Abstract
Aim
To describe the use of a “workable” visual profile of function and disability, based on a modified Brief International Classification of Functioning, Disability and Health (ICF) Core Set for chronic widespread pain, for initial assessments in a clinical setting of interdisciplinary pain rehabilitation teams.
Method
The Brief ICF Core Set was slightly adapted to meet the needs of an interdisciplinary rehabilitation medicine team working in a university outpatient clinic and admitting patients referred from primary care. The Core Set categories were made measurable by means of eg, assessment instruments and clinical investigations. The resulting profile was given a workable shape to facilitate rapid understanding of the initial assessment outcome.
Results
Individual patients showed different profiles of problems and resources, which facilitated individual rehabilitation planning. At the level of the study group, the profiles for the Core Set component Body Functions showed that most patients had severe impairment in the sensation of pain and exercise tolerance categories of function, but most had resources in the motivation and memory categories of function. Likewise, for the component Activities, most patients had limitations in lifting and carrying objects and remunerative employment, but most had resources in intimate relationships and family relationships. At first, the use of the modified Brief ICF Core Set in the team conference was rather time consuming, but after a couple of months of experience, the team assessment took approximately 30 minutes to complete per patient.
Conclusion
The profile of the modified Brief ICF Core Set for chronic widespread pain served as a common platform, facilitating cooperation between the rehabilitation team members and providing a uniform language, which helped in structuring the clinical work. The profile also provided an easily accessible, overall view of the patient’s problems and resources, which helped in understanding the functioning situation of the patient.
Introduction
In many countries, specialized health care and rehabilitation for patients with long-term/chronic pain conditions is provided by pain rehabilitation clinics or “pain clinics.” Rehabilitation for patients with long-term pain is often performed by interprofessional teams.Citation1–Citation3 This teamwork involves the patient and all team members working together in goal setting, planning of interventions, and evaluation of the rehabilitation (ie, evaluation of the interdisciplinary teamwork).Citation4–Citation6 An important task for these clinics is to evaluate patient functioning and disabilities. The literature indicates that the International Classification of Functioning, Disability and Health (ICF)Citation7 could be a helpful resource to provide a holistic, yet condensed picture of patient functioning and disabilities for this kind of evaluation. In a regular clinical setting, with its demand for high tempo, it is advantageous for the evaluation to be given a practical and “workable” shape. In this study, just such an easy-to-read version of the ICF categories was tested as a basis for evaluation.
The ICF provides a large number of categories covering different domains and therefore seems useful in the context of an interdisciplinary rehabilitation team, where different professions address different aspects of the ICF. The use of the ICF model seems helpful in directing our attention to different aspects of functioning rather than on focusing on diagnostic procedures.Citation8 To facilitate its clinical application, comprehensive Brief ICF Core Sets have been developed for different diagnoses, such as low-back pain (LBP)Citation9 and chronic widespread pain (CWP).Citation10
One study examined whether it was feasible to construct a psychometrically sound clinical instrument to measure functioning in fibromyalgia, based on the Brief ICF Core Set for CWP.Citation11 The study illustrated that it is possible to measure functioning as a unidimensional construct based on selected ICF categories. Following the analysis process, 14 of the 24 ICF categories remained in the model, each showing good fit to the model.
A systematic literature review spanning 2001 to 2009 included 32 papers describing practical clinical applications of the ICF and 47 papers describing its use for specific conditions.Citation12 Of these papers, only two addressed the clinical context of long-term pain.Citation8,Citation13 The validity of the ICF Core Set for CWP was studied from the perspective of fibromyalgia patients, using focus groups.Citation14 Patients reported 54 out of the 67 ICF categories in the earlier published version, and 48 additional categories not covered in the earlier presented version were identified. For instance, 27 and 15 additional concepts, respectively were linked to fine-motor hand use (d440) and hand and arm use (d445). Thirty-two additional concepts were linked to memory functions (b144).
