
Abstract
Background
The incidence of cancer is increasing, and cancer survivors are also growing exponentially. Cancer is defined as a new chronic disease. Nevertheless, the management of cancer in the form of chronic diseases in China is still in its infancy, without a standardized care model.
Objective
This study aimed to explore the current status of management of cancer care from the patient’s perspective.
Methods
This cross-sectional study was a questionnaire survey of patients diagnosed with cancer, including information of the current situation of daily medical consultation, status of comorbidity, and expectations of seeking cancer care in future. Chi-square test and logistic regression analysis were used to explore the factors influencing patients’ choice of cancer management mode.
Results
A total of 200 cancer patients were included in the study. The majority (n = 150) of cancer patients chose an oncologist in a tertiary hospital for cancer care. Difficulty in registration (45%), time-consuming (34.5%), repeated examinations (34.5%) and different treatment opinions (12.0%) were the main difficulties they encountered currently during tertiary hospital visits. In community hospital, lack of trust in general practitioners (n = 33) and the necessary drugs or testing items in community hospitals (n = 47) were the main difficulties during their visits. Logistic regression analysis showed that male (OR = 2.737, 95% CI, 1.332–5.627, p = 0.006) and elderly patients (OR = 3.186, 95% CI, 1.172–8.661, p = 0.023) were more likely to choose general practitioners (GPs) in community hospitals. Twenty-nine (14.5%) patients hope to have an integrated multidisciplinary management in tertiary and community hospitals with the active participation of GPs for cancer care.
Conclusion
Improving drug availability, equipment and quality of cancer care services can help to increase cancer patients’ recognition of community hospital. In addition, the multidisciplinary management integrated tertiary hospitals and communities with the participation of GPs is a worth exploring mode that improves the management of cancer care.
Introduction
In recent years, the incidence of cancer has significantly increased globally. In developed countries, for example, approximately half of all North Americans will be diagnosed with cancer at some point of their lifetimes.Citation1 This situation is even more severe in China. According to the Cancer Statistics 2023, cancer incidence and mortality rates of China rank first in the world. In China, there were 4.57 million newly diagnosed cancer patients, accounting for 23.7% of the world’s total, and 3 million cancer deaths, accounting for 30% of cancer deaths in 2020.Citation2 These have become an important public health problem for China. World Health Organization (WHO) has categorized cancer as a chronic disease, and the management of cancer is now a slow and progressive.Citation3
Cancer survivor is defined as an individual who has completed curative-intent therapy, need ongoing care on surveillance, prevention of adverse treatment-related effects and maintenance treatments.Citation4 In recent years, patients living with incurable cancer and living for years with chronic treatments were considered to the new survivor population. From this perspective, cancer has the characteristics of chronic diseases, that are developed slowly, last a long time (from months to years), be incurable, and be progressive and/or life-limiting.Citation5 Owing to improved screening, early detection and improved treatment modality, the number of cancer survivors grows exponentially in developed countries. There was estimated 18 million cancer survivors in the United States by 2022.Citation6 In Canada, 63% of patients diagnosed with cancer were expected to survive for five or more years.Citation1 According to the Norwegian Cancer Registry, in 2020, the relative 5-year survival of all cancer patients was about 77%.Citation7 This poses enormous demands on the healthcare system. Therefore, a series of guidelines for chronic disease management mode for cancer patients have been issued in developed countries. The influential US Institute of Medicine report from 2006 emphasized four broad goals that the follow-up of cancer patients should provide: 1) prevention of recurrent and new cancers, and of the late effects of cancer treatments; 2) surveillance for cancer recurrence or other cancers and possible late effects; 3) interventions to deal with consequences, such as symptoms, distress and concerns related to practical issues such as return to work; and 4) coordination between all providers to ensure that survivors’ needs are met.Citation8 In Australia, there were principles of Cancer Survivorship by Cancer Australia, and recommended Models of Cancer Survivorship Care by Clinical Oncology Society of Australia (COSA).Citation9
