
Abstract
Background
Although the inverted technique was shown to be more effective compared to other orthotic designs for the treatment of flatfeet, the biomechanical mechanisms underlying the therapeutic effect of the inverted angle orthoses is still unclear. Therefore, the aim of this study was to examine the effect of different inverted angles of foot orthoses on walking kinematics in females with flexible flatfeet.
Methods
Thirty-one female adults with flexible flatfeet aged 18–35 years old participated in this study. Kinematic data of the hip, knee, and ankle were collected via BTS motion-capture system during walking under three test conditions in random order: with shoes only; with 15° inverted orthoses; and with 25° inverted orthoses.
Results
Compared to the shoes only condition, both the 15° and 25° inverted orthotic conditions significantly decreased the maximum ankle plantarflexion angle during loading response, maximum ankle dorsiflexion angle during mid-stance, maximum ankle external rotation angle, and maximum ankle internal rotation angle. The maximum ankle plantarflexion angle at toe-off showed a significant decrease with the 25° inverted angle orthosis compared to both the 15° inverted angle and shoes only conditions. No significant differences were found in the knee kinematic variables, maximum hip extension angle, and maximum hip adduction angle between test conditions.
Conclusion
Using inverted orthoses at 15° and 25° inverted angles resulted in significant changes in ankle joint kinematics during walking in female adults with flexible flatfeet. A 25° inverted angle orthosis significantly decreased ankle plantarflexion during push-off, potentially impacting gait mechanics. This suggests that a smaller inverted angle may be more effective for managing flexible flatfeet in female adults.
Introduction
Flatfoot, also known as Pes planus, is a condition characterized by the absence of the medial longitudinal arch (MLA) of the foot, resulting in the full contact of the foot sole with the ground.Citation1 It is classified as flexible or rigid based on the flexibility of the medial arch. The most common type is flexible flatfeet, in which the MLA collapses only during weight bearing.Citation2 The typical presentation of flexible flatfeet includes subtalar pronation, which is associated with calcaneal eversion, midfoot pronation, and forefoot abduction/supination.Citation3 These deformities have been shown to increase the risk of foot injuries and are associated with various symptoms, including pain in the plantar fascia, foot instability, ligament laxity, and discomfort in the knee, hip, and trunk.Citation4–7 Flattening of the MLA and increased rearfoot eversion in individuals with flatfeet lead to excessive tension in the plantar fascia, contributing to conditions like plantar fasciitis and ankle pain.Citation5,Citation6 Additionally, excessive ankle movements during walking with flatfeet can reduce shock absorption ability and increase the load on the foot structure, leading to fatigue fractures in the forefoot, foot deformities, and degenerative arthritis in the knee.Citation7–10
Furthermore, the mechanical overload resulting from foot pronation in cases of flatfeet, transfers a chain of biomechanical deviations to the proximal regions, including the lower extremities and spine.Citation11 This excessive foot pronation induces femoral and tibial internal rotation in a closed kinematic chain, subsequently leading to increased pelvic anteversion.Citation12,Citation13 This further leads to an increased lordotic curve, that is compensated by an increase in the kyphotic angle at the thoracic spine.Citation14–17 As a result, these biomechanical deviations lead to more kinematic changes during weight bearing activities such as walking, running, climbing, and descending stairs, where the body is subjected to higher forces.Citation18 Studies have shown that individuals with flexible flatfeet exhibit slower walking speedCitation19 and specific alterations in their walking kinematics compared to individuals with normal arches. At the ankle joint, they demonstrate reduced peak dorsiflexion,Citation20,Citation21 plantarflexion,Citation22 and abductionCitation20 angles and increased eversion,Citation21,Citation23 and internalCitation10 and externalCitation21 rotation angles during walking. Moving up to the knee joint, flatfoot individuals show decreased peak extension, external rotation, and knee abduction during walking, as well as increased flexion.Citation20 At the hip joint, they exhibit higher peak values in hip flexion, hip internal rotation, and pelvic rotation with decreased extension and external rotation angles.Citation20,Citation24
Foot orthoses are considered the most commonly prescribed treatment method for controlling excessive pronation of the foot.Citation25,Citation26 These devices realign the collapsed foot arch, allowing for a more normal foot and lower limb function.Citation27 Previous studies have shown that orthotic insoles greatly improve foot alignment and posture, thereby affecting the biomechanics of the lower limbs and reducing both the foot pronation angle and tibial internal rotation.Citation28–30
Several orthotic designs have been investigated across the studies and different designs had different effects on the kinematic data.Citation25,Citation26 For instance, Jafarnezhadgero et alCitation28 investigated the use of forefoot medial posting insoles in patients with flexible flatfeet and found that they could decrease the peak rearfoot valgus movement. Tang et alCitation31 evaluated the impact of medial arch support orthoses on walking kinematics and reported a reduction in ankle and knee internal rotation, as well as knee external rotation angles. A systematic review examining different orthotic designs revealed that insoles with medial postings were the most efficient in terms of controlling calcaneal eversion.Citation25 However, this review indicated that the impact of foot orthoses is still not fully defined in terms of walking kinematics,Citation25 as some studies reported significant reduction in rearfoot eversion,Citation29,Citation32 while others found no difference with the use of foot orthoses.Citation33,Citation34 The variation in findings may be attributed to the different orthotic designs and arch heights used in each study, as suggested by Banwell et al.Citation26
Inverted orthosis is a type of rigid foot orthoses that was designed to aid in controlling high degrees of foot pronation.Citation35 The positive mold of the inverted orthoses is poured with different degrees of inversion compared to the vertical alignment of a standard orthoses.Citation36 According to Blake,Citation35 a 5° of rearfoot varus post is required to achieve a 1° change in the static calcaneal position due to the soft tissue compression of the heel. As a result, a 5° rearfoot correction would require a 25° inverted orthotic device. The rearfoot mechanics of patients treated with both a standard and inverted orthoses were compared, and it was found that the inverted orthoses were more effective in correcting rearfoot pronation than the standard orthotic device.Citation37 Furthermore, inverted orthoses were shown to significantly decrease the inversion moment and work at the rearfoot, and increase knee adduction and abduction moment when compared with standard and no orthoses conditions. Bok et alCitation38 tested the effects of inverted orthoses on the plantar pressure and force in children with flatfeet, and a significant reduction in peak pressure at the medial forefoot and rearfoot was achieved upon the use of the inverted insoles.
