Abstract
Carcinoid bronchopulmonary tumors represent approximately 25% of all carcinoid tumors and 1%–2% of all lung neoplasms. The most common symptoms are: persistent cough, asthma-like wheezing, chest pain, dyspnea, hemoptysis and obstructive pneumonitis. We present a case of a young adult diagnosed with a typical carcinoid tumor. The diagnosis was established on the basis of imaging examination and bronchoscopic biopsy. The patient was treated with bronchoscopic electrocautery therapy to relieve the obstructed airway, followed by surgical lobectomy in order to entirely remove the exophytic damage. This approach was not only a palliative management to bronchial obstruction but also avoided pneumonectomy. Recent studies support the use of such interventional resection methods, as they may result in a more conservative surgical resection.
Introduction
Carcinoid tumors develop from stem cells of the bronchial epithelium known as Kulchitsky cells, which have neuroendocrine activity. These neuroendocrine cells can develop tumors in many different organs with most common being the lungs, the appendix, the small intestine (duodenum), the rectum and the pancreas.Citation1 The most recent classification system from the World Health Organisation categorized neuroendocrine pulmonary tumors in four types: typical carcinoid; atypical carcinoid (ATC); large cell neuroendocrine carcinoma; and small cell lung cancer.Citation2
Carcinoid bronchopulmonary tumors represent approximately 25% of all carcinoid tumors and 1%–2% of all lung neoplasms.Citation3 Approximately 70% of these tumors are located centrally in the large bronchial tubes leading to the lung, while 10%–20%, known as peripheral carcinoids, develop in the pulmonary periphery.Citation4
Typical carcinoid pulmonary tumors manifest nine to ten times more often than ATC tumors. They are characterized by slow development and rare metastasis to other organs. Typical carcinoid tumors are seen in younger patients more often than ATCs and appear to be the most frequent pulmonary neoplasms during childhood and puberty.Citation5,Citation6 ATC lung tumors have a more aggressive histologic appearance and a greater tendency to metastasize than typical carcinoid lung tumors. These tumors are more frequent in males, and the average age of onset is 46 years.Citation7
Unlike most lung cancers, the development of carcinoid pulmonary tumors is not related to smoking or other environmental causes (eg, tobacco smoke, air pollution, or asbestos). The detection of carcinoid tumorlets in lung biopsies led to speculation that carcinoid tumors may grow from these cells.Citation1 However, further research needs to be conducted as this association has not been yet determined.
Case report
A 26-year-old female presented with wheezing episodes, cough and mild dyspnea. After a chest x-ray revealed normal findings and spirometry showed mild restriction (), she was commenced on bronchodilators and inhaled corticosteroids. Two years later, the symptoms were not entirely relieved and she had developed hemoptysis of approximately 10 mL/24 hours. Therefore, she was referred to the pulmonary department for further examinations.
Table 1 Spirometries performed pre- (first visit, upon diagnosis) and post-operatively (after treatment)
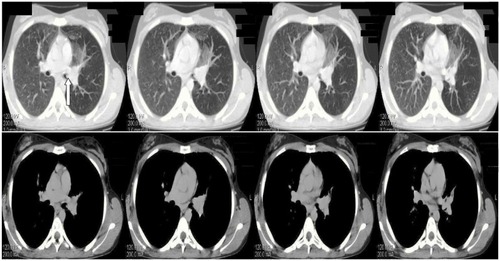
During clinical examination the patient had reduced respiratory whistling and mild wheezing in the upper left pulmonary field. The results of the exams revealed normal blood tests, a mild restrictive spirometry (), a negative Mantoux and a left perihilar shadow in the chest radiograph (). A chest high resolution computed tomography was performed showing a nodule in the left primary bronchus causing its partial obstruction (). The suspicion of malignancy was established and the patient underwent a bronchoscopy (Olympus BF-P240; 6 mm insertion tube, biopsy channel 2.6 mm, 55 cm working length, [Olympus Corp, Tokyo, Japan]). The findings showed exophytic damage with increased vascularization in the left primary bronchus 5 cm from the carina. This picture was compatible with a carcinoid tumor. The tumor was biopsied and the specimen was sent for histological examination. The biopsy demonstrated a typical carcinoid and the patient underwent pelvic and cerebral computed tomography, which both showed normal findings.
