Abstract
Background
The aim of this investigation was to analyze temporal changes in anxiety, depression, and stress in patients with musculoskeletal pain for a period of up to 2 years after a multidisciplinary rehabilitation program, in relation to sick-listing (registered with The Swedish Social Insurance Agency [Forsakringskassan] for sickness benefit).
Methods
Ten persons with full-time sick leave (absence from work for medical reasons) (group 1) and 49 with part-time or no sick leave (group 2) at the end of the 2-year study period participated. It was shown in a previous study that group 1 had higher pain rating and higher subjective physical disability than group 2, with little or no improvement during and after rehabilitation. In the present study, all participants were evaluated with the Hospital Anxiety and Depression scale and a self-rated stress test.
Results
Participants with full-time sick leave during the study period (group 1) showed improved stress levels but no change in anxiety and depression levels. Anxiety, depression, and stress changed more favorably in participants with part-time or no sick leave than in those with full-time sick leave.
Conclusion
The results of this study indicate that investigation and appropriate treatment of psychological symptoms, including anxiety and depression, are important in multidisciplinary rehabilitation of patients with musculoskeletal disorders.
Introduction
Depression, pain, and somatic symptoms are common and often occur concomitantly, leading to symptoms that cannot be explained fully by a general medical condition and use of health care.Citation1 It appears that with an increasing degree of pain, the risk of depression increases. On the other hand, symptoms such as pain are commonly associated with depression.Citation2 However, pain is more often considered to lead to depression than the reverse.Citation3
Pain in the lumbar region and the neck may not only reduce functional capacity but may also give rise to worry, anxiety, and depression.Citation4 Impaired mental function may cause difficulties in concentration, fatigue, and pain in muscles and joints, which may lead to a deterioration of movement patterns as well as a restricted capacity for activity.Citation4,Citation5 Cognitive and behavioral factors play a significant role in the transition from acute to chronic pain in the back and neck. Among the most powerful cognitive and behavioral risk factors are pain-related fear, distress, and avoidance of activity.Citation6 Prolonged pain tends to develop into a combination of physical, psychological, and social disabilities.Citation7,Citation8
In recent studies of a group of women and men with musculoskeletal disorders involving mainly neck and back pain, our research group found that most participants improved during a multidisciplinary rehabilitation program. This improvement was reflected in reduced disability and pain rating, and persisted during a follow-up period of 2 years.Citation9 However, it was noted that a small number of participants with higher disability and pain rating at the beginning of the rehabilitation program were sick-listed during the program or for a longer period of up to 2 years after its completion.Citation9
Lundgren and MolanderCitation10 see rehabilitation as a process of constant goal setting, new strategic choices, new measures, and evaluation. They state that the term “multidisciplinary” relates to the areas of knowledge on which the rehabilitation is based, and thus emphasize the aspect of theory. Rehabilitation is a multidisciplinary type of care, because it is based on knowledge generated in many different fields of science. The goal of multidisciplinary rehabilitation programs is that participants are able to learn to find management strategies for their problems and improve their quality of life, and possibly lower their consumption of outpatient treatment and other health care resources. Because there are few studies in this field, there is an urgent need for long-term scientific follow-up regarding the effects of multidisciplinary rehabilitation programs.
The aim of the present study, which was conducted on the same women and men as those who participated in the above-mentioned study,Citation9 was to analyze temporal changes in anxiety, depression, and stress in sick-listed and nonsick-listed persons with musculoskeletal pain during and up to 2 years after a 7-week multidisciplinary rehabilitation program. A further aim was to compare results between full-time sick-listed and part-time or nonsick-listed participants.
Materials and methods
Participants
Sixty-two persons with nonmalignant pain who had been consecutively referred to undergo a 7-week active rehabilitation program in a primary care setting were invited to participate in the study. Sixty persons (40 women, 20 men) who met the inclusion criteria agreed to take part.