General practitioners (GPs) are known as the health gatekeepers of the community residents.Citation10 The concept of GPs’ service emphasizes patient-centered, family-based, community-based, prevention-oriented, and provides continuous, comprehensive, accessible and coordinated and holistic care for patients. The long-term management of cancer participated by GPs in community hospitals plays an important role in the whole process of cancer diagnosis and treatment.Citation11,Citation12 Furthermore, the GPs played a very important role in the management of cancer comorbidities,Citation13 a disease status that needed coordinated and holistic care. In developed countries, a series of guidelines for chronic disease management mode for cancer patients have been issued, which all emphasize the important role of GPs. The geriatric multidisciplinary integration team (GIT) was the chronic disease management mode emerging in the 1990s. This mode underlines holistic management of patients, and emphasizes the dominant position of geriatric medicine and GPs, which has been used in the management of chronic diseases such as cancer.Citation14 In Australia, a series of guidelines for chronic disease management mode for cancer patients also emphasize the important role of GPs. For example, the long-term management of breast cancer patients was recommended to be conducted together by oncologists and GPs through shared post-treatment care.Citation15,Citation16 Studies also showed that cancer survivors could be managed safely and effectively by GPs.Citation17
In China, due to the relatively slow and backward development of community hospitals, there is a significant gap in their service capabilities compared to developed countries. Patients can freely choose health care facilities without being referred by community general practitioners. This results in overcrowding in higher-level hospitals and low utilization of primary care facilities, and undermines the effectiveness and efficiency of the health system.Citation18 In order to solve the above problems, China has been committed to strengthening the service level of community hospitals, improving the hardware facilities configuration of community hospitals, and cultivating general practitioners in recent years.Citation19 China has introduced a policy to establish a general practitioner department in comprehensive tertiary hospitals, whose main function is to cultivate more qualified general practitioners for community hospitals. In recent years, community hospitals have improved their ability to manage chronic diseases such as hypertension, diabetes, stroke, chronic obstructive pulmonary disease and other common diseases.Citation20 However, the management of cancer in the form of chronic diseases in China is still in its infancy, without an accepted and effective care model. Even in Guangzhou, a first-tier city in China, cancer has not yet been included in the standard community chronic disease management. There are few studies on the management of cancer, let alone those involving GPs, and fewer rare clinical studies focusing on the patients’ perspective on current situation in cancer management as a chronic disease.
This study aimed to explore the current status of management of cancer from the patient’s perspective and provide clinical basis for exploring a more optimal management model from the general practitioner’s (GP) point of view and how GP could be integrated into the cancer care management in the future.
Methods
Patients
This study was a cross-sectional questionnaire, which included the cancer patients attending the inpatient or outpatient clinic from different departments in Sun Yat-sen Memorial Hospital, and the questionnaire collection was completed electronically from March 2023 to November 2023. Inclusion criteria included age >18 years old, diagnosed with cancer /malignant tumor, understood and finished the questionnaire by themselves or with help of family members. Exclusion criteria included the patients who refuse to participate. Informed consent was obtained from patients throughout the course of the questionnaire. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the ethics committee of Sun Yat-sen Memorial Hospital (SYSKY-2023-850-01).
Questionnaire
The questionnaire covered three major parts, with 15 items in total.
1) The first part was informed notification and filling instructions.
2) The second part was the basic information of patients, which included gender, age, educational background, type of medical insurance, the type of cancer, comorbidity.
3) The third part is the current status of cancer management and the patients’ expectation of cancer care in future. The detailed questionnaire information was shown in supplement file.
Statistical Analysis
We analyzed the data of the questionnaire, summarized the responses to the different questions, and described them by the number of cases (percentage). The percentage was compared with the chi-square test. In the multivariate logistic regression analysis, age, educational background, and medical insurance type were transformed into binary data, and then included in the independent variables for analysis. OR value indicated the risk ratio, and p-values <0.05 were considered statistically significant.
Results
Participant Characteristics
A total of 200 patients diagnosed with cancer were included. The largest number was breast cancer cases (n = 92), followed by hepatobiliary pancreatic malignant tumor (n = 32), gastric-colorectal cancer (n = 27), lung cancer (n = 11), urinary system tumor (n = 7), gynecological system tumor (n = 12), thyroid cancer (n = 5), nasopharyngeal carcinoma (n = 2), lymphoma (n = 2), and other malignant tumors (n = 10), including melanoma, sarcoma, oral cancer, etc. Fifty-six of the 200 patients had comorbidity, the most common of them were endocrine and metabolic system (n = 31), cardiovascular system (n = 18), digestive system (n = 15), chronic obstructive pulmonary disease (n = 5), osteoarthritis (n = 4), and neuropsychological (n = 3). The results are shown in .
