
Abstract
Background
Stress urinary incontinence (SUI) is effectively managed through pelvic floor muscle training (PFMT), yet poor adherence often undermines its efficacy. Given square dancing’s popularity among middle-aged women, its integration with PFMT could potentially increase patient compliance. This study aims to investigate the impact of a hybrid program combining square dance and PFMT on SUI symptoms, quality of life, and treatment adherence in this demographic.
Methods
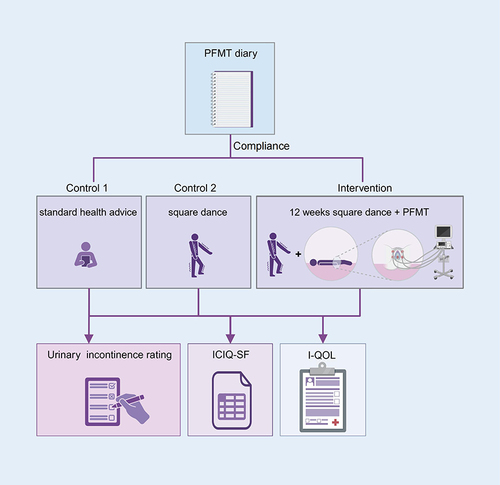
Seventy-seven female participants from Luoyang were randomly allocated to an intervention group undergoing a 12-week program combining square dancing with PFMT, and two control groups receiving standard health advice or square dancing alone. Outcomes were assessed using subjective urinary incontinence rating, the International Consultation on Incontinence Questionnaire Short Form (ICIQ-SF), and the Urinary Incontinence Quality of Life Scale (I-QOL), and a PFMT diary for compliance. Satisfaction was scored on a 10-point scale.
Results
Participants (mean age: 53.35±5.11 years) did not differ significantly at baseline. Post-intervention, the intervention group showed significant improvements in SUI symptoms and quality of life compared to both control groups (P < 0.05), with higher compliance (96.54% vs 54.82% in control I) and satisfaction (8.86±0.85).
Conclusion
Combining PFMT with square dancing significantly improved SUI symptoms, quality of life, and adherence among middle-aged women. Notably, despite the COVID-19 pandemic and associated restrictions during the 12-week intervention period, the communal and enjoyable nature of square dancing likely contributed to enhanced motivation and satisfaction.
Graphical Abstract
Introduction
Stress urinary incontinence (SUI) is the most common UI (urinary incontinence).Citation1 Women aged 40–60 years are more susceptible to this disease.Citation2 SUI treatments include surgery, medication, and behavior therapy.Citation3 The International Consultation on Incontinence recommends pelvic floor muscle training (PFMT) as an evidence-based first-line treatment for SUI, advising most patients to attempt PFMT before drug treatment or surgery.Citation3 However, the effect of PFMT lies in patients’ long-term adherence. Moreover, once you stop exercising, incontinence symptoms may reappear.Citation4 Short-term PFMT adherence was 64%; long-term adherence was only 23%.Citation5 Adherence is the key factor in maintaining PFMT efficacy.
There are many ways to improve PFMT adherence, like mobile applications (APP),Citation6,Citation7 continuous guidance,Citation7 repeated reminders,Citation5 interventions based on nursing management concepts,Citation8 and so on. However, those interventions are costly, require more medical personnel or fail to motivate patients to participate in the exercise.
Some studies have shown that recreational programs such as belly dance,Citation9 yoga,Citation10 and rumba danceCitation11 can exercise the pelvic floor muscles and improve patients’ compliance. So-YoungCitation11 pointed out that in order to be successful in engaging the patients’ sustained participation, the pelvic floor exercise program should be more interesting and entertaining.