The inclusion criteria were: working age, ability to understand and speak Swedish, having neck or back pain, having pain in the locomotor system when performing work tasks, having been accepted for the program by the regional social insurance office and their employer, and having been referred to the program by a doctor. Exclusion criteria were presentation with a serious pathological condition other than a locomotor system disorder and/or not having undergone a complete medical investigation.
The research ethics committee of Mid Sweden University reviewed the study and raised no objections from an ethics point of view. All participants gave their signed informed consent before the start of the study.
At the end of the 2-year study period, a group of 10 full-time sick-listed participants (group 1), for whom data had been gathered earlier and used in a previous study,Citation9 was compared with 49 participants who were part-time or not at all sick-listed (group 2, ). The median age of group 1 was 48.5 years and of group 2 was 48.0 years.
Table 1 Distribution according to gender (n), age (median and percentiles 25–75), civil status, profession, and diagnosis (n) in participants with full-time sickness benefit (group 1) and with part-time or no sickness benefit (group 2) at the end of the follow-up period
Procedure
The multidisciplinary rehabilitation team treating the participants consisted of two registered physiotherapists, two registered nurses, one registered psychologist, one physician, one fitness instructor, and two secretaries.
The participants were recruited by physicians, physiotherapists, and nurses, or from the regional social insurance office or employers. Referral of patients to the regional social insurance office came via general practitioners. A decision about participation was made together with the participant, the regional social insurance office, and possibly the employer. Relevant investigations and treatments had to be completed prior to referral to the program. Information concerning the rehabilitation program was given as part of the physician’s investigation, but information was also sent via post to the participants before the start of the program. The size of the rehabilitation group was a maximum of eight participants per group.
Rehabilitation program
The rehabilitation program was conducted over a period of 7 weeks, on 5 days a week, for 4 hours a day. The participants participated in the rehabilitation program for half days, allowing them to live in their regular home environment. The participants were taught training theory, ergonomics, and strategies for coping with pain and handling of stress. Lifestyle (sleep habits, diet, alcohol, tobacco), working life, and behavioral changes were also discussed. The participants practiced walking with or without a stick, participated in water gymnastics, back gymnastics, and in individual training programs, based on physical tests.Citation11
Individual exercise programs were focused on flexibility of the spine and strengthening of the stabilizing muscle groups. Warm-up exercises and stretching were performed prior to the program. The participants also practiced different relaxation techniques and Qi-gong, as well as body awareness training. They were offered individual counseling by a psychologist throughout the rehabilitation period and, if considered necessary, psychological follow-up after the course.Citation9,Citation11,Citation12
Group sessions were led by different team members, physiotherapists, nurses, a psychologist, and a fitness instructor. The different team members worked together. The participants also had regular once-weekly meetings with the team members during the 7-week rehabilitation program. The participants developed an individual rehabilitation plan at the start of the program. Follow-up was done at the end of the program and on different occasions over a 2-year period.Citation11
Measurement instruments
The study had a nonrandomized, prospective, interventional design. Data were obtained before and after the rehabilitation program and at intervals of 6, 12, and 24 months after completion of the program. All participants were evaluated using the Hospital Anxiety and Depression (HAD) scaleCitation13,Citation14 and a self-rated stress test.Citation15 The participants were not given any information about their scores from previous tests either before or during administration of the questionnaire.
