
Abstract
Introduction
The purpose of this study was to assess the bidirectional association between multimorbidity (MM) and probable depression in a longitudinal study in Thailand.
Methods
We analyzed longitudinal data of participants 45 years and older from two consecutive waves (in 2015 and 2017) of Health, Aging, and Retirement in Thailand (HART). Probable depression was assessed using the Center for Epidemiological Studies Depression scale. Logistic regression analysis was conducted to assess the association between baseline probable depression and incident physical MM, and baseline physical MM and incident probable depression.
Results
In all, 2712 participants without MM at baseline and 2684 without probable depression at baseline were included. At follow-up 15.6% of probable depression cases and 11.4% of nonprobable depression cases developed physical MM, and at follow-up 13.3% of physical MM cases and 8.9% of nonphysical MM cases developed probable depression. In the final logistic regression analysis, adjusted for age, sex, marital status, income, education, body mass index, physical activity, smoking tobacco, alcohol use, and social engagement, probable depression at baseline was positively associated with incident physical MM (aOR: 1.50, 95% CI: 1.09 to 2.06), and physical MM at baseline was positively associated with incident probable depression (aOR: 1.47, 95% CI: 1.07 to 2.02).
Discussion
Baseline physical MM increases the risk of incident probable depression and baseline probable depression increases the risk of incident physical MM among middle-aged and older adults in Thailand.
Introduction
Thailand has been undergoing a epidemiological and demographic transition, increasing ageing and chronic non-communicable diseases.Citation1,Citation2 This may include multimorbidity (MM) (co-existence of ≥2 chronic conditions) and depression increasing the burden on the health-care systems.Citation3,Citation4 Compared to people without MM, people with MM are two to three times more likely to have depression.Citation5 MM can have various negative health outcomes, such as disability, mental morbidity, higher health-care utilisation, and mortality.Citation5,Citation6 Depression in later life may increase comorbidity, reduce quality of life, social functioning,Citation7 suicidal behaviour,Citation8 and mortality.Citation9
In low- and middle-income countries (LMICs) the prevalence of MM was 29.7%,Citation10 in Thailand 30.4% among the general adult population,Citation11 among ageing adults in six LMICs, the prevalence of physical MM was 45.5%,Citation12 and among older adults in southern Thailand, the prevalence of MM was 16.8%.Citation13 Among older adults, the global prevalence of depression was 28.4%,Citation14 15.2% in India,Citation15 11.5% in Malaysia,Citation16 and in local studies in Thailand, the prevalence of probable depression ranged from 18.5%Citation17 to 28.5%.Citation18
Depression and MM are complex multifactorial conditions, and in unidirectional longitudinal studies, most investigations show an association between MM and incident depression, while fewer studies found an association between depression and incident MM, suggesting a possible bidirectional association between MM and depression.Citation19 So far, it appears that only two studies, namely from the China Health and Retirement Study, showed a bidirectional association between probable depression and MMCitation20 and self-reported diagnosed “hypertension, dyslipidaemia, diabetes, cancer, chronic lung disease, liver disease, heart problems, stroke, kidney disease, stomach or other digestive diseases, memory-related disease, arthritis or rheumatism and asthma”.Citation21 More studies are needed to investigate the bidirectional associations MM and depression to gain a better understanding of this relationship that can help improve the prevention and treatment of MM and depression.Citation19 Consequently, the objective of this study was to investigate the bidirectional association between probable depression and MM among middle-aged and older adults in Thailand.
Methods
Participants
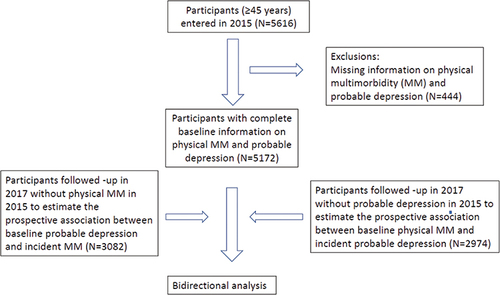
We analyzed longitudinal data from two consecutive waves (2015 and 2017) of the Health, Aging, and Retirement in Thailand (HART) cohort study. From the total population and household data in Thailand, a three-stage (regions, province, blocks, or villages) stratified random sampling was employed. In each household, one person (≥45 years) was randomly selected, being the inclusion criterium. Proxy interviews were conducted for frail participants.Citation22 The 2015 survey (from February to July) (N=5616) and 2017 survey (from January to June 2017) included 3,708 members of the 2015 HART cohort (192 died over the follow-up or 4.3% of the baseline respondents who were in the study area; 1,554 moved away from the study area; 270 declined participation; and the response rate: 72.33% and the retention rate: 66.03%).Citation22 A total of 3708 participants who responded to 2015 and 2017 survey were included in the study, and 3407 had complete information on our variables of interest (physical MM, and probable depression) (see ).
