
Abstract
Background
Access to safe drinking water, sanitation, and hygiene (WASH) facilities is crucial for health and human rights, impacting nutrition and weight.
Methods
Multiple Indicators Cluster Survey (MICS) 2017–18 has been used in this study to examine the association between WASH and underweight, alongside other factors. Analysis included descriptive statistics, association tests, logistic regression, and population-attributable fractions (PAF).
Results
According to results child were 1.8, 1.1 and 1.04 times less likely to be underweight if they had access to improved source of drinking water, improved sanitation and hygiene facilities respectively. The likelihood of child being underweight reduces by 1.4, 1.89, 2.01 and 2.55 times if the household wealth status increases from poorest to second, middle, fourth and richest wealth quintiles, respectively. As the mothers’ education level increases from no schooling to primary, middle, secondary, and higher level, the possibility of child being underweight reduces by 1.22, 1.24, 1.60 and 2.01 times, respectively. Moreover, the likelihood of a child being underweight decreases as the education level of the household head improves. If maternal age is less than 20 or more than 35 years the likelihood of the child being underweight is increased by 1.074 and 1.121 times, respectively. A child is 1.1 times more likely to be underweight if birth spacing is less than 2 years. A child’s risk of being underweight decreases by 1.1 times if they have not experienced diarrhea. A child who has never been breastfed has 1.3 times higher risk of being underweight. The results of Population Attributable Fraction (PAF) indicate that holding the other factors constant, approximately 36.46% burden of underweight was preventable by access to improved drinking water, sanitation, and hygiene practices.
Conclusion
Comprehensive strategy is needed that focuses on improving access to safe drinking water, sanitation infrastructure, and hygiene behaviors.
Introduction
Underweight children pose a significant public health concern worldwide, with profound implications for both individual well-being and societal development. Globally, it is estimated that approximately 149 million children under the age of five are affected by under nutrition, with underweight being a key indicator of this condition. Underweight is defined as low weight-for-age. A child who is underweight may be stunted, wasted or both. In 2022 worldwide the number of under age 5 stunted children has been 148.1 million, which was 22.3% of total children under age 5. Nearly all children affected lived in Asia (52% of the global share) and Africa (43% of the global share). In 2022, an estimated 45 million children under 5 (6.8%) were affected by wasting.Citation1 In Pakistan, the issue is particularly acute, with a considerable portion of the population experiencing inadequate access to water, sanitation and hygiene (WASH) facilities. As Pakistan demographic and health survey 2017–18, 23% of all children under 5 are underweight.Citation2 As per UNICEF report, 53,000 Pakistani children under five die annually from diarrhoea due to poor water and sanitation. In Pakistan an estimated 70% of households still drink bacterially contaminated water. Twenty-five million people still practice open defecation.Citation3 Hand washing facility on premises with soap and water is available to 60% of the population.Citation4 In Pakistan 57.5% of children are at high risk of poor water and sanitation.Citation5
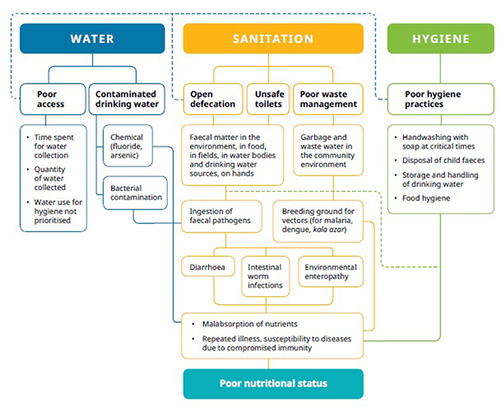
According to estimates, unclean water, poor sanitation, and inadequate hygiene practices cause 50% of malnutrition cases to be accompanied by recurrent diarrhea or intestinal worm infections.Citation6 Lack of access to WASH provision poses a number of health risks, including parasitic diseases, particularly in children, such as diarrhea, which is a major cause of fatality in children aged 1–5 years.Citation7–9 These infections may result in further issues such as anemia, a slowdown in physical growth, and restriction of cognitive development.Citation10,Citation11 WASH score has been linked to malnutrition through various direct and indirect processes. While examining this connection, poor WASH practices (dirty water, inadequate sanitation, and poor hygiene) are directly related to malnutrition, which will cause consumption of fecal-contaminated environmental materials.Citation12 Numerous illnesses, including diarrhea, environmental enteric infections, and intestinal infections, may be caused by its intake. Indirect connections between WASH scores and children’s nutritional status have also been emphasized by.Citation13,Citation14 These connections may include water availability, affordability, and onsite accessibility. Insufficient water supply leads to improper hygiene habits, such as washing hands after urination. illustrates how WASH and underweight are interconnected.
