
Abstract
Purpose
To evaluate the relationship between depressive symptoms and sarcopenia among older adults.
Materials and Methods
This is a cross-sectional study. A total of 700 community-dwelling older persons enrolled in this study. Sarcopenia is defined according to the Asian Working Group for Sarcopenia 2019 (AWGS 2019). The bioelectrical impedance analysis assessed muscle mass while a digital dynamometer quantified muscle strength. Furthermore, a 6-meter gait speed test measured physical performance. The Geriatric Depression Scale (GDS-30) screened for depressive symptoms. Data collected include those of socio-demographic, lifestyle, and comorbidity.
Results
The sample comprised 700 participants (455 women) with a mean age of 70.4±6.8 years. 21.5% had sarcopenia, among them, 5.6% at severe stage, while depressive symptoms were present in 8.1% (57/700). After adjusting for the potential confounders of age, sex, marital status, living status, hypertension, body mass index, and physical activity, the depressive symptoms that were found were not associated with sarcopenia but, instead, low gait speed. However, severe sarcopenia significantly impacted the risk of depressive symptoms, particularly in females.
Conclusion
Depressive symptoms are not associated with sarcopenia, but severe sarcopenia increases the risk of depressive symptoms in females, according to updated AWGS 2019 criteria. Gait speed is independently associated with depressive symptoms. The finding highlights that older people with sarcopenia should be screened for depressive symptoms, especially females. Future studies should evaluate the value of gait speed interventions for depressive symptoms among older adults.
Introduction
The Coronavirus disease 2019 (COVID-19) is an extraordinary emergency that has become a worldwide pandemic. Countries have implemented unprecedented draconian measures, such as travel bans, quarantines, and social distancing to contain the spread of the infection. While quarantines and social distancing seem essential for the time being, the widespread, substantial and potentially harmful physical and psychological health effects of such measures should not be ignored.Citation1,Citation2 This is because these measures will significantly increase the key risk factors related to sarcopenia, such as a sedentary lifestyle and the unavailability of a healthy diet.Citation3
Sarcopenia is an age-related skeletal muscle disorder characterized by the developing and generalized loss Of muscle strength, mass, and function.Citation4 Its prevalence increases with age and varies from 6.54% to 40.4% around the world.Citation5,Citation6 In the literature reports, sarcopenia contributes to multiple adverse outcomes, such as loss of mobility and independence, high risk of falls, fractures, and depression.Citation7–Citation10 All these undesirable outcomes may prolong hospital stays, create long-term disability, increase drug consumption,Citation11 and drive up healthcare costs for patients.Citation12 Sarcopenia is a predictable risk factor for infection and death in patients with COVID-19.Citation13 Patients with sarcopenia are more vulnerable to COVID-19, especially the older ones.Citation14 Therefore, more attention needs to be paid to the physical and mental health of the elderly, and to minimize the infection rate, morbidity and mortality of sarcopenia in the elderly during the pandemic.Citation3
With the increasing concerns about sarcopenia, and based on important advances in research, the Asian Working Group for Sarcopenia (AWGS) issued an updated consensus in 2019.Citation15 The updated diagnostic algorithm also recommends three core diagnostic components (low muscle mass, low grip strength, and low speed) for diagnosing sarcopenia and a grading of sarcopenia. The updated sarcopenia criteria have revised the cut-off point of the diagnostic components, which may have a potential impact on the prevalence and the association with adverse events. Although the AWGS 2019 criteria have been adopted in many studies, in China they were used only to assess the prevalence of sarcopenia.Citation16,Citation17
Depressive symptoms are common in older populations, and they are associated with a series of adverse health outcomes. It was reported that the prevalence rate of depressive symptoms in older populations ranges from 11% to 42%.Citation18,Citation19 Depressive symptoms are closely related to high risk of morbidity, disability and mortality; they have also been declared to be the main cause of suicides at older ages.Citation20,Citation21 High prevalence of depressive symptoms and their association with multiple adverse events represent a major public health problem.Citation22
Sarcopenia and depressive symptoms share similar pathways to pathophysiology (neurotrophins, inflammatory markers, and oxidative stress markers),Citation23,Citation24 etiology (physical inactivity),Citation24 and prognosis (high disability, mortality, and morbidity). Because sarcopenia and depressive symptoms and the adverse events caused by these diseases are severe, the association between the two clinical conditions cause public concern and have been explored in many studies, but with conflicting results.Citation23–Citation25
Although the association between depressive symptoms and sarcopenia has been investigated by cross-sectional studies,Citation26,Citation27 few used the AWGS 2019 definition. In addition, the studies using data from Asia (South Korea and Japan) reported no association between depressive symptoms and sarcopenia.Citation28,Citation29 So, the association between the two clinical conditions remains inconclusive based on the available literature. In addition, sarcopenia defined using the updated AWGS 2019 has yet to be evaluated in this manner. Therefore, the current survey aims to investigate the association between depressive symptoms and sarcopenia as explained used the AWGS 2019 criteria. We hypothesize in this present study that sarcopenia is associated with an increase in depressive symptoms in older adults.
