this study from Jun 15th to July 15th, 2020, in Dire Dawa City, found 515 km away from Addis Ababa to the East. The total number of population in the city is estimated to be 408,096 (according to the UN population estimates of major urban agglomerations in 2020). The city has nine Kebeles (administrative districts).
Study Design and Population
A cross-sectional community-based research design comprising both quantitative and qualitative approach was employed. The population of the study was all permanent residents of the city.
For qualitative: Participants of the study were volunteer groups, police officers, health bureau officials, and other stakeholders.
Sample Size and Sampling Technique
To calculate sample size, 50% of the proportion of practice of COVID-19 prevention measure, 95% confidence interval, 0.04 margin of error, and a 10% non-response rate were used. The sample was determined to be 660. Of the nine kebeles (administrative districts) of the city, five kebeles were selected using a simple random sampling method, and then 660 participants, using the sampling frame of households with house representatives, were selected by systematic random sampling technique.
For qualitative data, 16 key informant interviewees were used based on the saturation of data, and the interviewees were purposively selected. They were volunteers working on awareness creation activities, police officers, and health bureau officials”.
Data Collection, Instruments, and Procedures
Questionnaires and semi-structured interviews were used for data collection. We developed the questionnaire based on the literature. It comprises different sections such as sociodemographic characteristics, behavioral characteristics, knowledge, attitude, and practices towards COVID-19 prevention measures.Citation17–Citation19 The questionnaire was prepared in English and then translated to Amharic (the working language of the country), and back to English to check the language consistency of the tool. Eight trained nurses were collected the data, and four trained supervisors supervised the data collection process. The respondents filed the questionnaire in a face-to-face manner: the nurse read each item for the respondents and put their responses accordingly. For the qualitative data, a semi-structured interview guide was used. The researchers themselves conducted the interviews and were tape-recorded.
Data Quality Control
The data quality was assured by pre-testing the data collection tool on 5% (33 respondents) of the sample size in Kebele 03 before the actual data collection, and we incorporated the correction into the tool. The supervisors and investigators checked the collected data for completeness every day. Then, necessary feedback was offered to the data collectors every morning.
Measurement and Definitions
The dependent variable is the practice of COVID-19 prevention (Good/poor). The independent variables included (1) sociodemographic factors: age, sex, monthly household income, marital status, occupation, educational status, family size; (2) personal and behavioral factors: alcohol consumption, cigarette smoking, khat chewing, history of chronic disease, and (3) knowledge and attitude toward COVID-19.
Six questions assessed the practice of COVID-19 prevention measure and each scored 0 and 1 (0 = No, 1 = Yes). Then, those who scored less than the mean points of six questions were measured as they have a poor practice of COVID-19 prevention measure, and those who scored a mean point and above were considered as they have a good practice.
There were about 9 (nine) attitude questions, and each question scored 0 and 1 (0 = No, 1 = Yes). We took those participants who answered less than mean points out of nine questions as have an unfavorable attitude whereas those who answered a mean point and above the mean point as having a favorable attitude.
Also, there were 12 (twelve) knowledge measuring questions, in which each question scored 0 and 1 (0 = No, 1 = Yes). We considered those study participants who scored below the mean value out of twelve questions as they have poor knowledge and those who scored a mean and above the mean value as they have good knowledge.
Data Processing and Analysis
Data were checked for consistency and entered Epi Data version 3.1 and then exported to the statistical package for social sciences (SPSS) version 24.0 software for analysis. Descriptive statistics like frequency, proportion, mean, and standard deviation computed to describe study variables about the population. Both bivariate and multivariate were used to determine the effect of independent variables on the outcome variables. Variables found to have a P-value <0.25 in the bivariate logistic regression entered/exported into multivariate analysis to identify the predictor variables. Hosmer and Lemeshow’s goodness-of-fit test was used to assess whether they fulfilled the assumptions. Finally, the adjusted odds ratio with 95% CI at P-value <0.05 was considered a statistically significant association with the practice of COVID-19 prevention measures. The qualitative data collected was transcribed, reduced, coded, thematized, and analyzed using qualitative content analysis.