Figure 1 The interlinkages between water, sanitation and hygiene (WASH) and nutrition Adapted from MuraliCdharan (2019).The copyright permission has been obtained from the author, Arundati Muralidharan. Muralidharan A. The interlinkages between water, sanitation and hygiene (WASH) and nutrition. WaterAid India in Health, 9 August 2019. Available from https://www.wateraid.org/in/publications/the-interlinkages-between-water-sanitation-and-hygiene-wash-and-nutrition.Citation15
Since the early twentieth century, improved drinking water supplies, sanitation, and hygiene practices have been emphasized as public health priorities, with a particular focus on the well-being of infants and young children.Citation16 As a result of pioneering work in the nineteenth century by Snow, the subject of public health has emerged as a viable area of study in public policy.Citation17 WASH is regarded as an essential part of public health. Water quantity and quality are important components of WASH. At the point of use, the former concerns the amount of drinking water, whereas the latter concerns the microbiological quality of water. The technology and behavioral strategies used by individuals and organizations to securely confine excrement and avoid human contact are referred to as sanitation. However, hygiene practices involve frequent hand washing with soap (eg, after defecation and before eating). A protective barrier system that prevents human exposure to disease-causing organisms is formed by various public health aspects of WASH.
It is quite concerning that those who lack access to clean water, sanitary conditions, and good hygiene are also among those who experience food insecurity and nutritional deficiencies.Citation18
Unfortunately, children in low- and middle-income nations, notably South Asia, are disproportionately affected, leaving them in the most vulnerable state. According to the World Health Organization (WHO), an estimated 462 million adults and 52 million children under the age of five were underweight globally by 2020.Citation19 The highest prevalence of underweight children was observed in South Asia and sub-Saharan Africa. Pakistan is situated in South Asia, and Punjab is the most populated province in Pakistan, accounting for more than 50% population of the country’s population. There are some studies on the determinants of stunting in Punjab. Several individual, household, and community-level factors have been found associated with stunting. These factors include, age, sex, birth order, and low birth weight, low maternal education, poor wealth status, and lack of access to clean water and sanitation, high poverty rate, low female literacy rate, and lack of access to healthcare.Citation20–22 Although the existing studies in Punjab have used access to clean water and sanitation as determinants of under nutrition, however, there is hardly any study explicitly on the relationship between WASH and underweight in Punjab. Furthermore, neither of the study has considered the importance of hygienic practices in determining underweight either in Pakistan or Punjab. This study is also unique from existing as this study has applied population attributable function to determine the share of WASH in preventing underweight.
Materials and Methods
This study has used latest available data of multiple indicator cluster survey (MICS) 2017–18 for the province of Punjab, Pakistan. Pakistan is the fifth biggest nation in the world contributing 2.81% in the world populace with a population density of 281 people in each km2. The neighbor countries of Pakistan are: India, China, Afghanistan and Iran. Punjab has more than 50% population of the country with approx. 110 Million inhabitants at the time of survey. Multiple Indicator Cluster Survey (MICS) is a household survey program developed by the United Nations Children’s Fund (UNICEF) to assist countries in filling data gaps on the situation of children, men, and women. The MICS is designed to collect data on a range of indicators related to the health, education, child protection, and general well-being. In Punjab, Pakistan, the MICS is typically conducted by the Punjab Bureau of Statistics (PBS) in collaboration with UNICEF and other partners. The sample of the survey is representative up to the district level, with a sample of households selected using a multi-stage cluster sampling approach. It is normally conducted after four years interval and MICS 2017–18 was fifth round of survey since 2004 in Punjab, Pakistan. 51,660 households were surveyed and 74,010 women aged 15–49 were interviewed in MICS, 2017–18. During this survey ethical protocols were followed for consent, voluntary nature of participation and the confidentiality and anonymity of information. In this data set, information on the situation of women, children, and homes in each of Punjab’s 36 districts was available at the household level.Citation23 Underweight was used as a binary dependent variable. provides a detailed description of the variables used in this study.
