
Abstract
Background
Maternity health management has always been the area of concern and considering, and considering its complexity and multidisciplinary, it is necessary to provide effective training for healthcare workers.
Purpose
To evaluate the impact of a multidisciplinary experiential training model on the knowledge, attitude, and practice of healthcare workers in maternity health management.
Patients and Methods
We conducted a novel educational model, Multidisciplinary Maternity Health Experiential Training based on Knowledge, Attitude and Practice (MMHET), which combined theoretical knowledge, practical skills, and human-centred humanistic care, offering a comprehensive offline education program supported by online teaching materials structured around knowledge graphs. Pre- and post-test surveys were used to assess the changes in participants’ knowledge, attitudes, and practices.
Results
From May to July 2023, a total of 322 participants attended the course, and only a small percentage had participated in experiential training. For all topics, the vast majority of participants endorsed the course, and the attitude content had the highest percentage of participants who said they agreed. Among the groups with different years of working life, the highest percentage of participants in the >20 years group strongly endorsed the course.
Conclusion
The preliminary findings indicate that the MMHET model is well-received and feasible, demonstrating its potential to enhance maternity health management education.
Introduction
Maternity health management refers to the women’s health care during pregnancy, childbirth and the postnatal period, and is an integral part of the health of mothers and children. The World Health Organization (WHO) estimates that in 2020, approximately 287,000 women died during and after pregnancy and childbirth, with a disproportionate impact on low- and middle-income countries where pregnant populations are more susceptible to adverse outcomes, including stillbirths and early neonatal deaths.Citation1 These deaths are often accompanied by adverse outcomes such as stillbirths and early neonatal deaths, highlighting the persistent challenges in maternal health care.Citation2,Citation3
The high rates of maternal morbidity and mortality suggest that there are gaps in the quality of maternal health management.Citation4 One of the key issues is the need for effective training of healthcare workers, who are at the forefront of providing care during these critical periods.Citation5 Traditional education has primarily focused on delivering professional knowledge, yet there is a growing recognition of the importance of applying this knowledge in real-world clinical settings.Citation6
To address this gap, there has been a shift towards experiential training experiential training (ET), which is a multi-directional interactive teaching method that immerses students in interactive, scenario-based learning. ET is designed to help healthcare workers not only understand theoretical knowledge but also to apply it in practical, clinical situations. This approach is particularly relevant in maternal health, where the ability to respond effectively to complex and varied clinical presentations is crucial.
While expertise in the form of clinical practice proficiency is important, it is no longer the only indicator of maternity health management. Moreover, the focus on maternal health management has expanded beyond clinical proficiency to include human-centered humanistic care. Studies have shown that a patient-centered approach, which involves considering the emotional and psychological needs of pregnant women, can significantly improve health outcomes. This approach requires healthcare workers to be trained not only in medical work but also in empathetic communication and emotional support.Citation7–10
Given the importance of both clinical skills and humanistic care, this study integrates humanistic care into ET, establishing a novel educational model that combines knowledge, attitude and practice. It aims to provide multidisciplinary offline education for healthcare workers, supported by standardized teaching materials based on a knowledge graph.
Materials and Methods
Participants
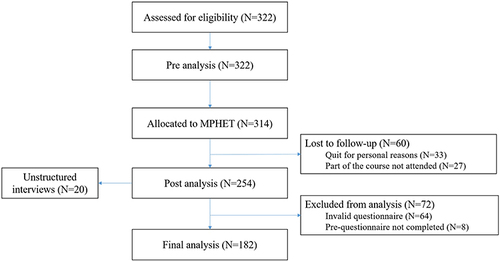
This study used purposive sampling to identify participants with relevant expertise, and inclusion criteria were healthcare workers in the field of maternity health from various hospitals in Beijing, including obstetricians, midwives, nurses, etc. To be included, candidates had to be healthcare professionals actively engaged in maternal healthcare services within various hospitals across Beijing and participants should not have previously served as instructors in ET settings. We will conduct 10 cycles of “Multidisciplinary Maternity Health Experiential Training based on Knowledge, Attitude and Practice (MMHET)” at a prestigious tertiary hospital in Beijing in a snowballing approach to sample collection. After obtaining consent, participants will be asked to complete an anonymous questionnaire before and after participating in the course. The participants inclusion process is shown in .