No CWP study was found that focused on practical clinical applications, and therefore, LBP studies were used to introduce the topic, since LBP is another common long-term pain condition within rehabilitation. In one study, patients’ with LBP were asked to specify their greatest difficulty arising from to their back pain and something they used to enjoy but were now unable to do because of their LBP.Citation13 This was compared to the LBP Core Sets, and the authors recommended an addition of the categories Recreation and Leisure, and Caring for Household Objects to the LBP Brief ICF Core Set. Low to moderate reliability was found when using the LBP Core Set, consequently the authors recommended improved operationalization of the categories.Citation15
The Comprehensive ICF Core Set for LBP was tested for clinical use in patients with LBP, in a nationwide study in Norway.Citation16 The authors concluded that it is possible to use the ICF in clinical settings. By using the ICF, the study personnel increased their knowledge about patients’ body function, activity, participation, and influential environmental factors. It was important that the personnel were first adequately trained to perform the scoring of the qualifiers. During the study, seminars and emails were used to discuss difficulties and uncertainties, and this was found to be important to accomplishing a common interpretation of the categories and scoring.
In a validation studyCitation17 that aimed to identify candidate categories from the ICF to be included in the Brief ICF Core Set for LBP, twelve ICF categories were found to be significant explanatory factors, four of which were not included in the previously proposed Brief Core Set for LBP.Citation9 This is one example of the ongoing scientific work to improve the practical clinical application of the ICF.
In another article,Citation18 more studies were recommended to improve reliability and to identify the best methods for using the ICF in daily clinical practice. The authors argued that further clinical research is needed to improve the possibilities for clinical applications of ICF.
Research is relatively sparse on the benefits of using ICF as a basis for interdisciplinary team assessments of patients with long-term pain conditions. It seems that there is a lack of internationally published studies that use the Brief ICF Core Set (fully or in a modified version) for CWP in a clinical setting, for interdisciplinary assessments using qualifiers and visual profiles.
Aim
The aim here, was to describe a modified Brief ICF Core Set with qualifiers for CWP as a basis for the initial assessment of patients with long-term pain conditions in a clinical setting and for its use by an interdisciplinary pain rehabilitation team. To achieve this, a workable visual profile of the modified Brief ICF Core Set for CWP was applied to a sample of patients with long-term pain who were referred for interdisciplinary assessment and rehabilitation.
Methods and material
The modified Brief ICF Core Set for chronic widespread pain
The rehabilitation team’s need of a core set for assessment had the following criteria: (1) the profile’s capacity should fit patients with long-term pain due to varied conditions of origin (but developed into widespread pain); (2) the category should match the needs of the clinical setting (not too time consuming to use, giving an overall view of the patient’s problems); (3) the Core Set should facilitate clinical activity; (4) the comprehensive generic assessments included in the Swedish Quality Registry for Pain Rehabilitation (NRS)Citation19,Citation20 should fit the Core Set categories; (5) the amount of available information from the team members’ assessments, including the NRS, should be enough to score the categories in the Core Set after the patients had seen each team member once; and (6) it should be possible to use different assessment methods for scoring the qualifiers, for eg, interviews, questionnaires, and physical examinations, as well as performance tests carried out to improve agreement in scoring.
The Brief ICF Core Set for CWP was selected based on the criteria above.Citation10 It included 24 different categories. A slight modification of the Brief ICF Core Set was made; the list was intended to be as short as possible and only contain categories that could be scored during the limited time available at the first visit with each team member. Thus, psychomotor functions (b147), control of voluntary movement function (b760), content of thought (b1602), solving problems (d175), and support from health professionals (e355) were all excluded. Drugs (e1101) were managed by the Physical and Rehabilitation Medicine physician without the need for consensus discussions by the rehabilitation team.