Square dancing is the most common recreational exercise in China. About 87.63% of exercisers are female, and their age ranges from 41 to 60.Citation12 Women at this age are at high risk for SUI.Citation13 Compared to other treatments, square dancing participants tend to exercise in groups, making it easier to increase patients’ motivation and exercise engagement through group therapies and peer education. Thus, the authors suppose that if we create a square-dancing incorporating PFMT for middle-aged women with SUI that is more convenient and entertaining, their compliance with PFMT might be improved. Therefore, the authors hypothesize that the development of a square-dancing program incorporating PFMT for middle-aged women suffering from SUI, designed to be both more convenient and entertaining, could enhance adherence to PFMT. Concurrently, such an intervention is expected to manage symptoms of urinary incontinence effectively and improve the participants’ quality of life.
Hence, this study aims to create a square-dancing program incorporating PFMT and examine its effect on urinary incontinence symptoms, quality of life and compliance to PFMT among middle-aged women with SUI.
Methods
This quasi-experimental study adopted a randomized controlled pretest-posttest follow-up research design with 3 study groups (1 intervention group and 2 control groups). Approval from the ethics committee was obtained. Written, fully informed consent was obtained from all participants, and all data were confidentially collected. Participants could quit the study at any time.
Participants
Participants who met the diagnostic criteria for SUI following the International Consultation on Incontinence Questionnaire Short Form (ICIQ-SF) were recruited from three geographically isolated communities in Luoyang, a city in central China, from July to October 2021 (Clinical Trial Registration Number: ChiCTR2100044354). Participants were included if they: (1) were 40–60 years; (2) had mild or moderate symptoms by Ingelman-Sundberg indexing; (3) had the intention of treatment; (4) could talk and walk without assistance; (5) could understand the study procedure and were willing to participate. Participants were excluded from the study if they: (1) were pregnant; (2) had severe symptoms requiring surgical treatment; (3) had urinary system infection during the study; (4) had participated in relevant researches before; (5) were acute exacerbation of chronic diseases and mental disorders; (6) were within three months after pelvic surgery; (7) had central nervous system damage and severe cardiopulmonary dysfunction. To avoid contamination, participants were divided into three groups based on their respective communities, with all participants from the same community being allocated to the same group.
To determine the appropriate sample size for this study, we utilized the formula for sample mean comparison, taking into account the statistical power considerations, effect size, and variability of the data. The formula used was:
where uα and uβ are the critical values from the standard normal distribution corresponding to the specified type I and type II error rates, respectively; S represents the standard deviation of the population, and δ is the expected difference in means (effect size). Referring to the study of Eleni,14 δ= 1.4, S = 1.3. Specifically, we assume the test level α = 0.05 (two-sided) and a desired test efficacy (power) of 1 - β = 0.9 (β = 0.1). Given these parameters, the initial calculation yielded a sample size of 20 for each group. However, to account for potential dropouts (assumed to be 20% based on similar studies), we adjusted the sample size upwards, resulting in a final sample size of 24 per group.
A total of 77 participants were finally included in the study, with the age of 53.35±5.11 years old. Among them, 16.9% had cesarean sections, 62.3% delivered vaginally, and 20.8% had both forms. The economic status of participants varied, with 15.6% earning less than 3000 yuan per month, 15.6% earning 3000–5000 yuan, 41.6% within the 5000–8000 yuan, and 27.3% earning over 8000 yuan. The educational level of the participants varied: 14.3% had primary education or less, 33.8% had completed junior high school, 40.3% had finished high school or technical secondary school, and 11.7% held a university degree or higher.
Interventions
Interventions for the Experimental Group
The participants of the experimental group received square dancing with PFMT. The Guidelines for the Diagnosis and Treatment of Stress Urinary Incontinence in WomenCitation15 claimed that PFMT’s effectiveness lies in adequate training. Each PFMT movement should continue to contract for at least 3 seconds, relax for 2–6 seconds, repeat pelvic floor muscle contraction and relaxation for 15–30 minutes, and practice three times daily.