Figure 1 Participants inclusion process.
Study Design
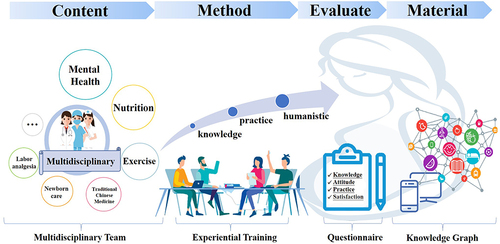
An overview of the MMHET model is shown in . The MMHET is an innovation of maternity health education, with four modules: content, method, evaluation and materials. Covering crucial topics like mental health and nutrition, it employs ET to develop healthcare workers’ theoretical knowledge, practical skills, and humanistic attitudes, and continuous evaluation through questionnaires ensures that educational objectives are met. It also provides a Knowledge Graph-based educational material module, which provides a wealth of educational resources to improve healthcare workers’ expertise in maternal health.
Figure 2 MMHET model.
Teaching Content
Our multidisciplinary team consists of multidisciplinary specialists in obstetrics, nutrition, psychology, dentistry, Traditional Chinese Medicine and sports medicine. Before the course was launched, we conducted literature research on education and teaching programs at home and abroad, as well as studies on maternity health management, and held regular multidisciplinary meetings. After several rounds of discussion by the multidisciplinary team, we summarized the experiences of domestic and international continuing education courses for maternity health management and determined the focuses of this course by combining the common problems or concerns in the practice of maternity health management in Beijing, and finally formulated the teaching modules and contents. Each session lasts 5 days, totaling 10 sessions, as shown in the . To fulfill the role of educator, all multidisciplinary team members had at least 5 years of experience in maternity health management.
Table 1 Teaching Content
Teaching Methods
A Safe, Equitable and Comfortable Teaching Environment
We set up a round table model to provide a safe, equitable and comfortable teaching environment. All participants (including instructors) are in a circle, allowing for multi-dimensional interaction and equidistant communication between any two participants. Providing a safe place for participants to practice skills has been shown to improve self-efficacy, confidence, and the ability to handle tasks in complex environments.Citation11,Citation12
Improve Interpersonal and Communication Skill
Research has found that the most effective method of interpersonal and communication skills training is ET,Citation13 and effective communication is the foundation of quality care, which could enhance the interpersonal and communication skills of healthcare workers allows for better clinical interpretation, listening and empathy.Citation14 The round table setting provides a good environment for communication, where all participants (including the instructor) can express and listen, includes viewpoints or problems during the case study, suggestions for the course, and their own experiences.
Pregnant Women are Invited to Course
In case practice teaching, we invite pregnant women to participate in the classroom, that allows participants to experience the real emotions of pregnant women and to listen to any difficulties encountered by pregnant women in a respectful and caring manner, so that they can take targeted measures to help pregnant women, provide them with quality health services, and enhance their sense of self-responsibility.
Multidisciplinary Collaborative
Since the participants in this course have different professional backgrounds, the teaching methods also includes multidisciplinary collaborative.Citation15,Citation16 For example, a case study approach will be used so that all trainees will be able to engage in a case study with different professional backgrounds.
Timely Course Feedback
We establish online discussion groups for both participants and instructors, where participants can give feedback on the course content at any time, including post-class feelings, course questions, teaching comments, etc. Timely feedback allows participants to master the knowledge process conscious reflection and allows instructors the opportunity to make appropriate modifications, thus promoting better education.
Effect Evaluation
The survey was electronically distributed and completed via “wenjuanxing”, a secure, web-based application designed for data collection for research studies. A semi-structured questionnaire based on a literature review and discussions with multidisciplinary was developed using the KAP framework.Citation17–19 The framework, a validated public health tool for assessing the effectiveness of intervention programs, is one of the most widely used models in medical education.Citation20 Healthcare workers’ knowledge, attitudes, and practice are determinants of quality continuing education and better delivery of health care services to pregnant women.Citation21 Our aim is to evaluate the impact of the educational model on KAP of healthcare workers for maternity health.