Since energy level (b1300) and motivation (b1301) are different dimensions, the category of mental function (b130) was divided into two. Motivation is particularly important for rehabilitation potential and needs to be assessed separately.Citation21 Since one of the important aims of the rehabilitation program was work resumption, the category fine hand use (d440) was also included. The profile adapted to the present project contained 21 categories, 18 of which were in agreement with the original Brief ICF Core Set for CWP.Citation10
In the ICF, the amount of impairment/degree of difficulty/degree of barrier is specified using five qualifiers scored from 0 to 4. These translate to “none,” “mild,” “moderate,” “severe,” and “complete.” Each category was distributed to professionals within the team, according to the competence profile of the professional (). Thus, the category emotional functions (b152) was assessed by the psychologist, the social worker and the physician, while exercise tolerance function (b455) was assessed primarily by the physiotherapist, and doing housework (d640) was assessed by the occupational therapist.
Table 1 ICF categories, ICF codes, assessment methods and rehabilitation team members involved in assessment
Seminars on the use of the ICF classification, the scoring system, the linking of assessment methods to the categories, and the discussion of difficulties when quantifying the categories were arranged for the team.
The modified Brief ICF Core Set for CWP was used as the basis for the assessment; all patients underwent an interdisciplinary assessment during a 2-week period.
Interdisciplinary assessment
The team consisted of a PRM physician, a nurse, a psychologist, a social worker, a physiotherapist, and an occupational therapist, all with many years of experience with pain rehabilitation. The assessment took the form of a clinical examination by the physician and physiotherapist, and each team member conducted a profession-specific interview and other investigations, lasting up to about 90 minutes. All patients also underwent comprehensive general assessments included in the NRS before the interdisciplinary assessment: the Short Form (SF)-36® Health Survey (QualityMetric Inc, Lincoln, RI, USA),Citation22 the Hospital Anxiety and Depression Scale (HAD),Citation23,Citation24 the EQ-5D,Citation25 the Multidimensional Pain Inventory (MPI),Citation26 and the Chronic Pain Acceptance Questionnaire.Citation27 Other standardized tests and instruments employed were: the Test Instrument for the Profile of Physical Ability (TIPPA),Citation28 the Assessment of Motor and Processing Skills,Citation29 the Valpar Component Work Samples (VCWS),Citation30 and the Tampa Scale for Kinesiophobia.Citation31
At the end of the 2-week comprehensive assessment period, the pain rehabilitation team met for a team conference. The outcomes of all assessments, interviews, and tests were interpreted, discussed, and translated into a qualifier number by consensus. If consensus was not directly reached, the qualifier number supported by the responsible PRM physician was chosen.
The needs and goals of the patients’ rehabilitation program were formulated based on discussions between the team members and the patients. Here, the Brief ICF Core Set profile was used as an essential guide during this planning process.
Patients
A consecutive series of 53 patients referred for interdisciplinary pain rehabilitation at an outpatient pain rehabilitation clinic at the Department of Rehabilitation Medicine at the Danderyd University Hospital, Stockholm, during September 2009 to May 2010 were all (18 men and 35 women) included for study (). Of these, 90% were referred from primary health care units and 10% from other sources.
Table 2 Sociodemographic data and self-assessment outcomes
The exclusion criteria for pain rehabilitation were: current substance abuse, other current severe somatic or psychiatric disease, inability to attend group interventions due to language or social barriers, or if previous adequate rehabilitation had not shown sustained results. The patients were all transferred to the same rehabilitation team (one team out of the seven teams at the pain rehabilitation clinic).