However, a normal square-dancing rhythm is too fast to enhance the pelvic floor muscle. Therefore, the authors selected three movements that help keep pelvic floor muscle contract and maintain by consulting literature and experts, together with a professional choreographer. We made these movements into four square dancing. Then, sports medicine specialists reviewed these dances and deleted the movements that may increase abdominal pressure, increasing the duration of contraction and relaxation movements.
Finally, these dances have three main movements, and the active contraction of the perineum and anal muscles is added. These movements are: (1) Heel raising: Bring legs together and heels facing each other, slowly lift heels, slowly contract the pelvic floor muscle while lifting the heels, and reach the maximum when the heel is lifted to their highest point, slowly lower heels after 3–5 seconds, and slowly relax the pelvic floor muscle while lowering the heels. (2) Leg opening and closing: The distance between the two legs is about shoulder width; relax the pelvic floor muscle while separating legs. Move the legs apart slowly, then slowly close the legs together. When closing, contract the pelvic floor muscles to the maximum extent, and hold for 3–5 seconds. (3) Leg crossing: The legs are positioned together, with one leg remaining stationary while the other crosses over it. During the leg cross, the pelvic floor muscles are contracted; maximum contraction is achieved when the legs are fully crossed and is sustained for 3–5 seconds. The legs then slowly return to the upright position, with the muscles relaxing as they revert to their original position.
In each movement, the pelvic floor muscle should contract for at least 3 seconds and relax for 2–6 seconds. Each dance lasts about 3 min, including contraction and relaxation about 20–30 times. Following the intervention process, patients practice daily. The daily intervention is shown in .
Table 1 Daily Intervention Process
Before formal intervention, a 4-week pre-experiment was conducted on two female SUI patients who met the inclusion criteria from April 1st to 28th, 2021. After the pre-experiment, the number of dances increased to 6, and the centralized exercise time was changed to 20:00–21:00 daily. If they missed the centralized exercise time, the study participants could make up the workout independently following the protocol. Researchers contacted participants in all three groups weekly for at least three months to answer questions about training and stress urinary incontinence.
Interventions for the Control Group
The control group I received conventional health education for SUI, including a Stress Urinary Incontinence Health Education Brochure containing information on the prevention and treatment of stress urinary incontinence and PFMT.
The control group II received routine square dancing and the Health Education Brochure. However, the square dance performed by control group II did not contain movements similar to the intervention group’s. Or, even if there are similar movements, they would not work the pelvic floor muscles because of their fast pace.
Data Collection
At baseline, general data like age, height, weight, education, and economic status of the patients, and clinical data like mode of delivery, frequency of delivery, duration of urine leakage, and disease history were collected with a self-designed questionnaire. Questionnaires were collected by trained researchers through a pencil-and-paper survey.
The International Consultation on Incontinence Questionnaire Short Form (ICIQ-SF) was used to measure symptom severity. This questionnaire was established and is highly recommended for assessing the prevalence, severity, and type of urinary incontinence.Citation16 Subjective incontinence rating was also used to measure severity. Stress incontinence is rated on a scale of 0 to 4, with each grade corresponding to a point value. However, this score can reflect the severity of urine leakage under varied stress levels; the higher the score, the more severe the incontinence.
The Incontinence Quality of Life Scale (I-QOL) questionnaire was used to measure the quality of life of SUI patients. It is a 22-item rating scale that covers three domains: behavioral restriction, psychological impact and social disorder. The reliability and validity of the questionnaire and all dimensions are good. The questionnaire score was positively correlated with the patient’s quality of life. The higher the score, the better the quality of life.
Adherence to pelvic floor muscle training was measured with the pelvic floor muscle exercise diary. No standardized measure exists for calculating the pelvic floor muscle exercise adherence rate. The present study defined good adherence as patients exercising following the required time and intensity. The compliance was good if the pelvic floor muscle can be exercised for more than 45 min daily. Adherence rate was calculated as the percentage of days with good adherence to the total number of days in the study. Subjects in the intervention group recorded the number, intensity, duration and reasons for non-compliance. Simultaneously, the diary’s accuracy was ensured by the weekly telephone interviews between the researchers and the subjects.