We designed “Knowledge, Attitude, Practice (KAP)-Based Questionnaire” to evaluate the impact of the educational model on the knowledge, attitudes, and practice of healthcare workers.
The evaluation questionnaire includes demographic information, knowledge, attitude, practice, and satisfaction. Responses were presented on Likert-5 scale, on a scale of 1 to 5, with 5 questions per module out of 25 scores. ()
Table 2 Evaluation Content
Teaching Materials
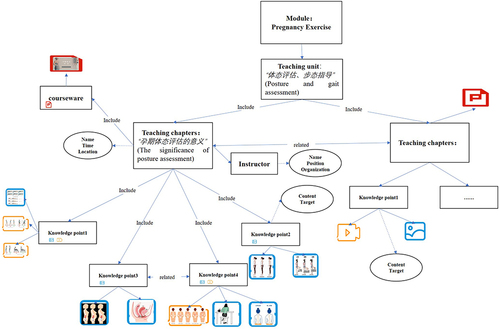
The online teaching materials in this study will combine the characteristics of multimodal teaching resources such as pictures and videos, and utilize multimodal knowledge graph to standardize, structure, and semantically express maternity health teaching materials. The top-level ontology structure of the multimodal knowledge graph includes teaching resources, people, teaching tools, periods, and topics. In the teaching resources, the content is split and organized using four different granularities of teaching resources: teaching courses, teaching units, teaching chapters, and knowledge points.
Data Analysis
Participant characteristics were summarized with Mean and SD for quantitative variables and relative and absolute frequencies for qualitative variables. The reliability of the scales was tested using the internal consistency reliabilities (Cronbach’s α). Statistical analysis was performed using SPSS and R software.
Results
A total of 182 questionnaires were included with a return rate of 59.0%, showed the basic information of the participants (n=182). The mean age of the participants was 39.75 ± 8.16 years, the vast majority were female. About half of the participants were aware of ET, but only a small percentage had participated in. This discrepancy suggests a significant opportunity for professional development in the area of ET within the maternity health field.
Table 3 Basic Characteristics of Participants
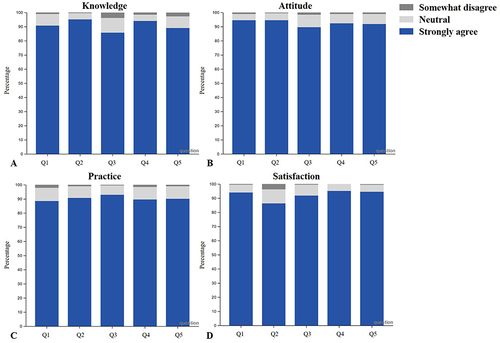
showed the results for all topics in the four aspects, the vast majority of participants endorsed the course, and the attitude content had the highest percentage of participants who said they agreed. We categorized the participants into 3 groups based on working life, <10 years (n=47), 10~20 years (n=74), and >20 years (n=61). showed the results of by the different groups, compared to the other groups, the percentage of “somewhat disagree” is extremely low for >20 years group. This could imply that more experienced healthcare workers found the course particularly beneficial, possibly due to its multidisciplinary and experiential approach complementing their extensive practice with new theoretical insights. provides a module-wise breakdown of the ratings for all questions. The attitude and practice modules received better ratings, suggesting that the MMHET program was particularly successful in enhancing these dimensions among participants. However, a minority of participants gave “somewhat disagree” results for Q3 in the knowledge module. This feedback is valuable for identifying areas that may require curricular adjustments or additional focus.
Figure 3 Ratings overall and by working life group.
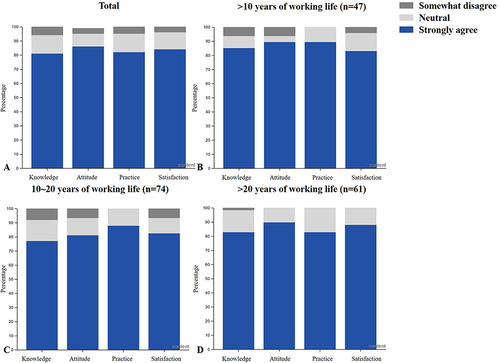
Figure 4 Ratings of different modules.