Table 1 Descriptive Statistics
Results
presents a summary of the responses against each variable taken into consideration in the study. The first column reports the frequencies of the variables, in second column the percentages are given, third column provides the average value followed by standard deviation.
Table 2 Summary of Responses
reports results of association test between underweight and various socio-economic repressors used in study. It is evident form results that except gender all repressors are significantly associated with underweight as shown in .
Table 3 Association Between Underweight and Independent Variables
A logistic regression model was used for the estimation, as the dependent variables were binary in nature, whereas the independent variables were categorically or continuously scaled. presents the results of the regression analysis are reported in . Access to drinking water was the first independent variable, and unimproved access to drinking water was the base category. According to an odds ratio of 0.567 as compared to base category (unimproved access to drinking water), a household’s child is 1.763 (It may be interpreted that “as compared to unimproved access to drinking water, the odds of underweight are 0.567” or alternatively we may convert it in how many times it is less likely by simply dividing the baseCitation1 by given odd ratio 0.567 ie 1/0.567= 1.763. Similar method has been followed where odd ratio has been less than 1) times less likely to be underweight if there is improved access to drinking water. The type of sanitary facility used by households was the following variable: the default category was unimproved sanitation facilities. A child is 1.129 times less likely to be underweight if the household uses improved sanitation facilities, according to the odds ratio associated with improved sanitation facilities (0.885). The odds ratio associated with hygiene practices was 0.96, which indicates that in households where hygiene practices are practiced, the child is less likely to be underweight. Improving hygiene practices such as hand washing with soap has also been associated with reduction in underweight among children.
Table 4 Logistic Regression Results: Dependent Variable = Underweight
The number of household members is found to be statistically significant. The odds ratio for this variable is 0.982, which shows that the likelihood that a child will be underweight decreases as the number of household members increases. Compared to a household head with no education, when the education level of the household head is primary and middle, the child is at the higher risk of being underweight. The associated odd ratios with primary and middle level of housed head education are 1.065 and 1.064 respectively. However, as compared to a household head with no education, when the education level of the household head is secondary and higher, the child is at the lower risk of being underweight. The associated odd ratios with secondary and higher level of housed head education are 0.984 and 0.939 respectively.
One of the key factors influencing underweight has been identified as household wealth status; as household wealth rises from the lowest quintile to the next higher level, the likelihood of a child being underweight continues to decline. The base group comprises households in the lowest or poorest quintile, with odds ratios of 0.710, 0.529, 0.497, and 0.392, respectively. According to data, a child’s risk of being underweight is reduced by 1.40, 1.89, 2.01, and 2.55 times, respectively, depending on whether family belongs to second, middle, fourth, or top quintile of wealth.
Compared to children in urban areas, those in rural households are less likely to be underweight. The child of a rural household had an odds ratio of 0.50, which means that the likelihood that a child will be underweight is two times less.
Under current analysis gender of kid affects underweight, as compared to female children; boys are more likely to be underweight as odd ratio for boys is 1.043.
There is statistically no significant difference between premature and mature child birth for child being at the risk of being underweight.
As compared to children of maternal age from 20–34 years, the children of maternal age above 35 years are 1.121 times more likely to be underweight. Similarly, the children of maternal age below 20 years are 1.074 times more likely to be underweight.
Birth spacing has been identified as a significant predictor of a child being underweight; a child is 1.106 times more likely to be underweight if the birth spacing is less than two years.
Mothers’ educational level has been identified as one of the key factors influencing the possibility that a child will be underweight. As the mother’s educational level increases from no formal education to a higher level, the likelihood of the child being underweight continues to decline. Preschool or no education for mothers was used as the base group. The Odds ratios for mothers with primary, medium, and higher education were 0.819, 0.801, 0.622, and 0.496, respectively. This shows that depending on the mother’s education level (primary, middle, secondary, and higher), the child is 1.22, 1.24, 1.607, and 2.01 times lower likelihood of being underweight, respectively. A child’s risk of being underweight has decreased by 1.11 times if they have not experienced diarrhea, which is a significant predictor of weight loss. Breastfeeding is a significant factor in determining whether a child is underweight, and a child who has never been breastfed has a 1.274 times higher risk of being underweight.