Sick leave data
The level of sick leave was recorded by the participant before and at the end of the rehabilitation program and at intervals of 6, 12, and 24 months after its completion. The Swedish Social Insurance Agency is responsible for a large part of the social security system. This task includes investigating, deciding upon, and paying grants and allowances in the social insurance scheme.Citation16
The most important part of sickness insurance is sickness benefits and the various forms of rehabilitation allowances. A sickness benefit is payable when there is sickness that reduces the work capacity of the insured by at least one quarter. A sickness benefit can be paid at 100%, 75%, 50%, or 25%, depending on the extent of reduction of the work capacity. The alternative sick-leave levels are decided by the Swedish sickness compensation system.Citation16
Hospital Anxiety and Depression scale
The HAD scale consists of 14 items and has two subscales, one for measuring anxiety and the other for measuring depression.Citation13 The scoring system ranges from absence of a symptom or the presence of positive features (scoring 0) to maximal presentation of symptoms or the absence of positive features (scoring 3). Thus, the higher the score, the greater the anxiety and/or depression.Citation13,Citation14 The HAD scale is considered to be a reliable instrument to screen for clinically significant anxiety and depression in patients attending a general medical clinic. The scale has also been shown to be a valid measure of the severity of these mood disorders. The internal consistency of the two subscales was examined by calculating correlations between each item and the total score of the remaining items in the subscales. Correlations for the anxiety items ranged from +0.76 to +0.41 and their level of statistical significance was P < 0.01. The correlations ranged from +0.60 to +0.30 for the depression items and their statistical significance was P < 0.02.Citation13
Stress test
The Everyday Life Stress scale is an instrument for assessing the level of self-rated stress behavior.Citation15 It consists of 20 statements referring to stress behavior in everyday life situations and is based on two major themes, ie, time urgency/impatience and easily aroused irritation/hostility. The score ranges between 0 and 60 points, higher scores indicating more stressful reactions. Internal consistency between the 20 items is high (Cronbach’s alpha 0.90). A five-point difference is of major clinical significance.Citation15
Statistical analysis
The Statistical Package for Social Science version 12.0.1 (SPSS Inc, Chicago, IL) was used for the statistical analysis. The median, percentiles, and percentage rates were calculated for each measurement. Friedman’s one-way analysis of variance, the Mann-Whitney U-test, and the Wilcoxon test were used to test for temporal change and the interaction between full-time sick-listed, part-time, or not at all sick-listed participants. Nonparametric techniques were used for ordinal data and small samples.Citation17 The statistical significance level was set at 5%.
Results
There were no differences in background characteristics (gender, civil status, profession, diagnosis) between the groups (see ). All participants completed the rehabilitation program, with the exception of one woman who did not participate for personal reasons in measurements at the 2-year follow-up, but attended and filled in the questionnaires before and after the rehabilitation program and attended follow-up visits at 6 and 12 months. This woman was included in the study.
Sick leave
Before the rehabilitation program, 30 participants had full-time sick leave and 30 had part-time sick leave or no sick leave at all. At the start of the study, three participants were on a 75% sickness benefit, eight on 50%, two on 25%, and 17 had no sick leave. At 2-year follow-up, 10 participants were on full-time sick leave (group 1), while 49 had part-time sick leave or no sick leave (group 2). Three participants were on 75% sickness benefit, 11 were on 50%, eight were on 25%, and 27 had no sick leave. In group 1, nine were sick-listed full-time during the entire 2-year follow-up period while one participant became sick-listed full time after the measurement at 12 months.
Hospital Anxiety and Depression scores
Participants in group 1 had a lower anxiety score than those in group 2 at the beginning of the study, and experienced no change in anxiety between the start of the program and 2-year follow-up (see ). Group 2 decreased their anxiety score (P < 0.0005) during the 2-year follow-up period (). Group 1 participants had a higher depression score than those in group 2 before the start of the program (). Depression decreased in group 2 (P < 0.01) in contrast to the development in group 1 between the start of the rehabilitation program and the 2-year follow-up ().
Figure 1 Development of the anxiety (HAD) score (y axis) in participants with a full-time sickness benefit (group 1, thick line, filled squares) and with part-time or no sickness benefit (group 2, hatched line, filled squares, P < 0.0005, Friedman’s one-way analysis of variance) before and after the rehabilitation program and 6, 12, and 24 months after completion (x axis).