Figure 1 Chest radiographs: (A and B) before treatment with arrow showing a left perihilar shadow, (C) After treatment (surgery) arrow indicates (D) staples on 5-year follow up.
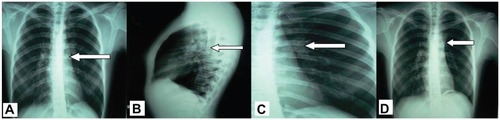
Figure 2 Chest HRCT showing nodule development in the left primary bronchus causing its partial obstruction (arrow) before treatment.
In an effort to avoid pneumonectomy, and to produce rapid palliation of hemoptysis and immediate tumor debulking, bronchoscopic electrocautery was selected as the most appropriate procedure.
A rigid bronchoscopy was inserted into the trachea under general anesthesia using a 7.5 mm Storz rigid bronchoscope (Karl Storz Gmbh and Co, Tuttlingen, Germany). Electrocautery (power setting of 40 Watts, blend mode, normal coagulation, electrosurgical monopolar unit PSD-20, with foot switch, flexible monopolar electrocautery blunt probe Olympus CD-6C-1, loop snare, [Olympus, Tokyo, Japan]) was performed on the exophytic tumor tissue followed by mechanical removal. This intervention fully re-opened the obstructed left main bronchus and the upper subsegment of the left upper lobe. The remaining tissue in the obstructed lower subsegment of the left upper lobe was treated by surgical resection, performing a lobectomy to remove the tissue entirely. During this procedure, three lymph nodes (subsegmental and segmental) were also removed. The final report stated that there was no expanding malignancy affecting the pleural cavity or the lymph nodes.
The patient was not given chemotherapy but was followed up with regular medical monitoring combined with imaging studies (ie, chest x-ray, chest computed tomography). Five years after surgical treatment, the patient was asymptomatic with normal chest radiographs and normal spirometry (; ).
Discussion
About 25% of patients with carcinoid lung tumors are asymptomatic. Citation8 The severity and variety of symptoms depend on the size of the carcinoid pulmonary tumor and the production of hormones. In symptomatic patients with central carcinoids, the most common symptoms are: persistent cough, asthma-like wheezing, chest pain, dyspnea, hemoptysis and obstructive pneumonitis.Citation9 A number of studies have reported that a mistaken diagnosis of asthma is frequent in these cases, delaying early diagnosis. Peripheral carcinoid tumors rarely manifest any symptoms.
Occasionally, carcinoid pulmonary tumors may initiate an excessive hormonal secretion causing various neuroendocrine syndromes such as carcinoid syndrome and Cushing syndrome.Citation9,Citation10 The most common symptoms of carcinoid syndrome are: facial flushing, sweating, diarrhea, rapid cardiac beats and wheezing. Even more rarely, patients with Cushing syndrome caused by the abnormal overproduction of cortisol can develop muscle weakness, obesity in the upper body, high blood pressure, high blood sugar and increased body and facial hair.
Almost 90% of typical carcinoid tumors are diagnosed at an early stage while more than 50% of ATC tumors are diagnosed at stage II or III.Citation11 The diagnosis of carcinoid pulmonary tumor is established on the basis of the patient’s symptoms combined with imaging examination such as chest radiography, computed tomography and magnetic resonance imaging.Citation12 To verify the histologic type of the pulmonary tumor detected, there are several biopsy options including bronchoscopic biopsy, needle biopsies and surgical biopsies (eg, thoracotomy).Citation13 However, it has been reported that bronchoscopic biopsy has a risk of hemorrhage, especially in cases of partial or total removal of vascular tumors.Citation14
The primary and most effective treatment for all pulmonary carcinoid tumors is surgical resection as long as no contraindications to surgery exist (eg, widespread metastatic disease).Citation15 Chemotherapy and radiotherapy have no therapeutic contribution and there is no verified optimal therapy for unresectable carcinoid lung tumors.Citation16
There are a variety of resection techniques that treat lung carcinoids effectively.Citation13 Presently, the most commonly utilized resection procedure is lobectomy. For smaller tumors located in the periphery or within a pulmonary segment, surgeons may perform segmental resection or wedge resection. Sleeve resection is usually performed for central lesions. In rare cases, a bilobectomy or pneumonectomy may be required due to the size or the location of the tumor. Postoperatively, the most common complications are excessive bleeding, atelectasis and prolonged air leak.Citation13