Different professions/work categories were represented by the patients: health care (n = 6), transportation (n = 4), cleaning (n = 2), restaurant/café (n = 5), teaching (n = 4), economics and self-employment (n = 6), and miscellaneous (n = 10). Sixteen were unemployed at the time of the assessment (). The patients had persistent pain for a mean of 7 years and an average pain intensity of 6.8 (on a numeric rating scale 0–10). The mean number of pain locations was 16, and 44% described their pain location as varying. Zigmond and SnaithCitation24 suggested two cut off scores ≥11 points for detecting depression and anxiety, and accordingly, 51% in the present sample were depressed and 54% experienced anxiety, as measured by the HAD. The EQ-5D showed very low health-related quality of life and low self-perceived health.Citation25 The SF-36 Health Survey subscales showed that all the patient’s health was decreased and well below the Swedish norms (see ) for the general population.Citation22
International Classification of Disease (ICD) diagnoses of the patients with chronic widespread pain
During the patients’ stay at the outpatient rehabilitation unit, a diagnostic investigation was performed in parallel with the functional assessment. The main, or major, diagnoses, as well as comorbidities, were established. In the current national insurance system, the major diagnosis (eg, for sickness allowances) is registered first in the documentation, followed by the comorbidity diagnoses (and in some documents, only the main diagnosis is available). The same principle with major diagnoses was applied for the registration in the National Pain Registry in the present study. This means that widespread pain need not be the main diagnosis; it may be an important comorbidity but consequently, not registered first in the document. For example, a spinal pain condition that has developed into a long-lasting widespread pain condition has the spinal diagnosis as the major and first registered diagnosis and widespread pain as a comorbidity.Citation32 Further, a patient can have depression as the major diagnosis and widespread pain as a comorbidity. In the present study, the major diagnoses were used, and some of those are “widespread” by definition, such as fibromyalgia, osteoporosis, and generalized pain (, upper 26 patients). However, others are regional or local diagnoses, and therefore, the number of pain locations was used as an indicator of the spreading of pain, in addition to the regional/local diagnosis (, lower 27 patients).
Table 3 Main diagnoses, according to ICD-10, of the patients with widespread pain conditions and the number of pain locations as an indicator of the spreading of pain
Data analysis and statistics
The IBM SPSS statistics software (version 18.0; IBM, Armonk, NY, USA) was used for the analyses.
Descriptive statistics was used for describing the patients’ level of functioning and disability for each category (); the ICF qualifiers ranging from 0 to 4 were used,Citation7 and the percentages of ratings within the above qualifier groups, respectively, were calculated.
Results
Individual profiles
The available individual profile, obtained from the scoring of the modified Brief ICF Core Set for CWP, can be used as a basis for individual rehabilitation plans and goal setting, thus serving as a link between assessment and interventions. An individual profile also gives an easily accessible rapid overall view of the patient’s problems and resources, which helps understanding of the functional level of a patient.
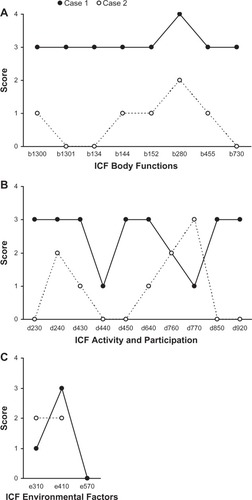
Two examples, Cases 1 and 2, of visualized profiles illustrate different patterns of functioning and disability ().
Figure 1 (A) Body Functions categories: b1300: energy and drive, b1301: motivation, b134: sleep, b144: memory, b152: emotional, b280: pain, b455: exercise tolerance, b730: muscle power. (B) Activity and Participation categories: d230: carrying out daily routines, d240: handling stress, d430: lifting and carrying, d440: fine hand use, d450: walking, d640: doing housework, d760: family relationships, d770: intimate relationships, d850: remunerative employment, d920: recreation and leisure. (C) Environment and the categories: e310: support from immediate family, e410: individual attitudes from immediate family, e570: social security service and policies.
Case 1
Case 1 was a male patient of 37 years, diagnosed with generalized pain. He was born in a country outside Europe. His highest education level was upper secondary school, and he worked as a taxi driver but had not been working for 37 months, on the grounds of sick leave. He scored a high degree of depression (HAD score 20) and anxiety (HAD score 16) and rated a low quality of life, ie, EQ-5D index = 0 [−1 to 1] and EQ-5D visual analog scale (VAS) = 15 [0 to 100]. The individual profile illustrates severe and even total impairment of the Body Functions presented (). The components of Activity and Participation illustrate severe limitations in seven categories but mild limitations in only two. Severe barrier was assessed in one category and mild/no barriers in two. Resources were seen in two categories within the component Activity and Participation, with only mild limitations and no problems regarding social security services, systems, and policies.