In addition to the above assessment questions, we set simple questions to obtain participants’ suggestions and feelings about different aspects of the course. Below were the feelings from three participants who completed the course.
Thank you to multidisciplinary team for providing learning opportunities for every participant. The course has allowed me to develop a professional, safe and cutting-edge clinical mindset. For what I see, hear and feel, recording it into words, forming my own thinking, being creative and helping others is the best growth I can have.
The Psychological Support course took me to draw a genogram and experience sculpture, which helps practitioners of counseling and therapy maintain a systemic view of the visitor and his or her family system. This is the first time I have experienced, very touching and moving, may I stay optimistic and love myself and my family.
After completing the course, I feel that I not only need to master the theoretical knowledge more importantly, I need to spread the clinical practice and good humanistic care skills to various local hospitals. I hope to have the opportunity to attend more courses in the future from participants.
In knowledge graph-based online educational materials, the top-level ontology consists of 40 classes, 10 relationships, 13 attributes, 2 courses and 24 teaching units. According to the structure of the top-level ontology, we selected the course “Physical Assessment and Gait Guidance” as an example, and the shown a teaching unit of the course.
Figure 5 Knowledge Graph Prototype.
Discussion
This study proposed an educational model (MMHET) for healthcare workers and evaluated the effectiveness of it using a quasi-experimental study to improve the quality of care for maternity health and the development of maternity health education.
showed that the assessment results for the group with >20 years of working life are in line with our expectations, but we are exploring the reasons for the results for the group with 10~20 years of working life. Since our data analysis followed unstructured interviews, we did not target groups of 10~20 years, while other information about the acceptance and satisfaction of the MMHET across different years of working life needs to be further investigated. both showed that the attitude was rated the best, which may be due to the fact that the MMHET incorporated humanistic teaching based on ET. Some studies have pointed out that healthcare workers have more duties than merely treating patients, and they require qualities other than medical knowledge, such as career-long humanistic values and humanistic care for patients, which cannot be learned in the traditional educational model.Citation22 To delve deeper into these findings, further analysis could examine the relationship between years of experience and knowledge, as well as the integration of attitudes and practices. It would also be insightful to conduct a qualitative review of the responses to Q3 to understand the reasons behind the lower ratings and to explore whether this is related to the content, delivery, or participants’ prior knowledge.
A study focused on assessing healthcare workers’ attitudes and knowledge of safe medication administration during breastfeeding.Citation23 However, practical skills are equally vital, bridging medical theory with clinical practice and establishing core competencies for healthcare providers. Based on this, there have also been studies that have utilized the knowledge, attitudes, and practices framework to evaluate the educational level of maternity healthcare workers regarding perinatal depression.Citation24 The study has underscored the importance of mental health education for healthcare providers. Multidisciplinary education fosters a comprehensive understanding of patient care by integrating knowledge from various medical fields. It is in this context that the advantages of a multidisciplinary approach to medical education become particularly evident for maternity healthcare workers.Citation25 Our model not only emphasizes the significance of mental health but also leverages the multidisciplinary integration advantage by effectively combining mental health with other aspects of health, such as exercise.
Emerging interactive teaching strategies like the MMHET are receiving increasing attention in medical education but their effectiveness has hardly been evaluated.Citation26 In response to the teaching characteristics of theoretical knowledge, clinical practice and humanistic care, our study designed an evaluation scheme to assess the teaching effectiveness in KAP. Since the attitudes and practice aspects are more abstract, so we used the Likert-5 scale to obtain changes in healthcare workers’ knowledge, attitude, and practice through their self-assessment. We ensured that the evaluation questions were as relevant, easy to understand and non-divergent as possible, and assessed the reliability of all items in a quasi-experimental study, all internal consistency reliabilities (Cronbach’s α) achieving 0.8 or higher, demonstrating the feasibility of the evaluation scheme.
The teaching materials of the course adopts multimodal knowledge graphs and is constructed based on the top-level logical framework of the ontology to meet the subsequent needs such as semantic reasoning. The knowledge graph realizes the retrieval and visualization of maternity health knowledge points, and allows access to all kinds of multimodal teaching materials related to the knowledge points, so that trainees can complete the sorting out and reviewing of the course knowledge points, and check for gaps in a timely manner. At the same time in the form of multimodal for trainees to bring a clearer and more intuitive learning effect, but also to recommend appropriate personalized learning resources and plan the learning path of the course. In addition, this standardized online teaching materials can be expanded to different levels of hospitals and other healthcare venues to provide convenient, low-cost, standardized online teaching guidance.