Materials and Methods
Study Population
The present cross-sectional research was performed in Xin Xiang City, located in the north of China, from May to August 2021. The estimated odds ratio for the association between sarcopenia and depressive symptoms was set at 3.13.Citation24 A sample size of 434 was deemed necessary in order to achieve the statistical power of 0.9 with an alpha error of 0.05 with G*Power 3.0.Citation30,Citation31 There were 700 community-dwelling older people enrolled in the study, therefore the sample size was sufficiently large to detect statistically significant differences.
A multi-stage sampling approach was used in the present investigation. In stage one, there were sixteen regions in Xin Xiang City, seven were randomly selected by computer according to geographical administrative divisions, resulting in two districts, one county-level city, two counties, and two development zones. In stage two, older people were proportionally (proportion=older population in region/total population) recruited from the seven selected regions. Individuals aged 60 years and older were included. Exclusion criteria consisted of the inability to walk even with walking aids, and the inability to communicate with interviewers. This study was conducted in compliance with the Declaration of Helsinki. Approval for this research was granted through the Ethics Committee of the University of Malaya (UM.TNC2/UMREC-673) and Xin Xiang Medical University (XYLL-20190523). Written informed consent was obtained before enrolment.
Data Collection
All participants completed a sociodemographic questionnaire, which included the following items: gender, age, marital status, education, work history, living arrangements, lifestyle, comorbidity. The levels of physical activity (PA) were evaluated by employing the Physical Activity Scale for the Elderly (PASE) by Washburn et al.Citation32 The scale comprised 12 items that addressed the frequency, duration, and intensity of physical, household, and work-related activities over one week. The Chinese version of PASE (PASE-C) had been tested in 2013 and showed acceptable reliability (intraclass correlation coefficient was 0.79).Citation33 PASE scores are categorized as: sedentary (0–40), light physical activity (41–90), and moderate to intense activity (>90).Citation34
Anthropometric assessments were obtained including height, weight, and body mass index (BMI). Height was assessed with a stadiometer accurate to the nearest cm, and weight was assessed with a digital floor scale accurate to 0.1 kg,Citation23 while body mass index (BMI) was determined as weight (kg) divided by height (m2). WHO have suggested BMI categories for East Asians as follows: underweight (<18.5 kg/m2), normal weight (18.5 to 22.9 kg/m2), overweight (23.0 to 24.9 kg/m2), and obese (≥25 kg/m2).Citation35
Assessment of Sarcopenia
According to the Asian Working Group for Sarcopenia (AWGS) 2019, sarcopenia is defined by the presence of low muscle mass alongside either low muscle strength or low physical performance. The presence of all three criteria, low muscle mass, low muscle strength, and low physical performance, defines severe sarcopenia.Citation36 In this study, muscle mass was assessed with a bioelectrical impedance analysis machine (BIA, InBody 230; Biospace Co. Ltd., Seoul, Korea); low muscle mass was defined through a relative skeletal muscle mass index [appendicular skeletal muscle mass (ASM)/height (Ht)2], <7.0 kg/m2 for males and <5.7 kg/m2 for females; muscle strength was assessed with the aid of handgrip strength (HGS) utilizing a digital dynamometer (EH101; Camry, Zhongshan, China). The highest-measured value (more often by the dominant hand) identified sarcopenia. The cut-off values for HGS were below 28kg for men and below 