Case 2
Case 2 was a male patient of 45 years, diagnosed with cervicobrachial syndrome and CWP. He was born in a country outside Europe. His highest education level was university degree. He was working as an employment officer and was not, at the time of study, on sick leave. He showed no signs of depression according to the HAD (HAD score 5) but some degree of anxiety (HAD score = 11). He had low quality of life, ie, EQ-5D index = 0.19 and medium EQ-5D VA S = 60. The individual profile of case 2 () illustrates mild or no impairments in seven and moderate impairment in only one of the Body Functions presented. The dimension of Activity and Participation illustrated no or mild limitations in seven categories and moderate or severe limitations in only one. Moderate barriers were assessed in the two categories presented. Resources were seen in all Body Functions but pain, and in all but three activities (handling stress, family relationships and intimate relationships).
The profiles of the two individuals show different patterns of problems and individual resources. The differences in profiles influenced the rehabilitation planning.
Note that, as seen in , all steps in the ICF qualifier scale were utilized.
The use of group profiles
Almost all of the categories’ qualifiers were scored by one to three team members/professions using different assessment methods (). As described in Methods, consensus about the scoring number was reached at a team conference.
In the group profiles, the 53 patients showed major limitations/restrictions in the ICF component Activity and Participation. In all categories, the qualifiers none, mild, moderate, and severe were used. The qualifier “complete” was only applicable in a few categories. Thus the scale points captured the referred patients’ variations in functioning status.
Activity and Participation
Difficulties were found in all important aspects of daily life activities (). The “severe” difficulties with highest frequency were: handling stress and other psychological demands (d240) (51%); in lifting and carrying objects (d430) (51%), remunerative employment (d850) (58%), and recreation and leisure (d920) (36%). The most prominent “moderate” difficulties were: carrying out daily routine (d230) (40%), handling stress and other psychological demands (d240) (45%), and doing housework (d640) (45%) (). Few patients had “complete” difficulties.
Figure 2 The percentage of patients in each ICF category of Activities and Participation.
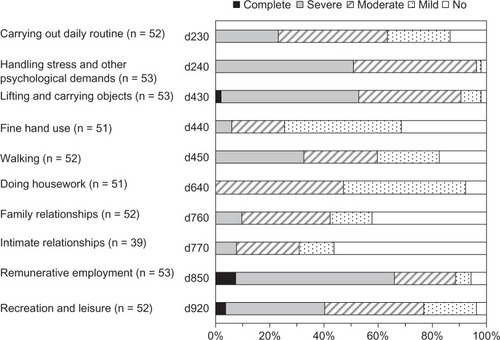
Fine-motor hand use in these patients, resources were seen in the categories of fine hand use, doing housework, intimate relationships, and family relationships.
Body Functions
In the component of Body Functions, the severe impairments with the highest frequencies were: sensation of pain (b280) (77%), exercise tolerance functions (b455) (45%), sleep functions (b134) (42%), and emotional functions (b152) (42%) (). The most prominent moderate impairments were in: muscle power functions (b730) (51%), emotional functions (b152) (49%), energy level (b1300) (42%), and in sleep functions (b134) (40%) (). Few patients had complete impairment.
Figure 3 The percentage of patients in each ICF category of Body Functions.
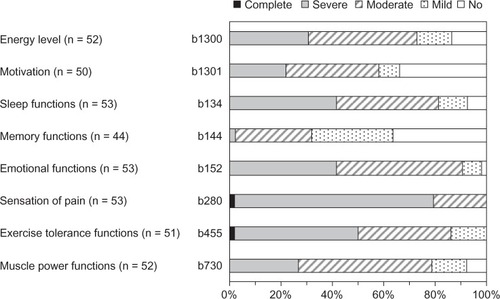
Resources were found in motivation and memory functions.
Environmental Factors
The most frequent severe barriers were: support from immediate family (e310) (12%), and attitudes of immediate family (e410) (12%) (). Approximately 25% of the patients had moderate barriers in support from immediate family (e310), and attitudes of immediate family (e410). Few patients had complete barriers in the component Environmental Factors ().