Limitations: 1) the results of the study cannot avoid a certain degree of subjectivity; 2) the lack of a control group; 3) due to the small class size of the ET, the overall effective sample data is small and the data collection period was long; 4) the content of humanistic teaching is abstract and some participants cannot understand and master the relevant teaching content well; 5) the course requires participants must come to the scene to achieve better teaching effect.
Despite these limitations, this study had several clinical and research implications. The successful implementation of this study proves the feasibility of the new educational model for workers in maternity health management. In addition, the new module is still being applied and attempted to be implemented in different regions and levels of hospitals or healthcare organizations. More rigorous, large-sample controlled trials are needed to validate its effectiveness in the future to facilitate the successful application of the MMHET.
Conclusion
The preliminary findings indicate that the new educational model, the MMHET, is well-received and feasible, demonstrating its potential to enhance maternity health management education. Although the model could be generalized to some extent to other subject areas, there is a need for ongoing improvement. Future validation of its effectiveness should be conducted using controlled trials with larger samples.
Ethics Approval and Consent to Participate
Permission to carry out the present study was obtained from the Ethics Committee of Chinese Academy of Medical Sciences & Peking Union Medical College (I-23PJ812). Participants were informed that they could leave the study whenever they wished. Informed consent forms were also obtained from participants and they were assured that leaving the study would not have any negative consequences for them.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We thank all multidisciplinary teaching team for Maternity Health Management and all those that participated in the study. This study was supported by the CAMS Innovation Fund for Medical Sciences (CIFMS) (Grant No.2021-I2M-1-056).
References
- Adebe KL, Wake SK, Mekebo GG, et al. Analysis of regional heterogeneity and determinants of perinatal mortality in Ethiopia: review. Ann Med Surg. 2023;85(4):902–907. doi:10.1097/MS9.0000000000000400
- Requejo JH, Bryce J, Barros AJ, et al. Countdown to 2015 and beyond: fulfilling the health agenda for women and children. Lancet. 2015;385(9966):466–476. doi:10.1016/S0140-6736(14)60925-9
- Norris M, Klabbers G, Pembe AB, et al. A growing disadvantage of being born in an urban area? Analysing urban-rural disparities in neonatal mortality in 21 African countries with a focus on Tanzania. BMJ Glob Health. 2022;7(1). doi:10.1136/bmjgh-2021-007544
- Smith RM, Calvert B, Kata E, et al. Midwifery education in Pacific Island countries: a discussion paper. Women Birth. 2023;36(6):e605–e12. doi:10.1016/j.wombi.2023.05.008
- Stritzke A, Murthy P, Fiedrich E, et al. Advanced neonatal procedural skills: a simulation-based workshop: impact and skill decay. BMC Med Educ. 2023;23(1). doi:10.1186/s12909-023-04000-1
- Gebremichael MA, Lema TB. Prevalence and predictors of knowledge and attitude on optimal nutrition and health among pregnant women in their first trimester of pregnancy. Int J Womens Health. 2023;15:1383–1395. doi:10.2147/IJWH.S415615
- Reis-Dennis S. Review of rethinking health care ethics by Stephen Scher and Kasia Kozlowska: Palgrave Macmillan, available open access. Monash Bioeth Rev. 2020;38(1):83–86. doi:10.1007/s40592-020-00107-z
- Dai J, Yu Y, Wang Y, et al. The experience of pregnant women in the health management model of internet-based centering pregnancy: a qualitative study. Int J Womens Health. 2022;14:1281–1289. doi:10.2147/IJWH.S375675
