
Abstract
Background
Stroke is one of the leading medical conditions in the Philippines. Over 500,000 Filipinos suffer from stroke annually. Provision of evidence-based medical and rehabilitation management for stroke patients has been a challenge due to existing environmental, social, and local health system issues. Thus, existing western guidelines on stroke rehabilitation were contextualized to draft recommendations relevant to the local Philippine setting. Prior to fully implementing the guidelines, an audit of current practice needs to be undertaken, thus the purpose of this audit protocol.
Methods
A clinical audit of current practices in stroke rehabilitation in the Philippines will be undertaken. A consensus list of data items to be captured was identified by the audit team during a 2-day meeting in 2012. These items, including patient demographics, type of stroke, time to referral for rehabilitation management, length of hospital stay, and other relevant descriptors of stroke management were included as part of the audit. Hospitals in the Philippines will be recruited to take part in the audit activity. Recruitment will be via the registry of the Philippine Academy of Rehabilitation Medicine, where 90% of physiatrists (medical doctors specialized in rehabilitation medicine) are active members and are affiliated with various hospitals in the Philippines. Data collectors will be identified and trained in the audit process. A pilot audit will be conducted to test the feasibility of the audit protocol, and refinements to the protocol will be undertaken as necessary. The comprehensive audit process will take place for a period of 3 months. Data will be encoded using MS Excel®. Data will be reported as means and percentages as appropriate. Subgroup analysis will be undertaken to look into differences and variability of stroke patient descriptors and rehabilitation activities.
Conclusion
This audit study is an ambitious project, but given the “need” to conduct the audit to identify “gaps” in current practice, and the value it can bring to serve as a platform for implementation of evidence-based stroke management in the Philippines to achieve best patient and health outcomes, the audit team is more than ready to take up the challenge.
Introduction
Stroke is one of the leading medical conditions in the Philippines. Over 500,000 Filipinos suffer from stroke annually. The reasons for this are thought to include genetics, diet, and/or lifestyle, coupled with lack of community awareness of and/or access to preventative health care (eg, blood pressure management).Citation1 Treating acute stroke (medical management and ongoing rehabilitation) incurs significant and ongoing costs to the health care system.Citation2 Moreover, suffering an acute stroke produces significant and often irreversible changes in the individual, in terms of resumption of usual function, self-esteem, and mental health, and full participation in family and community life.Citation3,Citation4 Despite this, equitable access to and provision of evidence-based rehabilitation for stroke sufferers in the Philippines is a challenge, for a range of environmental, social, personal, organizational, educational, and systems reasons.Citation5–Citation7 Not all Filipinos have access to specialist medical personnel for geographic and workforce availability reasons.Citation8 Thus, while decreasing stroke incidence should be a long-term aim, treating stroke consistently in the most evidence-based manner to produce the best health outcomes would have significant immediate advantages for the Philippines economy.Citation5,Citation8
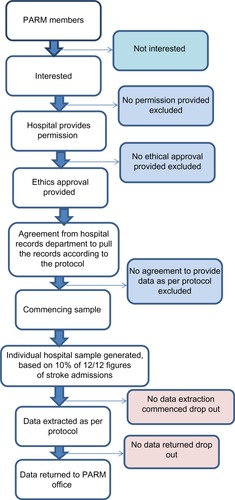
Figure 1 Flow chart of hospital recruitment process.
We recently published the first stage of the Filipino stroke guideline project, which was the contextualization of Western clinical guidelines for stroke, and targeted to conditions in the Philippines.Citation9 Prior to this work, there was no nationally agreed guideline to guide Filipino best practice for stroke rehabilitation. However, before this guideline can be implemented, current practice needs to be established. There has never been a national survey of stroke rehabilitation practices in the Philippines, and therefore nothing concrete is known about current stroke rehabilitation practices, or the incidence of adverse events from stroke, such as swallowing difficulties or pressure ulcers. Without this information, any campaign to increase evidence-based practices may fail to target areas of most need.