Although the inverted technique has been shown to be more effective compared to other designs, the biomechanical effect of these devices is not completely understood. Authors throughout the studies have used different inverted angles,Citation36,Citation39,Citation40 leading to a lack of evidence regarding the optimal angle for patients with flatfeet. To determine the proper angle for prescribing foot orthoses, it is essential to evaluate the different effects of inverted angles. This becomes particularly important considering that patients with flatfeet often experience discomfort and arch irritation when prescribed higher degrees of inverted angle orthoses, leading to poor compliance with foot orthoses.Citation38 Bok et alCitation38 concluded that foot orthoses with a lower inverted angle (ie, 15°) would be more effective, accommodating, and efficient for individuals with flatfeet in terms of plantar pressure distribution. However, despite some insights into plantar pressure, the specific kinematic changes associated with different inverted angles have not been investigated. This indicates the need for a comprehensive three-dimensional analysis of the effect of the inverted orthoses angles on the lower limb kinematics. Such analysis would provide clinicians with a clear justification for determining the most appropriate inverted angles, enhancing the effectiveness of foot orthoses prescription. Moreover, existing literature predominantly focuses on the effects of orthotic devices on foot structure,Citation41–43 with limited attention given to the lower limbs. As a result, the broader biomechanical implications of orthoses remain uncertain. Therefore, the aim of this study was to examine the effect of different inverted angles of foot orthoses on walking kinematics in females with flexible flatfeet. We hypothesized that the three-dimensional kinematics of the lower limb during walking would differ with different orthosis inverted angles and that an inverted angle of 15° or 25° would be most effective for females with flexible flatfeet.
Materials and Methods
Participants
An a priori power analysis using G*power 3.1.0 software revealed that for a statistical power of 0.80 and an effect size of 0.25 with an alpha level of 0.05, a sample size of at least 28 subjects was required.Citation44 Therefore, thirty-one female young adults aged between 18–35 years old, with flexible flatfeet were recruited for this study. Due to the biomechanical characteristics differences between males and females, participants were restricted to females to avoid gender differences.Citation45 Flatfoot was defined when either of the feet had ≥4° valgus of resting calcaneal stance position (RCSP) angle.Citation46 RCSP angle was measured based on RootCitation47 method. Subjects lay prone on a bed parallel to the floor with their feet over the edge of the bed. Three dots were drawn on the upper, middle, and lower sections of the calcaneus and connected together to create a bisection line. Then the subjects stood in a relaxed position with their feet apart and the angle between the bisector of the calcaneus and the vertical line to the ground was measured. Participants were excluded if they had any recent surgeries to the spine or lower limbs, lower limb injury within the previous six months, leg length discrepancy (>1 cm), or history of musculoskeletal or neurological conditions which might impair lower limb movement. Participants with a fixed flatfoot deformity were also excluded from this study. Interested participants underwent an eligibility assessment and were recruited accordingly. This study was approved by the Research Ethics Committee of the University of Sharjah, United Arab Emirates (REC-21-06-15-01-S) and was registered on ClinicalTrials.gov (NCT05316051). The study was conducted in accordance with the principles of the Declaration of Helsinki. All participants provided a signed informed consent after reading an information sheet explaining the study purpose and procedures prior to data collection.
Study Design
A randomized controlled crossover trial was used. Every participant underwent each intervention in a random order [(i) Shoes only, (ii) Foot orthoses with a 15° inverted angle, and (iii) Foot orthoses with a 25° inverted angle]. The control condition was participants walking with their shoes without foot orthoses, and walking with each of the inverted angle orthoses were the treatment conditions. The order in which different conditions were examined was randomized and allocation was concealed by asking each participant to pick an invisible sealed envelope that contains a paper demonstrating the testing order from a bag. All testing was performed in a single day, and a five-minute washout time was used between each condition.Citation3,Citation48,Citation49 Neither the examiner nor the participants could be blind to the testing order since it’s clear whether someone is wearing foot orthoses or not.
