
Abstract
Background
Dexamethasone is a common adjuvant for local anesthetics in regional anesthesia, but the optimal route of administration is controversial. Therefore, we did a systematic review and meta-analysis of randomized controlled trials to assess the effect of perineural versus intravenous dexamethasone on local anesthetic regional nerve-blockade outcomes.
Materials and methods
Medline (through PubMed), Embase, Cochrane, Web of Science, and Biosis Previews databases were systematically searched (published from inception of each database to January 1, 2017) to identify randomized controlled trials. The data of the selected trials were statistically analyzed to find any significant differences between the two modalities. The primary outcome was the duration of analgesia. Secondary outcomes included duration of motor block, postoperative nausea and vomiting, and postoperative analgesic dose at 24 hours. We conducted a planned subgroup analysis to compare the effects between adding epinephrine or not.
Results
Ten randomized controlled trials met the inclusion criteria of our analysis, with a total of 749 patients. Without the addition of epinephrine, the effects of perineural and intravenous dexamethasone were equivalent concerning the duration of analgesia (mean difference 0.03 hours, 95% CI –0.17 to 0.24). However, with the addition of epinephrine, the analgesic duration of perineural dexamethasone versus intravenous dexamethasone was prolonged (mean difference 3.96 hours, 95% CI 2.66–5.27). Likewise, the impact of epinephrine was the same on the duration of motor block. The two routes of administration did not show any significant differences in the incidence of postoperative nausea and vomiting, nor on postoperative analgesic consumption at 24 hours.
Conclusion
Our results show that perineural dexamethasone can prolong the effects of analgesic duration when compared to the intravenous route, only when epinephrine is coadministered. Without epinephrine, the two modalities show equivalent effect as adjuvants on regional anesthesia.
Introduction
Uncontrolled pain after surgery may produce a range of detrimental acute and chronic effects.Citation1 In some surgical procedures under regional anesthesia, commonly used local anesthetics cannot provide analgesia for a sufficiently prolonged time. Therefore, local anesthetic–opioid combinations or continuous catheterization are chosen to prolong analgesic duration. However, unintentional opioid-associated side effects and several problems associated with carrying a catheter, especially for day-care patients, make these treatment options unsatisfactory. Since 1982, anesthesiologists have been using a variety of adjuvants added to local anesthetics to enhance regional anesthesia.Citation2
Dexamethasone is one of these additives.Citation3 Dexamethasone has been proved to be an effective adjuvant for extending the duration of sensory and motor block for peripheral nerve block when given perineurally.Citation4–Citation6 Intravenous injection can also be used for alleviating postoperative pain.Citation7 However, there are conflicting reports about which of the two routes of administration is the best or if both exert an equivalent effect.Citation8–Citation12
To solve this query, a series of randomized controlled trials (RCTs) were conducted to compare the effect of prolongation of analgesia between perineural and intravenously administered dexamethasone. We carried out a systematic review and meta-analysis to assemble all the associated individual clinical trials to assess the two modalities on the main outcomes: prolonging sensory-block duration, decreasing postoperative nausea and vomiting, and sparing analgesic consumption at 24 hours after surgery.
Materials and methods
This systematic review and the meta-analysis results were reported following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Search strategy
Two authors (WLZ and XFO) independently searched the following databases: Medline (through PubMed), Embase, Cochrane Central Register of Controlled Trials, Web of Science, and Biosis Previews, from inception of each database to January 1, 2017. There were no language restrictions. The full literature-search strategies for PubMed and Embase are presented in . In brief, we used MeSH terminology for dexamethasone, regional anesthesia, and their synonyms to search the five databases to obtain relevant literature. Then, all the titles and abstracts were screened and full texts of eligible RCTs retrieved. The references of key English reviews and eligible studies were also manually searched.
Selection criteria
When the titles and abstracts were screened, four selection criteria were applied: 1) population – adult patients (aged ≤19 years) under surgery who received regional anesthesia; 2) intervention – dexamethasone given perineurally as an adjuvant to local anesthetics; 3) control – same-dose dexamethasone given intravenously; and 4) design – RCTs. Studies that satisfied these criteria were retrieved for full texts to be assessed. Meeting abstracts were eliminated due to their incomplete information.
Data extraction
Two authors (WLZ and XFO) independently extracted the following raw data from the selected studies: main authors, year of publication, country, number of patients, type of nerve block, ultraguided localization technique, type and dose of local anesthetics (including dexamethasone and other adjuvants), and main outcomes. Then, concrete data of the following outcomes were extracted: duration of analgesia or sensory block, duration of motor block, incidence of postoperative nausea and vomiting, and postoperative analgesic use (morphine equivalents) at 24 hours. For the continuous type of data, we emailed the corresponding author to obtain the raw data when the variables in full text were not reported as means and SD. If authors did not respond, we used a method of data conversion. For calculation of given means, 95% CIs, SD ((√n × [upper – lower]/2t), given medians, and interquartile ranges, the method reported by Hozo et al was used.Citation13 Each of the two aforementioned authors checked these data at least three times. Any disagreements on the results were resolved independently by a third experienced author (JL).