After the intervention, 0–10 points (from very dissatisfied to very satisfied) were used to collect subjects’ satisfaction.
Statistical Analysis
Statistical analyses were conducted using SPSS software, version 22.0. A p-value of less than 0.05 was deemed statistically significant for all analyses in the study. For data that followed a normal distribution, one-way ANOVA was employed to assess differences among the three groups, with independent samples t-tests utilized for pairwise comparisons between groups and paired-sample t-tests for intragroup comparisons. The choice of these parametric tests was based on their ability to effectively analyze normally distributed data while controlling for Type I error.
In cases where data did not conform to a normal distribution, nonparametric alternatives were applied to ensure appropriate statistical inference. Specifically, the Kruskal–Wallis test was used for intergroup comparisons, as it is a robust method for analyzing ranked data without assuming normality. For intragroup comparisons in non-normally distributed data, the Wilcoxon signed-rank test (also known as the nonparametric statistical rank-sum test) was employed, as it is suitable for paired comparisons and does not require data to follow a specific distribution.
Furthermore, for categorical or count data, the chi-square test was applied to examine associations or differences between groups. This test is widely used in statistical analysis and provides a measure of the degree of association between two categorical variables, allowing for the assessment of statistical significance.
Results
Characteristics of Participants
Initially, 25 subjects were included in the experimental group and 26 in control groups I and II. Four intervention group subjects were lost at the end of the intervention. These four subjects were lost in the 3rd, 6th, 6th, and 9th weeks of intervention due to illness and hospitalization, inability to use the live broadcasting equipment, inability to exercise on time and relocation to her daughter’s residence. Eventually, 73 subjects completed the entire study.
In the study, the subjects’ mean leakage history was 9.12±7.49 years, and their subjective incontinence grade was 1–2, mainly mild to moderate. No statistically significant differences were found between the two groups at baseline. Baseline data are presented in .
Table 2 Comparison of Baseline Data in Three Groups
Four intervention group subjects were lost after the intervention, representing a 16% attrition rate. The baseline data comparison between lost and non-lost subjects in the intervention group revealed no statistically significant difference (P > 0.05).
Comparison of ICIQ-SF
displays the ICIQ-SF scores of the three patient groups. The ICIQ-SF score data followed a normal distribution, and they were compared using a one-way ANOVA (F-statistic). Before the intervention, there was no significant difference between the ICIQ-SF scores of the three patient groups (P > 0.05). After the intervention, a significant difference was observed among the three groups. Intra-group comparisons before and after intervention indicated that the ICIQ-SF scores of the patients in the experimental group and control group II showed a decreasing trend. The decrease in ICIQ-SF scores following intervention in the experimental group (−2.29±2.41) was greater than that in the control group II (−0.39±1.42) (P < 0.05), indicating that the relief of urinary incontinence symptoms was more pronounced in the experimental group.
Subjective Incontinence Rating
As indicated in , there was no significant difference between the subjective incontinence grade ratings of the three patient groups before and after the intervention (P > 0.05). However, the mean subjective incontinence grade scores of the experimental group was lower than that of pre-intervention period (P < 0.05).
Table 3 Comparison of Subjects’ Urinary Incontinence Rating, Subjective Urinary Incontinence Rating and I-QOL
Incontinence Quality of Life Questionnaire (I-QOL)
As shown in , there were no significant difference in the I-QOL scores of the three groups before the intervention in all three dimensions and total quality of life scores (P > 0.05). After the intervention, there were significant differences among the three groups in terms of behavioral restriction, social disorder and total quality of life (P < 0.05). Pairwise comparisons between the groups revealed that each dimension score and total I-QOL score were higher in the experimental group, and there was no significant difference in the total I-QOL score and each dimension score between the control groups.