Figure 1 Study flow chart.
Participants were interviewed at their homes by trained field workers after written informed consent was obtained. The study was approved by the “Ethics Committee in Human Research, National Institute of Development Administration – ECNIDA (ECNIDA 2020/00012).” The study complies with the Declaration of Helsinki.
Measures
Outcome Variables
Chronic physical conditions were evaluated by self-reported health-care provider diagnosed conditions, including hypertension, diabetes, lung disease, emphysema, cardiovascular disease, heart disease, heart failure, rheumatism, arthritis, bone disease, low bone density, osteoporosis, kidney disease, cancer, and liver disease. Multimorbidity (MM) was defined as having two or more physical chronic conditions, and no MM as having no or one physical chronic condition.
Probable depression (≥10 scores) was defined using the Depression Scale of the Center for Epidemiologic Studies (CES-D-10).Citation23 The CES-D-10 had a reliability coefficient of 0.78 in wave 1 and 0.72 in wave 2 in this study. Previous studies have shown adequate validity of the CES-D-10 in the Thai (older) adult population.Citation24,Citation25
Independent variables
Social and demographic indicators: educational level, sex, age, marital status, and annual income quartile “1=0 to <380 US$, 2=380 to <1642, 3=1642 to <4093, 4≥4093 US$”.
Tobacco use: “Have you ever smoked cigarettes?” (response options: “1=yes, and still smoke now, 2=yes, but quit smoking, and 3=never”).
Alcohol use: “Have you ever drunk alcoholic beverages such as liquor, beer, or wine?” (response options: “1=yes, and still drinking now, 2=yes, but do not drink now, and 3=never)”.
Physical activity in the past week was divided into “none=inactivity, 1–149 min/week=low activity, and ≥150 min/week=high activity.”Citation26,Citation27
Body Mass Index (BMI): self-reported body weight and height, classified into “underweight (<18.5 kg/m2), normal weight (18.5–22.9 kg/m2), overweight (23–24.9 kg/m2), and obesity (25+ kg/m2).”Citation28
Social engagement included six items of formal social engagement (eg, participation in religious organisations) and one item of informal social engagement (meeting with close friends or relatives) and was defined as at least one activity in the past month.Citation22,Citation29
Data Analysis
Proportions of older adults with incident MM and incident probable depression are presented with frequencies and percent. Pearson chi-square tests are used to compare baseline characteristics among groups. The first logistic regression model estimated odds ratios (OR) and confidence intervals (CI) for baseline probable depression and incident MM, and the second model compared baseline MM and incident probable depression. Three models are presented for incident MM and incident probable depression. The first model is unadjusted, in the second model adjustments are made for age, income, sex, education, and marital status, and in the third model adjustments are made for model 2 variables plus smoking, physical activity, body mass index, alcohol use, and social engagement. p ≤0.05 was considered statistically significant. Missing values were excluded from the analyses. All statistical analyzes were done with StataSE 15.0 (College Station, TX, USA).
Results
Sample Characteristics
In the first model that estimates incident physical MM, a total of 2712 nonphysical MM individuals were included from baseline, with 320 (11.3%) having probable depression at baseline. At follow-up 15.6% of the probable depression cases and 11.4% of non-probable depression cases developed physical MM. Middle-aged and older adults with probable depression at baseline have a significantly higher prevalence of physical MM at follow-up (p<0.001). Those with physical MM were more likely to be older, not married, had a lower income, had a higher body mass index, had no social engagement, and had never smoked tobacco than those without physical MM (see )
Table 1 Sample Characteristics of Participants with Incident Physical Multimorbidity, Thailand, 2015–2017
In the second model that estimates incident probable depression, a total of 2684 individuals with non-probable depression were included from baseline, with 484 (16.2%) having MM at baseline. At follow-up 13.3% of MM cases and 8.9% of non-MM cases developed probable depression. Middle-aged and older adults with a physical MM at baseline have a significantly higher prevalence of probable depression at follow-up (p<0.001). Those with probable depression were more likely to be older, not married, and had lower income than those without probable depression (see ).