Foot Orthoses
Rigid foot orthoses was manufactured based on BlakeCitation35 inverted orthotic technique. This technique aims to invert the rearfoot and pronate the forefoot through the subtalar joint and longitudinal axis of the midtarsal joint in order to straighten the heel back to vertical. The orthotic insoles were designed with two variations: 15° inverted angle and 25° inverted angle ().
Figure 1 Inverted foot orthoses. (A) 15° inverted angle orthoses, (B) 25° inverted angle orthoses.

Gait Analysis
Three-dimensional kinematic data was collected by using a motion-capture system (SMART-DX, BTS Bioengineering, Milan, Italy) composed of 8 infrared cameras set at a frequency of 250 Hz. Initially, anthropometric measurements (ie, height (cm), weight (kg), anterior superior iliac spine (ASIS) breadth (cm), pelvis depth (cm), and leg length (cm)) were taken from all participants and recorded in the software. Then, 22 spherical retro-reflective markers were placed on the subject’s body in correspondence to the anatomical points defined by the “Helen Hayes with Medial Markers” protocol.Citation50 In particular, three upper body markers (7th cervical vertebra, right acromion, and left acromion), three pelvic markers (sacrum, right and left ASIS), and 8 markers on each lower limb (greater trochanter, lateral femoral epicondyle, medial femoral epicondyle, head of fibula, lateral malleolus, medial malleolus, heel, and by the head of the second and third metatarsals). Markers of the foot were applied over corresponding landmarks on the shoes as subjects were wearing their shoes with the orthoses inside, and therefore applying them on the skin was not applicable.
The gait analysis consisted of a standing phase and a walking phase. During the standing phase, the subject conducted one standing trial holding an orthostatic position for five seconds. Then the medial markers (markers on the medial femoral epicondyles and medial malleoli) were removed before starting the walking phase. The walking phase consisted of at least four valid walking trials under three test conditions: with shoes only; with 15° inverted orthoses; and with 25° inverted orthoses, over a 10 m walkway at self-selected comfortable speed. A trial was considered valid when all of the markers on the subject’s body were read during the gait. A five-minute period was used between each condition for familiarization and washout. Data from all trials was processed and analyzed with the Smart Analyzer software (BTS Bioengineering, Milan, Italy), and the lower limb kinematics were computed.
Data Processing
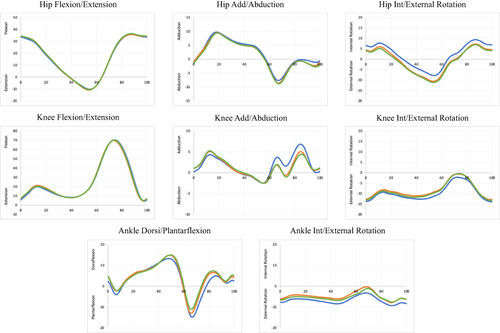
The joint kinematics were normalized as a percentage of the gait cycle (0% being heel contact, and 100% being toe-off). The lower limb kinematic parameters were averaged and produced in the form of graphs in all planes: hip flexion/extension, adduction/abduction, and rotation; knee flexion/extension, adduction/abduction, and rotation; ankle dorsiflexion/plantarflexion, and foot progression. The kinematics were expressed as angles (in degrees) with positive values representing flexion, adduction, internal rotation, and dorsiflexion, while negative values representing extension, abduction, external rotation, and plantarflexion.
From these graphs, the values of the following kinematic variables were calculated and entered into statistical analysis (these variables were selected based on previous studies on gait kinematics of subjects with flexible flatfeet):Citation10,Citation28,Citation51–53 (i) Maximum hip extension angle, (ii) Maximum hip adduction angle, (iii) Maximum hip external rotation angle, (iv) Maximum knee flexion angle during loading response, (v) Maximum knee extension angle during mid-stance, (vi) Maximum knee flexion angle at toe-off, (vii) Minimum knee abduction angle, (viii) Maximum knee abduction angle, (ix) Maximum knee external rotation angle, (x) Maximum knee internal rotation angle, (xi) Maximum ankle plantarflexion angle during loading response, (xii) Maximum ankle dorsiflexion angle during mid-stance, (xiii) Maximum ankle plantarflexion angle at toe-off, (xiv) Maximum ankle external rotation angle, (xv) Maximum ankle internal rotation angle.
Statistical Analysis
Statistical analysis was conducted using the IBM SPSS software, version 28 (IBM Corp., Armonk, NY, USA). Initially, descriptive characteristics were analyzed for the participants and stated as means and standard deviations (SD). The mean values over the four walking trials were calculated for each participant under each of the three test conditions. Data for all participants were averaged to produce a single data set representing the entire sample of 31 participants for each test condition. Normality of data was evaluated by the Shapiro–Wilk Test. As the data were not normally distributed, the Friedman test was used to compare the kinematic variables between the three test conditions. In addition to the median and interquartile range (IQR), the mean and SD of kinematic data were reported to facilitate comparison with existing literature and provide a more comprehensive representation of the data. If significant differences were found (p < 0.05), the Wilcoxon signed-rank test was used, along with post-hoc Bonferroni correction, to identify the differences across test conditions.