18kg for women. Physical performance was determined using the gait speed (GS) of the 6m walk. The test was conducted in an examination room with a walkway exceeding 8m in length; the start and end of a 6m distance were marked clearly. Participants were instructed to walk down the walkway at their usual speed, starting 1m before the first marker until they had cleared the second marker. The time taken for each participant to cover 6m was recorded using a stopwatch accurate to the nearest 0.1s, and the GS was determined in m/s. A cut-off value of 1 m/s of GS defined low physical performance in both males and females.Citation15
Assessment of Depressive Symptoms
The 30-item Geriatric Depressive Symptoms Scale (GDS-30) was developed specifically for the assessment of depressive symptoms in older people.Citation37 This is not a diagnostic tool to confirm depressive symptoms but can be used for case finding in older people who have high odds of having depressive symptoms.Citation24 The Chinese version of GDS-30 (GDS-30-C) showed good reliability and validity (internal consistency was 0.89, intraclass correlation coefficient was 0.85).Citation38 There are 30 items on the scale; each response in favor of depressive symptoms receives one point, while other responses are assigned zero points. The sum of scores for the 30 items ranges between 0 and 30, and a cut-off value of 11 and above signified the presence of depressive symptoms.Citation39
Statistical Analysis
The categorical variables were outlined as counts and percentages. Characteristics of participants according to depression status were compared using Chi-Square analysis or Fisher’s Exact analysis. Logistic regression examined the association between depressive symptoms and sarcopenia. Covariates were selected based on the results of univariate analysis and added to the model in sequence. The model was initially adjusted for age and sex (model 1). Then added variables including living status, marital status, hypertension, body mass index (model 2). The model was further adjusted for physical activity (model 3). Analysis with an interaction term between gender and sarcopenia and depressive symptoms verified the presence of effect modification by gender (Wald p =0.024 in gender-adjusted model), then conducted gender-stratified analysis (model 3a). Considering sarcopenia is an age-related muscle disease, age-stratified analysis was also performed (model 3b).
Statistical studies were conducted by employing SPSS Version 20.0 (IBM, Armonk, NY, www.ibm.com) with statistical significance set at p < 0.05.
Results
Among the 821 subjects recruited initially for the study, 65 did not meet the inclusion criteria (ie, could not walk). Among the remaining 756 subjects, 44 were uncontactable and 12 had insufficient data. 700 (98.3%) presented sufficient clinical data to be included in the present study ().
Figure 1 Flowchart of the participants included in this study.
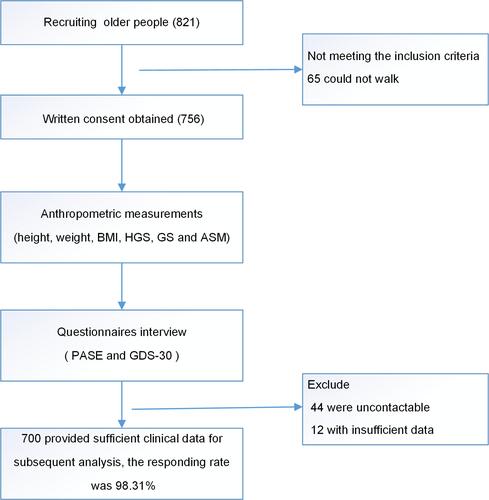
A total of 700 community-dwelling older persons (mean age=70.38±6.82, ranging from 60 to 93 years old, 65% female) from China enrolled in this study. Sarcopenia was found in 21.5% (150/700) of participants, while 5.6% (39/700) were at a severe stage. The prevalence of depressive symptoms was 8.1% (57/700). summarizes the characteristics of participants based on their status of sarcopenia. Individuals with sarcopenia were often older, living with others, and had hypertension (p<0.05). Furthermore, BMI and physical activity showed significant differences among different groups (p<0.001).
Table 1 Participants’ Characteristics According to Sarcopenia
Individuals with depressive symptoms (defined as GDS scores of 11 or greater) were closely tied with low GS (p<0.001) and severe sarcopenia (p<0.05) ().
