
Abstract
Background
The incidence of visual impairment(VI) in older people is gradually increasing. This review aimed to summarise the evidence on existing health management models and strategies for older adults with VI to improve health-related and vision-related quality of life (QoL) in older people.
Methods
Based on the framework of the scoping review methodology of Arksey and O’Malley (2005), a comprehensive literature search of relevant literature published between January 2010 and June 2022 in PubMed, CINAHL, EMBASE, Web of Science, Cochrane Library, CNKI, VIP, Wanfang database, Sinomed and the grey literature.
Results
Finally, 31 articles were included. The health management model had a multidisciplinary team low vision rehabilitation model, medical consortium two-way management model, low vision community comprehensive rehabilitation model, medical consortium-family contract service model, screening-referral-follow-up model, and three-level low vision care model. The health management strategy covers nine aspects, the combination of multi-element strategies is feasible, and network information technology has also shown positive results.
Conclusion
In the future, under the Internet and hierarchical management model, we should provide demand-based personalized support to rationalize and scientifically achieve hierarchical management and improve resource utilization efficiency and eye health outcomes.
Background
Visual impairment (VI) refers to low vision or a reduced visual field of both eyes caused by various reasons, which cannot or temporarily not restore visual function through multiple drugs, operations, and other treatments so that it is impossible to carry out work, learning or other activities.Citation1 In China, people with disabilities due to blindness and visual loss rank second among all disabilities, second only to hearing loss.Citation2 As of 2020, 43.3 million people in the world were blind, 295 million people had moderate and severe VI, 258 million people had mild VI, and 510 million people had uncorrected near VI due to a lack of reading glasses.Citation3 By 2050, due to the aging population, it is estimated that 61 million will be blind, 474 million people will suffer from moderate and severe VI, 360 million will suffer from mild VI, and 866 million p will suffer from uncorrected near VI.
Due to social and economic development and the increase in average life expectancy in various countries, the burden of diseases is changing from infectious diseases to noninfectious and aging-related conditions. VI has become an urgent and increasingly severe global public health problem.Citation3 According to the seventh national census results, 264.02 million elderly people aged 60 or above, accounting for 18.70% of the total population; there were 190.64 million people aged 65 and above, accounting for 13.50% of the total population.Citation4 The prevalence of presbyopia, cataract, glaucoma, and senile macular degeneration increases rapidly with age.Citation5–7
For the elderly, VI may lead to social isolation,Citation8 limited social activities, and inconvenient walking,Citation9 and the risk of falls and fractures, especially hip fractures, is higher.Citation10,Citation11 VI may also increase other physical challenges, such as cognitive decline,Citation12,Citation13 reduced vision-related quality of life (VRQoL),Citation14 and increased risk of chronic disease and death.Citation15,Citation16 The elderly with VI will also have psychological problems,Citation17 such as anxiety and depression.Citation18,Citation19 The incidence of depression and anxiety of the elderly with VI is twice that of the general elderly.Citation20 For family members and caregivers, it will lead to physical and mental diseasesCitation21 and increase the risk of anxiety and depression.Citation22 Patients with VI will also cause a substantial financial burden to society; for example, they are more inclined to live in nursing institutionsCitation23 and are more likely to move into nursing institutions in advance,Citation24 which increases the burden on nursing institutions. Previous studies have shown that VI also poses a substantial financial burden to the world.Citation25,Citation26
The VI of most elderly people can be prevented and treated.Citation27 Effective intervention measures can significantly reduce or eradicate the VI or reduce or eliminate the related living capacity limitations. Therefore, access to eye care services is a significant risk affecting eye disease development and treatment outcomes.Citation28,Citation29 Health management refers to the monitoring, evaluation, intervention, re-monitoring, re-evaluation, and re-intervention of health risk factors, which is a continuous cycle of movement state, in which intervention to solve health problems is the core.Citation30 The health management model of visual impairment refers to the combination of ophthalmic examination, assessment, rehabilitation, health education, and other ways to carry out systematic, continuous and personalized health services for patients, thereby reducing the recurrence rate and mortality of diseases, improving the survival rate of patients, and improving their quality of life. World Health Organization (WHO) 《World report on vision (2019) 》also proposes to integrate people-oriented comprehensive eye care into the health system.Citation31 Due to aging and changes in lifestyle, the demand for eye care will increase sharply in the next few years. If the demand is unmet elderly people will face the risk of VI.
Health management services are needed to address these issues in older people with VI. Li Shuqin et alCitation32 used conjoint analysis to identify six health management strategies and analyze the preferences of elderly VI patients for different health management services, aiming to assist healthcare providers in tailoring appropriate health management strategies for them. However, the conjoint analysis method has limitations such as a maximum of six attributes and 2–4 levels per attribute, which may not be comprehensive enough to cover all services. This paper adopts the scope review method framework proposed by Arksey and O’Malley et alCitation33 in 2005 and improved by Levac et alCitation34 to comprehensively search the existing research on the health management models and strategies of the elderly with VI, to provide a reference for formulating a management service system for the elderly with VI in the future.
Methods
Identifying the Research Questions
The research questions reviewed in this study are as follows: What were the health management models of the elderly with VI? What were the health management strategies? What was the effect?
Identifying Relevant Studies
Relevant studies published between January 2010 and June 2022 were identified using PubMed, CINAHL, EMBASE, web of science, Cochrane Library, CNKI, VIP, Wanfang, sinomed, and the grey literature database. The search terms used were: “old people”,/ “elder”/ “older adults”/“aged”/“geriatrics”, “glaucoma”/“macular degeneration”/“diabetic retinopathy”/ “cataract”/“vision disorders”/“visual impairment*”/“vision impairment”/“vision loss” /low vision, “rehabilitation”/“management”/“intervention*”/“model”/“strategy”/“system”. (Supplementary Material “Pubmed search strategy”)
Study Selection
Based on the participants, concepts, and context (PCC) principles for the scoping review. P: It complies with WHO’s grading standards for VI. C: It involves the health management model and strategy of the elderly with VI. C: 60 years old or older. Exclusion criteria: non-Chinese and English literature; unable to obtain full-text literature; conference papers, research programs, guides, single case reports and book chapters; repeated published articles; the research did not mention the management content and effect. The search studies were imported into EndnoteX9 for reduplication. Two trained researchers independently screened the titles and abstracts of the articles according to the inclusion and exclusion criteria, indicating the reasons for exclusion, and then further screened the full text of the included articles to indicate the reasons for exclusion. Disagreements that arose during the screening process were discussed by a third person, and the final decision was made on the included literature.