Discussion
A systematic review of studies conducted in low- and middle-income countries also found a significant association between access to improved drinking water and reduced risk of underweight in children. This review identified several mechanisms by which improved water access can lead to reduce under nutrition, including improved hygiene, reduced exposure to water-borne pathogens, and improved overall health.Citation24 The link between improved sanitation access and underweight is likely due to the impact of fecal-oral diseases on child health and nutrition. Poor sanitation can lead to the spread of diseases, such as diarrhea and intestinal worms, which can lead to malnutrition and weight loss in children. Studies have shown that a lack of access to improved sanitation facilities, such as toilets, is associated with underweight children. A study conducted in India found that children living in households without improved sanitation facilities were significantly more likely to be underweight than those living in households with access to such facilities.Citation25 A study conducted in Nepal found that children whose mothers reported washing their hands with soap before feeding their children had a lower prevalence of underweight than children whose mothers did not practice this behavior.Citation26
Compared to a household head with no education, when the education level of the household head is primary or medium, the child is at the higher risk of being underweight. It may due to the reason that the household head with no schooling may lack information regarding nutritious and health care needs of the child and may more likely to follow the instructions of health/nutrition practitioner while household head with primary and middle education may have low information levels, which may lack proper awareness of the nutritional and health care needs of the children at different stages of development. They may try to use their own knowledge and home remedies for child caring. In view of the fact “little knowledge is dangerous” can result in improper health care and inadequate feeding practices, leading to under nutrition among children. The children of house hold head with higher level of education are less likely to be under weight as compared to children whose house hold head has no schooling. The association between household higher education level and being underweight is likely due to a range of factors, including better access to healthcare, improved economic status, and increased knowledge of proper nutritional practices. Education can also lead to better decision making regarding child health and nutrition, which can have a positive impact on child growth and development. Educational programs that focus on proper nutrition practices, healthcare access, and child development can have a significant impact on child health and nutrition, particularly in low- and middle-income countries where education levels are often low.
Household wealth status is an important determinant of child nutrition, with wealthier households better able to access and afford nutritious foods, healthcare, and other basic needs. Several studies have found a significant association between household wealth status and being underweight among children. Household wealth status is also linked to food security, an important factor in child nutrition. A study conducted in Ethiopia found that households with better economic status were more likely to have food securityCitation27 their children were less likely to be underweight than those from poorer households.
Compared to children in urban areas, those in rural households are less likely to be underweight. It may be due to the fact that in rural areas with agricultural economies, households may have access to a wider variety of fresh, locally produced foods, including fruits, vegetables, and grains. A study byCitation28 found that rural children in Ethiopia had greater dietary diversity compared to urban children, potentially due to better access to diverse food sources. Furthermore, urban areas often face environmental challenges such as pollution and overcrowding, which can have negative impacts on child health. In contrast, rural areas may offer cleaner environments and less exposure to pollutants, which can support overall health and well-being. Boys had a higher risk of being underweight compared to girls may be due to biological differences. Boys and girls may have different growth patterns and nutritional requirements, with boys typically exhibiting higher energy needs and growth rates during certain stages of development. A study byCitation29 found that boys generally had higher energy expenditure and metabolic rates compared to girls, potentially increasing their susceptibility to under nutrition if their dietary intake is inadequate. Secondly, Boys may face barriers in accessing healthcare services or may be less likely to receive timely medical care compared to girls. A study byCitation30 found that boys in rural Uganda were less likely to receive appropriate treatment for illnesses compared to girls, which could contribute to poorer nutritional outcomes among boys.
The link between premature birth and being underweight may be due to several factors. Preterm infants may have reduced nutrient stores at birth and may require specialized feeding strategies to support their growth and development. Additionally, preterm infants may be at an increased risk of infection and other health complications that could affect their growth and development. However, in the current study, there was no conclusive evidence that premature birth causes a child to be underweight which may be due to the reason that preterm infants often undergo catch-up growth, a rapid increase in weight and size, particularly during the first few years of life. This phenomenon helps them attain a weight similar to that of full-term infants over time, thereby reducing the disparity in underweight status.Citation31 Ong et al provide evidence in this regard and provide insights into the growth patterns of preterm infants and their long-term health outcomes. Furthermore, preterm infants receive intensive medical care in neonatal intensive care units (NICUs), where they are closely monitored for growth and nutritional status. Healthcare interventions, such as monitoring growth parameters, adjusting feeding strategies, and providing appropriate medical interventions contribute to optimizing the growth and nutritional status of preterm infants.