Table 2 Sample Characteristics of Participants with Incident Probable Depression, Thailand, 2015–2017
Odds Ratios for Bidirectional Associations Between Probable Depression and Physical Multimorbidity
In the final logistic regression model, adjusted for education, income, age, marital status, sex, smoking tobacco, body mass index, alcohol use, physical activity, and social engagement, probable depression at baseline was positively associated with incident physical MM (aOR: 1.50, 95% CI: 1.09 to 2.06), and physical MM at baseline was positively associated with incident probable depression (aOR: 1.47, 95% CI: 1.07 to 2.02) (see ).
Table 3 Odds Ratios for Bidirectional Associations Between Probable Depression and Physical Multimorbidity (MM)
Discussion
This is the first longitudinal study investigating the bidirectional associations between MM and probable depression in Southeast Asia. Consistent with two studies in China,Citation20,Citation21 we found that physical MM (hypertension, diabetes, lung disease, emphysema, cardiovascular disease, heart disease, heart failure, rheumatism, arthritis, bone disease, low bone density, osteoporosis, kidney disease, cancer, and liver disease) and probable depression were bidirectionally associated among older adults in Thailand. These associations were independent of body mass index, sex, marital status, age, education, income, smoking, physical activity, alcohol use, and social engagement.
Other previous studies have shown a bidirectional association between depression or depressive symptoms and specific chronic conditions, such as chronic kidney disease,Citation30 rheumatoid arthritis,Citation31 chronic lung disease,Citation32 type 2 diabetes,Citation33 ischaemic heart disease, and stroke,Citation34 and hypertension.Citation35 Therefore, the bidirectional association between physical MM and probable depression can be attributed in part to the specific chronic disease that has a stronger effect on probable depression among those with physical MM. For example, we found that diabetes and rheumatism or arthritis had a higher prevalence of incident probable depression (see Appendix 1).
Possible mechanisms that could explain the bidirectional association between MM and probable depression may include 1) shared risk factors, such as older age, obesity, physical inactivity, smoking, and alcohol use, for both MM and probable depression,Citation20 2) the immune-inflammatory effects stemming from specific chronic conditions, such as heart disease, arthritis, and hypertension, may influence the development of probable depression,Citation19 3) having MM may negatively impact various body organs increasing disempowerment and negative emotions leading to probable depression,Citation36 and 4) the effects of peripheral immune dysfunction among people with probable depression on specific chronic conditions, such as arthritis and hypertension.Citation20,Citation37
Clinical implications may include screening and treatment of depression in patients with MM as well as screening and treatment of MM in patients with depression.Citation5,Citation38 This cohort study only had a 2-year follow-up period, and future studies should be conducted over a longer time frame to assess more comprehensively multiple interacting pathways.Citation19
Study Strength and Limitations
The study utilized a national cohort study with a large sample size, and we adjusted for various confounding social, health, and demographic factors. Study limitations include that MM was assessed by self-reported diagnosed chronic conditions, depression was only measured with a screening questionnaire, and no objective measurements were used. Furthermore, MM could change over time, causing classification bias.
Conclusion
Baseline physical MM increases the risk of incident probable depression and baseline probable depression increases the risk of incident physical MM among middle-aged and older adults in Thailand. Results may help guide the prevention and treatment of MM and probable depression concurrently in middle and late adulthood in Thailand.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgment
The Health, Aging, and Retirement in Thailand (HART) study received support from the “Thailand Science Research and Innovation (TSRI) and the National Research Council of Thailand (NRCT)”.