Results
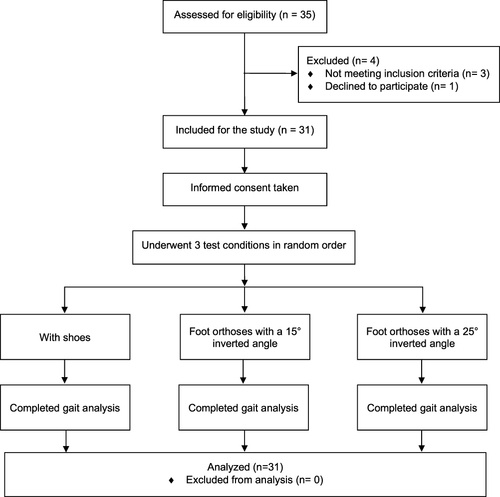
A CONSORT flow diagram of the progress of participants is provided in . A total of 35 individuals underwent eligibility assessment, and 31 were eligible. Participants’ demographic characteristics are summarized in . The mean age of the participants was 21.74 ± 2.49 years old, and the mean body mass index (BMI) was 23.08 ± 4.08 kg/m2.
Table 1 Participant Characteristics (n=31)
Figure 2 Study flowchart.
Kinematic Data
The mean, SD, median, and IQR of the kinematic variables in each test condition are detailed in . The statistical analysis indicated significant differences (p < 0.05) between different test conditions for maximum ankle plantarflexion angle during loading response, maximum ankle dorsiflexion angle during mid-stance, maximum ankle plantarflexion angle at toe-off, maximum ankle external rotation angle, maximum ankle internal rotation angle, and maximum hip external rotation angle. No significant changes were shown in the knee kinematic variables, maximum hip extension angle, and maximum hip adduction angle.
Table 2 Kinematic Variables in Each Test Condition (n=31)
Compared to the shoes only condition, a significant decrease was observed in the maximum ankle plantarflexion angle during loading response (p = 0.002), maximum ankle dorsiflexion angle during mid-stance (p = 0.005), maximum ankle external rotation angle (p < 0.001), and maximum ankle internal rotation angle (p < 0.001) in both orthotic conditions. However, no significant differences were found between the two orthotic conditions with different inverted angles.
In addition, our post-hoc analysis revealed that the maximum ankle plantarflexion angle at toe-off decreased significantly only at a 25° inverted angle compared with the 15° inverted angle (p = 0.001) and shoes only conditions (p < 0.001), yet no significant changes were observed between the 15° inverted angle and shoes only conditions.
Moreover, the maximum hip external rotation angle significantly increased (p < 0.001) in both orthotic conditions compared to the shoes only condition, although no significant changes were observed between the two orthotic conditions with different inverted angles. These changes are presented in , which illustrates the average lower limb kinematics during a walking cycle under the three test conditions.
Figure 3 Average lower limb kinematics. The blue, orange, and green curves represent the values of the shoes-only, 15° inverted angle orthoses, and 25° inverted angle orthoses conditions respectively.
Discussion
This study examined the effect of different foot orthoses inverted angles on walking kinematics in females with flexible flatfeet. Our findings demonstrated that foot orthoses at all tested inverted angles resulted in significant improvements/changes in the maximum hip external rotation angle, as well as several ankle kinematic variables including maximum ankle plantarflexion angle during loading response, maximum ankle dorsiflexion angle during mid-stance, maximum ankle external rotation angle, and maximum ankle internal rotation angle in females with flexible flatfeet compared to the shoes only condition. However, there were no significant differences observed in most of the kinematic variables between the two different inverted angle orthotic conditions.
According to our findings, the ankle joint was the most affected joint by the application of inverted foot orthoses in all measured variables, rather than the knee or the hip joints. Significant changes were found in ankle internal rotation, external rotation, plantarflexion, and dorsiflexion angles. This result is in line with those of previous studies. In the study by Chen et al,Citation51 results showed that custom-made insoles produced significant changes in ankle joint angles but had only minor effects on the knee and hip joints. Similarly, Nester et alCitation42 demonstrated that both medially and laterally wedged orthoses had the greatest effect on the kinematics and moments of the rearfoot complex, while the knee, hip, and pelvis were generally unaffected.
During walking, the ankle joint undergoes specific movements throughout the gait cycle. At heel strike, the ankle joint is initially in a few degrees of dorsiflexion, but it rapidly plantarflexes until the foot is flat on the ground (loading response). This mechanism aids in shock absorption and facilitates the immediate acceptance of body weight during this phase. As the gait cycle progresses, the ankle gradually transitions from plantarflexion to a neutral position and then further into dorsiflexion during the mid-stance phase. Finally, at toe-off, the ankle returns to a plantarflexed position, which assists in propulsion.Citation54,Citation55 The results of this study revealed that using inverted orthoses at both tested angles significantly decreased the maximum ankle plantarflexion angle during loading response and the maximum ankle dorsiflexion angle during mid-stance in adults with flexible flatfeet. This reduction can be attributed to the control of foot motion provided by the orthoses, suggesting a positive impact on foot mechanics by limiting excessive ankle movements. This is particularly relevant for individuals with flatfeet, as excessive ankle motions during flatfooted walking can impair shock absorption and increase stress on the foot structures.Citation9,Citation10 These findings align with previous studies investigating the effects of orthotic insoles on lower limb kinematics in people with flatfeet. Zonouzi et alCitation53 reported reduced ankle plantarflexion and dorsiflexion angles when walking with sandals and medical insoles compared to barefoot walking. Similarly, Chen et alCitation51 observed decreased peak ankle plantarflexion angle and moment when walking with foot insoles in individuals with flatfeet.