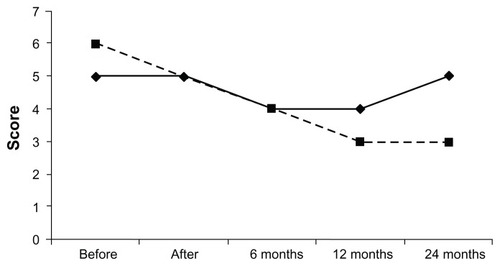
Figure 2 Development of the depression (HAD) score (y axis) in participants with a full-time sickness benefit (group 1, thick line, filled squares) and with a part-time or no sickness benefit (group 2, hatched line, filled squares, P < 0.01, Friedman’s one-way analysis of variance) before and after the rehabilitation program and 6, 12, and 24 months after completion (x axis).
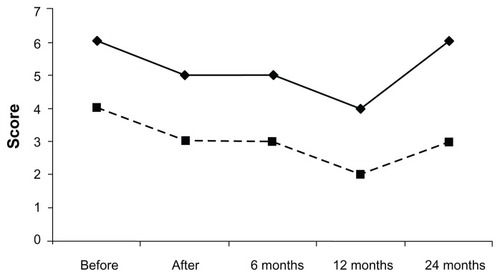
Table 2 Anxiety, depression, and stress scores (medians and percentiles 25–75) in individuals with a full-time sickness benefit (group 1) and with part-time or no sickness benefit (group 2) before rehabilitation and at 2-year follow-up
Stress
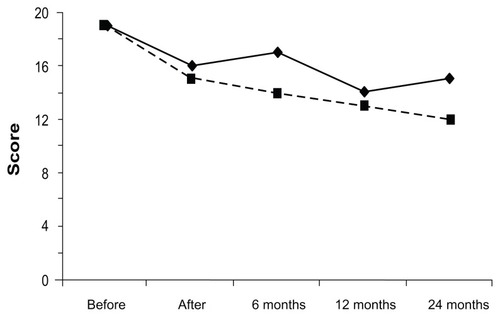
A decrease in stress was found in both groups at the 2-year follow-up compared with scores before the rehabilitation program (). In group 1, there was a decrease in stress after the rehabilitation program followed by an increased stress score at 6 months, followed by a decrease at the 12-month and 24-month follow-up visits. In group 2, stress gradually decreased and this reduction was maintained at the 2-year follow-up (P < 0.0005, ).
Figure 3 Development of the stress test score (y axis) in participants with full-time sickness benefit (group 1, thick line, filled squares) and with part-time or no sickness benefit (group 2, hatched line, filled squares, P < 0.0005, Friedman’s one-way analysis of variance) before and after rehabilitation program and at months 6, 12, and 24 after completion (x axis).
Discussion
In an earlier study of the outcome of multidisciplinary rehabilitation in patients with musculoskeletal pain, it was found that most participants improved in terms of self-reported physical disability and pain.Citation9 This was particularly true in those who were not or only part-time sick-listed (ie, group 2 patients in the present study). However, in a subgroup of patients (group 1), amounting to 16% of our total study group, with full-time sick-listing during rehabilitation and who were still sick-listed at the 2-year follow-up, little or no improvement was recorded during and after rehabilitation. These participants had higher scores for disability and pain at the 2-year follow-up visit than before the start of the program.Citation9
It was also found that anxiety and stress scores changed more favorably in group 2 than in group 1 during and after rehabilitation, and that the depression rating was higher in group 1 than in group 2 during the entire 2-year study period.
Group 1 reported lower self-estimated anxiety at the start of the rehabilitation program than group 2, but did not improve during the follow-up period, in contrast with group 2. The decrease in anxiety in group 2 was gradual and was maintained up to the 2-year follow-up. Group 1 showed higher self-estimated depression than group 2 throughout the study period. The development of the depression score was almost the same in the two groups, up until the 12-month follow-up, after which time there was an increase in group 1 but not in group 2. The participants in our study had nonmalignant pain in the neck, chest, and lower back, and they had a mixture of short-term and long-term sick-listing.