Figure 4 The percentage of patients in each ICF category of Environmental Factors.
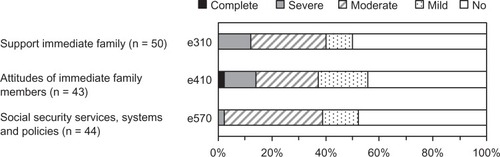
Resources were found in support and attitudes from immediate family. Social security and services, systems, and policies were assessed as a resource in 60% of the patients.
Discussion
The modified Brief ICF Core Set for CWP profile was given a workable shape to facilitate the rapid understanding of the initial assessment outcome by any of the rehabilitation team members. At first, the use of the modified Brief ICF Core Set during the team conference was rather time consuming, but after a couple of months of experience, the team assessment took approximately 30 minutes per patient. This can be compared with, due to the lack of CWP studies, a LBP study, where it was found that the clinical feasibility of the ICF Comprehensive Core Set for LBP was affected by the fact that the scoring was rather time consuming.Citation16 In that study, the time spent on coding the ICF Core Set for LBP varied from 10 to 120 minutes (mean 48 minutes, standard deviation [SD] 25 minutes). The coding lasted for >60 minutes in 22% of the cases, while in 5%, the time consumed was >90 minutes.
The visual profile provided by the modified Brief ICF Core Set also provided an easily accessible, overall view of the patient’s problems and resources, which helped in understanding the functional level of the patient. The profile provided by the modified Brief ICF Core Set for CWP was used as a basis for individual rehabilitation plans and goal setting, thus serving as a link between assessment and interventions, ie, for decisions about content of individual rehabilitation programs.
It should be noted that the study group profiles (–) can be used in two complementary directions; reading first from left to right gives an impression of the severe/moderate impairments, disabilities, and environmental barriers, while reading in the opposite direction, from right to left, gives an idea of the patients’ resources, ie, the occurrence of low qualifier numbers can be considered as patient resources. This has particular importance when planning for further vocational rehabilitation. No or mild barriers in the environmental categories also constitute relevant information. Similarly, concerning individual profiles (), high numbers in upper parts of the graphs indicate severe/moderate problems, while low numbers in lower parts of the graph suggest resources for that individual.
The two individual profiles () can be used as examples for discussing rehabilitation planning. Case 1 exemplifies how a patient with great difficulties and few resources can be assessed. The difficulties included low motivation for rehabilitation, high impact on activities, and severe pain. This has to be accounted for in the planning of motivational measures, psychological measures, such as cognitive therapy, and a carefully implemented increase in physical and daily activities. The primary long-term goal here would not be resuming work but rather, increasing the patient’s ability to manage activities in daily life.
Case 2 () exemplifies a patient with many resources and some difficulties. This patient profile includes high motivation, mild impact on activities (except for intimate relationships), and moderate pain. This patient would need less rehabilitation measures, which might include physical exercises and supportive measures for maintaining working capacity, as a long-term goal.
To our knowledge, no similar study with individual and group profiles (–), including the frequencies of the category qualifiers has been described for CWP. Due to the lack of CWP studies, a study of LBP patients, of similar scope to the present study, was used for comparison; in that study, few impairments/limitations or restrictions were scored as severe and extremely few as complete, while the qualifier zero/no problem showed high frequencies.Citation16 In the present study of Swedish CWP patients, a similar pattern of distribution of frequencies was observed, with few or none scored as severe or complete. However, the patients with LBP differed from the CWP patients in the present study in duration of pain and chronicity, since the LBP study also included patients with acute and subacute pain. On account of this, further comparisons between the two studies are not meaningful.