The value of a comprehensive multicenter stroke audit to chart current practice has been reported by Luker et al.Citation10,Citation11 Their work demonstrated that application of an audit tool that sought basic information on patient demographics, stroke descriptors, and rehabilitation care could identify gaps in recording of important information on current practice, as well as identify areas where records could be improved and used for future quality improvement activities. This audit protocol builds on the work of Luker et al.Citation10,Citation11
Championing the project
Improving the quality of stroke rehabilitation in the Philippines and implementing evidence-based practice in the area has been championed by the Philippines Academy of Rehabilitation Medicine (PARM) for the last 2 years. Evidence-based practice is relatively new to the Philippines,Citation6,Citation9 and thus developing and implementing clinical guidelines has been a vehicle for encouraging the body of Filipino physiatrists to reflect on their practices, and improve them if indicated.
Rehabilitation occurs after the initial medical management of acute stroke, which is undertaken by neurologists, internists, emergency room physicians, and family medicine physicians. Appropriate referral of medically stable patients to physiatrists is an important element in ensuring equity of access to best practice rehabilitation care. Thus, other medical personnel are stakeholders in quality improvement programs for stroke rehabilitation.
An audit to establish current rehabilitation practices for stroke patients in the Philippines would also have the potential to capture “gaps” in current practice patient records, as was found by Luker et al.Citation11 These gaps could be addressed as part of the education provided to Filipino health care practitioners as part of the guidelines implementation program. For instance, capture of information on stroke severity (National Institutes of Health Stroke Scale) is recommended as part of best practice stroke management.Citation3,Citation10,Citation11 However, its frequency of use in Filipino settings is unknown. As stroke severity is a strongly evidence-based indicator of stroke rehabilitation outcomes,Citation12 standard collection of this information should be encouraged, as part of describing a comprehensive Filipino stroke rehabilitation profile.
The objective of this study was to establish current prac-tice in stroke rehabilitation in the Philippines. Once current practice is established, the clinical practice stroke guidelines that have been contextualized to Filipino conditions can be implemented.Citation9,Citation13
Operational definition of terms
Clinical audit: a quality improvement process that seeks to improve patient care and outcomes through systematic review of care against explicit criteria and implementation of change.
Quality improvement: combined and unceasing efforts of health care professionals, patients and their families, researchers, payers, planners and educators, to make the changes that will lead to better patient outcomes (health), better system performance (care), and better professional development (learning).
Implementation: process of translating research findings into clinical practice.
Clinical practice guidelines: systematically developed statements designed to help practitioners and patients decide on appropriate health care for specific conditions and/or circumstances.
Behavior change interventions: coordinated sets of activities designed to change specified behavior patterns. In general, these behavior patterns are measured in terms of the prevalence or incidence of particular behaviors in specified populations. Interventions are used to promote uptake and optimal use of effective clinical services and to promote healthy lifestyles.
Practice protocol: suggested course of management for a specific diagnosis or a condition. Practice protocols are generally preagreed approaches and as such make rigid statements allowing for little or no variation in the process of care.
Materials and methods
Ethics
Ethical approval was obtained from the ethics review board of the participating hospitals (University of Santo Tomas Hospital, Philippine Orthopedic Center, Our Lady of Lourdes Hospital, Amang Rodriguez Hospital, Veterans Memorial Medical Center). Ethical approval is currently being obtained from other hospitals in other areas of the Philippines. A standard ethics application was written by the authors of this paper and circulated to all hospitals that indicated interest in participating. It is proposed to use the protocol required at the University of Santo Tomas Hospital, Manila, Philippines, this being the institution of the principal author. No changes were made at any participating site with regard to the methodology outlined in the standard ethics protocol, although site-by-site clarifications may be required depending on local processes regarding accessing patient records. Permission will also be sought from the medical director of the participating hospital. If required by the hospital, a consent form will be signed by the attending physician so that charts can be reviewed (see Supplementary materials [Figure S1]).
Type of study
This is to be a clinical audit study using medical records review. The study will be done in hospitals with a rehabilitation unit.