References
- Anantanasuwong D. Population Ageing in Thailand: critical Issues in the Twenty-First Century. In: Narot P, Kiettikunwong N, editors. Education for the Elderly in the Asia Pacific, Education in the Asia-Pacific Region: Issues, Concerns and Prospects 59. Springer; 2021. doi:10.1007/978-981-16-3326-3_3
- Prasartkul P, Thaweesit S, Chuanwan S. Prospects and contexts of demographic transitions in Thailand. JPSS. 2019;27(1):1–22. doi:10.25133/JPSSv27n1.001
- Pati S, Swain S, Hussain MA, et al. Prevalence and outcomes of multimorbidity in South Asia: a systematic review. BMJ Open. 2015;5(10):e007235. doi:10.1136/bmjopen-2014-007235
- Pengpid S, Peltzer K. Multimorbidity in chronic conditions: public primary care patients in four greater Mekong countries. Int J Environ Res Public Health. 2017;14(9):1019. doi:10.3390/ijerph14091019
- Read JR, Sharpe L, Modini M, Dear BF. Multimorbidity and depression: a systematic review and meta-analysis. J Affect Disord. 2017;221:36–46. doi:10.1016/j.jad.2017.06.009
- Nunes BP, Flores TR, Mielke GI, Thumé E, Facchini LA. Multimorbidity and mortality in older adults: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2016;67:130–138. doi:10.1016/j.archger.2016.07.008
- Wen Y, Liu C, Liao J, Yin Y, Wu D. Incidence and risk factors of depressive symptoms in 4 years of follow-up among mid-aged and elderly community-dwelling Chinese adults: findings from the China health and retirement longitudinal study. BMJ Open. 2019;9(9):e029529. doi:10.1136/bmjopen-2019-029529
- Fernandez-Rodrigues V, Sanchez-Carro Y, Lagunas LN, et al. Risk factors for suicidal behaviour in late-life depression: a systematic review. World J Psychiatry. 2022;12(1):187–203. doi:10.5498/wjp.v12.i1.187
- Wei J, Hou R, Zhang X, et al. The association of late-life depression with all-cause and cardiovascular mortality among community-dwelling older adults: systematic review and meta-analysis. Br J Psychiatry. 2019;215(2):449–455. doi:10.1192/bjp.2019.74
- Nguyen H, Manolova G, Daskalopoulou C, et al. Prevalence of multimorbidity in community settings: a systematic review and meta-analysis of observational studies. J Comorb. 2019;9:2235042X19870934. doi:10.1177/2235042X19870934
- Phulkerd S, Thapsuwan S, Chamratrithirong A, Gray RS. Influence of healthy lifestyle behaviors on life satisfaction in the aging population of Thailand: a national population-based survey. BMC Public Health. 2021;21(1):43. doi:10.1186/s12889-020-10032-9
- Vancampfort D, Stubbs B, Koyanagi A. Physical chronic conditions, multimorbidity and sedentary behavior amongst middle-aged and older adults in six low- and middle-income countries. Int J Behav Nutr Phys Act. 2017;14(1):147. doi:10.1186/s12966-017-0602-z
- Sukchan P, Chemoh W, Payanglee K. Morbidity and multi-morbidity among the elderly population in southernmost Thailand: cox proportional hazards regression model of survival approach. PNUJR. 2019;12(1):89–105.
- Hu T, Zhao X, Wu M, et al. Prevalence of depression in older adults: a systematic review and meta-analysis. Psychiatry Res. 2022;311:114511. doi:10.1016/j.psychres.2022.114511
- Lotfaliany M, Hoare E, Jacka FN, et al. Variation in the prevalence of depression and patterns of association, sociodemographic and lifestyle factors in community-dwelling older adults in six low- and middle-income countries. J Affect Disord. 2019;251:218–226. doi:10.1016/j.jad.2019.01.054
- Ahmad NA, Abd Razak MA, Kassim MS, et al. Association between functional limitations and depression among community-dwelling older adults in Malaysia. Geriatr Gerontol Int. 2020;20(Suppl 2):21–25. doi:10.1111/ggi.14012
- Charoensakulchai S, Usawachoke S, Kongbangpor W, et al. Prevalence and associated factors influencing depression in older adults living in rural Thailand: a cross-sectional study. Geriatr Gerontol Int. 2019;19(12):1248–1253. doi:10.1111/ggi.13804
- Haseen F, Prasartkul P. Predictors of depression among older people living in rural areas of Thailand. Bangladesh Med Res Counc Bull. 2011;37(2):51–56. doi:10.3329/bmrcb.v37i2.8434
- Triolo F, Harber-Aschan L, Belvederi Murri M, et al. The complex interplay between depression and multimorbidity in late life: risks and pathways. Mech Ageing Dev. 2020;192:111383. doi:10.1016/j.mad.2020.111383
- Ye B, Xie R, Mishra SR, et al. Bidirectional association between physical multimorbidity and subclinical depression in Chinese older adults: findings from a prospective cohort study. J Affect Disord. 2022;296:169–174. doi:10.1016/j.jad.2021.09.067
- Qiao Y, Liu S, Zhang Y, et al. Bidirectional association between depression and multimorbidity in middle-aged and elderly Chinese adults: a longitudinal cohort study. Aging Ment Health. 2022;26(4):784–790. doi:10.1080/13607863.2021.1877609
- Anantanasuwong D, Theerawanviwat D, Siripanich P. Panel survey and study on health and aging, and retirement in Thailand. In: Gu D, Dupre M, editors. Encyclopedia of Gerontology and Population Aging. Cham: Springer; 2019.