Table 1 Characteristics of Patients Who Completed the Questionnaire (n = 200)
The Current Status of Cancer Management
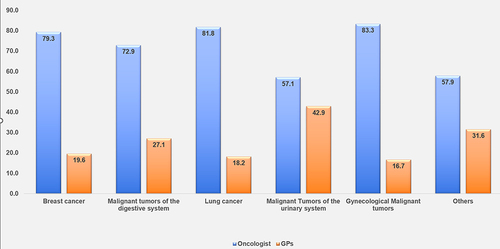
One hundred fifty (75%) patients chose the oncologists in tertiary hospitals for cancer care, while only 47 visited GPs, among which 42 are GPs in tertiary hospitals and five are GPs in community hospitals. There was no significance in the patients’ choice between various cancer type (X2 = 4.171, P = 0.525), as illustrated in . The percentage choice of GPs was highest in malignant tumors of the urinary system, followed by malignant tumors of the digestive system, breast cancer, lung cancer, and gynecological malignant tumors ().
Figure 1 Patient preferences for oncology care based on cancer type. This figure illustrates that patients predominantly preferred oncologists affiliated with tertiary hospitals for cancer treatment across various cancer types. A minority of patients opted for general practitioners within tertiary hospitals. The proportion of patients selecting general practitioners at community hospitals was notably low.
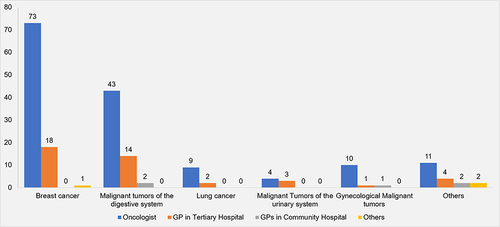
Figure 2 Patients’ choice of oncologist vs GP based on cancer type (%). The figure demonstrated that 57.1–83.3% patients were more inclined to choose oncologist over GP, with only 16.7–42.9% opting for GPs.
When we asked these patients on their expectation on their future management model, 103 patients chose oncologists in tertiary hospitals, 52 patients chose GPs in tertiary hospitals,14 patients chose GPs in community hospitals. Twenty-nine patients anticipated a multidisciplinary and integrated management between tertiary and community hospitals with the active participation of GPs ().
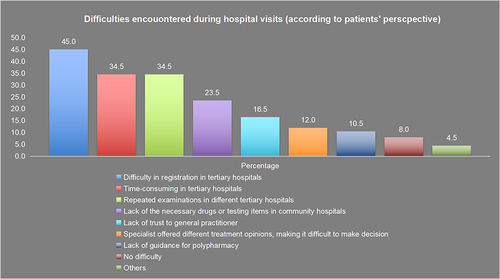
Although cancer patients preferred oncologists in tertiary hospitals for cancer care, they encountered many difficulties during hospital visits. There were 45% patients faced difficulty in registration, resulting from too many patients and scarce specialist physicians in tertiary hospitals, 34.5% patients thought that it was time-consuming, which meant longer waiting time for consultation, examination, getting medication, and treatment in tertiary hospitals and repeated examinations in different tertiary hospitals also resulted in resource waste. In tertiary hospitals, specialists offered different treatment opinions, making it difficult for decision-making (12%). Furthermore, 10.5% patients worried about the lack of guidance for polypharmacy. Lack of the necessary drugs or testing items (23.5%cases) and lack of trust in general practitioner (16.5% cases) were the main difficulties when visiting GPs in community hospitals ().
Figure 3 Challenges encountered during hospital visits from the patients’ perspective. This figure highlights the primary difficulties faced by cancer patients during visits to tertiary hospitals, including cumbersome registration processes, time-consuming procedures, and repetitive examinations. In community hospitals, the main challenges identified by patients include the unavailability of necessary medications or testing items, and a lack of trust in the capabilities of GPs.