However, contrary to our findings, some studies reported that foot orthoses increased the peak ankle dorsiflexion angle during walking.Citation51,Citation56 These contrasting findings highlight the complex nature of ankle kinematics in individuals with flexible flatfeet and the potential influence of various factors such as age, foot morphology, and the severity of the deformity.Citation3 The existing literature presents mixed results and implications regarding ankle dorsiflexion in individuals with flatfeet. One perspective suggests that a flexible flatfoot has a greater range of dorsiflexion and excessive hindfoot eversion, resulting in increased flattening of the medial arch, indicating the need to control ankle dorsiflexion and hypermobility.Citation4,Citation57 Conversely, another viewpoint proposes that the pronated foot with everted hindfoot was compensated by the limited range of motion at the ankle joint, which should be restored.Citation21,Citation22 These discrepancies contribute to conflicting results on ankle dorsiflexion in relation to the use of insoles across various studies. Overall, these findings emphasize the importance of carefully considering individual factors when developing orthotic interventions for individuals with flatfeet. Additionally, age group differences, with studies conducted on children rather than adults, and variations in instrumentation and measurement techniques could also explain the variations in the results.
In this study, we observed contrasting effects between the 15° and 25° inverted angle orthotic conditions on the maximum plantarflexion angle during toe-off. The 25° inverted orthoses significantly reduced the plantarflexion angle compared to the shoes only condition, potentially further restricting ankle motion during push-off. Kerr et alCitation58 explained that the everted ankle position in individuals with flatfeet results in a less stable posture lacking the required rigid lever for effective push-off. To compensate for this instability, individuals with flatfeet tend to reduce and delay hindfoot-tibia plantarflexion to limit the load-bearing requirements of the arch and forefoot.Citation58 Furthermore, a previous study by HaagCitation59 indicated that individuals with low arches have a greater stride velocity and frequency compared to those with normal arches due to diminished dorsiflexion at heel strike and reduced plantarflexion at toe-off. This leads to a shorter stance phase duration, resulting in increased stride velocity and more strides taken per minute, potentially increasing stress on the involved joints.Citation59 Over time, this increased stress could have long-term consequences, possibly causing damage to these joints.Citation59 This suggests that the 25° orthoses, which potentially offer greater pronation control, may further limit the natural ankle plantarflexion motion during the push-off phase, which can adversely affect gait mechanics. On the other hand, although not statistically significant, the maximum plantarflexion angle during toe-off increased with the 15° inverted orthoses compared to the shoes only condition. This suggests that a lower inverted angle might be more accommodating to the natural biomechanics of the foot, providing necessary support while allowing a more natural ankle plantarflexion motion during late stance, promoting a more efficient push-off phase during walking.
Although our findings indicated that the inverted orthoses had a significant effect on the ankle joint kinematics, minimal effects were produced at the knee and hip joints. Several studies in the literature show broad agreement in this regard.Citation42,Citation51 However, since the lower limb acts as a closed kinematic chain, significant angular changes in the ankle joint must lead to alterations in the proximal joints. A possible explanation as suggested by a previous study, is that orthoses might indirectly affect the knee, hip, and pelvis kinematics by altering the proprioception mechanisms involved in regulating muscle function within these joints.Citation60 Another explanation proposed by Lafortune et alCitation61 is that since the knee is not directly affected by the orthoses, compensation for the effects on the foot must occur at the hip joint. This is supported by our findings, where a significant increase in the maximum hip external rotation angle was found in both tested orthotic conditions compared to the shoes only condition. Similarly, Ataabadi et alCitation62 reported an increase in the hip external rotation with foot orthoses in individuals with flexible flatfeet.
The present study had a few limitations that warrant discussion. Since only female adults were included in our study, results cannot be generalized to male adults due to the biomechanical gait differences between both genders. Furthermore, the results presented in this study only provided insight into the immediate effects of foot orthosis with different inverted angles. It is unknown if these effects remain or are likely to change over a longer-term period. Therefore, the long-term effects require further investigation. Another restriction is that we did not use a standardized footwear for all the participants in order to reduce any possible effects of footwear on the findings.
Conclusion
The experimental findings in this study demonstrate that using 15° and 25° inverted angle orthotic insoles resulted in significant changes in ankle joint kinematics during walking in female adults with flexible flatfeet. While both angles showed positive effects, the 25° inverted angle orthotic insoles demonstrated a decrease in the peak ankle plantarflexion angle during the push-off phase, which could lead to inefficient push-off and potentially impact gait mechanics and increase stress on the involved joints during late stance. These observations suggest that a smaller foot orthosis inverted angle may be more effective and feasible for managing flexible flatfeet in female adults.