- Andresen EM, Malmgren JA, Carter WB, Patrick DL. Screening for depression in well older adults: evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). Am J Prev Med. 1994;10(2):77–84. doi:10.1016/S0749-3797(18)30622-6
- Nilmanut S, Kuptniratsaikul V, Pekuman P, Tosayanonda O. The study of the Center for Epidemiologic Studies-Depression Scale (CES-D) in Thai People Siriraj Hospital. ASEAN J Rehabil Med. 1997;6(3):25–29.
- Mackinnon A, McCallum J, Andrews G, Anderson I. The center for epidemiological studies depression scale in older community samples in Indonesia, North Korea, Myanmar, Sri Lanka, and Thailand. J Gerontol B Psychol Sci Soc Sci. 1998;53(6):P343–P352. doi:10.1093/geronb/53b.6.p343
- Kim SH, Park S. A meta-analysis of the correlates of successful aging in older adults. Res Aging. 2017;39(5):657–677. doi:10.1177/0164027516656040
- World Health Organization. World Health Organization (WHO) guidelines on physical activity and sedentary behaviour. Licence: CC BY-NC- SA3.0 IGO; 2020. Available from: file:///C:/Users/user/Downloads/9789240015128-eng%20(2).pdf. Accessed May 2, 2022.
- Wen CP, David Cheng TY, Tsai SP, et al. Are Asians at greater mortality risks for being overweight than Caucasians? Redefining obesity for Asians. Public Health Nutr. 2009;12(4):497–506. doi:10.1017/S1368980008002802
- Berkman LF, Sekher TV, Capistrant B, Zheng Y. Social networks, family, and care giving among older adults in India. In: Smith JP, Majmundar M, editors. Aging in Asia: Findings from New and Emerging Data Initiatives. Washington DC: The National Academic Press; 2012:261–278.
- Liu M, Zhang Y, Yang S, et al. Bidirectional relations between depression symptoms and chronic kidney disease. J Affect Disord. 2022;311:224–230. doi:10.1016/j.jad.2022.05.104
- Ng CYH, Tay SH, McIntyre RS, et al. Elucidating a bidirectional association between rheumatoid arthritis and depression: a systematic review and meta-analysis. J Affect Disord. 2022;311:407–415. doi:10.1016/j.jad.2022.05.108
- Zheng J, Li J, Pei T, et al. Depressive symptoms and chronic lung disease in middle-aged and older Chinese adults: prospective bidirectional association and mediation analysis. J Affect Disord. 2022;297:283–293. doi:10.1016/j.jad.2021.10.023
- Zhao F, Pan A, Yang X, et al. Bidirectional association between depressive symptoms and type 2 diabetes mellitus: the China Health and Retirement Longitudinal Study. J Diabetes Complications. 2019;33(10):107387. doi:10.1016/j.jdiacomp.2019.05.018
- Wium-Andersen MK, Wium-Andersen IK, Prescott EIB, et al. An attempt to explain the bidirectional association between ischaemic heart disease, stroke and depression: a cohort and meta-analytic approach. Br J Psychiatry. 2020;217(2):434–441. doi:10.1192/bjp.2019.130
- Jeon SW, Chang Y, Lim SW, et al. Bidirectional association between blood pressure and depressive symptoms in young and middle-age adults: a cohort study. Epidemiol Psychiatr Sci. 2020;29:e142. doi:10.1017/S2045796020000542
- Bi YH, Pei JJ, Hao C, Yao W, Wang HX. The relationship between chronic diseases and depression in middle-aged and older adults: a 4-year follow-up study from the China Health and Retirement Longitudinal Study. J Affect Disord. 2021;289:160–166. doi:10.1016/j.jad.2021.04.032
- Grippo AJ, Johnson AK. Stress, depression and cardiovascular dysregulation: a review of neurobiological mechanisms and the integration of research from preclinical disease models. Stress. 2009;12(1):1–21. doi:10.1080/10253890802046281
- Birk JL, Kronish IM, Moise N, et al. Depression and multimorbidity: considering temporal characteristics of the associations between depression and multiple chronic diseases. Health Psychol. 2019;38(9):802–811. doi:10.1037/hea0000737