Charting the Data
The main extraction contents include author, publication year, country, study type, sample size, time, management strategies, outcome indicators, measurement tools and management effects.
Collating, Summarizing, and Reporting the Literature
We outlined and analyzed the health management models and strategies of the included literature, and extracted the data in the form of tables.
Results
Study Selection and Characteristics
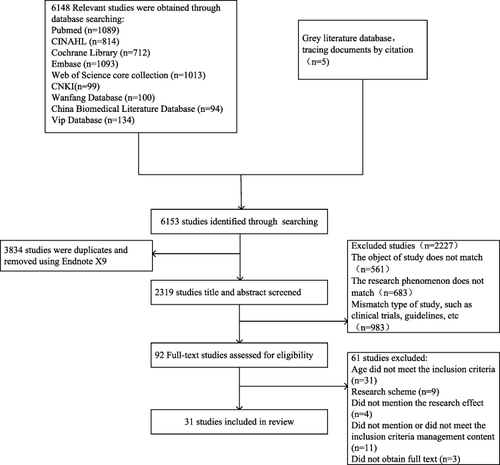
6153 articles were retrieved, and 3834 studies remained after removing duplicate articles using EndnoteX9. 2319 studies were removed after reading titles and abstracts. The remaining 92 studies were read in full text and screened for a second time, and 31 studies were finally included. The PRISMA flow diagram shows the studies’ screening process and the reasons for exclusion. The study selection process is shown in .
Figure 1 PRISMA flow diagram.
Basic Characteristics of Included Studies
The types of studies included randomized controlled trials (n=23) and quasi-experimental trials (n=8); In China (n=11), the United States (n=5), Australia (n=4), Britain (n=3), Germany (n=2), Iran (n=1), India (n=1), Canada (n =1), France (n=1), Hungary (n=1) and Brazil (n=1). The basic characteristics of the included studies are shown in Supplementary Table 1.
Health Management Models for the Elderly with VI
The health management models of the elderly visually impaired population mainly include: (1) Multidisciplinary team low vision rehabilitation model:Citation35–39 a multidisciplinary team composed of optometrists, ophthalmologists, rehabilitation therapists, nurses with rich clinical experience, community medical staff, social workers, nutritionists, etc., to assess the residual functional vision and determine patients’visual needs. According to the difficulties, requirements, and patient goals reported, create a unique visual rehabilitation plan with appropriate visual aids for each patient, provide non-optical interventions such as screening, family environment safety modification, optical interventions such as refraction, glasses, magnifying glasses, and personalized low vision rehabilitation such as orientation and mobile training, referral, and appointment medical services. (2) Medical consortium two-way management model:Citation40–42 the ophthalmologist of the tertiary hospital conducts knowledge training for the medical staff of the community health service center, the community medical staff conducts health education, individualized risk factor intervention guidance, telephone follow-up, and community outpatient follow-up, and the patients who cannot complete the ophthalmic examination in the community or have complications and whose visual acuity recovery effect is not significant are transferred to the ophthalmology department of a tertiary hospital of the medical union, and after the treatment is completed, they are transferred to the community outpatient for follow-up. Ophthalmologists in tertiary hospitals and medical personnel in community health service centers jointly manage to achieve hierarchical diagnosis and treatment and a two-way referral model. (3) Low vision community comprehensive rehabilitation model:Citation43–46 the patients with poor vision found in the daily outpatient service and physical examination in the community are transferred to the low vision joint outpatient service for vision screening, optometry, evaluation and classification, and then rehabilitation management measures are implemented. Remote optical aids, use training and health education measures are provided. Medical optometry and glasses are provided for ametropia, and surgery is required to refer them to the superior hospital for surgery. If the patient’s condition is unstable, he will be treated with traditional Chinese and western medicine in the ophthalmology department. The responsible doctor in the community will follow up for a long time. (4) Medical consortium-family contract service model:Citation47,Citation48 the family and the general practice service team sign a service agreement to jointly develop and implement targeted and personalized family support programs for patients, and encourage family members to do an excellent patient support, assistance and treatment. (5) Screening-referral-follow-up model:Citation49 it provides closed-loop eye health management services. The community conducts screening and decides whether to go to the local hospital or a tertiary hospital for treatment according to the condition of the patient. After the referral, the patient’s treatment-related data will be returned to the community hospital for follow-up and management. (6) Three-level low vision care model:Citation40,Citation45 according to the three-level low vision care recommended by WHO, the primary level provides non-optical interventions, including vision screening, family environment safety transformation, and the secondary level provides patients with the limited scope of optical interventions such as magnifying glasses. The tertiary level is provided by multidisciplinary teams with optical, non-optical, and electronic low vision aids, including visual function assessment, refraction, prescription, multidisciplinary rehabilitation, and visual skills and mobility training. See Supplementary Table 2.