Compliance with PFMT
The pelvic floor muscle exercise diary revealed that the lowest number of days of good adherence in the experimental group was 78, the highest was 84, and the mean was 81.10±1.61 days. The experimental group’s adherence rate (= number of days with good adherence/total number of days in the intervention program × 100%) was 96.54%.
The compliance data from the control group I showed a minimum of 20 days with good adherence, a maximum of 72 days, and an average of 46.30±14.50 days. The compliance rate was 54.82%. These findings highlight the significant improvement in compliance observed in the experimental group as compared to the control group I.
Subjects’ Satisfaction with the Intervention
The results showed that one of the subjects in the experimental group had the lowest satisfaction score of 7. In contrast, five subjects had the highest score of 10, with an average score of 8.86±0.85, indicating significant patient satisfaction.
Discussion
Square Dancing Incorporating PFMT Was Efficient in Alleviating Urinary Incontinence Symptoms
After 12 weeks of intervention, control group I’s ICIQ-SF scores did not differ from those before the intervention, indicating that the influence of health education alone on improving patients’ symptoms was not evident. After the intervention, the ICIQ-SF scores of the subjects in control group II decreased. It might be related to the fact that although the type of dance and movements of the square dance selected for the exercise in this group differed from the pelvic floor muscle contraction movements in PFMT, the various movements of the square dancing pull the pelvic floor muscles, thus alleviating the symptoms of urinary incontinence.
The experimental group’s ICIQ-SF ratings reduced significantly more than control groups I and II, demonstrating that square dancing with PFMT effectively reduced urine incontinence symptoms. The following factors might contribute to this result: (1) the patients contracted and stretched the pelvic floor muscles actively during exercise and repeatedly strengthened them. (2) In a group exercise, square dancing was more convenient, engaging, and they felt supported, resulting in high compliance and pleasure in the experimental group.
When asked why they did not sought treatment for urinary incontinence, most of the subjects said that they did not realize that urinary leakage was a disease, and they thought that urinary incontinence “naturally occurs when you get older” and “occurs after giving birth to a child”. These patients thought that urinary incontinence “occurs naturally with age”, “will occur after giving birth”, “does not affect life”, and “many friends around me also have such a situation and have not been treated”. This confirms the findings of YangCitation17 and ZhangCitation18 that most women have an insufficient understanding of urinary incontinence. Lack of knowledge combined with cumbersome medical treatment and shyness about urinary incontinence contributed to the low rate of incontinent patients seeking medical treatment. It is easier to treat patients whose urinary leakage symptoms are moderate, and the complexity of therapy increases significantly after the condition has advanced to a severe stage.Citation15 Therefore, urinary incontinence should be treated as early as possible. Despite the subjects’ inadequate understanding of stress urinary incontinence, which increased the difficulty of intervention, the intervention still achieved good results. This indicates that square dancing incorporating PFMT is easily accepted by patients and can be easily promoted.
Square Dancing Incorporating PFMT Improved the Quality of Life of SUI Patients
Data in our study showed that square dancing incorporating PFMT improved patients’ quality of life. As for control group II, subjects’ I-QOL scores slightly increased after intervention, maybe because square dancing enhances the physical fitness of the exerciser. However, the effect of square dancing with PFMT was significantly more effective in improving SUI patients’ quality of life.
Regarding the behavioral restriction dimension, the improvement of the experimental group was significantly higher than that of the control group. This shows that the experimental group’s intervention program can significantly enhance patients’ behavioral restrictions. Many SUI patients limit their behavior for fear of urine leakage, and some limit their outings.Citation19 The positive research results in our study might be related to the fact that the exercise format of the square dancing was conducted as a group activity where group members can help each other and promote healthy behavior development. This is congruent with the findings of YangCitation20, who discovered that group members could solve potential problems through conversation and by learning from the experience of other group members. Thus, they were supported, improving their ability to deal with the problems. Together, square dancing with PFMT can exercise the function of the pelvic floor muscle through effective contraction and diastole, which improves the control of incontinence symptoms and alleviates behavioral restriction in turn.