Ethical Considerations
Ethical clearance was obtained from the Dire Dawa University research ethics review committee. Then, a support letter with this was offered to Dire Dawa administration Health Bureau, and we got permission from each Kebele’s administrative. Participation of all respondents was voluntary, and we ensured informed written consent before engaging in the study. We took measures to assure the respect, norms, values, beliefs, culture, and freedom of each individual participating in the study. Information on the purpose and procedures of the study was explained; confidentiality was maintained by omitting their identifications such as names and assured a great deal of care and the information obtained is anonymized to all study participants. This study was conducted by the Declaration of Helsinki.
Result
Sociodemographic Characteristics
Six hundred forty-four participants were involved, making the response rate of 97.6%. The mean age of the respondents was 30 (SD= 9.2) years. The majority, 303 (47%) and 312 (48.4%) of the participants were 20–30 years old age and Orthodox followers by religion, respectively. Three-hundred (46.6%) of the respondents were attending secondary education, and two-fifth (40%) was a governmental employee ().
Table 1 Sociodemographic Characteristics of Study Participants in Dire Dawa, Eastern Ethiopia, 2020 (n=644)
Personal and Behavioral Profiles of the Participants
The majority of 515 (80%) the residents had a current history of alcohol drinking without holiday, and 103 (16%) were chewing khat. Only 48 (7.5%), and 80 (12.4%) of the participants were smoked cigarettes, and had a history of chronic disease, respectively.
Knowledge of Participants About COVID-19
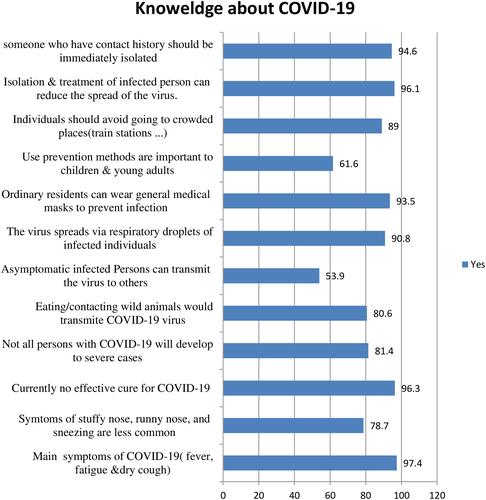
Of the total, 455 (70.7%) (95% CI: 66.3–73.6) of the residents have good knowledge about prevention methods and clinical symptoms of COVID-19. The majority, 620 (96.3%) of the respondents said that currently no effective treatment to cure COVID-19. The majority, 519 (80.6%) and 585 (90.8%) of the respondents were stated as eating or contacting with wild animals are the main source of infection to COVID-19, and respiratory droplets are the main source of COVID-19 transmission, respectively. Most, 619 (96.1%) of the participants believed that the isolation and treatment of an infected person in the place can reduce the spread of the virus ().
Figure 1 Knowledge of participants about COVID-19 in Dire Dawa, Eastern Ethiopia, 2020.
The Attitude of Participants Towards COVID-19
Among the total respondents, 387 (60.1%), (95% CI: 56.2–63.8) of them had a positive attitude about COVID-e majority, 633 (98.3%) and 630 (97.8%) of the study subjects replied that COVID-19 disease is dangerous and stays at home/avoids going to crowded places to prevent the transmission of COVID-19, respectively ().
Table 2 Attitude of Study Participants About COVID-19 Prevention Methods and Clinical Symptoms in Dire Dawa City, Eastern Ethiopia, 2020 (n=644)
The Practice of COVID-19 Prevention Methods
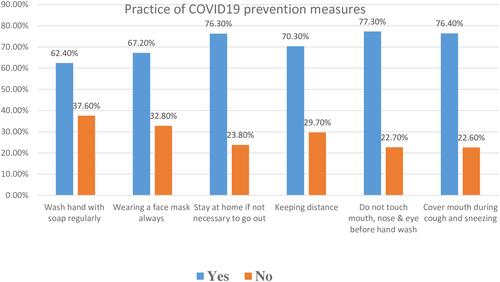
Out of the total respondents, 262 (40.7%), (95% CI: 37–44.4) of the residents had a good practice on prevention methods of COVID-19. Nearly one-third (32.7%), and 29.7% of the respondents were cover their mouth and nose during coughing and sneezing, and keeping their social distance, respectively ().