Health Management Strategies for the Elderly with VI
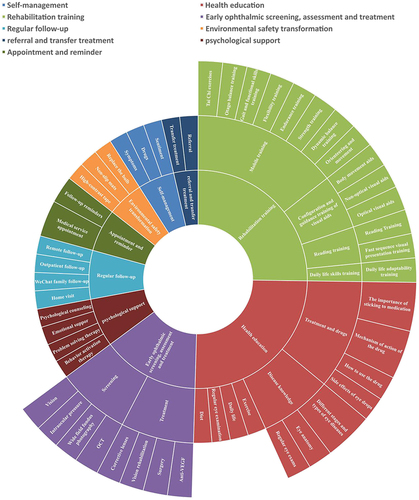
The health management strategy for people with VI involves 9 topics, including self-management,Citation36,Citation38,Citation39,Citation50 health education,Citation41–43,Citation47,Citation48,Citation50–55 rehabilitation training,Citation35,Citation37,Citation38,Citation40,Citation44–46,Citation56–65 ophthalmic examination,Citation36,Citation42,Citation43,Citation59,Citation64 evaluationCitation37,Citation38,Citation40,Citation42,Citation59 and treatment,Citation35,Citation44,Citation45,Citation49,Citation56 regular follow-up,Citation35–37,Citation42–44,Citation47,Citation49,Citation54,Citation55,Citation60 environmental safety improvement,Citation39,Citation60–62 referral and transfer treatment,Citation40,Citation41,Citation43,Citation46,Citation49 psychological support,Citation46,Citation47,Citation50,Citation63 medical service appointment and reminder.Citation35,Citation42,Citation46,Citation52,Citation54 See .
Figure 2 Health management strategies for the elderly with VI.
Evaluation Indicators
The evaluation of the control effect of visually impaired people mainly involves 10 aspects, including psychological state (n=10), quality of life (n=10), compliance (n=8), patient safety (n=4), adaptability (n=5), satisfaction (n=2), reading function (n=3), social participation (n=2), knowledge, attitude, behavior (n=5) and physiological function (n=19).
Discussion
The Advantages and Disadvantages of the Multidisciplinary Low Vision Rehabilitation Model
Multidisciplinary low vision rehabilitation maximizes residual vision through the use of visual aids and visual adaptation exercises. It is usually goal-oriented to develop personalized rehabilitation according to the needs of patients. There is no standardized rehabilitation plan, and it is not intended to generally improve all aspects of patients’lives. After rehabilitation, the overall functional ability and QoL of patients with impaired vision were enhanced.Citation37 However, the study found that the overall functioning capacity of visual rehabilitation improved in the 30-day follow-up, but recovered to the level before rehabilitation in the 3-month follow-up.Citation40 The overall visual ability of patients may deteriorate over time due to the progress of visual impairment. Other studies have shown that multidisciplinary rehabilitation has a little or uncertain impact on VRQOL.Citation66 Differences in patient needs, rehabilitation programs, and components of multidisciplinary low vision rehabilitation can also contribute to differences in management outcomes.Citation67 Therefore, the long-term benefits of multi-disciplinary low vision rehabilitation need to be further verified. There may be a need to make better use of low vision rehabilitation and to integrate low vision services into the holistic care of older persons.Citation68
The Advantages and Disadvantages of the Medical Consortium Two-Way Management Model
The two-way referral model has been widely used in managing patients with diabetes and chronic heart failure, but less used in the health management of people with VI.Citation69,Citation70 Through cooperation with hospitals and community organizations, the current low vision model tries to provide services that conform to the people-oriented nursing principle to the greatest extent.Citation71 This model combines the advantages of general hospitals and community hospitals, which can significantly alleviate the burden of diagnosis and treatment in general hospitals, reduce the waste of medical resources and the loss of staff in grass-roots hospitals,Citation72 and greatly promote compliance behavior, emotion and QoL of cataract patients in communities.Citation73 Based on community service, combined treatment for patients and focusing on health education can significantly reduce medical expenses and strengthen patient compliance. Community doctors and residents can maintain a close relationship through close community intervention, and patients’ strangeness and psychological barriers to doctors will weaken.Citation74 Patients can better understand disease-related health knowledge, and community doctors’ clinical skills can also be improved.Citation69 However, some patients are still skeptical of general community practitioners. The work enthusiasm of community healthcare needs to be improved, and communication with patients should be strengthened to gain the trust of patients. At the same time, their professional standards should be improved.Citation69
The Advantages and Disadvantages of Low Vision Community Comprehensive Rehabilitation Model
Community rehabilitation services for low vision patients include multiple rehabilitation services such as medical treatment, evaluation, rehabilitation training and visual aid examination, which can meet the personalized needs of patients with VI. The community health service center is relatively close to facilitating the low vision patients” rehabilitation and medical treatment. Community-based screening programs provide convenience for seniors and increase affordability and continuity of access to much-needed essential vision screening and care.Citation75 The World Health Organization (WHO) also recommends promoting community-based rehabilitation and providing comprehensive rehabilitation services to people in under-resourced settings, such as rural areas.Citation76 In addition, there is a capable management team of local physicians who are more in touch with the workers and inhabitants of the community, which helps the growth of rehabilitation work. It achieved promising results for clinical outcomes, function, and QoL, but could not provide clear evidence due to the heterogeneity of interventions and the quality of the included studies.Citation77 Community-based Rehabilitation coverage is typically poor and seldom had in social security or health systems.Citation78 Community general practitioners are generally of low professional quality and cannot accurately assess and provide individual services for chronic diseases of the elderly.Citation79 The World Health Organization also agrees that no single community-based rehabilitation model is applicable globally and recommends using existing community-based rehabilitation as a framework.
The Advantages and Disadvantages of the Medical Consortium-Family Contract Service Model
Family contract service is a kind of family support treatment, which is to sign service contracts, service contents, service methods, responsibilities and obligations of both parties based on families, and establish a stable service relationship with patients’ families in the form of contracts.Citation80 Through the health evaluation of patients, a personalized health management plan is formulated to enable the whole family to actively participate in and provide support, encouragement and supervision for patients to the maximum extent. The signing of a family doctor solidifies the contractual relationship between community residents and general practitioners through a contract, which can effectively improve the continuity of patient nursing.Citation81 Family doctors provide primary care services and community health education can reduce the disease burden by up to 70%.Citation82 The community health service agency factor is the factor that affects the effect of the family contract service model.Citation83 During the implementation process, there may be some complex problems, such as team organization structure not being in line with the actual work, easy to become a mere formality, and supervision, assessment and incentive mechanism challenging to get rid of institutional constraints,Citation84 low enthusiasm of doctors,Citation85 and information system can not play a better role in helping. Community healthcare institutions should establish and improve supporting performance appraisal systems and incentive mechanisms, increase the enthusiasm of family doctors, and help them better provide health services for patients.Citation86 The family doctor team should provide high-quality personalized services for patientsCitation83 and actively communicate with patients, so that patients can receive continuous psychological counseling, to better control the patient’s condition.Citation87 The contract between the family doctor and the service provider and the service content needs to be improved.Citation88 National government factors are the main trigger for family contract services. Public health services provided by family doctors should be included in the scope of health insurance and linked to health insurance to assist family doctor health management.