Multivariate Logistic Regression Analysis
We then carried out multivariate logistic regression analysis to analyze the factors that influence the patients choose when seeking for cancer care. The choice of hospital for regular follow-up of cancer was related to gender and age. Male patients (OR = 2.737, 95% CI, 1.332–5.627, p = 0.006) and elderly patients (OR = 3.186, 95% CI, 1.172–8.661, p = 0.023) were more inclined to visit GPs, regardless of medical insurance and degree of education, with or without comorbidity (). While in terms of future expectations, older cancer patients were seen to be favoring management mode with participants of GPs in their upcoming cancer care (OR=2.110, 95% CI, 1.010–4.407, p = 0.047) ().
Table 2 Multivariate Logistic Regression Analysis to Analyze Factors That Influenced Patients Seeking General Practitioners (GPs) for Cancer Care
Table 3 Multivariate Logistic Regression Analysis to Analyze Factors That Influenced Patients’ Expectation of Seeking General Practitioners (GPs) in Future for Cancer Care
Discussion
With increasing incidence and mortality, cancer is the leading cause of death in China and has become a major public health problem.Citation21 With the growing of aging and the significant improvement of the survival rate of cancer, cancer has been defined as a chronic disease, and cancer care has also become an important content of chronic disease management. This study was a cross-sectional questionnaire study from the perspective of cancer patients to explore the current status and difficulties of management in cancer patients from patients’ point. In total, 200 patients were included in the present study, including 56 patients with cancer comorbidity. The study found that majority (75%) of cancer patients chose oncologists in tertiary hospitals for regular follow-up of cancer, even if they were facing many difficulties. Patients expressed lack of trust in GPs, worried about the lack of medical equipment for diagnosis and treatment in community hospitals. Currently, compared with female and middle-aged patients, male and elderly patients are more inclined to choose community hospitals for cancer care. Elderly patients are more expected to visit GPs for cancer care in community hospitals in future. From the patient’s perspective, the multidisciplinary management integrated tertiary hospitals and communities with the participation of GPs was worth exploring from patients’ perspective.
The types of cancer reported in this study were most common in breast cancer, followed by hepatobiliary pancreas, gastric, colorectal, and lung cancer, which was in line with the cancer types reported by cancer data in China.Citation21 In our present study, 56 patients had cancer comorbidity (accounted for 28%), which was lower than previously reported. Previous studies reported the proportion of patients with advanced prostate cancer suffering from one or more chronic diseases was 82%.Citation22 Williams reported 539 elderly cancer patients, of which 92% had one chronic disease.Citation23 The reason may be a higher proportion of non-elderly patients under 60 years of age in the present study (76.5%). Furthermore, the identification of comorbidity in the present study was patient self-report, and there might be information gaps. The common comorbidities were endocrine and metabolism, cardiovascular system, digestive system disease, chronic obstructive pulmonary disease, osteoarthritis, and neuropsychology, which were similar to the results of previous studies.Citation24 A meta-analysis divided the included comorbidities into three major patterns, namely cardiovascular and metabolic diseases, mental health problems and musculoskeletal muscle disorders and classified cancer into patterns of mental health problems with an incidence of 100%.Citation25 The most common chronic comorbidities in breast cancer patients are muscle and joint bone disease, gastrointestinal disorders, diabetes, and hypertension.Citation26 Diabetes, peptic ulcer and previously reported malignancies were the top 3 common comorbidities in patients with colon cancer.Citation27 The existence of cancer comorbidity was an important reason for frequent medical visits, higher medical expenses, lower quality of life and poorer prognosis of cancer patients. Thus, cancer patients with comorbidity needed coordinated and holistic care, which was the expertise and characteristics of GPs.