Table 2 Univariate Association of Depressive Symptoms and Sarcopenia
Crude analysis showed handgrip strength, low GS and severe sarcopenia were associated with a high probability of depressive symptoms. In multiple logistic regression adjusted for age and gender, only low GS had an increased risk of depressive symptoms (, model 1). The significant association between GS and depressive symptoms persisted after successively adjusting for BMI (, model 2), physical activity (, model 3), and being female (, model 3a). In the gender-stratified analysis, severe sarcopenia increased the risk of depressive symptoms in females, but not for the males (, model 3a). In the age-stratified analysis, the presence of depressive symptoms was not associated with sarcopenia and its diagnostic components (, model 3b).
Table 3 Multivariate Association Between Depressive Symptoms and Sarcopenia and Its Diagnostic Components
Discussion
The overall results indicate that depressive symptoms are not associated with sarcopenia, but severe sarcopenia is associated with depressive symptoms in females. The presence of the component of low physical performance, defined using low GS alone, was independently associated with the presence of depressive symptoms, although this was not the case in the components of low muscle mass or low muscle strength. The results are therefore inconsistent with the assumed association between sarcopenia and depressive symptoms.
This study assessed the prevalence of sarcopenia defined by the AWGS 2019 criteria and yielded comparable findings with previous studies in the context of proportions of the populations which fulfilled the predefined criteria for sarcopenia.Citation40,Citation41 A cross-sectional investigation by Mo et alCitation40 showed a similar prevalence of sarcopenia, described by the AWGS 2019 criteria, in 21% of 1050 community-dwelling older people in Changsha City, China. Population characteristics and geographical location may potentially influence the prevalence of sarcopenia, even with the standardization of definitions using the AWGS criteria.Citation5,Citation42 In their study involving 542 community-dwelling Singaporeans aged 21‒90 years old, Pang et alCitation43 found a higher prevalence of sarcopenia (32.2%) in older adults using the AWGS 2019 criteria.
The prevalence of depressive symptoms in this study is in agreement with the results of previously published works on Chinese older adults. Wang et al enrolled 865 older people and evaluated depressive symptoms with GDS-15, establishing an 8.2% prevalence of depressive symptoms among their participants.Citation44 The prevalence of depressive symptoms ranged from 8% to 9% in other studies on older Asian populations,Citation45 which was significantly lower than in Europe and the United States. For example, the prevalence of depressive symptoms in the United Kingdom and the United States was 12.8% and 17.8%, respectively.Citation46,Citation47
The lack of association between sarcopenia and depressive symptoms within this study is consistent with the findings of several previous studies. ByeonCitation28 reported no association between sarcopenia and depressive symptoms in Korean adults. Similarly, Ishii et alCitation29 examined the relationship between sarcopenia, obesity and depressive symptoms with the 15-item GDS scale in 1732 community-dwelling older Japanese and found sarcopenia did not raise the odds of depressive symptoms. Studies that found no association between depressive symptoms and sarcopenia were from Asian countries (Japan, Korea). Depressive symptoms appeared to be influenced by low GS but not sarcopenia, which is in accordance with the findings of several previous investigations.Citation48–Citation52 Chen et alCitation52 examined the relationship between the three basic diagnostic components of sarcopenia and depressive symptoms with the 30-item GDS scale, in 250 older persons in a Chinese community and found a substantial association between depressive symptoms and GS. Gait speed is one of core diagnostic component of sarcopenia and a key indicator of physical performance. Physical performance in a frail population deteriorates as a result of decreasing muscle mass and muscle strength the two main diagnostic components of sarcopenia ie, not all frail individuals have poor physical performance but certainly have alterations in either muscle mass, muscle strength or both.Citation3 In the meantime, low GS is integral to depressive symptoms.Citation49,Citation53 In that case, slow GS does not result from muscle wasting/weakness and its association with GS is just an association with a symptom that frequently occurs in depression. This, therefore, highlights the potential role of GS interventions in preventing the progression of sarcopenia in individuals with depressive symptoms. An alternative explanation for the association between low GS and depressive symptoms is that reduced physical performance leads to a reduction in social participation, with resultant social isolation and depressive symptoms.Citation51,Citation53 Further, the task of GS as a potentially modifiable risk factor for depressive symptoms should be explored.