Urinary incontinence causes mental stress, anxiety and even depression.Citation19 Moreover, patients may feel ashamed due to urine leakage.Citation21 After the intervention, psychological effects improved for all three groups, with no significant differences. The following reasons may be listed: Patients in the control group who received health education about the etiology, pathogenesis, and preventive measures of urinary incontinence could comprehend that the disease was avoidable and treated, hence reducing their psychological stress, the experimental group and the control group II used square dancing, which was conducted in the form of group, and the members established a good relationship, and they supported and encouraged each other. The same experience of the disease made them more capable of generating empathy.Citation22 Thus, their psychological state was improved. The improvement in the psychological impact dimension was more pronounced in the experimental group, as patients’ symptoms improved, promoting their psychological state.
Referring to the dimension of social barriers, the patients in the experimental group had a significantly higher score of social impairment. UI patients frequently avoid social activities due to leakage and body odor concerns. Even if they participate in social interactions, they keep a deliberate distance from others.Citation6 Therefore, urinary incontinence is also known as “social cancer”.Citation23 Stress urinary incontinence directly limits the patient’s social interactions and causes the patient low self-esteem, shame, and reduces their confidence to participate in social activities. The social impairment caused by stress urinary incontinence was alleviated in the present study. The cause may be due to the social atmosphere created by square dancing, where group members congregate in comparable settings and better understand one another. Mutual support and understanding among them improved their social confidence and reduced their social impairment.
PFMT combined with square dancing significantly improved quality of life of SUI patients. However, it is important to acknowledge that the COVID-19 pandemic may have influenced our results in several ways. First, the pandemic has disrupted people’s daily routines and lifestyles, potentially affecting their physical activity levels, dietary habits, and mental health. These changes could have impacted the effectiveness of the interventions. Second, access to healthcare services and support may have been limited during the pandemic, which could have influenced participants’ adherence to the PFMT program or their ability to seek additional treatment for incontinence.
Square Dancing Incorporating PFMT Gained High Compliance and Satisfaction from Experimental Patients
It is widely accepted that adherence rates below 80% will significantly diminish the benefits of exercise.Citation4 In the current study, the average adherence rate of the experimental group was 96.54%, which was a good adherence rate, while the adherence rate of the control group I was 54.82%. According to the Theory of Planned Behavior,Citation24 the patient’s ability to correctly master the exercise mode will promote the development of healthy behaviors Therefore, square dance is easier for patients to accept, and peers and leaders encourage and support it, which may explain high compliance. Together, there is feedback from patients about whether they are exercising correctly. Thus, the patients’ mastery is better, resulting in better healthy behaviors. Furthermore, the patients of experimental group were very satisfied (8.86±0.85 points) with the intervention. Patients reported that this exercise improved their social and psychological status by making good friends and helping them control their symptoms.
Conclusions
In conclusion,square-dancing program incorporating PFMT could enhance adherence to PFMT. Concurrently, the intervention effectively improved the participants’ quality of life and manage symptoms of urinary incontinence. The intervention method of square dancing with PFMT is economical and has strong entertainment value, which is worth promoting.
One limitation of our study is its short duration. Only the results of the 12-week intervention were evaluated; the long-term effects were not studied. To address this limitation, future research should embark on longitudinal studies with an extended follow-up period, ideally spanning several years. These studies should aim to assess not only the persistence of the initial improvements but also any potential changes in the trajectory of the outcomes over time. Moreover, exploring the factors that may influence the longevity of the intervention’s effects, such as patient adherence, lifestyle modifications, and the presence of comorbidities, could provide valuable insights for clinical practice and future intervention development. Furthermore, incorporating qualitative methods, such as in-depth interviews or focus groups, could help elucidate the patients’ experiences and perceptions of the intervention’s long-term impact, which could inform the design of more effective and sustainable interventions.