Figure 2 Practice of COVID-19 prevention measures among participants in Dire Dawa, Eastern.
Associated Factors with Practices of COVID-19 Prevention Measures
Those females were 1.79 [AOR= 1.79 (1.17, 2.72)] times more likely to have a good practice toward COVID-19 prevention as compared to their counterparts. Married respondents were 2.75 [AOR= 2.75 (1.68, 4.48)] times more likely to practice COVID-19 prevention as compared to those currently unmarried. Those who had monthly income greater than 10,000 were 7.33 [AOR= 7.33 (3.84, 13.98)] times more likely to practice COVID-19 prevention as compared to those who had monthly income less than 5000. Respondents who had a chronic disease were 3.46 [AOR = 3.46 (1.69, 7.08)] times more likely to practice COVID-19 prevention as compared to their counterparts. Those who had no chewing habits were 2.15 [AOR= 2.15 (1.09, 4.23)] times more likely to practice COVID-19 prevention as compared to those chewers. Those who had good knowledge about COVID-19 were 5.23 [AOR= 5.23 (3.02, 9.08)] times more likely to have good practice about COVID-19 prevention as compared to their counterparts. Respondents who had a favorable attitude towards COVID-19 were 3.87 [AOR= 3.87 (2.44, 6.14)] times more likely to practice COVID-19 prevention as compared to those who had an unfavorable attitude ().
Table 3 Factors Associated with Practice on COVID-19 Prevention Measures Among Participants in Dire Dawa City, Eastern Ethiopia, 2020 (n=644)
Qualitative Result
Sixteen in-depth interviews were done among selected key informants. We merged the result into four thematic areas. Those are COVID-19 prevention activities in the administration, perception towards COVID-19, COVID-19 prevention practices in Dire Dawa Administration, and measures taken to improve the realization of COVID-19 prevention.
COVID-19 Prevention Activities in the Administration
As of interview participants’ reflection on general knowledge regarding COVID-19 prevention measures, there is no consistency in the prevention activities.
However, according to some administration health bureau participants mentioned some activities considered as good practices and exemplary achievements in the efforts towards preventing the pandemic. For instance, we have observed financial institutions in the administration implementing prevention measures seriously and consistently (e.g. providing water and soap and forcing customers to wash their hands before entering, making wearing a face-mask mandatory).
Perception Towards COVID-19
Regarding attitude towards COVID-19, the interviewees have expressed they do not believe that the administration is not seriously working on the pandemic. They justified that in the early stage of the pandemic, the administration was actively working on it as a campaign. However, as times go, the activities towards prevention and awareness creation have become loose and disorganized.
COVID-19 Prevention Practices in Dire Dawa Administration
It seems the community has an awareness of the pandemic, but they are not practicing the prevention mechanisms. The interviewees unanimously agreed that the prevalence of the pandemic increasing day to day.
An interviewee has said:
As to me, the people are undermining COVID-19, believing that they are safe and will not be infected. This might be because significant death cases are not reported as high as Europeans and/or Americans. Therefore, if I am not pessimistic, it will cost as much in terms of life and finance.
Some people try to abuse them thinking that government and health professionals over-emphasize the pandemic. Here are some to mention.
“When people see me in face-mask, they think as if I am discriminating them, thus they feel doubtful about me.
One more participant has added that “when you tell somebody to wear a face-mask, for instance, he/she doesn’t accept”.