The Advantages and Disadvantages of the Three-Level Low Vision Care Model
The three-level low vision rehabilitation model is divided into primary, intermediate and three-level management according to the severity of visual impairment. The primary low vision service should be able to meet the needs of 30% of the low vision population, the other 20% of the low vision service should be completed by tertiary care, and the needs of the remaining 50% of the low vision population should be met adequately in secondary care. Primary health workers can treat simple eye diseases at the primary level and prevent large numbers of patients from going to overburdened secondary hospitals, thereby saving patient costs and freeing up the capacity of specialist eye staff to treat more complex eye diseases. Compared with other health management models, this model is conducive to hierarchical management and rational use of resources. However, not all multidisciplinary centers can provide comprehensive tertiary services, and the distinction between secondary and tertiary levels may not be evident.Citation89 Difficulties in transportation, service distance, low referral rate, insufficient understanding of services, lack of equipment and facilities, lack of trained staff and other issues will affect the best cost-effectiveness.Citation90,Citation91
The Advantages and Disadvantages of the Screening-Referral-Follow-Up Model
Grassroots hospitals are responsible for large-scale primary screening, and superior hospitals are accountable for eye disease prevention and treatment, which can prevent and delay the occurrence and development of eye diseases in high-risk groups, and effectively reduce the waste of resources in grade A tertiary hospitals.Citation92 At the same time, it improves the patient’s awareness of early screening and treatment of eye diseases as early as possible and reduces medical and health expenditures.Citation93 Recruitment - screening - referral - turnaround - follow-up model can improve the diagnosis and treatment of patients and reduce the burden on patients and society. In transmitting large-scale screening results to the superior hospital, due to the huge workload, the resulting feedback may be delayed in time (especially in rural regions), resulting in long waits. How to save time and cost in the future so as not to delay the development of the disease is worth considering.
The Health Management Strategy of Combining Multiple Elements is Feasible
Only a few studies provided a single health management strategy such as self-management education, environmental safety modification, and reading training.Citation39,Citation57 The majority also offered health services that combined multiple management strategies such as eye screening, assessment, and psychological support. The health management mode combined with multiple strategies has significantly improved patients’ self-reported mental state, QoL, visual function, etc. In contrast, a single strategy, such as only providing family reform suggestions, has not changed QoL,Citation60 only providing reading training, has not changed the visual function of patients,Citation57 and only providing daily exercise and directional and directional walking mobile training. The patient’s emotional state, falls, and quality of life have not changed.Citation39,Citation58 90% of people who are blind or have poor vision still have some useable residual vision, which can benefit from professional low vision rehabilitation.Citation94 In light of this, comprehensive vision rehabilitation should be carried out through multidisciplinary teamwork combined with multiple management strategies.
Network Information Technology Shows Positive Effects
The difficulties of timely information transmission and health education have been solved by new solutions made possible by information technology. Daily text messages from mobile phones have increased patients’ awareness of eye information and compliance with routine eye exams.Citation52 The patient’s blood sugar was reduced, and their self-management behavior and knowledge awareness increased after their relatives adopted WeChat interactive follow-up, health education, and follow-up reminder. Electronic health records can ensure that patients can easily view their records. The tertiary-level hospitals’ medical staff and the community’s accountable doctors can assess the condition of patients and their families at any time, conduct in-depth analyses, send individualized education materials as required based on the various needs of patients, and conduct long-term follow-ups. It is a convenient way to strengthen the communication between patients, communities and hospitals.Citation93
Differences and Linkages Between Health Management Models in Different Countries
Multidisciplinary low vision rehabilitation services have been widely used in developed countries such as AustraliaCitation38 and France.Citation35 The multidisciplinary team initially assesses residual functional vision, determines the patient’s visual needs, develops a personalized visual rehabilitation program and equips it with visual aids such as orientation and mobility training, independent living training, recreational and leisure improvement, use of adaptive techniques and equipment, and modification of the living environment. Multi-disciplinary teams in different countries have different workplaces and flexible working styles, such as Australia and Brazil. Training can occur in specialized low vision rehabilitation centers or medical facilities, or rehabilitation management can be carried out at home or in the community through home rehabilitation therapists, community low vision service teams, and social volunteers. Whether the visually impaired are in a hospital, community, or family, they can receive systematic and standardized low-vision rehabilitation services. Low vision rehabilitation self-management has been empirically studied in Australia,Citation38,Citation39 Iran,Citation36 and other countries. The main contents include life skills training and regular evaluation, learning to apply problem-solving models, increased recreational activities and exercises, and more. Participants are encouraged to leverage and share their wealth of life experiences, coping mechanisms, and develop new skills and strategies to apply and learn new skills in everyday life. Girdler et alCitation39 showed significant improvements in depression, social engagement, visual impairment adaptability, and self-efficacy. Rees et alCitation38 differed from Girdler in that no differences were found between groups in vision-specific quality of life, emotional well-being, adaptation to vision loss, or self-efficacy. Community-based health management is more effective in developing countries such as China. Health education programs are particularly prominent in management methods, including the importance of disease knowledge, diet, exercise, medication, and regular follow-up through the Internet. Lack of awareness and understanding of vision loss is one of the barriers to using low vision services, as older people tend to perceive deterioration of vision as a natural part of aging,Citation95 so the health education is particularly important, especially in rural areas.Citation96 Community health management has also been used to promote the independence of persons with disabilities through assisted living projects. In developing countries, community-based health management is feasible.Citation97 In countries such as the UK,Citation58,Citation60 the focus on providing home-based services is more prominent, with more home exercise, home environment assessment, and modification so that older people with low vision in everyone’s community can access rehabilitation services and reduce the incidence of falls. However, the cost of such training is usually not reimbursable by Medicare or private insurance in the USA.Citation98 In short, the availability of low vision services in developing countries such as China is limited; although the service models of various countries are different, there are some common characteristics and practices. We should improve community-based rehabilitation, learn from the experience of multidisciplinary and hierarchical diagnosis and treatment in developed countries, solve the difficulties of regional and cultural differences in a demand-oriented manner, formulate regional and flexible health management methods that meet China’s national conditions, and improve the effectiveness of policy implementation.