The link between maternal age and being underweight may be due to several factors. Younger mothers may be less likely to have access to adequate healthcare during pregnancy and may be at a higher risk of poor nutrition and inadequate prenatal care. Additionally, younger mothers may have less knowledge and experience with infant feeding and care practices. Similarly, older mothers may be at an increased risk of chronic health conditions that could affect maternal nutrition during pregnancy, and may have different infant feeding and care practices.
Birth spacing, which is the time interval between consecutive births, can influence a child’s nutritional status, including that of underweight. A short birth interval does not allow sufficient time for the mother to fully recover from the physical and nutritional demands of the previous pregnancy and childbirth. This can lead to maternal health depletion, where the mother’s body has not had adequate time to replenish essential nutrients and regain strength before conceiving again. Consequently, the subsequent child may experience suboptimal intrauterine conditions, affecting their growth and development.Citation32 Conde-Agudelo et al also highlight the association between short birth intervals and adverse perinatal outcomes, including low birth weight. Furthermore, closely spaced pregnancies can impose additional stress and fatigue on the mother, both physically and emotionally. Chronic stress and fatigue can affect maternal health, including nutritional status and the ability to provide optimal care for the subsequent child, potentially contributing to low birth weight.
Maternal education plays a crucial role in reducing the risk of under nutrition among children less than five years of age. Improving maternal education can increase their knowledge of nutrition, health practices, and sanitation, which can positively affect their children’s health and nutritional status.
Citation33 Reveal a significant association between maternal education and the weight status of school-age children. Children of mothers with higher levels of education were found to have lower rates of underweight and higher rates of normal weight compared to children of mothers with lower levels of education. This suggests that maternal education plays a crucial role in determining the nutritional outcomes of children, with higher maternal education being associated with better weight status among school-age children.
The link between diarrhea and underweight can be attributed to the loss of nutrients and electrolytes during diarrhea. This can lead to reduced absorption of essential nutrients, particularly if the child continues to experience diarrhea over a prolonged period. As a result, the child’s growth can be stunted, leading to underweight status. According to a study in Uganda, children with diarrhea are more likely to be underweight.Citation34 Another study conducted in Bangladesh found that children with diarrhea had a significantly higher risk of being underweight than those without diarrhea.Citation35 Breastfeeding provides nutrients necessary for a child’s growth, including proteins, carbohydrates, and healthy fats. Breast milk also contains antibodies that help to protect children from infections and diseases, which can contribute to underweight if left untreated. Breastfeeding duration also plays a critical role in preventing underweight status. Children who are breastfed for an extended period have a lower risk of being underweight than those who are breastfed for a shorter duration.Citation36
Estimating Population Attributable Fractions
To assess the role of the WASH in determining underweight, we determined the population attributable fraction (PAF) introduced by.Citation37 PAF estimates the proportion of underweight that can be attributed to WASH, holding other factors constant. In our case, PAF represents the portion of underweight issues that can be eliminated by the provision of improved drinking water, sanitation, and hygiene to all households across Punjab. PAF results are presented in . PAF analysis demonstrated that a 36.46% burden of underweight is preventable by the provision of improved drinking water, sanitation, and hygiene in Punjab, Pakistan.
Table 5 PAF of WASH of Being Underweight
This study demonstrated strong connections between WASH-related parameters and under nutrition in children under the age of five, both before and after controlling for potential confounders. It has contributed to a better understanding of malnutrition and its causes by evaluating a wide range of variables, such as the household WASH score, education levels of parents, and income levels. Our findings are consistent with earlier research, which highlighted access to clean drinking water and adequate sanitation as crucial defenses against malnutrition and under nutrition in low-income and middle-income countries.Citation38 Similar findings were obtained byCitation39 who examined the connection between child nutrition status and household sanitation.
