
Abstract
Introduction
Sexual harassment in the workplace is still the tip of the iceberg among front-line health workers, resulting in a high turnover of professionals, job dissatisfaction, absenteeism, and disharmonized health-care delivery. Research on the magnitude of workplace sexual harassment and factors associated with the workplace among nurses and midwives in Ethiopia is lacking. The study aimed to assess the magnitude and its associated factors among nurses and midwives working in northwestern Ethiopia referral hospitals.
Methods
This multicenter hospital-based cross-sectional study was conducted from April 11 to May 15, 2021 in northwestern Ethiopia referral hospitals. A self-administered structured questionnaire was used to collect data. Data were entered into EPI info 7.2.3.2 and analyzed using SPSS version 25. Binary logistic regression was utilized to identify factors associated with sexual harassment, and associations were deemed significant at P<0.05.
Results
As the findings show, sexual harassment prevalence in the workplace among female nurses and midwives was found to be 17.4% (95% CI 14.5%–19.5%). Many nurses and midwives who had experienced sexual harassment were harassed by patients’ families — 43.2%. Factors associated with sexual harassment in the workplace were being unmarried (AOR 4, 95% CI 2.3–12.6), work experience of less than 5 years (AOR 5, 95% CI 1.2–19), and participant age of 18–25 (AOR 7.2, 95% CI 5.9–17) years, all strongly associated with the outcome variable.
Conclusion and Recommendation
Sexual harassment among midwives and nurses employed in northwestern Ethiopia referral hospitals is not tolerable, as indicated in these findings. The government should address this by amending and reforming policies and strategies to obviate this problem.
Introduction
Sexual harassment is any form of unpleasant sexual act, requests for sex, and other psychological or physical conduct of a sexual nature that harms emotionally an individual’s employment or creates an intimidating, hostile, or offensive work environment. Sexual harassment is a form of gender discrimination that violates the human rights of the victim.Citation1,Citation2 Globally, sexual harassment is a chronic occupational health problem that negatively affects the dignity and psychological and mental health of health-care providers. Nurses and midwives are frontline workers with close interactions with opposite-sex patients, medical attendants, informal caregivers, paramedical staff, doctors, and administrative superiors.Citation2,Citation3
A global paradigm shift has resulted in increased female participation in the medical care workforce and is considered an indicator of development in general. Also, their skills and potential are highly recognized.Citation4 However, the issue of violence related to their sex, particularly sexual harassment in the workplace, is a significant problem.Citation5 Due to a lack of protocols and policies enabling an environment to address this issue in their workplace, they fail to report it and take it as part of the job, even when they realize that they are being harassed.Citation6 A recent report on the global supply chain showed that 85% of female health-care providers were frustrated with sexual harassment. During their working life, about 25%–50% of women are sexually harassed. Partly because nurses and midwives have long shifts, both night and day, in hospitals, the degree of harassment is extensive, and worse, many cases go unreported. Around 80% of female workers in the US reported experiencing sexual harassment in the health sector.Citation7,Citation8
Between 2015 and 2018, harassment of midwives and nurses in hospitals increased by 48% in Queensland and 44% in New South Wales, Australia. In Victoria, the number of nurses assaulted in health settings increased by 60% over the same period. A recent study of regional nurses in Australia reported that violence toward nurses is occurring on a daily basis and increasing in frequency.Citation9 A systematic review and meta-analysis worldwide of 28 studies showed that pooled prevalence of sexual harassment was 53%.Citation10 Research done in Ghana showed that 83% reported that they were harassed inside the hospital and over 50% indicated that a medical doctor sexually harassed them. The second–most commonly reported perpetrators of sexual harassment were patients, followed by coworkers.Citation11
Sexual harassment of nurses and midwives damages health-care delivery beyond individual violence, causing high-grade turnover, poor job satisfaction, absenteeism from work and sick leave, depression, anxiety, posttraumatic stress disorder, overlooking professional ethics, lack of a humanistic approach, decreased productivity, and a loss of teamwork passion.Citation2,Citation12,Citation13 Contributing and preventive factors related to sexual harassment are being researched worldwide. Shortage of staff, lack of security facilities, and lack of training on dealing with violence have been investigated as contributing factors, and reporting harassment, separating addicted patients from other patients, and guidelines to deal with harassment were listed as preventive factors.Citation14 This study intended to disover the prevalence of sexual harassment and associated factors among nurses and midwives in northwestern Amhara referral hospitals.