People with chronic pain may suffer from pain-related anxiety. Belief that pain is a sign of damage or harm to the body, and that activities that might cause pain should be avoided, is also thought to be an important contributor to disability and adjustment among such patients.Citation18,Citation19 Therefore, it is important that the rehabilitation program is focused on teaching the participants strategies for handling the disorder in question, to give them a better understanding not only of symptoms such as pain and disability but also of anxiety and depression.
The instrument used for assessing the level of self-rated stress behaviorCitation15 in this study showed that participants in both groups decreased their levels of stress during the study period. The two groups had nearly the same stress score at the start of the rehabilitation program, but at the 2-year follow-up, group 2 had a lower score for stress than group 1. In another study it was shown that in stressed employees, the illness burden represented by absenteeism was not affected by a stress reduction program, and that there was no substantial difference in effectiveness between the cognitive and physical interventions.Citation20 The participants in our rehabilitation program were offered a combination of theoretical and practical education and also individual guidance. They were offered individual counseling by a psychologist during their rehabilitation and if necessary during the follow-up period. At 5-year follow-up, after a multimodal program, Westman et al found a decrease in sick leave, improved quality of life, and reduction in pain. Improvements in perceived health and psychosomatic symptoms were also maintained at 5-year follow-up.Citation21 Several other studies and reviews of multidisciplinary treatment with a functional restoration approach similar to ours have shown strong support for the efficacy of the treatments regarding return to work, psychosocial variables, quality of life, and pain reduction.Citation22
The present study has limitations that need to be considered. The total study group, and group 1 in particular, were small. The study group was also heterogeneous, in that participants had both specific and nonspecific disorders related to the neck, chest, and lower back. There was also a mixture of nonsick-listed participants, included for preventive purposes, and participants on short-term and long-term sick leave. This is a disadvantage, considering that the aim of the study was to analyze results in specific diagnostic groups.
The strength of the study was that all individuals in a geographical area who met the inclusion criteria were offered rehabilitation in our program. Virtually no alternative service providers were available. Thus, the results achieved in this study group are highly applicable to patients in primary health care, and the risk of selection bias is consequently small. Five measurements were taken over a 2-year period. There was good consistency between the results obtained with different test instruments over time. All instruments have been widely used and have shown good validity.Citation13–Citation15 The participants underwent measurements by the same physiotherapists on all occasions and the researcher did not know the subjects personally.
We showed in our study that participants with musculoskeletal disorders who were sick-listed full-time throughout the 2-year study period (group 1) did not deteriorate in anxiety, depression, or stress scores during that period. In a previous study, the same group of subjects was found to have high pain rating and high self-reported physical disability, with little or no improvement during and after rehabilitation. They even reported higher scores for pain rating and disability at the 2-year follow-up than before the start of the program.Citation9 Participants who had part-time or no sick leave (group 2) showed an improvement in anxiety, depression, and stress during the 2-year study period. It has previously been reported that individuals with extreme pain prior to rehabilitation are at risk for having a lower rate of completion of rehabilitation, a higher rate of post-rehabilitation depression and disability, and lower levels of tolerance for physical activity.Citation23 The participants who were sick-listed full-time in the present study did not benefit from the rehabilitation program. Their sick-listing did not change during the 2-year study period, and neither did their pain rating score or anxiety and depression score. These results indicate that persons with musculoskeletal pain and psychological symptoms may require rehabilitation with a different content from that which we were able to give this group. Our findings also indicate that investigation and appropriate treatment of psychological symptoms, including anxiety and depression, are important in multidisciplinary rehabilitation of musculoskeletal disorders.
Conclusion
Anxiety, depression, and stress changed more favorably in participants with part-time or no sick leave than in those with full-time sick leave during and after rehabilitation. The results indicate that investigation and appropriate treatment of psychological symptoms like anxiety, depression, and stress is essential in multidisciplinary rehabilitation of musculoskeletal disorders.
Acknowledgments
This study was supported by the Jämtland County Council, Sweden. The authors would like to thank Hälsan Rehabilitation, Strömsund, Sweden, and especially Ann Färdvall, Britt-Marie Bryntesson, and Marita Oscarsson, for their help in making this study possible.