Working group
The research proposal was formulated by a volunteer multidisciplinary working group formed from eleven PARM members and affiliate members, reflecting key health care personnel engaged in stroke rehabilitation in the Philippines (seven physiatrists [rehabilitation doctors], three physical therapists, and two occupational therapists). An external international facilitator (KG) participated, providing educational input and an independent evaluation and critique of the working group’s activities.
Data items
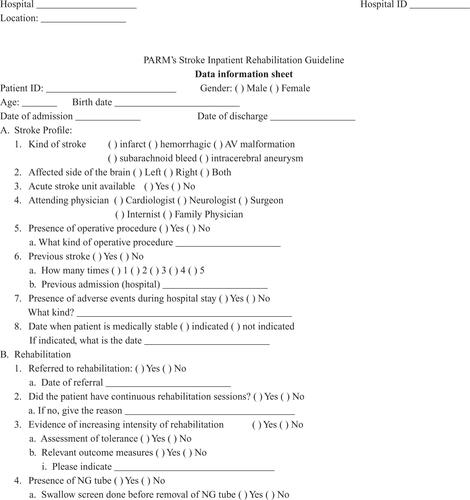
As part of the group’s deliberations, a consensus list of data items believed to provide a comprehensive profile of stroke sufferers who are referred for rehabilitation was developed.Citation13 Items in this list could also be used for later reaudit purposes after the Filipino stroke guidelines are implemented. The list of data items relating to current practices is presented in our previously published paperCitation13 and in . The data information sheet is in Supplementary materials (Figure S2).
Table 1 Current practice audit items
Sample size
It was estimated using GPower that if each invited hospital participated, and 10% of each invited hospital’s annual stroke admissions was audited, this would provide a sample of at least 40,000 patients, which would have (estimated) 90% power to describe typical Filipino stroke presentations, per hospital and nationally, as well as providing a robust description of the variability in rehabilitation practices and adverse events.
Process of registering for the audit
The contact PARM members from interested hospitals that have provided ethics approval should contact the PARM office, and provide the following information:
Name of institution
Location (metropolitan, regional, remote)
Number of beds
Number of stroke patients presenting in the last 12 months
Number of physiatrists, physical therapists, and occupational therapists working in the institution.
This information would be kept in a confidential file, which would only be accessed by the independent PARM research administrator whilst the data were being collected and analyzed. This information would be destroyed once the project was completed. Each participating hospital would be given a unique code regarding its identity. This code would link to a master file that recorded its location, total number of beds, number of stroke patients presenting in the last 12 months, and number of rehabilitation staff. The PARM office would give the hospital the sample size for its audit.
Data collection processes
Validity of the data collection tool
The data collection form was presented in a forum to rehabilitation doctors, physical therapists, and occupational therapists for face and content validation. This was undertaken to ensure that the data audit items to be retrieved from the medical records will answer the clinical audit objectives. Revisions were undertaken based on the validation procedure and sent back to the group for approval. Thus the data collection form/audit form to be used in the proposed audit has already been validated for its purpose.
Data collectors
Two to three data collectors identified from each participating hospital will be required to retrieve the audit items from the medical records. They should have experience in data recording or management to ensure their capacity to reliably extract the information needed. An orientation to the clinical audit project and training for data collection will be conducted among the data collectors. A reliability procedure will also be undertaken by asking the data collectors to complete data extraction of five sample cases independently. The interrater reliability for percentage of agreement recommended by Dixon and PearceCitation14 will be used to compute the reliability of the data collectors. This is done by dividing the number of bits of data for which there was complete agreement among the data collectors and the total number of bits of data (for example, 25 bits of data per case × five cases). Further training will be provided as needed based on the results of the reliability testing procedure.
Data handling and management
A purpose-built MS Excel® file will be constructed, which restricts the type of data that can be entered into each column. This will reduce data entry errors and ensure efficiency of data amalgamation per site. Completed data files will be sent to the PARM office, which will check the integrity of the file and ensure that only the unique coding of the hospital is provided, and that all patient data are deidentified.