The results of this study showed that currently, cancer patients preferred visiting oncologists in tertiary hospitals to GPs in community hospitals both in treatment and follow-up period (shown in ). This phenomenon was different from previous studies. A survey from Germany pointed to the importance of the GP during cancer therapy from the patient’s point of view, and patients wanted their GP to take an active part in the cancer therapy.Citation28 The above survey suggested that 71% had visited the GP during cancer therapy, and the most relevant reasons to visit the GP during cancer therapy were to get a blood test (63.3%), comorbidities (42.7%) and complaints and side effects (38.3%). The current inadequate level of chronic disease management for cancer in community hospitals of China might be the main reason. In the present study, patients considered that the ability of GPs in community hospitals was insufficient professional and technical level, hence showed not full trust of them. Furthermore, the facilities of diagnosis and treatment in community hospitals were defective, which was also the patients’ concern. The treatment of cancer patients with comorbidities should include many inter-disciplines, such as oncology, nutrition, rehabilitation, psychiatry, etc. These patients often needed multidisciplinary teamwork (MDT) for comprehensive management, which was difficult for GPs in community hospitals currently. A cross-sectional survey study from Changchun in China suggested that residents with chronic disease were more likely to have a usual source of community health service.Citation29 Another study reviewed the factors influencing choice of health system access level in China and suggested that improving drug availability, equipment and perceived quality of primary care services could improve the use of primary care facilities.Citation18 Therefore, how to improve the cancer management ability of community hospitals was the key point to solving the above problems.
Figure 4 The current model of cancer management in southern China vs the proposal model in our study. Currently, cancer patients in southern China are mainly managed by oncologists. In the future, we expect that GPs could play a more active role in cancer management, such as deal with mild side effects, comorbidity, psychological counselling, monitoring recurrence or referral.
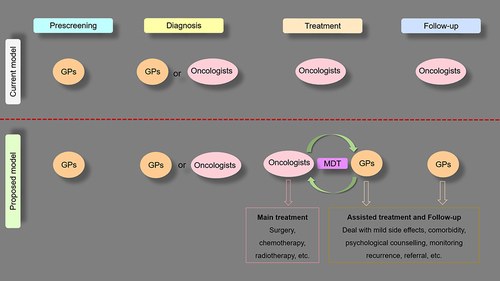
GPs played a very important role in the whole process of diagnosis and treatment of cancer, including cancer screening, diagnosis, evaluation and dealing with treatment side effects, follow-up and monitoring of cancer survivors.Citation30 Participants of GPs could reduce the workload of specialized physicians in tertiary hospitals and relieve overcrowding in tertiary hospitals, which was benefit for reducing delay in registration and remission of time-consuming. However, because the treatment details about cancer patients in tertiary hospitals often could not be well conveyed to community hospitals,Citation31 there was an information disconnect between tertiary hospitals and community hospitals, which was not conducive to the effective and accurate management of cancer patients by GPs. Some scholars have shown that the multidisciplinary teamwork (MDT) management mode of cancer patients with a primary care representative could fill the gap between superior hospitals and the community and strengthen the connection between them, so as to improve the management of cancer in community hospitals.Citation32 Another study recommended the application of multidisciplinary care mode combined specialists with general practitioners in the management of breast cancer. In the present study, part of patients also proposed the comprehensive management mode of linkage between community hospitals and general hospitals, which may be a preferred chronic disease management mode adapted to the current national conditions of China at this stage. GPs should fully consider the patient’s needs and make an effort to explore the feasibility and effectiveness of the MDT management mode integrating tertiary hospitals and communities with the participation of GPs in the future study, in order to improve their survival prognosis and quality of life. shows the above MDT management mode, with a higher expectation on GPs to play a more active role in cancer management, such as dealing with mild side effects, comorbidity, psychological counselling, monitoring recurrence, and referral.