Conclusion
The five health management models’ efficacy and viability have already been shown, but further cost-effectiveness analysis will be required in the future. In the future, we should explore the hospital-community-family linkage support service system under a hierarchical management model, actively use artificial intelligence technology to provide demand-based personalized support, rationalize and scientifically implement hierarchical health control, improve resource utilization efficiency, and improve eye health outcomes.
Abbreviations
VI, Visual impairment; VRQoL, Vision-related quality of life.
Data Sharing Statement
All data is displayed in text or uploaded as Supplementary Material.
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The poster’s abstract was published in “Poster Abstracts” in [Research Square: hyperlink with DOI:10.21203/rs.3.rs-2770331/v1].
Additional information
Funding
References
- The Central People’s Government of the People’s Republic of China. Practical assessment standards for the disabled in China[EB/OL](2006 −12 −01)[2014 −08 −26]; Availabe from: http://www.gov.cn/ztzl/gacjr/content_459939.htm-26. Accessed May 7, 2024.
- Xu T, Wang B, Liu H, et al. Prevalence and causes of vision loss in China from 1990 to 2019: findings from the global burden of disease study 2019. Lancet Public Health. 2020;5(12):e682–e691. doi:10.1016/S2468-2667(20)30254-1
- Bourne R, Steinmetz JD, Flaxman S, et al. Trends in prevalence of blindness and distance and near vision impairment over 30 years: an analysis for the global burden of disease study. Lancet Glob Health. 2021;9(2):e130–e143. doi:10.1016/S2214-109X(20)30425-3
- Statistics NBo: Statistical communiqué of the people’s Republic of China on national economic and social development in; 2021 Available from: http://www.stats.gov.cn/tjsj/zxfb/202202/t20220227_1827960.html. Accessed May 7, 2024.
- Fricke TR, Tahhan N, Resnikoff S, et al. Global prevalence of presbyopia and vision impairment from uncorrected presbyopia: systematic review, meta-analysis, and modelling. Ophthalmology. 2018;125(10):1492–1499. doi:10.1016/j.ophtha.2018.04.013
- Song P, Wang H, Theodoratou E, Chan KY, Rudan I. The national and subnational prevalence of cataract and cataract blindness in China: a systematic review and meta-analysis. J Glob Health. 2018;8(1):010804. doi:10.7189/jogh.08.010804
- Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
- EF HS, Loneliness, social isolation and sight loss. Retrieved from Lancaster University, division of health research website; 2013 Available from: http://goo.gl/T8GDDB. Accessed May 7, 2024.
- Swenor BK, Muñoz B, West SK. A longitudinal study of the association between visual impairment and mobility performance in older adults: the Salisbury eye evaluation study. American j Epidem. 2014;179(3):313–322. doi:10.1093/aje/kwt257
- Crews JE, Chou C-F, Stevens JA, Saaddine JB. Falls among persons aged≥ 65 years with and without severe vision impairment—United States, 2014. MMWR. 2016;65(17):433–437. doi:10.15585/mmwr.mm6517a2
- Menezes C, Vilaça KHC, Menezes RLD. Menezes RLd: falls and quality of life of people with cataracts. Rev Bras Oftalmol. 2016;75:40–44. doi:10.5935/0034-7280.20160009
- Bowen MED, Hancock B, Haque S, Shah R, Buchanan S; Health Services and Delivery Research. The prevalence of visual Impairment in people with dementia (the PrOVIDe study): a cross-sectional study of people aged 60–89 years with dementia and qualitative exploration of individual, carer and professional perspectives. Southampton; 2016.
- Guthrie DM, Davidson JG, Williams N, et al. Combined impairments in vision, hearing and cognition are associated with greater levels of functional and communication difficulties than cognitive impairment alone: analysis of interRAI data for home care and long-term care recipients in Ontario. PLoS One. 2018;13(2):e0192971. doi:10.1371/journal.pone.0192971
- Taipale J, Mikhailova A, Ojamo M, et al. Low vision status and declining vision decrease health-related quality of life: Results from a nationwide 11-year follow-up study. Qual Life Res. 2019;28(12):3225–3236. doi:10.1007/s11136-019-02260-3
- Crews JE, Campbell VA. Vision impairment and hearing loss among community-dwelling older Americans: implications for health and functioning. Am J Public Health. 2004;94(5):823–829. doi:10.2105/AJPH.94.5.823
- Lee DJ, GomezMarin O, Lam BL, Zheng DD. Visual acuity impairment and mortality in US adults (vol 120, pg 1544, 2002). Arch Ophthalmol. 2003;121(7):972.