Methods
Study Design, Period, and Area
This multicenter hospital-based cross-sectional study was conducted from April 11 to May 15, 2021 in four northwestern Ethiopia referral hospitals. These institutions serve a population of around 12 million in their catchments, and around 680 female midwives and nurses were working at them during the data-collection period.Citation15
Study Population
All-female nurses and midwives working in the four hospitals were included in the study. Midwives and nurses who had transferred from other health institutions and had been employed less than 6 months before the beginning of the data-collection period were considered ineligible.
Variables
Sexual harassment (ever encountered: yes/no) was the outcome variable. Independent variables were sociodemographic (age, profession, work experience, marital status, monthly income, ethnicity, religion, education) and institutional (working unit, number of staff, shift).
Operational Definition
Sexual harassment in this research included sexual coercion, unwanted sexual attention, and gender harassment in either verbal or physical form.
Diploma
Minimum of 3 years’ professional training as a health professional after completion of secondary school.
Number of Staff
Assigned staff on duty and working hours in a single working unit.
Unmarried
Single, widowed, and separated.
To calculate the representative sample size, a single population–proportion formula was applied by considering common assumptions:
P=0.5, since this was a study on sexual harassment of women
margin of error 5%
z = confidence level 95%.
Therefore, . After adding a 10% nonresponse rate, the final sample size needed was 423. A list of midwives and nurses in the referral hospitals was obtained and proportional allocation based on nurse and midwife numbers applied, after which simple random sampling was used to select study subjects.
Data were collected with a pretested and self-administered structured questionnaire adapted from WHO and International Labour Organization (ILO) assessment tools and from reviewing the literature. Four professional nurses, one for each hospital, participated in data collection. Two MSc midwives also participated in supervision for all hospitals. The data-collection tool was developed in English and translated to the local language (Amharic). For the sake of consistency, the tool was translated back to English by language experts. Data collectors and supervisors were given training for 2 days on the aim of the study and the techniques of data collection. The data collectors were under supervision during data collection, and each data-collection tool was checked for completeness daily. Two persons were assigned to two computers for data entry to minimize error. Data-collection tools were pretested to check response consistency and watch for ambiguity. The pretest was done at Debre Markos Referral Hospital with 10% of the sample size. A correction measure was taken for the findings.
Following the dataset being checked for potential errors and accuracy, it was coded manually, then transferred to Epi Info version 7.2.3.2 and exported to SPSS version 25 for further analysis. Descriptive statistics were generated for numerical values, means, frequencies, and proportions to describe the study population, the outcomes, and explanatory variables. A binary logistic regression model was used and fitted to determine each explanatory variable with sexual harassment. Bivariate logistic regression analysis was used to determine the crude ORs and filter the explanatory variables for further analysis. Variables with a P<0.2 were considered for further multivariate logistic backward likelihood-ratio regression. Adjusted ORs with 95% CIs were used to estimate the strength of association betweens explanatory variables and sexual harassment. Finally, variables with P<0.05 were considered significantly associated with sexual harassment. To check model fitness, the Hosmer–Lemeshow goodness-of-fit test was used (P=0.66).
Ethics
The Ethics Review Committee of the School of Midwifery on behalf of the Institutional Review Board of the University of Gondar was the body responsible for giving clearance. Clearance was given to an author who was a former student in a postgraduate program, so the research proposal was examined by an ethics review board of the University of Gondar in addition to his master’s thesis proposal. To make data collection smooth, a formal cooperation letter was written by the university to relevant bodies.
The purpose and aim of the research were briefly explained to the study participants. Both oral and written consent was taken and attached to the information sheet of the data-collection tool. Data security and participants’ confidentiality were maintained at all levels of data management. This study was carried out in such a way that potential harm to the study participant was kept to a minimum. Prior to commencement, a comprehensive assessment of the expected risks and burdens for individuals participating was made, as well as expected benefits to them and other persons affected by the disease under investigation. This research adhered to the Declaration of Helsinki. All procedures followed the relevant guidelines and regulations.
Results
Sociodemographic Information
A total of 200 and 185 female nurses and midwives, respectively, of 385 participated in this study, making a 91% response rate. The mean age of respondents was 28.45±2.91 years. A majority (83.6%, 322) were aged 25–35 years, and 51.2% (197) were married ().
Table 1 Sociodemographic information (n=385)
Organizational Information
Of the 385 nurses and midwives, nearly half were working in the inpatient department (IPD; 48.8%, 188), 15.1% (58) in the maternity and obstetrics inpatient department, 14.5% (56) in the adult and pediatric emergency department, 12.2% (47) in the adult outpatient department (OPD), and 9.6% (36) in maternal and child health (MCH) clinics.