Data Sharing Statement
All data generated or analyzed during this study were included in the published article. Further inquiries about data resets can be directed to the corresponding author: Professor Fatma A. Hegazy on reasonable request.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We acknowledge all the participants who agreed to participate in this study.
Additional information
Funding
References
- Atik A, Ozyurek S. Flexible flatfoot. North Clin Istanb. 2014;1(1):57–64. doi:10.14744/nci.2014.29292
- Deland JT, De Asla RJ, Sung IH, Ernberg LA, Potter HG. Posterior tibial tendon insufficiency: which ligaments are involved? Foot Ankle Int. 2005;26(6):427–435. doi:10.1177/107110070502600601
- Cheng KW, Peng Y, Chen TLW, et al. A three-dimensional printed foot orthosis for flexible flatfoot: an exploratory biomechanical study on arch support reinforcement and undercut. Materials. 2021;14(18):5297. doi:10.3390/ma14185297
- Saraswat P, MacWilliams BA, Davis RB, D’Astous JL. Kinematics and kinetics of normal and planovalgus feet during walking. Gait Posture. 2014;39(1):339–345. doi:10.1016/j.gaitpost.2013.08.003
- Kirby KA. Longitudinal arch load-sharing system of the foot. Rev Esp Podol. 2017;28(1). doi:10.1016/j.repod.2017.03.003
- Huang YC, Wang LY, Wang HC, Chang KL, Leong CP. The relationship between the flexible flatfoot and plantar fasciitis: ultrasonographic evaluation. Chang Gung Med J. 2004;27(6):443–448.
- Buldt AK, Forghany S, Landorf KB, Levinger P, Murley GS, Menz HB. Foot posture is associated with plantar pressure during gait: a comparison of normal, planus and cavus feet. Gait Posture. 2018;62:235–240. doi:10.1016/j.gaitpost.2018.03.005
- Paton JS. The relationship between navicular drop and first metatarsophalangeal joint motion. J Am Podiatr Med Assoc. 2006;96(4):313–317. doi:10.7547/0960313
- Kim MK, Lee YS. Kinematic analysis of the lower extremities of subjects with flat feet at different gait speeds. J Phys Ther Sci. 2013;25(5):531. doi:10.1589/JPTS.25.531
- Levinger P, Murley GS, Barton CJ, Cotchett MP, McSweeney SR, Menz HB. A comparison of foot kinematics in people with normal- and flat-arched feet using the Oxford Foot Model. Gait Posture. 2010;32(4):519–523. doi:10.1016/j.gaitpost.2010.07.013
- Franco AH. Pes cavus and pes planus: analyses and treatment. Phys Ther. 1987;67(5):688–693. doi:10.1093/ptj/67.5.688
- Khamis S, Yizhar Z. Effect of feet hyperpronation on pelvic alignment in a standing position. Gait Posture. 2007;25(1):127–134. doi:10.1016/j.gaitpost.2006.02.005
- Pinto RZA, Souza TR, Trede RG, Kirkwood RN, Figueiredo EM, Fonseca ST. Bilateral and unilateral increases in calcaneal eversion affect pelvic alignment in standing position. Man Ther. 2008;13(6):513–519. doi:10.1016/j.math.2007.06.004
- Ghasemi MS, Koohpayehzadeh J, Kadkhodaei H, Ehsani AA. The effect of foot hyperpronation on spine alignment in standing position. Med J Islam Repub Iran. 2016;30:466.
- Abdel-Raoof N, Kamel DM, Tantawy S. Influence of second-degree flatfoot on spinal and pelvic mechanics in young females. Int J Ther Rehabil. 2013;20(9):428–434. doi:10.12968/ijtr.2013.20.9.428
- Ingle PV, Puntambekar A. Influence of pronated foot on lumbar lordosis and thoracic kyphosis and Q angle in young adults. Int J Sci Res Publ. 2020;10(6):2250–3153.
- Sdeek F, Shehata S, Hussein M, Elwan MA. Correlation between flexible flat foot and lumbar lordotic angle. Med J Cairo Univ. 2016;84(1):567–572.