In the present study, patients raised the current problems during the tertiary hospitals’ visits, such as difficult to register, time-consuming, repeated examinations, wasting medical resources, and polypharmacy. China has a population of 1.4 billion, so medical resources are very scarce. Due to the relatively slow and backward development of community hospitals in China, there is a significant gap in their service capabilities compared to developed countries. In China, patients can go to a tertiary hospital of their choice, without the need to be referred by community GPs. These results in overcrowding in higher tier hospitals. Due to the large number of patients visiting tertiary hospitals and shortage of physicians, it is difficult for patients to register, and the waiting time for consultation and examination queues are too long.Citation18 In fact, these were common problems in the management of other chronic diseases,Citation33 but these issues might be more prominent in cancer management, due to the specificity of tumor treatment. At the present stage, China has formulated a hierarchical diagnosis and treatment mode of chronic diseases with
First diagnosis at the grass-roots level, Both-way referral, Separate treatment for urgent and slow diseases, and Connection of higher and lower-level hospitalsCitation34,
Conclusion
Cancer patients preferred choosing oncologists in tertiary hospitals than GPs in community hospitals for follow-up of cancer currently, even if they were facing many difficulties during visits in tertiary hospitals. Our survey indicated that there is a lack of drugs and equipment in community hospitals, which could be the reason why some patients did not fully trust GPs in the community hospitals. These will be the aspects that need improvement in the future. Our study suggested that we need a new management model of cancer care, to meet the medical demands of a large number of cancer patients in China. Improving drug availability, equipment and quality of cancer care services can help increase cancer patients’ recognition of community hospitals. In many instances, GPs could be the bridge between community hospitals and tertiary hospitals. Multidisciplinary management integrating tertiary hospitals and communities with the participation of GPs was a worth exploring mode for cancer care.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgment
This work was supported by the 111 Project (No. B20062), the Science and Technology Program Project Foundation of Guangzhou (No. 2022-01-01-04-3001-0003), Guangzhou Bureau of Basic Science Grant (202201010856) and the “Three million for Three Years” Project of the High-level Talent Special Funding Scheme of Sun Yat-sen Memorial Hospital (132090023).
References
- Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. CMAJ. 2020;192(9):E199–E205. doi:10.1503/cmaj.191292
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
- World Health Organization. Policies and managerial guidelines for national cancer control programs. Rev Panam Salud Publica. 2002;12(5):366–370. doi:10.1590/S1020-49892002001100015
- Pituskin E. Cancer as a new chronic disease: oncology nursing in the 21st Century. Can Oncol Nurs J. 2022;32(1):87–92.
- Nasmith L, Kupka S, Ballem P, et al. Achieving care goals for people with chronic health conditions. Can Fam Phys. 2013;59(1):11–17.
- Henley SJ, Ward EM, Scott S, et al. Annual report to the nation on the status of cancer, part I: National cancer statistics. Cancer. 2020;126(10):2225–2249. doi:10.1002/cncr.32802
- Cancer Registry of Norway. Cancer in Norway 2020 - Cancer Incidence, Mortality, Survival and Prevalence in Norway. Oslo: Cancer Registry of Norway; 2021.
- Ganz P. From cancer patient to cancer survivor: lost in transition. In: an American Society of Clinical Oncology and Institute of Medicine Symposium. The National Academies Press; 2006.
- Vardy JL, Chan RJ, Koczwara B, et al. Clinical Oncology Society of Australia position statement on cancer survivorship care. Aust J Gen Pract. 2019;48(12):833–836. doi:10.31128/AJGP-07-19-4999
- Bi YN, Liu YA. GPs in UK: From health gatekeepers in primary care to health agents in primary health care. Risk Manag Healthc Policy. 2023;16:1929–1939. doi:10.2147/RMHP.S416934
- Dodd N, Henley SJ, Ward EM, et al. Testing the effectiveness of a general practice intervention to improve uptake of colorectal cancer screening: a randomised controlled trial. Aust N Z J Public Health. 2019;43(5):464–469. doi:10.1111/1753-6405.12913