Conclusion
Given the significance of WASH services for nutrition, we used the MICS (2017–18) to examine the impact of WASH on the nutritional status of children under five in Punjab. Underweight was used to assess the impact of WASH score on children’s nutrition. Along with various control factors, water, sanitation, and hygiene were considered independent variables. Descriptive statistics, association tests, logistic regression and PAF were used in the statistical analysis to find the association between children being underweight and other independent variables. The results indicate that a child is 1.8 and 1.1 times less likely to be underweight, if he/she has improved access to drinking water and sanitation facilitates, respectively. Moreover, the likelihood of a child being underweight decreases as the education level of the household head improves and household wealth status increases. The results further indicate that if maternal age less than 20 years or more than 35 years the likelihood of the child being underweight increases. Birth spacing is a significant predictor of a child’s underweight; a child is 1.1 times more likely to be underweight if birth spacing is less than 2 years. The mothers’ improved educational level influences the possibility that the child will not be underweight. Lastly, a child’s risk of being underweight decreases by 1.1 times if they have not experienced diarrhea, which is a significant predictor of weight loss. This is coupled with the fact that a child who has never been breastfed has 1.3 times higher risk of being underweight than one who has breastfed. According to the PAF findings, 36.46% of the burden of underweight is attributable to WASH, which indicates that 36.46% of the burden of underweight is preventable by the provision of improved drinking water, sanitation, and hygiene practices in Punjab, Pakistan.
Policy Implications
Based on the results of the study, several policy implications can be drawn to address underweight among children: Policymakers should prioritize investments in WASH infrastructure, particularly in areas with poor access. Integrated approaches that combine WASH interventions with nutrition, health, and education programs can yield synergistic effects. Inter-sectoral collaboration among relevant stakeholders, including government agencies, NGOs, and community-based organizations, is essential for implementing comprehensive interventions. Policies aimed at improving access to education, especially for women and girls, can have positive implications for child nutrition. This may involve initiatives such as awareness campaigns and adult literacy programs. Poverty alleviation programs targeting the poorest quintiles can help reduce disparities in nutrition outcomes by improving access to food, healthcare, and education for disadvantaged families. Community-based nutrition programs and outreach initiatives can play a crucial role in reducing child underweight.
Limitations of the Study
The study’s cross-sectional design limits its ability to establish causality. It provides a snapshot of the association between WASH and underweight at a single point in time, but it cannot determine the direction of causality or account for changes over time. Longitudinal data would provide a more comprehensive understanding of the dynamic relationship between WASH and underweight over time. While the study accounts for various socio-economic factors, there may be unmeasured confounding variables that influence the relationship between WASH and underweight.
The Potential Future Research
Future research avenues may be conducting longitudinal studies to track changes in WASH practices, and child nutritional outcomes over time would provide more robust evidence on causality and temporal relationships. Complementing quantitative analyses with qualitative research methods, such as in-depth interviews and focus group discussions, can offer insights into the contextual factors shaping WASH practices and their impact on child nutrition.
Data Sharing Statement
Data used to support the findings of this study are available from the corresponding author upon request.
Ethical Approval
The ethical clearance has been given by institutional review board (IRB) of the institute vide letter no UEV/IRB/2024/0010 dated 2/5/2024.
Disclosure
The authors declare no conflicts of interest in this work.
Acknowledgments
The authors of this study extend their appreciation to the Researchers Supporting Project (project number RSP2024R378) King Saud University,Riyadh, Saudi Arabia, for supporting this study and funding this work.
Additional information
Funding
References
- United Nations Children’s Fund (UNICEF). (2023). Levels and trends in child malnutrition, retrieved from https://data.unicef.org/topic/nutrition/malnutrition/. Accessed May 17, 2024. Accessed 26 april 2024
- National Institute of Population Studies (NIPS) Pakistan demographic and health survey (PDHS) 2017-18 key findings available at https://dhsprogram.com/pubs/pdf/SR257/SR257.pdf. Accessed May 17, 2024
- UNICEF, WASH: Water, sanitation and hygiene Retrieved from https://www.unicef.org/pakistan/wash-water-sanitation-and-hygiene-0. Accessed May 17, 2024. on 23-04,-2024
- Cooper R (2018). Water, sanitation and hygiene services in Pakistan. K4D Report.