- Farokhmanesh K, Shirzadian T, Mahboubi M, Shahri MN. Effect of foot hyperpronation on lumbar lordosis and thoracic kyphosis in standing position using 3-dimensional ultrasound-based motion analysis system. Glob J Health Sci. 2014;6(5):254. doi:10.5539/gjhs.v6n5p254
- Lin CJ, Lai KA, Kuan TS, Chou YL. Correlating factors and clinical significance of flexible flatfoot in preschool children. J Pediatr Orthop. 2001;21(3). doi:10.1097/01241398-200105000-00022
- Marouvo J, Sousa F, Fernandes O, Castro MA, Paszkiel S. Gait kinematics analysis of flatfoot adults. Appl Sci. 2021;11(15):7077. doi:10.3390/app11157077
- Hösl M, Böhm H, Multerer C, Döderlein L. Does excessive flatfoot deformity affect function? A comparison between symptomatic and asymptomatic flatfeet using the Oxford Foot Model. Gait Posture. 2014;39(1):23–28. doi:10.1016/J.GAITPOST.2013.05.017
- Kim HY, Shin HS, Ko JH, Cha YH, Ahn JH, Hwang JY. Gait analysis of symptomatic flatfoot in children: an Observational Study. Clin Orthop Surg. 2017;9(3):363. doi:10.4055/CIOS.2017.9.3.363
- Kothari A, Dixon PC, Stebbins J, Zavatsky AB, Theologis T. The relationship between quality of life and foot function in children with flexible flatfeet. Gait Posture. 2015;41(3):786–790. doi:10.1016/J.GAITPOST.2015.02.012
- Twomey DM, McIntosh AS. The effects of low arched feet on lower limb gait kinematics in children. Foot. 2012;22(2):60–65. doi:10.1016/J.FOOT.2011.11.005
- Desmyttere G, Hajizadeh M, Bleau J, Begon M. Effect of foot orthosis design on lower limb joint kinematics and kinetics during walking in flexible pes planovalgus: a systematic review and meta-analysis. Clin Biomech. 2018;59:117–129. doi:10.1016/j.clinbiomech.2018.09.018
- Banwell HA, Thewlis D, Mackintosh S. Adults with flexible pes planus and the approach to the prescription of customised foot orthoses in clinical practice: a clinical records audit. Foot. 2015;25(2):101–109. doi:10.1016/j.foot.2015.03.005
- Banwell HA, Mackintosh S, Thewlis D. Foot orthoses for adults with flexible pes planus: a systematic review. J Foot Ankle Res. 2014;7(1):23. doi:10.1186/1757-1146-7-23
- Jafarnezhadgero AA, Madadi-Shad M, Alavi-Mehr SM, Granacher U, Padulo J. The long-term use of foot orthoses affects walking kinematics and kinetics of children with flexible flat feet: a randomized controlled trial. PLoS One. 2018;13(10):e0205187. doi:10.1371/journal.pone.0205187
- Telfer S, Abbott M, Steultjens MPM, Woodburn J. Dose-response effects of customised foot orthoses on lower limb kinematics and kinetics in pronated foot type. J Biomech. 2013;46(9):1489–1495. doi:10.1016/j.jbiomech.2013.03.036
- Braga UM, Mendonça LD, Mascarenhas RO, Alves COA, Filho RGT, Resende RA. Effects of medially wedged insoles on the biomechanics of the lower limbs of runners with excessive foot pronation and foot varus alignment. Gait Posture. 2019;74:242–249. doi:10.1016/j.gaitpost.2019.09.023
- Tang SFT, Chen CH, Wu CK, Hong WH, Chen KJ, Chen CK. The effects of total contact insole with forefoot medial posting on rearfoot movement and foot pressure distributions in patients with flexible flatfoot. Clin Neurol Neurosurg. 2015;129:S8–S11. doi:10.1016/S0303-8467(15)30004-4
- Johanson MA, Donatelli R, Wooden MJ, Andrew PD, Cummings GS, Mueller MJ. Effects of three different posting methods on controlling abnormal subtalar pronation. Phys Ther. 1994;74(2):149–161. doi:10.1093/ptj/74.2.149
- Hurd WJ, Kavros SJ, Kaufman KR. Comparative biomechanical effectiveness of over-the-counter devices for individuals with a flexible flatfoot secondary to forefoot varus. Clin J Sport Med. 2010;20(6):428–435. doi:10.1097/JSM.0b013e3181fb539f
- Zifchock RA, Davis I. A comparison of semi-custom and custom foot orthotic devices in high- and low-arched individuals during walking. Clin Biomech. 2008;23(10):1287–1293. doi:10.1016/j.clinbiomech.2008.07.008
- Blake RL. Inverted functional orthosis. J Am Podiatr Med Assoc. 1986;76(5):275–276. doi:10.7547/87507315-76-5-275
- Williams DS, Davis IM, Baitch SP. Effect of inverted orthoses on lower-extremity mechanics in runners. Med Sci Sports Exerc. 2003;35(12):2060–2068. doi:10.1249/01.MSS.0000098988.17182.8A
- Baitch SP, Blake RL, Fineagan PL, Senatore J. Biomechanical analysis of running with 25 degrees inverted orthotic devices. J Am Podiatr Med Assoc. 1991;81(12):647–652. doi:10.7547/87507315-81-12-647
- Bok SK, Lee H, Kim BO, Ahn S, Song Y, Park I. The effect of different foot orthosis inverted angles on plantar pressure in children with flexible flatfeet. PLoS One. 2016;11(7):e0159831. doi:10.1371/journal.pone.0159831