Limitation of the study
A limitation of the present study is the adaptation made to the original version of the Brief ICF Core Set for CWP, due to the time limitations of the primary assessment. However, the modified profile contained 21 categories, of which 18 were in agreement with the original Brief ICF Core Set for CWP.Citation10 Since one of the important aims of the rehabilitation program was work resumption, the category fine hand use (d440) was included. In a focus group study,Citation14 27 additional concepts were linked to fine hand use (d440), which may be seen as support for the addition of this category in the present study.Citation14
In an extensive study with psychometric analysis, 14 of the categories of the Brief ICF Core Set for CWP were included in the final model.Citation11 Those 14 categories did not contain: control of voluntary movement functions (b760), muscle power function (b730), lifting and carrying objects (d430), doing housework (d640), or recreation and leisure (d920), compared with the original list of the 19 categories of the components Body Functions, and Activities and Participation from the Brief ICF Core Set for CWP.Citation10 For comparison, in the present study, control of voluntary movement functions (b760) was also excluded. In addition, four categories were excluded due to apprehension of difficulties in their assessment, analysis, and scoring within a limited time; these were: psychomotor functions (b147), content of thought (b1602), solving problems (d175) and support from health professionals (e355). Excluding categories may limit an assessment; however, we argue that the modified Core Set profile covered the essential parts of the patients’ functioning. There are, in fact, several ongoing scientific studies investigating the development of the Brief and Comprehensive ICF Core Sets for CWP.Citation11,Citation14,Citation33,Citation34
Another limitation may have been the mix of primary diagnoses in the patients included. However, in our opinion, the number of pain locations documented for each patient has probably been a sufficient indicator of the spreading of pain (see ).
Clinical experience and implications
By using the modified Brief ICF Core Set for CWP, the team members experienced value in discussing the resulting profile, and the team-based assessment became more structured. By visualizing the completed easy-to-read profile, the team members got an overview of the patients’ abilities and disabilities. This can serve as a tool when discussing the rehabilitation plan with the patient. The profile provided by the modified Brief ICF Core Set for CWP may facilitate the dialogue between team members during consensus discussions and thus, probably, improve team cooperation.
Disclosure
The authors report no conflicts of interest in this work.
References
- HoefsmitNHoukesINijhuisFJIntervention characteristics that facilitate return to work after sickness absence: a systematic literature reviewJ Occup Rehabil201222446247722476607
- NorlundARopponenAAlexandersonKMultidisciplinary interventions: review of studies of return to work after rehabilitation for low back painJ Rehabil Med200941311512119229442
- ScascighiniLTomaVDober-SpielmannSSprottHMultidisciplinary treatment for chronic pain: a systematic review of interventions and outcomesRheumatology (Oxford)200847567067818375406
- Pietilä HolmnerEFahlströmMNordströmAThe effects of interdisciplinary team assessment and a rehabilitation program for patients with chronic painAm J Phys Med Rehabil2013921778323255272
- ManleySThe rehabilitation teamGraboisMGarrisonSHartKLehmkuhlLPhysical Medicine and RehabilitationMalden, Blackwell Science20002632
- ChamberlainMAFialka MoserVSchüldt EkholmKO’ConnorRJHercegMEkholmJVocational rehabilitation: an educational reviewJ Rehabil Med2009411185686919841836
- World Health Organization (WHO)International Classification of Functioning Disability and HealthGenevaWorld Health Organization2001
- WormgoorMEIndahlAvan TulderMWKemperHCFunctioning description according to the icf model in chronic back pain: disablement appears even more complex with decreasing symptom-specificityJ Rehabil Med2006382939916546765
- CiezaAStuckiGWeiglMICF Core Sets for low back painJ Rehabil Med200444Suppl 44S69S74