Both AWGS 2019 and the revised European Working Group on Sarcopenia in Older People (EWGSOP2) define “severe sarcopenia” as low muscle mass, low muscle strength, and low physical performance.Citation4,Citation54 The present study shows that the correlation is due to severe sarcopenia associated with depression in females, but not for the males, suggesting that the association between the two may depend on the stage of sarcopenia in females. These findings are in line with Yazar’s findings.Citation55 Yazar et al demonstrated that, compared to the normal aging group, a higher prevalence of severe sarcopenia was found in depressive older people (16.7% vs 7.1%, p<0.01), and depression was associated with sarcopenia stages. The possible explanation of the association might be that: First, the alterations in endocrine and metabolism caused by gender play an important role in the bilateral association between the two.Citation23,Citation56 Females, especially post menopause, are more prone to sarcopenia and depression than males. Menopause comes with unhappy physical changes, which may upset women more than men.Citation57 Second, in severe sarcopenic patients with lower muscles, grip strength and poor GS, synergistic adverse effects of the three components make them susceptible to depression.Citation58
The results remind us that identification of sarcopenia in the early stages and precautions against developing mental disorders are beneficial for the improvement of clinical outcomes of, in particular, sarcopenic older females. In view of the potential impact of different diagnostic methods on the association between the two common clinical conditions, the results of this study can broaden the data and provide direction for subsequent intervention strategies in the older, depressed population.
This study has some limitations. First, the study assessed muscle mass using BIA rather than gold standard magnetic resonance imaging (MRI), which may overestimate muscle mass and the results may fluctuate due to the distribution of water.Citation3,Citation59 However, compared with the expensive and time-consuming MRI, BIA has the advantages of being reliable, affordable, and portable.Citation60 Therefore, the consensus still recommends BIA as a good alternative to muscle mass measurement.Citation15 Second, the cross-sectional study design precludes the assignment of any temporal relationship. Indeed, a bidirectional relationship is expected between severe sarcopenia and depressive symptoms. Finally, the involvement of a community-based sample without being randomly selected but rather recruited through attendance at a research center may have inadvertently excluded frailer and home-bound individuals and hence resulted in an underestimate of the severity and prevalence of sarcopenia in this population. Future prospective studies should establish the cause-effect relationship between severe sarcopenia and depressive symptoms.
Conclusion
Depressive symptoms are not associated with sarcopenia as defined by the updated AWGS 2019 criteria, and severe sarcopenia is associated with depressive symptoms in females but not males. Gait speed is independently associated with depressive symptoms. Early treatments focusing on sarcopenia and GS may help females delay the development of sarcopenia and the onset of depressive symptoms.
Acknowledgments
We would like to express our appreciation to Prof. Chong Mei Chan, Prof. Tan Maw Pin, Prof. Chua Yan Piaw and Prof. Zhang Jin Hua for valuable comments in the paper revision. We also would like to say thanks to Prof. Zhang Jin Hua, for her assistance in the data collection for this study.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Williams SN, Armitage CJ, Tampe T, Dienes K. Public perceptions and experiences of social distancing and social isolation during the COVID-19 pandemic: a UK-based focus group study. BMJ open. 2020;10(7):e039334. doi:10.1136/bmjopen-2020-039334