- Akuffo KO, Sewpaul R, Darrah S, et al. Vision loss, vision difficulty and psychological distress in South Africa: results from SANHANES-1. BMC Psychol. 2021;9(1). doi:10.1186/s40359-021-00558-x
- van der Aa HP, Comijs HC, Penninx BW, van Rens GH, van Nispen RM. Major depressive and anxiety disorders in visually impaired older adults. Invest Ophthalmol Vis Sci. 2015;56(2):849–854. doi:10.1167/iovs.14-15848
- van Nispen RM, Vreeken HL, Comijs HC, Deeg DJ, van Rens GH. Role of vision loss, functional limitations and the supporting network in depression in a general population. Acta Ophthalmol. 2016;94(1):76–82. doi:10.1111/aos.12896
- Heesterbeek TJ, van der Aa HPA, van Rens G, Twisk JWR, van Nispen RMA. The incidence and predictors of depressive and anxiety symptoms in older adults with vision impairment: a longitudinal prospective cohort study. Ophthalmic Physiol Opt. 2017;37(4):385–398. doi:10.1111/opo.12388
- Strawbridge WJ, Wallhagen MI, Shema SJ. Impact of spouse vision impairment on partner health and well-being: a longitudinal analysis of couples. J Gerontol B Psychol Sci Soc Sci. 2007;62(5):S315–S322. doi:10.1093/geronb/62.5.S315
- Kulkarni S, Gilbert C, Zuurmond M, Agashe S, Deshpande M. Blinding retinopathy of prematurity in Western India: Characteristics of children, reasons for late presentation and impact on families. Indian Pediatrics. 2018;55(8):665–670. doi:10.1007/s13312-018-1355-8
- Wagner H, Stifter J, Engesser D, et al. Ophthalmic care in nursing homes for the blind: A growing challenge. Klin Monbl Augenheilkd. 2020;237(11):1326–1333. doi:10.1055/a-1194-5381
- Owsley C, McGwin G, Scilley K, Meek GC, Dyer A, Seker D. The visual status of older persons residing in nursing homes. Arch Ophthalmol. 2007;125(7):925–930. doi:10.1001/archopht.125.7.925
- Eckert KA, Carter MJ, Lansingh VC, et al. A simple method for estimating the economic cost of productivity loss due to blindness and moderate to severe visual impairment. Ophthalmic Epidem. 2015;22(5):349–355. doi:10.3109/09286586.2015.1066394
- Naidoo KS, Fricke TR, Frick KD, et al. Potential lost productivity resulting from the global burden of myopia: systematic review, meta-analysis, and modeling. Ophthalmology. 2019;126(3):338–346. doi:10.1016/j.ophtha.2018.10.029
- Bourne RRA, Flaxman SR, Braithwaite T, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(9):e888–e897. doi:10.1016/S2214-109X(17)30293-0
- Ramke J, Gilbert CE, Lee AC, Ackland P, Limburg H, Foster A. Effective cataract surgical coverage: An indicator for measuring quality-of-care in the context of universal health coverage. PLoS One. 2017;12(3):e0172342. doi:10.1371/journal.pone.0172342
- Wong TY, Sun J, Kawasaki R, et al. Guidelines on Diabetic eye care: the international council of ophthalmology recommendations for screening, follow-up, referral, and treatment based on resource settings. Ophthalmology. 2018;125(10):1608–1622. doi:10.1016/j.ophtha.2018.04.007
- Jianxun C, Liangcai M, Wenlong Y, Zhengzheng Z, Zhikai Z. The concept and practice of “health management”. Chin Public Health Manage. 2006;22(1):7–10.
- Launch of the World Report on Vision at the United Nations. Available from: https://www.who.int/news/item/18-11-2019-launch-of-The-world-report-on-vision-at-The-united-nations-headquarters. Accessed May 7, 2024.
- Li S, Wang AP. Demand preferences for health management services in a population of older adults with visual impairment in China: a conjoint analysis. BMC Geriatr. 2022;22(1):252. doi:10.1186/s12877-022-02957-0
- Arksey H, O’Malley L. O’Malley L: Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
- Levac D, Colquhoun H, KK O. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69. doi:10.1186/1748-5908-5-69
- Bon V, Ghemame M, Fantou P, Philliponnet A, Mouriaux F. Feedback on ophthalmologic telemedicine in a nursing home. J Fr Ophtalmol. 2020;43(9):e293–e297. doi:10.1016/j.jfo.2020.09.002
- Ghasemi A, Moonaghi HK, Mohajer S, Mazlom SR, Shoeibi N. Effect of Self-management educational program on vision-related quality of life among elderly with visual impairment. J Evid-Based Care. 2018;8(1):35–44.
- Gothwal VK, Bharani S. Outcomes of multidisciplinary low vision rehabilitation in adults. Invest Ophthal Vis Sci. 2015;56(12):7451–7461. doi:10.1167/iovs.15-16892
- Rees G, Xie J, Chiang PP, et al. A randomised controlled trial of a self-management programme for low vision implemented in low vision rehabilitation services. Patient Educ Couns. 2015;98(2):174–181. doi:10.1016/j.pec.2014.11.008
- Girdler SJ, Boldy DP, Dhaliwal SS, Crowley M, Packer TL. Vision self-management for older adults: A randomised controlled trial. Br J Ophthalmol. 2010;94(2):223–228. doi:10.1136/bjo.2008.147538
- Wang BZ, Pesudovs K, Keane MC, Daly A, Chen CS. Evaluating the effectiveness of multidisciplinary low-vision rehabilitation. Optom Vis Sci. 2012;89(9):1399–1408. doi:10.1097/OPX.0b013e3182678d82
- Haishuang YX HU, Chen Y. Management model of community cataract patients based on bidirectional management. Hospl Manage Forum. 2016;33(07):59–62.
- Wang Dengxue LIUL, Guangjun X, Jue L, Zaihong C. Study on the effect of community intervention in diabetic retinopathy in the medical combination model. Chongqing Medical Science. 2020;49(11):1855–1858.
- Chen PD CHEN, Lee B. Evaluation of the effect of community-based comprehensive intervention by a family-specialist team on patients with early diabetic retinopathy. Shanghai Med J. 2020;41(18):47–51.
- Xiaoyun DH YANG. WANG Jian, et al.Establishment and application of low-vision community comprehensive rehabilitation model. China Rural Medicine. 2015;2015(12):57–58.
- Man REK, Gan ATL, Constantinou M, et al. Effectiveness of an innovative and comprehensive eye care model for individuals in residential care facilities: results of the residential ocular care (ROC) multicentred randomised controlled trial. Br J Ophthalmol. 2020;104(11):1585–1590. doi:10.1136/bjophthalmol-2019-315620
- Hark LA, Madhava M, Radakrishnan A, et al. Impact of a social worker in a glaucoma eye care service: A prospective study. Health Social Work. 2019;44(1):48–56. doi:10.1093/hsw/hly038
- Zhe ZY XU. Effect of family contract service in the management of type 2 diabetic retinopathy in the community. J Nurse Training. 2015;2015(20):1885–1887.