Magnitude of Workplace Sexual Harassment
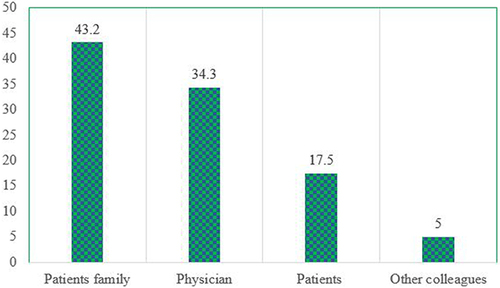
The overall prevalence of workplace sexual harassment in this study was found to be 17.4% (95% CI 14.5%–19.5%). Regarding perpetrators of harassment, about 43.1% (29) had been harassed by patients’ families, as shown in .
Figure 1 Initiators of sexual harassment toward nurses and midwives.
Factors Associated with Sexual Harassment
On bivariate binary logistic analysis, being unmarried, not having a degree, work experience <5 years, age 18–25 years, monthly income <US$100, working in the emergency department, and fewer than staff on the unit were associated with sexual harassment in the workplace. On multivariate analysis, being unmarried, <5 years’ work experience, and age 18–25 years remained significantly associated with sexual harassment at the workplace ().
Table 2 Bivariate and multivariate logistic regression analysis of factors associated with workplace sexual harassment
Discussion
Sexual harassment in the workplace is a systemic and pervasive problem within health care. It is not a series of random acts, but is an intentional crime.Citation16 In this research, the prevalence of sexual harassment was found to be 17.4% (95% CI 14.5%–19.5%). This finding is in line with research done in southern Ethiopia (13.5%).Citation17 The reason could be the similarity of settings and sociocultural makeup. On the contrary, our finding is much higher than in studies in Gambia and Uganda, where prevalence was about 10% and 8.1%, respectively.Citation18,Citation19 This also could be due to differences in catchment population, security protocols, and cultural characteristics. This might be due to differences in the cultural nature of abusers and participants. Our finding was much lower than a study in an Egypt university hospital, where prevalence was 58.1%.Citation19 A possible reason might be the study setting difference, which was a single university hospital, while this research used both university hospitals and nonteaching public hospitals. The finding of this scientific paper is much lower than a systematic meta-analysis done in 2020 of 22 peer-reviewedarticles on health-care workers in Africa, which found 7.2%–84.6%. This could be due to the approach or study-design difference, as this report is of a single study, whereas that study used pooled prevalence.
Initiators of sexual harassment toward nurses and midwives in this research were found to be patients’ families, physicians, patients themselves, and other colleagues. This study is similar to a report done among Iranian nurses, which could be due to setting similarity.Citation20 Being unmarried, work experience <5 years, and age 18–25 years in this research were significantly and independently associated with the outcome variable. The odds of sexual harassment among unmarried nurses and midwives were fourfold those of their married counterparts. This finding also resembles research done in China among nurses. This might be due to norms and culture of the society whereby sexual desire toward the unmarried is stronger than toward married individuals.Citation21
The odds of sexual harassment in the workplace among young (18–25 years) midwives and nurses in this research were 7.2-fold those of the others. This might be due to young female nurses and midwives being sexually attractive to attackers. In addition, work experience <5 years in hospitals increases the odds of workplace sexual harassment (AOR 5), which may be due to less adaptation to the health system and lack of soft skills in their career or senior nurses having dominance or power over less experienced nurses and midwives. These two related variables are in line with research done in Greece, where young and less experienced nurses were more likely to have been harassed sexually.Citation22
Limitations
Since this research used a cross-sectional study design, and recall bias may have occurred among research participants, so the authors tried to remember by provoking questions in the questionnaire. The research method was quantitative cross-sectional, which has the defect of exploring multiple variables and should be supported with a qualitative approach.
Conclusion and Recommendation
The magnitude of sexual harassment among nurses and midwives working in northwestern Amhara referral hospitals is not tolerable, as indicated by our findings. Being unmarried, <5 years of work experience, and age 18–25 years were significantly associated with sexual harassment in the workplace. The government of the country should work on this by amending and reforming policy strategies to enhance project execution on the gender issue. Working with nongovernmental organizations and the Gender Affairs Bureau is recommended to reduce the burden of workplace sexual harassment in the health system. Hospitals should have incident-reporting systems and should work with police, women and gender affairs offices, and judiciary bodies. The authors additional research with qualitative support in addition to quantitative measurement is preferable to address other associated variables.
Disclosure
The authors declare no conflicts of interest.
Acknowledgment
The authors want to thank the University of Gondar for the ethics approval and cooperation. We also want to thank all data collectors and study participants. Our thanks go to Amhara Regional Health Bureau for writing permission letters and to all referral hospitals for their cooperation.