- Setiawati Y, Wahyuhadi J, Joestandari F, Maramis MM, Atika A. Anxiety and resilience of healthcare workers during COVID-19 pandemic in Indonesia. J Multidiscip Healthc. 2021;14:1. doi:10.2147/JMDH.S276655
- Ali AM, Kunugi H. Screening for sarcopenia (physical frailty) in the COVID-19 era. Int J Endocrinol. 2021;2021:8738. doi:10.1155/2021/5563960
- Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age and Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
- Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393(10191):2636–2646. doi:10.1016/S0140-6736(19)31138-9
- Tian S, Xu Y, Han F. Prevalence of sarcopenia in the community-dwelling, elderly Chinese population: a systematic review and meta-analysis. Lancet. 2017;390:S35. doi:10.1016/S0140-6736(17)33173-2
- Ali AM, Kunugi H. Physical frailty/sarcopenia as a key predisposing factor to coronavirus disease 2019 (COVID-19) and its complications in older adults. BioMed. 2021;1(1):11–40. doi:10.3390/biomed1010002
- Ali AM, Kunugi H. Skeletal muscle damage in COVID-19: a call for action. Medicina. 2021;57(4):372. doi:10.3390/medicina57040372
- Ali AM, Kunugi H. Apitherapy for age-related skeletal muscle dysfunction (sarcopenia): a review on the effects of royal jelly, propolis, and bee pollen. Foods. 2020;9(10):1362. doi:10.3390/foods9101362
- Chen X, Guo J, Han P, et al. Twelve-Month Incidence of Depressive Symptoms in Suburb-Dwelling Chinese Older Adults: role of Sarcopenia. J Am Med Dir Assoc. 2019;20(1):64–69. doi:10.1016/j.jamda.2018.07.017
- Beaudart C, Reginster JY, Petermans J, et al. Quality of life and physical components linked to sarcopenia: the SarcoPhAge study. Exp Gerontol. 2015;69:103–110. doi:10.1016/j.exger.2015.05.003
- Goates S, Du K, Arensberg M, Gaillard T, Guralnik J, Pereira SL. Economic impact of hospitalizations in US adults with sarcopenia. J Frailty Aging. 2019;8(2):93–99. doi:10.14283/jfa.2019.10
- Wang PY, Li Y, Wang Q. Sarcopenia: an underlying treatment target during the COVID-19 pandemic. Nutrition. 2021;84:111104. doi:10.1016/j.nut.2020.111104
- Lim WS, Liang CK, Assantachai P, et al. COVID‐19 and older people in Asia: asian Working Group for Sarcopenia calls to action. Geriatr Gerontol Int. 2020;20(6):547–558. doi:10.1111/ggi.13939
- Chen WJ, Assantachai P, et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(3):300–307. doi:10.1016/j.jamda.2019.12.012
- Liu X, Hou L, Zhao W, et al. The Comparison of Sarcopenia Diagnostic Criteria using AWGS 2019 with the Other Five Criteria in West China. Gerontology. 2021;67(3):290–300. doi:10.1159/000513247
- Huang J, He F, Gu X, Chen S, Tong Z, Zhong S. Estimation of sarcopenia prevalence in individuals at different ages from Zheijiang province in China. Aging. 2021;13(4):6066. doi:10.18632/aging.202567
- Assariparambil AR, Noronha JA, Kamath A, et al. Depression among older adults: a systematic review of South Asian countries. Psychogeriatrics. 2021;21(2):201–219. doi:10.1111/psyg.12644
- Radovanović S, Kocić S, Sekulić M, Ristić G, Radević S, Janićijević K. Prevalence of depression over 65 in Serbia-public health significance. Vojnosanitetski pregled. 2020;1:132. doi:10.2298/VSP1912260132R
- Casey DA. Depression in older adults: a treatable medical condition. Primary Care. 2017;44(3):499–510. doi:10.1016/j.pop.2017.04.007
- Ali AM, Ali EM, Abou Mousa A, Ahmed ME, Hendawy AO. Bee honey and exercise for improving physical performance, reducing fatigue, and promoting an active lifestyle during COVID-19. Sports Med Health Sci. 2021;3(3):177–180. doi:10.1016/j.smhs.2021.06.002
- Ali AM, Alkhamees AA, Hori H, Kim Y, Kunugi H. The Depression Anxiety Stress Scale 21: development and Validation of the Depression Anxiety Stress Scale 8-Item in Psychiatric Patients and the General Public for Easier Mental Health Measurement in a Post COVID-19 World. Int J Environ Res Public Health. 2021;18(19):10142. doi:10.3390/ijerph181910142