- Yuanyuan WX ZHOU, Yuqiong LIU. Effect of community intervention on treatment adherence and effect in patients with diabetic retinopathy.Anhui. Medical J. 2016;37(8):1034–1036.
- Gao Wenxue QM, Jiafang Y, et al. Rapid screening and referral practice of eye disease in middle-aged and elderly groups in community hospitals. PLA Hospital Manage J. 2021;28(8):752–754.
- Jing LT MA. Application of health management model in patients with age-related macular degeneration.Chinese. J Modern Nursing. 2012;18(7):783–785.
- Li WW DENG, Xiaoting MAO. Effect of health education on the management effect of patients with diabetic retinopathy in the community. Clinical Research in Medicine. 2020;37(7):1098–1099.
- Chen TT, Zhu WH, Tang B, et al. A mobile phone informational reminder to improve eye care adherence among diabetic patients in rural china: a randomized controlled trial. Am J Ophthalmol. 2018;194:54–62. doi:10.1016/j.ajo.2018.07.006
- Fiscella R, Caplan E, Kamble P, Bunniran S, Uribe C, Chandwani H. The effect of an educational intervention on adherence to intraocular pressure-lowering medications in a large cohort of older adults with glaucoma. J Manag Care Spec Pharm. 2018;24(12):1284–1294. doi:10.18553/jmcp.2018.17465
- Wenjing LY JIANG, Jihong YAN. Effect of WeChat follow-up of relatives on patients with diabetic retinopathy. Chin J Health Manage. 2017;11(3):228–233.
- Djafari F, Lesk MR, Giguère CE, Siam G, Freeman EE. Impact of a brief educational intervention on glaucoma persistence: A randomized controlled clinical trial. Ophthalmic Epidem. 2015;22(6):380–386. doi:10.3109/09286586.2015.1083036
- Ikeda MC, Hamada KU, Bando AH, et al. Interventions to improve reading performance in glaucoma. Ophthalmol Glaucoma. 2021;4(6):624–631. doi:10.1016/j.ogla.2021.03.013
- Kaltenegger K, Kuester S, Altpeter-Ott E, et al. Effects of home reading training on reading and quality of life in AMDa randomized and controlled study. Graefes Arch Clin Exper Ophthalmol. 2019;257(7):1499–1512. doi:10.1007/s00417-019-04328-9
- Adams N, Skelton DA, Howel D, et al. Feasibility of trial procedures for a randomised controlled trial of a community based group exercise intervention for falls prevention for visually impaired older people: the VIOLET study. BMC Geriatr. 2018;18:18. doi:10.1186/s12877-018-0716-4
- Deemer AD, Massof RW, Rovner BW, Casten RJ, Piersol CV. Functional outcomes of the low vision depression prevention trial in age-related macular degeneration. Invest Ophthalmol Vis Sci. 2017;58(3):1514–1520. doi:10.1167/iovs.16-20001
- Waterman H, Ballinger C, Brundle C, et al. A feasibility study to prevent falls in older people who are sight impaired: the VIP2UK randomised controlled trial. Trials. 2016;17(1):464. doi:10.1186/s13063-016-1565-0
- Acton JH, Molik B, Court H, Margrain TH. Effect of a home visit-based low vision rehabilitation intervention on visual function outcomes: An exploratory randomized controlled trial. Invest Ophthalmol Vis Sci. 2016;57(15):6662–6667. doi:10.1167/iovs.16-19901
- Rovner BW, Casten RJ, Hegel MT, et al. Low vision depression prevention trial in age-related macular degeneration a randomized clinical trial. Ophthalmology. 2014;121(11):2204–2211. doi:10.1016/j.ophtha.2014.05.002
- Rovner BW, Casten RJ, Hegel MT, et al. Improving function in age-related macular degeneration: a randomized clinical trial. Ophthalmology. 2013;120(8):1649–1655. doi:10.1016/j.ophtha.2013.01.022
- Renieri G, Pitz S, Pfeiffer N, Beutel ME, Zwerenz R. Changes in quality of life in visually impaired patients after low-vision rehabilitation. Int J Rehabil Res. 2013;36(1):48–55. doi:10.1097/MRR.0b013e328357885b
- Kovacs E, Toth K, Denes L, et al. Effects of exercise programs on balance in older women with age-related visual problems: a pilot study. Arch Gerontol Geriatrics. 1975;55; 2012:446‐452. doi:10.1021/bi00696a008
- van Nispen RM, Virgili G, Hoeben M, et al. Low vision rehabilitation for better quality of life in visually impaired adults. Cochrane Database Syst Rev. 2020;1:CD006543.
- Virgili G, Acosta R, Bentley SA, Giacomelli G, Allcock C, Evans JR. Reading aids for adults with low vision. Cochrane Database Syst Rev. 2018;4(4):CD003303. doi:10.1002/14651858.CD003303.pub4
- Varadaraj V, Chung SE, Swiatek KS, et al. Caring for older adults with vision impairment and dementia. Innov Aging. 2020;4(6):262. doi:10.1093/geroni/igaa057.841
- Wang Xinling XJ. Research on hospital community joint two-way management model for patients with chronic heart failure. Int J Cardiova Dis. 2017;2017:1.