- Jefford M, Koczwara B, Emery J, et al. The important role of general practice in the care of cancer survivors. Aust J Gen Pract. 2020;49(5):288–292. doi:10.31128/AJGP-10-19-5133
- Fidjeland HL, Vistad I, Gjelstad S, et al. Exploring why patients with cancer consult GPs: a 1-year data extraction. BJGP Open. 2019;3(4). doi:10.3399/bjgpopen19X101663
- Fulmer T, Hyer K, Flaherty E, et al. Geriatric interdisciplinary team training program: evaluation results. J Aging Health. 2005;17(4):443–470. doi:10.1177/0898264305277962
- Druel V, Gimenez L, Paricaud K, et al. Improving communication between the general practitioner and the oncologist: a key role in coordinating care for patients suffering from cancer. BMC Cancer. 2020;20(1):495. doi:10.1186/s12885-020-06993-0
- Schutze H, Chin M, Weller D, et al. Patient, general practitioner and oncologist views regarding long-term cancer shared care. Fam Pract. 2018;35(3):323–329. doi:10.1093/fampra/cmx105
- Emery JD, Shaw K, Williams B, et al. The role of primary care in early detection and follow-up of cancer. Nat Rev Clin Oncol. 2014;11(1):38–48. doi:10.1038/nrclinonc.2013.212
- Liu Y, Kong Q, Yuan S, et al. Factors influencing choice of health system access level in China: a systematic review. PLoS One. 2018;13(8):e0201887. doi:10.1371/journal.pone.0201887
- Li X, Lu J, Hu S, et al. The primary health-care system in China. Lancet. 2017;390(10112):2584–2594. doi:10.1016/S0140-6736(17)33109-4
- Yu Y, Ye A, Chen C, et al. The impact of family doctor system on patients’ utilisation of general practitioner in primary care facilities-Evidence from Hangzhou, China. Int J Health Plann Manage. 2022;37(6):3089–3102. doi:10.1002/hpm.3540
- Qiu H, Cao S, Xu R. Cancer incidence, mortality, and burden in China: a time-trend analysis and comparison with the United States and United Kingdom based on the global epidemiological data released in 2020. Cancer Commun. 2021;41(10):1037–1048. doi:10.1002/cac2.12197
- Benzo RM, Moreno PI, Fox RS, et al. Comorbidity burden and health-related quality of life in men with advanced prostate cancer. Supp Care Can. 2023;31(8):496. doi:10.1007/s00520-023-07962-6
- Williams GR, Deal AM, Lund JL, et al. Patient-reported comorbidity and survival in older adults with cancer. Oncologist. 2018;23(4):433–439. doi:10.1634/theoncologist.2017-0404
- Hu Y, Wang Z, He H, et al. Prevalence and patterns of multimorbidity in China during 2002-2022: a systematic review and meta-analysis. Ageing Res Rev. 2024;93:102165. doi:10.1016/j.arr.2023.102165
- Prados-Torres A, Calderón-Larrañaga A, Hancco-Saavedra J, et al. Multimorbidity patterns: a systematic review. J Clin Epidemiol. 2014;67(3):254–266. doi:10.1016/j.jclinepi.2013.09.021
- Topaloglu US, Ozaslan E. Comorbidity and polypharmacy in patients with breast cancer. Breast Canc. 2020;27(3):477–482. doi:10.1007/s12282-019-01040-8
- Gheybi K, Buckley E, Vitry A, et al. Occurrence of comorbidity with colorectal cancer and variations by age and stage at diagnosis. Can Epidem. 2022;80:102246. doi:10.1016/j.canep.2022.102246
- Lang V, Walter S, Fessler J, et al. The role of the general practitioner in cancer care: a survey of the patients’ perspective. J Cancer Res Clin Oncol. 2017;143(5):895–904. doi:10.1007/s00432-017-2343-4
- Zhang L, Li J, Ma T, et al. Usual source of care and experiences with primary care among community health service centre patients in Changchun, China: a cross-sectional survey. Health Soc Care Comm. 2020;28(6):1979–1988. doi:10.1111/hsc.13009
- Sarfo MC, Bertels L, Frings-Dresen MHW, et al. The role of general practitioners in the work guidance of cancer patients: views of general practitioners and occupational physicians. J Cancer Surviv. 2023;17(2):416–424. doi:10.1007/s11764-022-01211-1
- Fairweather L, Tham N, Pitcher M. Breaking the general practice-hospital divide: engaging primary care practitioners in multidisciplinary cancer care. Asia Pac J Clin Oncol. 2021;17(5):e208–e211. doi:10.1111/ajco.13435
- Cancer Australia. Cancer Australia Statement - Influencing Best Practice in Breast Cancer. Cancer Australia, Surry Hills, NSW; 2016.
- Wang Y, Li X, Jia D, et al. Exploring polypharmacy burden among elderly patients with chronic diseases in Chinese community: a cross-sectional study. BMC Geriatr. 2021;21(1):308. doi:10.1186/s12877-021-02247-1
- The guiding opinions of the general office of the state council on promoting the construction of the hierarchical medical system. Gazette Stat Coun People’s Repub China. 2015; 2015(27).