- Szlejf C, Suemoto CK, Brunoni AR, et al. Depression is associated with sarcopenia due to low muscle strength: results from the ELSA-Brasil study. J Am Med Dir Assoc. 2019;20(12):1641–1646. doi:10.1016/j.jamda.2018.09.020
- Chen GJ, Han P, et al. Twelve-month incidence of depressive symptoms in suburb-dwelling Chinese older adults: role of sarcopenia. J Am Med Dir Assoc. 2019;20(1):64–69. doi:10.1016/j.jamda.2018.07.017
- Byeon CH, Kang KY, Kang SH, Kim HK, Bae EJ. Sarcopenia Is Not Associated with Depression in Korean Adults: results from the 2010-2011 Korean National Health and Nutrition Examination Survey. Korean J Fam Med. 2016;37(1):37–43. doi:10.4082/kjfm.2016.37.1.37
- Nipp RD, Fuchs G, El‐Jawahri A, et al. Sarcopenia is associated with quality of life and depression in patients with advanced cancer. The oncologist. 2018;23(1):97. doi:10.1634/theoncologist.2017-0255
- Kim KHS, Eun CR, et al. Depression Is Associated with Sarcopenia, Not Central Obesity, in Elderly K orean Men. J Am Geriatr Soc. 2011;59(11):2062–2068. doi:10.1111/j.1532-5415.2011.03664.x
- Byeon C-H, Kang K-Y, Kang S-H, Kim H-K, Bae E-J. Sarcopenia is not associated with depression in Korean adults: results from the 2010–2011 Korean National Health and Nutrition Examination Survey. Korean J Fam Med. 2016;37(1):37. doi:10.4082/kjfm.2016.37.1.37
- Ishii S, Chang C, Tanaka T, et al. The association between sarcopenic obesity and depressive symptoms in older Japanese adults. PLoS One. 2016;11:9. doi:10.1371/journal.pone.0162898
- Faul F, Erdfelder E, Lang AG, Buchner A. G* Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
- Faul F, Erdfelder E, Buchner A, Lang A-G. Statistical power analyses using G* Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
- Washburn R, Smith K, Jette A, Janney C. Physical Activity Scale for the Elderly: Administration and Scoring Instruction Manual. Watertown: New England Research Institute; 1991.
- Vaughan K, Miller WC. Validity and reliability of the Chinese translation of the Physical Activity Scale for the Elderly (PASE). Disabil Rehabil. 2013;35(3):191–197. doi:10.3109/09638288.2012.690498
- Curcio F, Liguori I, Cellulare M, et al. Physical activity scale for the elderly (PASE) score is related to sarcopenia in noninstitutionalized older adults. J Geriatric Physical Therapy. 2019;42(3):130–135. doi:10.1519/JPT.0000000000000139
- World Health Organization. Regional Office for the Western P. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment. Sydney: Health Communications Australia; 2000. Available from: http://iris.wpro.who.int/handle/10665.1/5379. Accessed March 26, 2022.
- Chen WJ, Assantachai P. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Med Res. 2020;21(3):300–307. e2. doi:10.1016/j.jamda.2019.12.012
- Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982;17(1):37–49. doi:10.1016/0022-3956(82)90033-4
- Chan AC-M. Clinical validation of the geriatric depression scale (GDS) Chinese version. J Aging Health. 1996;8(2):238–253. doi:10.1177/089826439600800205
- Jongenelis K, Pot A, Eisses A, et al. Diagnostic accuracy of the original 30‐item and shortened versions of the Geriatric Depression Scale in Nursing home patients. Int J Geriatric Psychiatry. 2005;20(11):1067–1074. doi:10.1002/gps.1398
- Mo Y-H, Zhong J, Dong X, et al. Comparison of three screening methods for sarcopenia in community-dwelling older persons. J Am Med Dir Assoc. 2020;22(4):746–750.e1. doi:10.1016/j.jamda.2020.05.041
- Chen HL, Zhang Y, Dong B. Analysis of the Prevalence of Sarcopenia and Its Risk Factors in the Elderly in the Chengdu Community. J Nutr Health Aging. 2021;25(5):600–605. doi:10.1007/s12603-020-1559-1
- Lee R, Liu LK, Peng LN, Lin MH, Chen LK. Comparisons of sarcopenia defined by IWGS and EWGSOP criteria among older people: results from the I-Lan longitudinal aging study. J Am Med Dir Assoc. 2013;14(7):528.e1–528. e7. doi:10.1016/j.jamda.2013.03.019