- CiezaAStuckiGWeiglMICF Core Sets for chronic widespread painJ Rehabil Med2004Suppl 44S63S68
- ProdingerBSalzbergerTStuckiGStammTCiezaAMeasuring functioning in people with fibromyalgia (FM) based on the international classification of functioning, disability and health (ICF) – a psychometric analysisPain Pract201212425526521797963
- CerniauskaiteMQuintasRBoldtCSystematic literature review on ICF from 2001 to 2009: its use, implementation and operationalisationDisabil Rehabil201133428130921073361
- MullisRBarberJLewisMHayEICF core sets for low back pain: do they include what matters to patients?J Rehabil Med200739535335717549324
- HieblingerRCoenenMStuckiGWinkelmannACiezaAValidation of the International Classification of Functioning, Disability and Health Core Set for chronic widespread pain from the perspective of fibromyalgia patientsArthritis Res Ther2009113R6719442275
- HilfikerRObristSChristenGLorenzTCiezaAThe use of the comprehensive International Classification of Functioning, Disability and Health Core Set for low back pain in clinical practice: a reliability studyPhysiother Res Int200914314716619194959
- Bautz-HolterESveenUCiezaAGeyhSRøeCDoes the International Classification of Functioning, Disability and Health (ICF) core set for low back pain cover the patients’ problems? A cross-sectional content-validity study with a Norwegian populationEur J Phys Rehabil Med200844438739719002088
- RøeCSveenUCiezaAGeyhSBautz-HolterEValidation of the Brief ICF core set for low back pain from the Norwegian perspectiveEur J Phys Rehabil Med200945340341419396057
- MainiMNocentiniUPrevediniAGiardiniAMuscoloEAn Italian experience in the ICF implementation in rehabilitation: preliminary theoretical and practical considerationsDisabil Rehabil200830151146115219230223
- NybergVSanneHSjölundBHSwedish quality registry for pain rehabilitation: purpose, design, implementation and characteristics of referred patientsJ Rehabil Med2011431505721042698
- NybergVPain Rehabilitation in Sweden: A Quality Registry Study [doctoral thesis]UmeåUmeå University2011 Available from: http://umu.diva-portal.org/smash/record.jsf?searchId=1&pid=diva2:416699Accessed June 3, 2013
- GardGLarssonAFocus on motivation in the work rehabilitation planning process: a qualitative study from the employer’s perspectiveJ Occup Rehabil200313315916712966690
- TaftCKarlssonJSullivanMPerformance of the Swedish SF-36 version 2.0Qual Life Res200413125125615058805
- LisspersJNygrenASödermanEHospital Anxiety and Depression Scale (HAD): some psychometric data for a Swedish sampleActa Psychiatr Scand19979642812869350957
- ZigmondASSnaithRPThe hospital anxiety and depression scaleActa Psychiatr Scand19836763613706880820
- BurströmKJohannessonMDiderichsenFSwedish population health-related quality of life results using the EQ-5DQual Life Res200110762163511822795
- BergströmGJensenIBBodinLLintonSJNygrenALCarlssonSGReliability and factor structure of the Multidimensional Pain Inventory – Swedish Language version (MPI-S)Pain19987511011109539679
- McCrackenLMVolwesKEEcclestonCAcceptance of chronic pain: component analysis and a revised assessment methodPain20041071–215916614715402
- Missaghi-WedefalkMTest Instrument for profile of physical ability = TippaNordisk Fysioterapi200487483
- FisherAGThe assessment of IADL motor skills: an application of many-faceted Rasch analysisAm J Occup Ther19934743193298322873
- DusikLAMenardMRCookeCFairburnSMBeachGNConcurrent validity of the ERGOS work simulator versus conventional functional capacity evaluation techniques in a workers’ compensation populationJ Occup Med19933587597678229325
- LundbergMStyfJCarlssonSA Psychometric evaluation of the Tampa Scale for Kinesiophobia – from a physiotherapeutic perspectivePhysiotherapy Theory and Practice2004202121133
- LarssonBBjörkJBörsboBGerdleBA systematic review of risk factors associated with transitioning from regional musculoskeletal pain to chronic widespread painEur J Pain20121681084109322362638
- BrageSDonceelPFalezFWorking Group of the European Union of Medicine in Assurance and Social SecurityDevelopment of ICF core set for disability evaluation in social securityDisabil Rehabil200830181392139618850352
- FingerMEEscorpizoRGlässelAICF Core Set for vocational rehabilitation: results of an international consensus conferenceDisabil Rehabil201234542943821981443