Interventional therapeutic bronchoscopies such as laser bronchoscopy, electrocautery therapy, cryotherapy, endobronchial brachytherapy, photodynamic therapy and airway stents may also be performed in certain cases.Citation17,Citation18 Nd-YAG lasers and electrocautery, together with mechanical tumor removal, are more appropriate for rapid palliation and immediate tumor debulking.Citation19 In particular, electrocautery therapy, as applied in our case, can achieve immediate relief of the symptoms resulting from obstructed airways in 55%–75% of patients. Its advantages over laser treatment include cost effectiveness, higher availability, and faster removal of tumors and components resistant to laser coagulation. Citation18 Moreover, in a study evaluating the degree of damage and bronchial wall healing after photodynamic, Nd-YAG laser, and electrocautery therapy, electrocautery produced the least amount of airway scarring and subepithelial fibrosis.Citation19 In another study, the amount of mucosal damage visualized after electrocautery was correlated with histologic tissue damage. The investigators concluded that this is a potential advantage of electrocautery compared to other therapies, where the real histologic damage may be more severe than what is visualized after the therapy.Citation20 Side effects of electrocautery therapy include burn, haemorrhage, and inadvertent electrical shock to the endoscopist or the patient, but there are no reports of treatment-related deaths or respiratory failure episodes.Citation18,Citation21
These bronchoscopic techniques are usually used for palliative management of bronchial obstruction, for mass reduction prior to surgery, or for patients unsuitable for formal surgery.Citation18 A number of studies of endobronchial resection have confirmed that bronchoscopic techniques are successful modalities of treatment.Citation22 Several therapeutic modalities used in conjunction may be essential to achieve the best management of the disease, rather than a single invasive approach.Citation23 In a recent review, even though 50% of patients underwent a lung resection after a single bronchoscopic resection, the authors reported that the inability to remove the remaining tumor was entirely due to the inaccessibility of the tumor.Citation24–Citation26 Some experts believe that tumor reduction by this method may result in a more conservative surgical resection.Citation15 Our study confirms these findings as the use of bronchoscopic electrocautery followed by surgical lobectomy not only removed the tumor entirely but also avoided pneumonectomy.
Among pulmonary malignancies, carcinoid tumors have the highest prognostic rates. Typical carcinoid tumors have better prognoses than the atypical forms. The 5-year survival rate reaches 92%–100% for typical lung carcinoids and only 61%–88% for ATCs.Citation27 Previous studies have shown that lymph node involvement as well as the presence of tumorlets, have significant negative effects on prognoses.Citation28
Early suspicion, combined with imaging examination and biopsy, is the key to diagnosis. Improved surgical techniques allow smaller incisions resulting in shorter hospitalization and less postoperative pain.Citation19 Many studies suggest that the use of endobronchial management techniques not only improve clinical symptoms and quality of life, but also increase overall survival.Citation21,Citation23 Therefore, performing less invasive procedures should be considered throughout the management of lung cancer patients, provided no poor prognostic factors exist.Citation29 Series utilizing this mode of therapy must be reported in order to determine long-term outcomes.
A carcinoid tumor may be considered a challenging disease due to its infrequency. It is very important that scientists continue to investigate and publish results from such cases so that new information about the etiology and treatment of the disease can be made available.
Disclosures
The authors declare no conflicts of interest in this work. Written informed consent for publication of this case report and all accompanying images was obtained from the patient upon discharge.