Data analysis
Analysis of the data will be undertaken by an independent analyst. The data will be reported per hospital and overall using means and percentages as appropriate, with relevant measures of variability. Subgroup analysis will be undertaken using the overall sample data to look at differences in stroke patient descriptors and rehabilitation activities, per general hospital location (eg, metropolitan, rural), and also to report on differences that relate to size (eg, number of beds, number of stroke admissions). The extent of missing data will also be reported for stroke and rehabilitation descriptors. This will inform future education programs that can target reasons for missing information and identify needs for further education (for instance on the use of the National Institutes of Health Stroke Scale). This approach is necessary to improve compliance prior to guideline implementation. summarizes the operational definition of process indicators and auditing requirements that will be used to determine whether or not the process indicators have been met.
Table 2 Auditing guideline: definitions of process indicators and auditing requirements
Publication of audit data
The overall audit data will be reported in peer-reviewed journals. Individual sets of hospital data will be returned to the hospital for use in quality improvement. Lessons learnt from the audit regarding stroke descriptors, rehabilitation practices, and common sources of missing data will be presented to PARM, the Philippines Hospital Association, and Phil Health. This is important because this information will provide the first known robust data collection on characteristics of Filipino stroke patients, rehabilitation practices, and the need for further education. Subsequent guideline roll out should be underpinned by appropriate training in recording accurate patient data.
Discussion
This protocol outlines the way that the first comprehensive profile of Filipino stroke rehabilitation practices will be collated. This information is essential not only to describe the previously unknown variability of Filipino stroke patient descriptors, but also to highlight areas of practice that could be improved by the implementation of evidence into clinical decision-making and practices.Citation13
It is an ambitious project because it will be largely undertaken using goodwill, from the champions of change and PARM members. However, the PARM group has recognized the need to improve stroke rehabilitation practices nationwide, to reduce unnecessary costs, decrease variability in treatment decisions, and improve health outcomes. This audit is therefore an essential next step for PARM in implementing evidence-based practice in the Philippines regarding stroke rehabilitation.
Audits in the Western world have identified opportunities for improved care by acting on “current practice” information.Citation15,Citation16 Quality improvement activities have gained in popularity in conjunction with evidence-based practice initiatives, as audits of current practice provide a wealth of information on what could be improved.Citation15,Citation16 Luker et al highlighted a range of derived information on quality of stroke care that could be obtained from a simple audit of quality care indicators from 300 consecutive patients in three Australian hospitals.Citation10,Citation11
The proposed audit could be of value on many levels. On a basic level, it will provide PARM with a comprehensive association initiative to collect data on what its members do and what the health and process outcomes are. It will also identify data items that are variably collected, eg, information on stroke severity, and will provide opportunities to consider how rehabilitation practices fit within the overall continuum of stroke care provided in institutions around the Philippines (eg, the number of stroke patients who are referred for rehabilitation). On a more advanced level, it will provide information regarding the importance of data items to describe stroke care, and will provide a platform for comparison of care, once the Filipino- contextualized guidelines are implemented in 2014. This audit will also highlight the need for training regarding evidence-based practice, which is the core component of guideline recommendation and implementation.Citation15,Citation16 Evidence-based practice is known to result in effective patient outcomes and an efficient health care system.Citation15,Citation16 In a resource-limited country such as the Philippines, a greater need for treatment and management known to result in effective outcomes (such as in the case of stroke rehabilitation) is emphasized to ensure that no money or resource is put to waste.
Acknowledgments
This project is funded by the Philippine Academy of Rehabilitation Medicine.
Supplementary material
Figure S1 Consent form for attending physician.
Abbreviation: NG, nasogastric.