- Murtaza F, Muzaffar M, Mustafa T, Anwer J. Water and sanitation risk exposure in children under-five in Pakistan. J Family Comm Med. 2021;28(2):103–109. doi:10.4103/jfcm.jfcm_149_21
- World Health Organization (2022). The double burden of malnutrition. Policy brief. Available at: https://apps.who.int/iris/bitstream/handle/10665/255413/WHONMHNHD-17.3-eng.pdf?ua=1.Last. accessed on October 22, 2023.
- Shrestha SK, Vicendese D, Erbas B. Water, sanitation and hygiene practices associated with improved height-for-age, weight-for-height and weight-for-age z-scores among under-five children in Nepal. BMC Pediatric. 2020;20(1):1. doi:10.1186/s12887-020-2010-9
- Liu L, Johnson HL, Cousens S, et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379 9832:2151–61 doi: 10.1016/S0140-6736(12)60560-1.
- Brooker S, Clements AC, Bundy DA. Global epidemiology, ecology and control of soil-transmitted helminth infections. Adv Parasitol. 2020;62. 221–261.
- Or PP-L, Wong BY-M, Chung JW-Y. To investigate the association between the health literacy and hand hygiene practices of the older adults to help them fight against infectious diseases in Hong Kong. Am J Infect Control. 2020;48 5 485–489 doi: 10.1016/j.ajic.2019.12.021.
- Ziegelbauer K, Speich B, Mäusezahl D, Bos R, Keiser J, Utzinger J. Effect of sanitation on soil-transmitted helminth infection: systematic review and meta-analysis. PLoS Med. 2012;9 1 e1001162 doi: 10.1371/journal.pmed.1001162.
- Dangour AD, Hawkesworth S, Shankar B, et al. Can nutrition be promoted through agriculture-led food price policies? A systematic review. BMJ Open. 2013. 3(6):e002937. Doi:10.1136/bmjopen-2013-002937.
- Riiser K, Helseth S, Haraldstad K, Torbjørnsen A, Richardsen KR. Adolescents’ health literacy, health protective measures, and health-related quality of life during the Covid-19 pandemic. PLoS One. 2020;15 8 e0238161 doi: 10.1371/journal.pone.0238161.
- Manzoni G, Laillou A, Samnang C, et al. Child-sensitive WASH composite score and the nutritional status in Cambodian children. Nutrients. 2019, 11 9 2142 doi: 10.3390/nu11092142.
- Muralidharan A. The interlinkages between water, sanitation and hygiene (WASH) and nutrition. WaterAid India in Health, 9 August 2019. Available from https://www.wateraid.org/in/publications/the-interlinkages-between-water-sanitation-and-hygiene-wash-and-nutrition. Accessed 19 May 2024.
- Hutton G, Chase C. Water supply, sanitation, and hygiene. Mock CN, Nugent R, Kobusingye O, et al. editors. Injury Prevention and Environmental Health, 3rd. Washington (DC). The International Bank for Reconstruction and Development / The World Bank. 2017. Oct. 27. Doi:10.1596/978-1-4648-0522-6_ch9
- Snow J. On the mode of communication of cholera. John Churchill German, WASH network (2017) 2 + 6 = 17 linking WASH and nutrition - A blueprint for Living SDG 17. Paulsenstr. 1855;23:12163. Berlin, Germany.
- World Health Organization. (2021). Malnutrition. Retrieved from https://www.who.int/news-room/fact-sheets/detail/malnutrition. Last accessed on October 22, 2023.
- Unicef Surveys. Available from https://mics.unicef.org/surveys.Last. accessed on October 22, 2023.
- Haq W, Abbas F. A multilevel analysis of factors associated with stunting in children less than 2 years using Multiple Indicator Cluster Survey (MICS) 2017–18 of Punjab, Pakistan. SAGE Open. 2022;12(2):21582440221096127. doi:10.1177/21582440221096127
- Chaudhry TT, Khan M, Mir AS. Gender gaps in child nutritional status in Punjab. Pakistan Develo Rev. 2020;1:1.
- Ponum M, Khan S, Hasan O, et al. Stunting diagnostic and awareness: impact assessment study of sociodemographic factors of stunting among school-going children of Pakistan. BMC Pediatric. 2020;20(1):1–9. doi:10.1186/s12887-020-02139-0
- Bureau of Statistics (BOS) Punjab, available From https://bos.punjab.gov.pk/mics-2017.Accessed 18 May 2024.