- Craft-Blacksheare M, Kahn P. Midwives’ and other perinatal health workers’ perceptions of the black maternal mortality crisis in the United States. J Midwifery Womens Health. 2023;68(1):62–70. doi:10.1111/jmwh.13433
- Alves SP, Costa T, Ribeiro I, Nene M, Sequeira C. Perinatal mental health counselling programme: a scoping review. Patient Educ Couns. 2023;106:170–179. doi:10.1016/j.pec.2022.10.347
- Dieterich R, Demirci J. Communication practices of healthcare professionals when caring for overweight/obese pregnant women: a scoping review. Patient Educ Couns. 2020;103(10):1902–1912. doi:10.1016/j.pec.2020.05.011
- Silberman NJ, Litwin B, Panzarella KJ, Fernandez-Fernandez A. High fidelity human simulation improves physical therapist student self-efficacy for acute care clinical practice. J Phys Ther Educ. 2016;30(1):14–24. doi:10.1097/00001416-201630010-00003
- Parry RH, Brown K. Teaching and learning communication skills in physiotherapy: what is done and how should it be done? Physiotherapy. 2009;95(4):294–301. doi:10.1016/j.physio.2009.05.003
- Tuohy D. Communication skills for nursing practice. J Clin Nurs. 2008;17(12):1680. doi:10.1111/j.1365-2702.2007.02058.x
- Liu C, Li W, Liu T, et al. Effect of multidisciplinary collaborative empowerment education on psychological distress and quality of life in patients with colorectal cancer undergoing chemotherapy. Support Care Cancer. 2023;31(2):116. doi:10.1007/s00520-023-07573-1
- Russ MJ. The psychiatric inpatient multidisciplinary team meeting: a model for current practice. J Psychiatr Pract. 2021;27(2):101–108. doi:10.1097/PRA.0000000000000532
- Mert-Karadas M, Yucel-Ozcirpan C. The impact of an educational program based on the reproductive health of LGBT individuals developed for nursing students to improve the knowledge, skills and attitudes of students: a quasi-experimental study. Nurse Educ Pract. 2023;70:103668. doi:10.1016/j.nepr.2023.103668
- Alzghoul BI, Abdullah NA. Pain management practices by nurses: an application of the Knowledge, Attitude and Practices (KAP) Model. Glob J Health Sci. 2015;8(6):154–160. doi:10.5539/gjhs.v8n6p154
- Guo T, Sun Y, Knowledge LG, Ali L. Attitude, and practice regarding narrative medicine among Chinese medical personnel: an online cross-sectional survey. Comput Math Methods Med. 2022;2022:3329360. doi:10.1155/2022/3329360
- Szymona-Palkowska K, Janowski K, Pedrycz A, et al. Knowledge of the disease, perceived social support, and cognitive appraisals in women with urinary incontinence. Biomed Res Int. 2016;2016:3694792. doi:10.1155/2016/3694792
- Zhang YB, He L, Gou L, et al. Knowledge, attitude, and practice of nurses in intensive care unit on preventing medical device-related pressure injury: a cross-sectional study in western China. Int Wound J. 2021;18(6):777–786. doi:10.1111/iwj.13581
- Chen L, Zhang J, Zhu Y, Shan J, Zeng L. Exploration and practice of humanistic education for medical students based on volunteerism. Med Educ Online. 2023;28(1):2182691. doi:10.1080/10872981.2023.2182691
- Al-Sawalha NA, Sawalha A, Tahaineh L, Almomani B, Al-Keilani M. Healthcare providers’ attitude and knowledge regarding medication use in breastfeeding women: a Jordanian national questionnaire study. J Obstetrics Gynaecol. 2017;38(2):217–221. doi:10.1080/01443615.2017.1345876
- Kaushal S, Gupta J, Priya T. Knowledge, attitude, and practices of healthcare providers about perinatal depression in Himachal Pradesh—A cross-sectional study. J Fam Med Prim Care. 2023;12(3):478. doi:10.4103/jfmpc.jfmpc_1170_22
- Vinayak S, Temmerman M, Villeirs G, Brownie S. A curriculum model for multidisciplinary training of midwife sonographers in a low resource setting. J Multidiscipl Healthc. 2021;14:2833–2844. doi:10.2147/JMDH.S331371
- Xie H, Wang L, Pang Z, Chen S, Xu G, Wang S. Application of problem-based learning combined with a virtual simulation training platform in clinical biochemistry teaching during the COVID-19 pandemic. Front Med. 2022;9:985128. doi:10.3389/fmed.2022.985128