- Munteanu SE, Bassed AD. Effect of foot posture and inverted foot orthoses on hallux dorsiflexion. J Am Podiatr Med Assoc. 2006;96(1):32–37. doi:10.7547/0960032
- Lee HJ, Lim KB, Yoo JH, Yoon SW, Jeong TH. Effect of foot orthoses on children with lower extremity growing pains. Ann Rehabil Med. 2015;39(2). doi:10.5535/arm.2015.39.2.285
- Han KH, Bae K, Levine N, Yang JO, Lee JS. Biomechanical effect of foot orthoses on rearfoot motions and joint moment parameters in patients with flexible flatfoot. Med Sci Monit. 2019;25:5920. doi:10.12659/MSM.918782
- Nester CJ, Van Der Linden ML, Bowker P. Effect of foot orthoses on the kinematics and kinetics of normal walking gait. Gait Posture. 2003;17(2):180–187. doi:10.1016/S0966-6362(02)00065-6
- Vimal AK, Sharma S, Gahlawat B, Pandian G, Sural S. The effect of customized and silicon insoles on mid- and hindfoot in adult flexible pes planovalgus. Indian J Orthop. 2022;56(11):1897–1905. doi:10.1007/S43465-022-00699-0/FIGURES/6
- Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
- Bruening DA, Frimenko RE, Goodyear CD, Bowden DR, Fullenkamp AM. Sex differences in whole body gait kinematics at preferred speeds. Gait Posture. 2015;41(2):540–545. doi:10.1016/j.gaitpost.2014.12.011
- Cho Y, Park JW, Nam K. The relationship between foot posture index and resting calcaneal stance position in elementary school students. Gait Posture. 2019;74:142–147. doi:10.1016/j.gaitpost.2019.09.003
- Root MI. Biomechanical examination of the foot. J Am Podiatry Assoc. 1973;63(1):28–29. doi:10.7547/87507315-63-1-28
- Klein T, Lastovicka O, Janura M, Svoboda Z, Chapman GJ, Richards J. The immediate effects of sensorimotor foot orthoses on foot kinematics in healthy adults. Gait Posture. 2021;84. doi:10.1016/j.gaitpost.2020.11.022
- Klein T, Chapman GJ, Lastovicka O, Janura M, Richards J. Do different multi-segment foot models detect the same changes in kinematics when wearing foot orthoses? J Foot Ankle Res. 2022;15(1). doi:10.1186/s13047-022-00574-z
- Davis RB, Õunpuu S, Tyburski D, Gage JR. A gait analysis data collection and reduction technique. Hum Mov Sci. 1991;10(5):575–587. doi:10.1016/0167-9457(91)90046-Z
- Chen YC, Lou SZ, Huang CY, Su FC. Effects of foot orthoses on gait patterns of flat feet patients. Clin Biomech. 2010;25(3):265–270. doi:10.1016/j.clinbiomech.2009.11.007
- Shih YF, Chen CY, Chen WY, Lin HC. Lower extremity kinematics in children with and without flexible flatfoot: a comparative study. BMC Musculoskelet Disord. 2012;13. doi:10.1186/1471-2474-13-31
- Zonouzi FM, Sadeghi H, Peeri M. The effect of medical insoles on the kinematics of lower-limb joints in people with flexible flatfeet during walking. J Clin Physiother Res. 2020;5(3):e17. doi:10.22037/jcpr.v5i3.32814
- Brockett CL, Chapman GJ. Biomechanics of the ankle. Orthop Trauma. 2016;30(3):232–238. doi:10.1016/j.mporth.2016.04.015
- Pease WS, Bowyer BL, Kadyan V. Human walking. In: DeLisa JA, Gans BM, Walsh NE, editors. Physical Medicine and Rehabilitation: Principles and Practice. 4th ed. Vol. 1. Lippincott Williams & Wilkins; 2005:1926.
- Hsu CY, Wang CS, Lin KW, Chien MJ, Wei SH, Chen CS. Biomechanical analysis of the flatfoot with different 3D-printed insoles on the lower extremities. Bioengineering. 2022;9(10):563. doi:10.3390/BIOENGINEERING9100563
- Needleman RL. Current topic review: subtalar arthroereisis for the correction of flexible flatfoot. Foot Ankle Int. 2005;26(4):336–346. doi:10.1177/107110070502600411/ASSET/IMAGES/LARGE/10.1177_107110070502600411-FIG5.JPEG
- Kerr CM, Zavatsky AB, Theologis T, Stebbins J. Kinematic differences between neutral and flat feet with and without symptoms as measured by the Oxford foot model. Gait Posture. 2019;67:213–218. doi:10.1016/J.GAITPOST.2018.10.015
- Haag MJ. The Effect of Arch Height on Variances in Gait Phases: A Kinematic Analysis. University of Northern Iowa; 2019.
- Stacoff A, Reinschmidt C, Nigg BM, et al. Effects of shoe sole construction on skeletal motion during running. Med Sci Sports Exerc. 2001;33(2):311–319. doi:10.1097/00005768-200102000-00022
- Lafortune MA, Cavanagh PR, Sommer HJ, Kalenak A. Foot inversion-eversion and knee kinematics during walking. J Orthop Res. 1994;12(3):412–420. doi:10.1002/jor.1100120314
- Ataabadi PA, Abbassi A, Letafatkar A, Vanwanseele B. The effects of foot orthosis and low-dye tape on lower limb joint angles and moments during running in individuals with pes planus. Gait Posture. 2022;96. doi:10.1016/j.gaitpost.2022.05.024