Disclosure
The authors report no conflicts of interest in this work.
References
- HenningsenPLöweBDepression, pain, and somatoform disordersCurr Opin Psychiatry2006191192416612174
- DelgadoPLCommon pathways of depression and painJ Clin Psychiatry200465Suppl 12161915315473
- FishbainDACutlerRRosomoffHLRosomoffRSChronic pain-associated depression: antecedent or consequence of chronic pain? A reviewClin J Pain19971321161379186019
- SBUThe Swedish Council on Technology Assessment in Health CareBack pain, neck pain volume I 2000 http://www.sbu.se2012
- SBUThe Swedish Council on Technology Assessment in Health CareSick-listing- reasons, consequences and praxis. A review 2003 http://www.sbu.se2012
- BoeresmaKLintonSJScreening to identify patients at risk: profiles of psychological risk factors for early interventionClin J Pain2005211384315599130
- SoaresJJJablonskaBPsychosocial experiences among primary care patients with and without musculoskeletal painEur J Pain200481798914690678
- KarjalainenKMalmivaaraAvan TulderMMultidisciplinary bio-psychosocial rehabilitation for sub-acute low-back pain among working age adultsCochrane Database Syst Rev20032CD00219312804427
- SjöströmRAlricssonMAsplundRNordenmarkMBack to work – a two year outcome of a multidisciplinary rehabilitation programme focused on physical function and painDisabil Rehabil200931323724218608399
- LundgrenCMolanderCTeamwork in Medical RehabilitationStockholm, SwedenLiber AB2008 Swedish
- SjöströmRAlricssonMAsplundRBack to work – evaluation of a multidisciplinary rehabilitation programme with emphasis on musculoskeletal disorders. A two-year follow-upDisabil Rehabil200830964965517852298
- SjöströmRAsplundRAlricssonMTwo-year outcome of a multidisciplinary vocational rehabilitation programme focused on range of motion of the neck and backWork201037434134821099009
- ZigmondASSnaithRPThe Hospital Anxiety and Depression ScaleActa Psychiatr Scand19836763613706880820
- BaldaccihnoDRBowmanGSBuhagiarAReliability testing of the hospital anxiety and depression (HAD) scale in the English, Maltese and back-translation versionsInt J Nurs Stud200239220721411755451
- ClaessonMBurellGBirganderLSLindahlBAsplundKPsychosocial distress and impaired quality of life – targets neglected in the secondary prevention in women with ischaemic heart diseaseEur J Cardiovasc Prev Rehabil200310425826614555880
- Swedish Social Insurance AgencyYour Guide to Försäkringskassan and social insurance in SwedenFörsäkringskassan2008
- PallantJSPSS, Survival Manual A Step by Step Guide to Data Analysis Using SPSS for Windows3rd edSydney AustraliaThe McGraw-Hill Companies2007
- GeisserMERobinsonMEMillerQLBadeSMPsychosocial factors and functional capacity evaluation among persons with chronic painJ Occup Rehabil200313425927614671990
- VowlesKEZvolenskyMJGrossRTSperryJAPain-related anxiety in the prediction of chronic low-back pain distressJ Behav Med2004271778915065477
- van RhenenWBlonkRWBSchaufeliWBvan DijkFJHCan sickness absence be reduced by stress reduction programs: on the effectiveness of two approachesInt Arch Occup Environ Health200780650551517093962
- WestmanALintonSJTheorellTÖhrvikJWahlénPLeppertJQuality of life and maintenance of improvements after early multimodal rehabilitation: a 5-year follow-upDisabil Rehabil200628643744616507506
- SchonsteinEKennyDTKeatingJKoesBWWork conditioning, work hardening and functional restoration of workers with back and neck painCochrane Database Syst Rev20031CD00182212535416
- McGearyDDMayerTGGatchelRJHigh pain ratings predict treatment failure in chronic occupational musculoskeletal disorderJ Bone Joint Surg Am200688231732516452743