Measures are Taken to Improve the Realization of COVID-19 Prevention
Dire Dawa administration has been taking different measures to tackle the spread of the pandemic among these; the lockdown of public gathering, lockdown of school and market place and awareness creation for the surrounding community particularly on frequent hand washing, physical distancing, and staying at home if it is possible, and different humanitarian activities, have been undertaking to address a vulnerable segment of the community by volunteers in the administration. However, it is observed that negligence on behalf of the community towards effective implementing physical distancing and staying at home.
Discussion
The practice of COVID-19 prevention measures in this finding was 40.7% with 95% CI (36.9, 44.5). The qualitative study finding an interviewee supported this finding has said that as to me the people are undermining COVID-19 believing that they are safe and will not be infected. This might be because significant death cases are not reported as high as Europeans and Americans. This finding was higher than the study done in south Ethiopia, which was 20%.Citation17 This discrepancy might be because in this research all respondents were urban residence was as a study in south Ethiopia more than half of the respondents were rural residence. Since urban residents are near to information regarding COVID-19 and might have adequate knowledge and a positive attitude towards the pandemic that leads to practice COVID-19 prevention.
However, the result was lower than the study done in Indian which was 83.7%.Citation18 This variation maybe because of using different methods of data collection. In our case, we used a direct interview method which includes all populations whereas the study done in India used online data collection which includes only a more educated population. Also, this finding lower than the finding of a study conducted in the Amhara region, Ethiopia which was 62%.Citation26 The justification might be because of the difference in the study population as our study included a community member with different health and educational background, and the study conducted in the Amhara region included only health care worker that they have better, access information, and closely for COVID-19 prevention measures than our study population.
In our study, females were approximately two times more likely to practices COVID-19 prevention methods compared to males. This finding was consistent with a study conducted in Iran.Citation3 This might be because females spent most of their time at home and they are naturally more prone to practice handwashing. Also, mostly females involved in childcare, food preparation, and other tasks as compared with males. So, preventive measures are more likely to be practiced better among females to protect themselves and others from infection.
Married populations were 2.75 times more likely to practices COVID-19 prevention methods as compared to those currently unmarried. A study done in China supported this finding.Citation20 This could be explained that those married are better economically income that leads to afford the COVID-19 prevention types of equipment. Those who had a monthly income of >10,000 ETB were 7.33 times more likely to practice COVID-19 prevention as compared to those who had a monthly income <5000 ETB. This result was consistent with other studies in Malaysia and the United States,Citation19,Citation21 which showed that those populations with low economic status showed poor knowledge of COVID-19 prevention methods. The study in China reported income was statistically significant with the practice of COVID-19 prevention.Citation22 This is because economic status is the main indicator of behavior and actions for maintaining one’s health. This is also supported with the qualitative result, which was the reason for not responding to COVID-19 prevention practice was Economic reasons (not able to afford alcohol, a face-mask, etc., poor socioeconomic status). It implies that low socioeconomic status leads to the difficulty of change one’s behavior or condition, and finally inability of performing recommended protective behaviors of COVID-19.Citation20 Also, an increase in income leads to the possibility of satisfying needs for protecting COVID-19. For example, buying facemask and hand sanitizer is possible when there is adequate income. Individuals with low income will not stay at home, rather prefer to continue their daily activities to satisfy their basic needs during the transmission period.
Those who had good knowledge about COVID-19 were 5.23 times more likely to practice COVID-19 prevention as compared to their counterparts. This finding is consistent with a study in China and Amhara region, Ethiopia.Citation23,Citation26 This might be because knowledge is the main modifier of positive attitudes toward COVID-19 preventive practices, and these activities are practiced after having awareness and knowledge of activities to be performed. Knowledge of COVID-19 decreases the risk of infection by improving patient’s prevention practices. Knowledge about coronavirus disease (COVID-19) sign and symptoms, transmission, treatment, and how to prevent infection will increase the prevention practice of individuals and they might be implemented the key messages of the guideline include causes, how to choose and wear face masks, proper handwashing habits, preventive measures at different locations (eg, at home, on public transportation, and in public space), disinfection methods, and medical observation at home.Citation3
Respondents who had a favorable attitude towards COVID-19 prevention were 3.87 times more likely to practice COVID-19 prevention as compared to those who had an unfavorable attitude. This finding is supported by a study conducted in China.Citation24 This might be because having a positive attitude leads to more awareness of prevention measures of COVID-19 and leads to more practices.