- Pang BWJ, Wee S-L, Lau LK, et al. Prevalence and associated factors of Sarcopenia in Singaporean adults—the Yishun Study. J Am Med Dir Assoc. 2021;22(4):885.e1–885. e10. doi:10.1016/j.jamda.2020.05.029
- Wang H, Hai S, Liu Y, et al. Association between depressive symptoms and sarcopenia in older Chinese community-dwelling individuals. Clin Interv Aging. 2018;13:1605. doi:10.2147/CIA.S173146
- Heok KE, Ho R. The many faces of geriatric depression. Curr Opin Psychiatry. 2008;21(6):540–545. doi:10.1097/YCO.0b013e328311cdae
- Cheruvu VK, Chiyaka ET. Prevalence of depressive symptoms among older adults who reported medical cost as a barrier to seeking health care: findings from a nationally representative sample. BMC Geriatr. 2019;19(1):1–10. doi:10.1186/s12877-019-1203-2
- Robb CE, de Jager CA, Ahmadi-Abhari S, et al. Associations of social isolation with anxiety and depression during the early COVID-19 pandemic: a survey of older adults in London, UK. Front Psychiatry. 2020;11:11. doi:10.3389/fpsyt.2020.00011
- Marino FR, Lessard DM, Saczynski JS, et al. Gait speed and mood, cognition, and quality of life in older adults with atrial fibrillation. J Am Heart Assoc. 2019;8(22):e013212. doi:10.1161/JAHA.119.013212
- Sanders JB, Bremmer MA, Comijs HC, Deeg DJ, Beekman AT. Gait speed and the natural course of depressive symptoms in late life; an independent association with chronicity? J Am Med Dir Assoc. 2016;17(4):331–335. doi:10.1016/j.jamda.2015.11.016
- Veronese N, Stubbs B, Trevisan C, et al. Poor physical performance predicts future onset of depression in elderly people: progetto Veneto Anziani Longitudinal Study. Phys Ther. 2017;97(6):659–668. doi:10.1093/ptj/pzx017
- Briggs R, Carey D, Claffey P, et al. Do differences in spatiotemporal gait parameters predict the risk of developing depression in later life? J Am Geriatr Soc. 2019;67(5):1050–1056. doi:10.1111/jgs.15783
- Chen L, Sheng Y, Qi H, Tang T, Yu J, Lv S. Correlation of sarcopenia and depressive mood in older community dwellers: a cross-sectional observational study in China. BMJ open. 2020;10(9):e038089. doi:10.1136/bmjopen-2020-038089
- Sanders JB, Bremmer MA, Deeg DJ, Beekman AT. Do depressive symptoms and gait speed impairment predict each other’s incidence? A 16‐year prospective study in the community. J Am Geriatr Soc. 2012;60(9):1673–1680. doi:10.1111/j.1532-5415.2012.04114.x
- Chen L-K, Woo J, Assantachai P, et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(3):300–307. doi:10.1016/j.jamda.2019.12.012
- Yazar HO, Yazar T. Prevalence of sarcopenia in patients with geriatric depression diagnosis. Ir J Med Sci. 2019;188(3):931–938. doi:10.1007/s11845-018-01957-7
- Chen X, Guo J, Han P, et al. Twelve-month incidence of depressive symptoms in suburb-dwelling Chinese older adults: role of sarcopenia. J Am Med Dir Assoc. 2019;20(1):64–69. doi:10.1016/j.jamda.2018.07.017
- Gómez-Tabares G, García W, Bedoya-Dorado E, Cantor EJC. Screening sarcopenia through SARC-F in postmenopausal women: a single-center study from South America. Climacteric. 2019;22(6):627–631. doi:10.1080/13697137.2019.1631788
- Kao T-W, Peng T-C, Chen W-L, Han D-S, Chen C-L, Yang W-SJA. Impact of adiposity on muscle function and clinical events among elders with dynapenia. Aging (Albany NY). 2021;13(5):7247. doi:10.18632/aging.202581
- Buckinx F, Reginster J-Y, Dardenne N, et al. Concordance between muscle mass assessed by bioelectrical impedance analysis and by dual energy X-ray absorptiometry: a cross-sectional study. BMC Musculoskelet Disord. 2015;16(1):1–7. doi:10.1186/s12891-015-0510-9
- Zambone MA, Liberman S, Garcia MLB. Anthropometry, bioimpedance and densitometry: comparative methods for lean mass body analysis in elderly outpatients from a tertiary hospital. Exp Gerontol. 2020;138:111020. doi:10.1016/j.exger.2020.111020