Another limitation is that we failed to adjust the rhythm to match the patient’s habits, as they often complained the slow rhythm of the square dancing with PFMT, which was not consistent with their original exercise habits. Future iterations of the program could incorporate customizable rhythm settings or offer a range of pace options to cater to diverse preferences.
Thirdly, the form of collective exercise was changed to an online live broadcast in August 2021 due to COVID-19 restrictions on gatherings. Despite our best efforts, some subjects were not skilled in operating the live broadcast equipment, which potentially resulted in participant attrition and decreased compliance. Although researchers can help patients exercise with the help of internet technology and electronic devices,Citation25 we should still pay attention to the applicability. Interventions that are more acceptable and accessible should be considered for older people, persons with low levels of education, and those unfamiliar with smart tools. To address the challenge of technology barriers, future studies should incorporate user-friendly training sessions on operating the live broadcast equipment. Additionally, developing simplified interfaces and accessible platforms tailored for older adults, those with low literacy levels, or limited technological proficiency, could significantly enhance intervention accessibility.
In our study, four participants discontinued the intervention program, which may have introduced biased into our results and limited our ability to draw definitive conclusions. Future research should strive to minimize missing data by implementing robust retention strategies, such as regular follow-ups, incentives for participation, and flexible data collection methods.
Ethics Approval and Informed Consent
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Institutional Review Board of College of Clinical Medicine of The First Affiliated Hospital, and College of Clinical Medicine of Henan University of Science and Technology (No.2023-699). Clinical Trial Registration Number: ChiCTR2100044354. All the study subjects provided informed consent.
Consent for Publication
Not applicable.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have declared that no competing interest exists in this work.
Acknowledgments
Fangfang Du and Yujing Dong are co-first authors for this study. We thank all the women who participated in this study. Furthermore, we would like to thank Home for Researchers (https://www.home-for-researchers.com/) for English language editing.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Abufaraj M, Xu T, Cao C, et al. Prevalence and trends in urinary incontinence among women in the United States, 2005-2018. Am J Obstet Gynecol. 2021;225(2):166.e1–166.e12. doi:10.1016/j.ajog.2021.03.016
- Yu K, Xie ZG. Yu ZH, et al. Prevalence of urinary incontinence in Chinese adult women: a meta-analysis. Chin J Evid-Based Med. 2019;1:36–43.
- Abrams P, Andersson K, Apostolidis A, et al. 6th international consultation on incontinence. recommendations of the international scientific committee: evaluation and treatment of urinary incontinence, pelvic organ prolapse and faecal incontinence. Neurourol Urodynam. 2018;37(7):2271–2272. doi:10.1002/nau.23551
- Venegas M, Carrasco B, Casas-Cordero R, Casas-Cordero R. Factors influencing long-term adherence to pelvic floor exercises in women with urinary incontinence. Neurourol Urodynam. 2018;37(3):1120–1127. doi:10.1002/nau.23432
- Dumoulin C, Hay-Smith J, Frawley H, et al. Consensus statement on improving pelvic floor muscle training adherence: international continence society 2011 state-of-the-science seminar. Neurourol Urodynam. 2014;34:600–605.
- Latorre GFS, de Fraga R, Seleme MR, et al. An ideal e-health system for pelvic floor muscle training adherence: systematic review. Neurourol Urodynam. 2019;38(1):63–80. doi:10.1002/nau.23835
- Mu XY, Ding YP, Liu SY, et al. Influence of extended nursing service based on micro channel platform on quality of life of female patients with urinary incontinence. Chin Nurs Res. 2016;30(005):1878–1879.
- Luo FJ, Huang CM, He HL. Application of quality control circle in improving pelvic floor muscle exercise during perinatal period of pregnant women. Chin Mod Med. 2019;26(14):241–244.