References
- VuitchFSekidoYFongKMackayBMinnaJDGazdarAFNeuroendocrine tumors of the lung: pathology and molecular biologyChest Surg Clin North Am1997712147
- World Health OrganizationClassification of Tumors Pathology and Genetics Tumors of the Lung, Pleura and HeartLyon, FranceIARC Press2004
- AsamuraHKameyaTMatsunoYNeuroendocrine neoplasms of the lung: a prognostic spectrumJ Clin Oncol2006241707616382115
- Rosado de ChristensonMLAbbottGFKirejczykWMGalvinJRTravisWDThoracic carcinoids: radiologic-pathologic correlationRadiographics199919370773610336200
- GroteTHMaconWRDavisBGrecoFAJohnsonDHAtypical carcinoid of the lung: a distinct clinicopathologic entityChest19889323703752827965
- WangLTWilkinsEWJrBodeHHBronchial carcinoid tumors in pediatric patientsChest19931035142614288387419
- ValliMFabrisGADewarAHornallDSheppardMNAtypical carcinoid tumour of the lung: a study of 33 cases with prognostic featuresHistopathology19942443633698045525
- DucrocqXThomasPMassardGOperative risk and prognostic factors of typical bronchial carcinoid tumorsAnn Thorac Surg1998655141014149594876
- McCaughanBCMartiniNBainsMSBronchial carcinoids. Review of 124 casesJ Thorac Cardiovasc Surg19858918172981373
- IliasITorpyDJPacakKMullenNWesleyRANiemanLKCushing’s syndrome due to ectopic corticotropin secretion: twenty years’ experience at the National Institutes of HealthJ Clin Endocrinol Metab20059084955496215914534
- TravisWDRushWFliederDBSurvival analysis of 200 pulmonary neuroendocrine tumors with clarification of criteria for atypical carcinoid and its separation from typical carcinoidAm J Surg Pathol19982289349449706973
- SoubaniAOThe evaluation and management of the solitary pulmonary nodulePostgrad Med J20088499545946618940947
- PaganaKDPaganaTJMosby’s Manual of Diagnostic and Laboratory Tests4th edSt LouisMosby2010
- MedfordARLElectrocautery, bronchoscopic biopsy and hemorrhageAnn Thorac Med201161484921264177
- DaddiNFerollaPUrbaniMSurgical treatment of neuroendocrine tumors of the lungEur J Cardiothorac Surg200426481381715450578
- ThomasCFJrTazelaarHDJettJRTypical and atypical pulmonary carcinoids: outcome in patients presenting with regional lymph node involvementChest200111941143115011296182
- MachucaTNCardosoPFCamargoSMSurgical treatment of bronchial carcinoid tumors: a single-center experienceLung Cancer201070215816220223552
- PrakashUBAdvances in bronchoscopic proceduresChest199911651403140810559105
- van BoxemAJWestergaJVenmansBJPostmusPESutedjaGPhotodynamic therapy, Nd-YAG laser and electrocautery for treating early-stage intraluminal cancer: which to choose?Lung Cancer12001311313611162864
- van BoxemTJWestergaJVenmansBJPostmusPESutedjaTGTissue effects of bronchoscopic electrocautery: bronchoscopic appearance and histologic changes of bronchial wall after electrocauteryChest2000117388789110713021
- BolligerCTSutedjaTGStrauszJFreitagLTherapeutic bronchoscopy with immediate effect: laser, electrocautery, argon plasma coagulation and stentsEur Respir J20062761258127116772389
- SutedjaTGSchreursAJVanderschuerenRGKwaBvd WerfTSPostmusPEBronchoscopic therapy in patients with intraluminal typical bronchial carcinoidChest199510725565587842794
- ErnstAFeller-KopmanDBeckerHDMehtaACCentral airway obstructionAm J Respir Crit Care Med2004169121278129715187010
- LuckrazHAmerKThomasLGibbsAButchartEGLong-term outcome of bronchoscopically resected endobronchial typical carcinoid tumorsJ Thorac Cardiovasc Surg2006132111311516798310
- DeygasNFroudarakisMOzenneGVergnonJMCryotherapy in early superficial bronchogenic carcinomaChest20011201263111451811
- FroudarakisMFournelPBurgardGBronchial carcinoids. A review of 22 casesOncology19965321531588604242
- Garcia-YusteMMatillaJMCuetoAPaniaguaJMSpanish Multi-centric Study of Neuroendocrine Tumours of the Lung for the Spanish Society of Pneumonology and Thoracic Surgery (EMETNE-SEPAR). Typical and atypical carcinoid tumours: analysis of the experience of the Spanish Multi-centric Study of Neuroendocrine Tumours of the LungEur J Cardiothorac Surg200731219219717196822
- ChughtaiTSMorinJESheinerNMWilsonJAMulderDSBronchial carcinoid-twenty years’ experience defines a selective surgical approachSurgery199712248018089347859
- HerthFJFEndobronchial management of central cancersSpiroSGHuberRMJanesSMThoracic MalignanciesEuropean Respiratory Society Monograph200944336348