Additional information
Funding
References
- Papantoniou P. Are male nurses sexually harassed? A cross-sectional study in the Greek Health System. BMC Nurs. 2021;20(1):137. doi:10.1186/s12912-021-00656-6
- Hejase HJ. Sexual harassment in the workplace: an exploratory study from Lebanon. J Manage Res. 2015;7(1):107.
- Abo Ali EA, Saied SM, Elsabagh HM, Zayed HA. Sexual harassment against nursing staff in Tanta University Hospitals, Egypt. J Egypt Public Health Assoc. 2015;90(3):94–100. doi:10.1097/01.EPX.0000470563.41655.71
- Sadruddin MM. Sexual harassment at workplace in Pakistan-Issues and remedies about the global issue in the managerial sector. J Manage Sci. 2015;7(1):113–125.
- Cheung T, Lee PH, Yip PS. Workplace violence toward physicians and nurses: prevalence and correlates in Macau. Int J Environ Res Public Health. 2017;14(8):879. doi:10.3390/ijerph14080879
- Mento C, Silvestri MC, Bruno A, et al. Workplace violence against healthcare professionals: a systematic review. Aggress Violent Behav. 2020;51:101381. doi:10.1016/j.avb.2020.101381
- Gutek BA, Done R. Sexual harassment. In: Unger R, editor. Handbook of the Psychology of Women and Gender. New York: John Wiley & Sons, Inc; 2001.
- Keplinger K, Johnson SK, Kirk JF, Barnes LY. Women at work: changes in sexual harassment between September 2016 and September 2018. PLoS One. 2019;14(7):e0218313. doi:10.1371/journal.pone.0218313
- Pich J, Roche M. Violence on the job: the experiences of nurses and midwives with violence from patients and their friends and relatives. Healthcare. 2020;8(4):522. doi:10.3390/healthcare8040522
- Lu L, Dong M, Lok GKI, et al. Worldwide prevalence of sexual harassment towards nurses: a comprehensive meta-analysis of observational studies. J Adv Nurs. 2020;76(4):980–990. doi:10.1111/jan.14296
- Boafo IM, Hancock P, Gringart E. Sources, incidence, and effects of non-physical workplace violence against nurses in Ghana. Nurs Open. 2016;3(2):99–109. doi:10.1002/nop2.43
- Hersch J. Sexual harassment in the workplace. IZA World Labor. 2015. doi:10.15185/izawol.188
- Mushtaq M, Sultana S, Imtiaz I. The trauma of sexual harassment and its mental health consequences among nurses. J College Phy Surg Pak. 2015;25(9):675–679.
- Khoshknab MF, Oskouie F, Ghazanfari N, et al. The frequency, contributing and preventive factors of harassment towards health professionals in Iran. Int J Community-Based Nurs Midwifery. 2015;3(3):156.16.
- Dagnaw EH, Bayabil AW, Yimer TS, Nigussie TS. Working in labor and delivery unit increases the odds of workplace violence in Amhara region referral hospitals: cross-sectional study. PLoS One. 2021;16(10):e0254962. doi:10.1371/journal.pone.0254962
- Sharma A. Sexual harassment at workplace experiences of women managers and organizations. IPEM LAW J. 2020;27:43.
- Fute M, Mengesha ZB, Wakgari N, Tessema GA. High prevalence of workplace violence among nurses working at public health facilities in Southern Ethiopia. BMC Nurs. 2015;14:9. doi:10.1186/s12912-015-0062-1
- Sisawo EJ, Ouedraogo S, Huang SL. Workplace violence against nurses in the Gambia: mixed methods design. BMC Health Serv Res. 2017;17(1):311. doi:10.1186/s12913-017-2258-4
- Maghraby RA, Elgibaly O, El-Gazzar AF. Workplace sexual harassment among nurses of a university hospital in Egypt. Sex& Reprod Healthcare. 2020;25:100519.
- Zeighami M, Mangolian Shahrbabaki P, Dehghan M. Iranian nurses’ experiences with sexual harassment in workplace: a qualitative study. Sex Res Soc Policy. 2022;4:1–14.
- Zeng LN, Lok KI, An FR, et al. Prevalence of sexual harassment toward psychiatric nurses and its association with quality of life in China. Arch Psychiatr Nurs. 2020;34(5):394–397. doi:10.1016/j.apnu.2020.07.016
- Papantoniou P. Sexual harassment and organizational silencing in nursing: a cross-sectional study in Greece. BMJ open. 2021;11(11):e050850. doi:10.1136/bmjopen-2021-050850