- An S-Y, Kim -S-S, Han G, So-Young A, Seung-Suk K, Gunsoo H. Effect of belly dancing on urinary incontinence-related muscles and vaginal pressure in middle-aged women. J Phys Ther Sci. 2017;29(3):384–386. doi:10.1589/jpts.29.384
- Huang AJ, Chesney M, Lisha N, et al. A group-based yoga program for urinary incontinence in ambulatory women: feasibility, tolerability, and change in incontinence frequency over 3 months in a single-center randomized trial. Am J Obstet Gynecol. 2019;220(1):87.e1–87.e13. doi:10.1016/j.ajog.2018.10.031
- Tang YT, Guo X, Wang Y, et al. Rumba dance combined with breathing training as an exercise intervention in the management of stress urinary incontinence in postmenopausal women: a randomized controlled trial. Int J Environ Res Public Health. 2022;20(1):522. doi:10.3390/ijerph20010522
- Wang LZ. Analysis of the mass cultural boom in the context of square dancing. Chin Natl Exp. 2022;01(01):156–158.
- Mao LT A qualitative study on the behavior characteristics and motivation evolution of participants in square dance. Master thesis. Shanxi University; 2020.
- Eleni Konstantinidou E, Apostolidis A, Kondelidis N, et al. Short-term efficacy of group pelvic floor training under intensive supervision versus unsupervised home training for female stress urinary incontinence: a randomized pilot study. Neurourol Urodynam. 2007;26(4):486–491. doi:10.1002/nau.20380
- Gynecologic Pelvic Floor Group of the Obstetrics and Gynecology Section of the Chinese Medical Association. Guidelines for the diagnosis and treatment of female stress urinary incontinence (2017). Chin J Obstet Gynecol. 2017;52(5):289–293.
- Abrams P, Avery K, Gardener N, Donovan J. The international consultation on incontinence modular questionnaire: https://www.iciq.net. J Urol. 2006;175(3):1063–1066. doi:10.1016/S0022-5347(05)00348-4
- Yang Y, Xiao YY, Zhang T, et al. Survey of disease cognition and quality of life in female stress urinary incontinence patients. Chin Gen Pract Nurs. 2018;016(011):1281–1284.
- Zhang MN, Xiao Q, Wu Y, et al. Knowledge-attitude-practice of pelvic floor muscle function training and the current situation of its needs in puerperium women. Chin J Mod Nurs. 2017;23(30):3862–3869.
- Wang HH, Shen HJ, Yu L, et al. A qualitative study of the psychological experience of female patients with stress urinary incontinence. Nurs Rehab J. 2021;20(9):38–41.
- Yang ZY The effect of the combination of individual instruction and group therapy for female stress urinary incontinence. Master thesis. Chinese Academy of Medical Sciences & Peking Union Medical College; 2013.
- Liu M, Zhang HJ. Study on correlation among social anxiety, stigma and resilience in elderly female patients with urinary incontinence. Chin Gen Pract Nurs. 2021;15:2022–2026.
- He XP. The effect of group visits and with peer education on adherence to postpartum pelvic rehabilitation in pregnant women. Clin Edu Gen Pract. 2019;11:1045–1046+1049.
- Sazonova NA, Kiseleva MG, Gadzhieva ZK, et al. Urinary incontinence in women and its impact on quality of life. Urologiia. 2022;2:136–139. doi:10.18565/urology.2022.2.136-139
- Fishbein M, Ajzen I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory And research. RAddison-Wesley Publishing Company; 1975:53.
- Wang X, Xu X, Luo J, et al. Effect of app-based audio guidance pelvic floor muscle training on treatment of stress urinary incontinence in primiparas: a randomized controlled trial. Int J Nurs Stud. 2020;104:103527. doi:10.1016/j.ijnurstu.2020.103527