Those participants who had the chronic disease were 3.46 times more practice COVID-19 prevention methods as compared to those who had no chronic disease. This finding was consistent with a study conducted in southern Ethiopia, the Amhara region in Ethiopia, and Thailand.Citation17,Citation25,Citation26 The justification might be those having chronic diseases have a chance of caring for themselves regularly because they are close with a health professional to care for themselves.
Those who had no chewing habits were 2.15 times more likely to practice COVID-19 prevention as compared to those chewers. This might be because that khat chewer is more likely going out home to buy khat, group chewing that leads less likely of applying keeping distance. This study has some strengths and limitations. As a strength, our study used both quantitative and qualitative data methods were employed. It was conducted during a critical period, few months of the COVID-19 outbreak in Ethiopia, and it included community populations with different sociodemographic characteristics to assess their practices toward COVID-19 prevention measures. However, as a limitation, it did not include rural areas around Dire Dawa City. Since it is a cross-sectional study, it does not show a cause–effect relationship.
Conclusion
The practice of preventive measures of the coronavirus was low. Factors such as sex, marital status, monthly family income, history of chronic disease, history of khat chewing, knowledge, and attitude about COVID-19 were predictors of the practice of COVID-19 prevention methods. We recommend the government, concerned stakeholders, and media to work continuously on the spread of COVID-19 to increases the knowledge and attitude of the societies which ultimately results in better preventive practices toward COVID-19. Further, still the governments of Africa and WHO to emphasize preparedness for the practices of COVID-19 prevention measures for Africa.
Abbreviations
nCoV, novel coronavirus; COVID-19, coronavirus disease 2019; WHO, World Health Organization.
Data Sharing Statement
All related data are presented within the paper, and its supporting information file.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Acknowledgment
First, our thanks go to Dire Dawa University Research and Technology Interchange, College of Medicine and Health Sciences, and all respective Health Bureau, and kebeles management body for their support and providing information. Our thanks are also to all data collectors and supervisors for their valuable contribution during the data collection. Last, we would like to thank the study participants.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
- Meo S, Alhowikan A, Al-Khlaiwi T, et al. Novel coronavirus 2019-nCoV: prevalence, biological and clinical characteristics comparison with SARS-CoV and MERS-CoV. Eur Rev Med Pharmacol Sci. 2020;24(4):2012–2019. doi:10.26355/eurrev_202002_20379
- Worldometers. COVID-19 Coronavirus pandemic; 2021. Avalable from: https://www.worldometers.info/coronavirus/?. Accessed January 15, 2021.
- Adhikari SP, Meng S, Wu Y-J, et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infect Dis Poverty. 2020;9(1):1–12. doi:10.1186/s40249-020-00646-x
- Zhu H, Guo Q, Li M, et al. Host and infectivity prediction of Wuhan 2019 novel coronavirus using a deep learning algorithm. BioRxiv. 2020.
- COVID, Coronavirus. Global Cases by Johns Hopkins CSSE. Johns Hopkins University (JHU); 2020.
- World Health Organization. Coronavirus disease (COVID-19) advice for the public; 2020. Avalable from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public. Accessed January 23, 2021
- Brown A, Horton R. A planetary health perspective on COVID-19: a call for papers. Lancet. 2020;395(10230):1099. doi:10.1016/S0140-6736(20)30742-X
- World Health Organization. Coronavirus disease 2019 (COVID-19): situation report, 82. Avalable from: https://scholar.google.com/scholar?hl=en≈sdt=0%2C5&q=world+report+COVID19&btnG. Accessed January 23, 2021.