- Jiang Xiaojun LG. Discussion on hospital community standardized management model for diabetes patients under two-way referral. Chinese Med Guide. 2013;2013
- Senjam SS. Developing a disability inclusive model for low vision service. Indian J Ophthalmol. 2021;69(2):417–422. doi:10.4103/ijo.IJO_236_20
- Niu DW, Wang LC, Li W, Ma YC. An International Comparative Study on the Resilience of Urban Communities after COVID-19 Pandemic: a One-Year Case Study between Lanzhou, China and Sarajevo, Bosnia and Herzegovina. Int J Environ Res Public Health. 2022;19(21):14458. doi:10.3390/ijerph192114458
- Wang Xiaodong WH, Fengyun Z, Wang L, Wu Yaqin. Design and implementation of two-way referral management system under the hierarchical diagnosis and treatment model. J Med Info. 2019;2019
- Li TT, Lv M, Lei T, et al. Who benefits most from influenza vaccination policy: a study among the elderly in Beijing, China. Intl J Equity Health. 2016;15:15. doi:10.1186/s12939-016-0306-z
- Hussey M, MacLachlan M, Mji G. Barriers to the Implementation of the Health and Rehabilitation Articles of the United Nations Convention on the Rights of Persons with Disabilities in South Africa. Int J Health Policy Manag. 2017;6(4):207–218. doi:10.15171/ijhpm.2016.117
- Khasnabis C, Heinicke Motsch K, Achu K, et al. Community-Based Rehabilitation: CBR Guidelines. 2010; Geneva.
- Iemmi V, Blanchet K, Gibson LJ, et al. Community-based rehabilitation for people with physical and mental disabilities in low- and middle-income countries: a systematic review and meta-analysis. J Dev Effect. 2016;8(3):368–387. doi:10.1080/19439342.2016.1157623
- Mason C, Weber J, Atasoy S, Sabariego C, Cieza A, Martinuzzi A. Development of indicators for monitoring Community-Based Rehabilitation. PLoS One. 2017;12(6):e0178418. doi:10.1371/journal.pone.0178418
- Qiao L, Li R. Influence of personalized health management model based on internet mode on self-management ability and life quality of patients with chronic diseases undergoing physical examination. Comput Math Meth Med. 2022;4434436. doi:10.1155/2022/4434436
- Shang X, Huang Y, Li B, et al. Residents’ awareness of family doctor contract services, status of contract with a family doctor, and contract service needs in Zhejiang Province, China: A cross-sectional study. Int J Environ Res Public Health. 2019;16(18):3312. doi:10.3390/ijerph16183312
- Li LL, He XT, Zhang CH. The impact of public policy of family doctor contracting on medical expenses from the perspective of residents at community level in China. Front Psych. 2023;13.
- Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians - Implications for patient safety and continuity of care. JAMA J Am Med Assoc. 2007;297(8):831–841. doi:10.1001/jama.297.8.831
- Wang H, Shi L, Han X, et al. Factors associated with contracted services of Chinese family doctors from the perspective of medical staff and consumers: a cross-sectional study. BMC Health Serv Res. 2019;19(1):986. doi:10.1186/s12913-019-4801-y
- Sun JJ, Zhang YL, Zhang XH, Song XM, Chen G. Situation, challenges, and countermeasures of home-based healthcare service supply and demand in China. China CDC Weekly. 2021;3(40):847–852. doi:10.46234/ccdcw2021.209
- Liu S, Meng W, Yu Q, et al. Evaluation and countermeasures of contracted services of Chinese family doctors from demanders’ point of view - A case study of a city. BMC Health Serv Res. 2022;22(1):1534. doi:10.1186/s12913-022-08891-6
- Ma Z, Su J, Pan H, Li M. A signaling game of family doctors and residents from the perspective of personalized contracted service. Int J Environ Res Public Health. 2022;19(17):10744.
- Fogelman Y, Goldfracht M, Karkabi K. Managing diabetes mellitus: A survey of attitudes and practices among family physicians. J Community Health. 2015;40(5):1002–1007. doi:10.1007/s10900-015-0024-2
- Dai H, Tang L, Wang Z, et al. Facilitate signing with the family Doctor: A study of the practice in Shanghai, China. Int J Gen Med. 2021;14:6907–6917. doi:10.2147/IJGM.S332890
- Chiang PP, Marella M, Ormsby G, Keeffe J. Critical issues in implementing low vision care in the Asia-Pacific region. Indian J Ophthalmol. 2012;60(5):456–459. doi:10.4103/0301-4738.100549
- Ryan B. Models of low vision care: past, present and future. Clin Exp Optom. 2014;97(3):209–213. doi:10.1111/cxo.12157
- Ryan B, White S, Wild J, Court H, Margrain TH. The newly established primary care based Welsh Low Vision Service is effective and has improved access to low vision services in Wales. Ophthal Physiol Opt. 2010;30(4):358–364. doi:10.1111/j.1475-1313.2010.00729.x
- da Silva EN, Powell-Jackson T. Does expanding primary healthcare improve hospital efficiency? Evidence from a panel analysis of avoidable hospitalisations in 5506 municipalities in Brazil, 2000-2014. BMJ Glob Health. 2017;2(2):e000242. doi:10.1136/bmjgh-2016-000242
- Troncoso LL, Biancardi AL, de Moraes Jr HV Jr, Zaltman C. Ophthalmic manifestations in patients with inflammatory bowel disease: a review. World J Gastroenterol. 2017;23(32):5836–5848. doi:10.3748/wjg.v23.i32.5836
- Lamoureux EL, Pallant JF, Pesudovs K, Rees G, Hassell JB, Keeffe JE. The effectiveness of low-vision rehabilitation on participation in daily living and quality of life. Invest Ophthalmol Vis Sci. 2007;48(4):1476–1482. doi:10.1167/iovs.06-0610
- Gold D, Zuvela B, Hodge WG. Perspectives on low vision service in Canada: a pilot study. Can J Ophthalmol. 2006;41(3):348–354. doi:10.1139/I06-025
- Lam N, Leat SJ, Leung A. Low-vision service provision by optometrists: a Canadian nationwide survey. Optom Vis Sci. 2015;92(3):365–374. doi:10.1097/OPX.0000000000000512
- Axelson H, Lindén A, Andersson JE, Skehan T. Equalization and Participation for All: Swedish Disability Policy at a Crossroads. Stud Health Technol Inform. 2016;229:69–77.
- Bowman EL, Liu L, Lv Z. Individuals with severely impaired vision can learn useful orientation and mobility skills in virtual streets and can use them to improve real street safety. PLoS One. 2017;12(4):e0176534. doi:10.1371/journal.pone.0176534