- Franse CB, Boelens M, Fries LR, Constant F, van Grieken A, Raat H. Interventions to increase the consumption of water among children: a systematic review and meta-analysis. Obes Rev. 2020;21(7):e13015. doi:10.1111/obr.13015.
- Jadhav A, Weitzman A, Smith-Greenaway E. Household sanitation facilities and women’s risk of non-partner sexual violence in India. BMC Public Health. 2016;16(1):1. doi:10.1186/s12889-016-3797-z
- Adhikari D, Khatri RB, Paudel YR, Poudyal AK. Factors associated with underweight among under-five children in eastern Nepal: community-based cross-sectional study. Front Public Health. 2017;5:350. Doi:10.3389/fpubh.2017.00350
- Tadesse Tantu A, Demissie Gamebo T, Kuma Sheno B, Yohannis Kabalo M. Household food insecurity and associated factors among households in Wolaita Sodo town, 2015. Agri Food Sec. 2017;6(1):1–8. doi:10.1186/s40066-017-0098-4
- Jones AD, Ickes SB, Smith LE, et al. W orld H ealth O rganization infant and young child feeding indicators and their associations with child anthropometry: a synthesis of recent findings. Maternal and Child Nutrition. 2014;10(1):1–17. doi:10.1111/mcn.12070
- Schell LM, Gallo MV, Ravenscroft J. Environmental influences on human growth and development: historical review and case study of contemporary influences. Ann Hum Biol. 2009;36(5):459–477. doi:10.1080/03014460903067159
- Wamani H, Tylleskär T, Åstrøm AN, Tumwine JK, Peterson S. Mothers’ education but not fathers’ education, household assets or land ownership is the best predictor of child health inequalities in rural Uganda. Interna J equ hea. 2004;3(1):1–8. doi:10.1186/1475-9276-3-9
- Ong KK, Kennedy K, Castañeda‐Gutiérrez E, et al. Postnatal growth in preterm infants and later health outcomes: a systematic review. Acta paediatrica. 2015;104(10):974–986. doi:10.1111/apa.13128
- Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Birth spacing and risk of adverse perinatal outcomes: a meta-analysis. JAMA. 2006;295(15):1809–1823. doi:10.1001/jama.295.15.1809
- Feng Y, Ding L, Tang X, Wang Y, Zhou C. Association between maternal education and school-age children weight status: a study from the China health nutrition survey, 2011. Int J Environ Res Public Health. 2019;16(14):2543. doi:10.3390/ijerph16142543
- Omona S, Malinga GM, Opoke R, Openy G, Opiro R. Prevalence of diarrhoea and associated risk factors among children under five years old in Pader District, northern Uganda. BMC Infect Dis. 2023;20(1):37. Doi:10.1186/s12879-020-4770-0.
- Hossain MM, Abdulla F, Rahman A. Prevalence and risk factors of underweight among under-5 children in Bangladesh: evidence from a countrywide cross-sectional study. PLoS One. 2023;18 4 e0284797 doi: 10.1371/journal.pone.0284797.
- Ene-Obong HN, Alozie Y, Abubakar S, Aburime L, Leshi OO. Update of the nutrition situation in Nigeria. North African J Food Nutr Res. 2020;4 9 S63–S74 doi: 10.51745/najfnr.4.9.S63-S74.
- Greenland S, Drescher K. Maximum likelihood estimation of the attributable fraction from logistic models. Biometrics. 1993;49(3):865–872. (). doi:10.2307/2532206
- Sangalang SO, Medina SA, Ottong ZJ, et al. Protocol for a trial assessing the impacts of school-based wash interventions on children’s health literacy, handwashing, and nutrition status in low-and middle-income countries. Int J Environ Res Public Health. 2021;18(1):226. doi:10.3390/ijerph18010226
- Bekele T, Rawstorne P, Rahman B. Effect of water, sanitation and hygiene interventions alone and combined with nutrition on child growth in low and middle income countries: a systematic review and meta-analysis. BMJ open. 2020. 10 7 e034812 doi: 10.1136/bmjopen-2019-034812.