- Walker PG, Whittaker C, Watson OJ, et al. The impact of COVID-19 and strategies for mitigation and suppression in low-and middle-income countries. Science. 2020;eabc0035. doi:10.1126/science.abc0035
- Gilbert M, Pullano G, Pinotti F, et al. Preparedness and vulnerability of African countries against importations of COVID-19: a modeling study. Lancet. 2020;395(10227):871–877. doi:10.1016/S0140-6736(20)30411-6
- Maclean R Africa braces for coronavirus, but slowly. The New York Times; 2020. Avalable from: https://scholar.google.com/scholar?hl=en≈sdt=0%2C5&q=11.%09Maclean+R.+Africa+braces+for+coronavirus%2C+but+slowly.+The+New+York+Times.+2020.+&btnG=. Accessed January 23, 2021.
- Jump up to a b c d “African Countries respond quickly to spread of COVID-19”. Avalable from: NPR.org. Accessed January 23, 2021.
- World Health Organization. Barriers to rapid containment of the Ebola outbreak. Emergencies preparedness response; 2014. Available from: https://www.who.int/csr/disease/ebola/overview-august-2014/en/. Accessed January 23, 2021.
- Mehari TM Africa versus Coronavirus: four much-needed capabilities. Aljazeera center for studies; 2020. Avalable from: https://studies.aljazeera.net/en/reports/africa-versus-coronavirus-four-much-needed-capabilities. Accessed January 23, 2021.
- World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19–11 March 2020. Avalable from: https://scholar.google.com/scholar?hl=en≈sdt=0%2C5&q=WHO+Director-General%27s+opening+remarks+at+the+media+briefing+on+COVID-19+-+11+March+2020&btnG=. Accessed January 23, 2021.
- Üstün TB, Chatterji S, Kostanjsek N, et al. Developing the World Health Organization disability assessment schedule 2.0. Bull World Health Organ. 2010;88:815–823. doi:10.2471/BLT.09.067231
- Mola S, Aweke Z, Jemal B, et al. Magnitude and associated factors for attitude and practice of Southern Ethiopian residents toward COVID-19 and its preventions: a community-based cross-sectional study. 2020. doi:10.21203/rs.3.rs-36120/v1
- Tomar BS, Singh P, Nathiya D, et al. Indian communities knowledge, attitude & practice towards COVID-19. medRxiv. 2020. doi:10.1101/2020.05.05.20092122
- Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes, and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. doi:10.1371/journal.pone.0233668
- Braveman PA, Cubbin C, Egerter S, Williams DR, Pamuk E. Socioeconomic disparities in health in the United States: what the patterns tell us. Am J Public Health. 2010;100(S1):S186–S196. doi:10.2105/AJPH.2009.166082
- Wolf MS, Serper M, Opsasnick L, et al. Awareness, attitudes, and actions related to COVID-19 among adults with chronic conditions at the onset of the US outbreak: a cross-sectional survey. Ann Intern Med. 2020;173:100–109. doi:10.7326/M20-1239
- Mantwill S, Monestel-Uma S, Schulz PJ. The relationship between health literacy and health disparities: a systematic review. PLoS One. 2015;10(12):1–22. doi:10.1371/journal.pone.0145455
- Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745. doi:10.7150/ijbs.45221
- Zhong NS, Zheng BJ, Li YM, et al. Epidemiology and cause of severe acute respiratory syndrome (SARS) in Guangdong, People’s Republic of China, in February 2003. Lancet. 2003;362(9393):1353–1358. doi:10.1016/S0140-6736(03)14630-2
- Srichan P, Apidechkul T, Tamornpark R, et al. Knowledge, attitude and preparedness to respond to the 2019 Novel Coronavirus (COVID-19) among the bordered population of Northern Thailand in the early period of the outbreak: a cross-sectional study. SSRN Electron J. 2020. doi:10.2139/ssrn.3546046
- Asemahagn MA. Factors determining the knowledge and prevention practice of healthcare workers towards COVID-19 in Amhara region, Ethiopia: a cross-sectional survey. Trop Med Health. 2020;48(1):1. doi:10.1186/s41182-020-00254-3