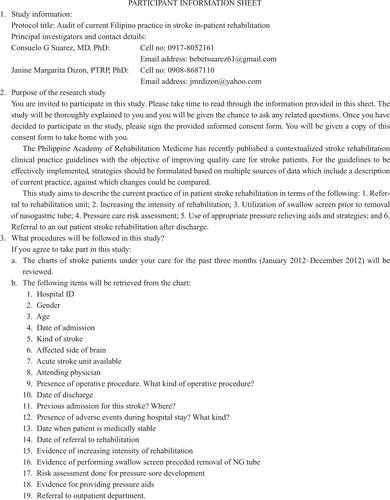
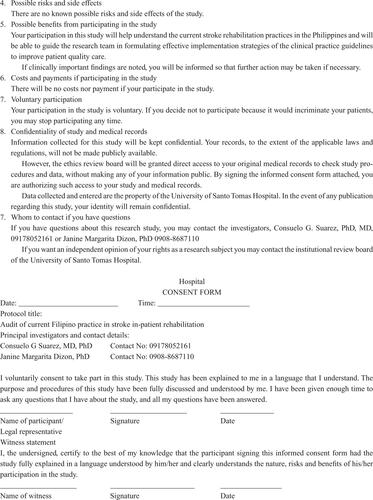

Figure S2 Data information sheet.
Abbreviations: AV, arteriovenous; NG, nasogastric; NIHSS, National Institutes of Health Stroke Scale; PARM, Philippines Academy of Rehabilitation Medicine.
Disclosure
The authors report no conflicts of interest in this work.
References
- Country Health Information Profiles, World Health Organization, Western Pacific Region, Philippines2011 Available from: http://www.wpro.who.int/countries/phl/26PHLpro2011_finaldraft.pdfAccessed August 10, 2014
- World Health OrganizationNeurological disorders: public health challenges2006 Available from: http://www.who.int/mental_health/neurology/neurological_disorders_report_web.pdfAccessed March 10, 2013
- MiddletonSMcElduffPWardJImplementation of evidence-based treatment protocols to manage fever, hyperglycaemia, and swallowing dysfunction in acute stroke (qasc): a cluster randomised controlled trialLancet20113781699170621996470
- HamiltonSMcLarenSMulhallAAssessing organisational readiness for change: use of diagnostic analysis prior to the implementation of a multidisciplinary assessment for acute stroke careImplement Sci200722117629929
- AndersonBAlcantaraMOTechnical assistance to the Republic of Philip pines for the health sector development program ADB TA 4647-PHI: final report2007 Available from: http://www2.adb.org/Documents/Reports/Consultant/39066-PHI/39066-PHI-TACR.pdfAccessed March 15, 2012
- DizonJMGrimmer-SomersKAKumarSA pilot study of the evidence-based practice training program for Filipino physiotherapists: emerging evidence on outcomes, feasibility and acceptabilityInternet Journal of Allied Health Sciences and Practice2012102
- DizonJMGrimmer-SomersKKumarKEffectiveness of the tailored EBP training program for Filipino physiotherapists: a randomized controlled trialBMC Med Educ20111114
- World Health OrganizationCountries: Philippines2012 Available from: http://www.who.int/countries/Phl/en/Accessed March 15, 2012
- Gonzalez-SuarezCGrimmer-SomersKKingEContextualising Western guidelines for stroke and low back pain to a developing country (Philippines): an innovative approach to putting evidence into practice efficientlyJ Healthc Leadersh20124141156
- LukerJBernhardtJGrimmer-SomersKAge and gender as predictors of allied health quality stroke careJ Multidiscip Healthc2011423924521847346
- LukerJBernhardtJGrimmer-SomersKDemographic and stroke-related factors as predictors of the quality of acute stroke care provided by allied health professionalsJ Multidiscip Healthc2011424725921847347
- DuncanPWZorowitzRBatesBManagement of adult stroke rehabilitation care: a clinical practice guidelineStroke200536e100e14316120836
- Gonzalez-SuarezCDizonJGrimmerKImplementation of recommendations from the PARM stroke in-patient rehabilitation guideline: a plan of actionClinical Audit201357789
- DixonNPearceMClinical Audit ManualRomsey, UKHealthcare Quality Quest Ltd2010
- GrolRImplementing guidelines and innovations in general practice: which interventions are effective?Br J Gen Pract1998489919979624774
- GrolRGrimshawJFrom best evidence to best practice: effective implementation of change in patients’ careLancet20033621225123014568747
- National Stroke FoundationAcute stroke services framework, 2008: a framework to enable the delivery and monitoring of optimal acute stroke care across AustraliaMelbourneNational Stroke Foundation2008 Available from: http://strokefoundation.com.auAccessed November 26, 2011