Assessment for risk of bias in included studies
Risks of included studies were assessed by the Cochrane risk-of-bias tool. We classified risk of bias as low, unclear, or high for each of random-sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias (such as missing participant data). To grade the qualities of evidence and the strength of recommendations, we used GradePro version 3.6.1 for our four outcomes.
Statistical analysis
Continuous variables, analgesic duration, duration of motor block, and postoperative analgesic use at 24 hours were reported as mean differences (MDs) with 95% CIs. We analyzed postoperative nausea and vomiting as the categorical variable and expressed relative risk with 95% CIs. Heterogeneity of the four outcomes was evaluated by using the χ2 and I2 tests. A fixed-effect model was used when χ2 P-value was >0.1 and I2<50%. When P<0.1 and I2>50%, we chose a random-effect model, and the planned subgroup analysis was performed to compare adding epinephrine or not to the local anesthetic mixture. Potential publication biases were assessed by funnel-plot analysis. All analyses were performed with RevMan (version 5.3; Cochrane Library, Oxford, UK).
Results
Study selection and characteristics
A flowchart of the study-selection procedure is shown in . In order to avoid any missing studies, we did not restrict the design of RCTs in searching Web of Science and Biosis Previews or define the route of administration. A total of 2,939 studies were identified during our first search: 638 articles were removed due to duplication, and 2,301 titles and abstracts were eliminated after screening. Finally, ten studies were included in our ultimateanalysis.Citation14–Citation23 One study was eliminated due to its high standard deviation, which was even larger than the mean value, possibly due to the small-study effect.Citation24,Citation25 The basic information of the ten studies is presented in . Patients of seven studies received brachial nerve block, one study used a nerve simulator to localize the nerve, and the rest were ultrasound-guided. The remaining studies were on perianal block, sciatic nerve block, and ankle block. Two of the studies were multicenter clinical trials, which were conducted in Canada and Thailand. The dose of dexamethasone ranged from 4 to 10 mg. Three trials added epinephrine with local anesthetics and dexamethasone, and hence they constituted the planned subgroup analysis in this study.
Figure 1 Flowchart of the search strategy.
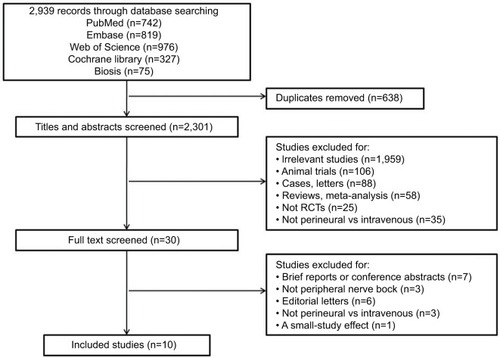
Table 1 Characteristics of included studies
The risks of bias for the ten studies included here were discussed by all the authors; the risks discussed are summarized in . One studyCitation16 did not present the process they used to generate random sequences for group allocation. They also unveiled the allocation results to the anesthesiologists who participated in that trial, and did not refer to any blinding of the outcome assessment, as with another one.Citation14 For one of the ten studies,Citation22 the methods section did not clearly show the approach used for blinding the participants.
Duration of analgesia
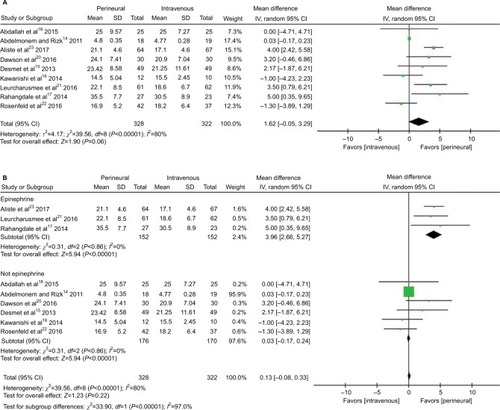
The duration of sensory block or analgesia was reported by nine trials. OneCitation19 was eliminated due to its definition of median analgesia time, namely time to first analgesic request in >50% of patients, which was far different to other studies’ definitions (). In a random-effect model, a pooled analysis of nine trials showed that the MD between perineural and intravenous dexamethasone was 1.62 hours (95% CI –0.05 to 3.29, I2=80%; P=0.06; ), which indicated that dexamethasone given perineurally or intravenously had a similar effect on the duration of sensory block or analgesia. Due to the high heterogeneity, we conducted a subgroup analysis comparing the addition or exclusion of epinephrine. When epinephrine was used, perineural dexamethasone prolonged analgesic duration by 3.96 hours (95% CI 2.66–5.27, P<0.00001) in comparison to the intravenous dexamethasone group, with no heterogeneity (I2=0). In the absence of epinephrine, both groups had equal analgesic duration (MD 0.03 hours, I2=7%, 95% CI –0.17 to 0.24; P=0.75; ). There were no observations of publication biases when constructing the funnel plots ().
Figure 2 Forest plots showing the duration of analgesia.
Duration of motor block
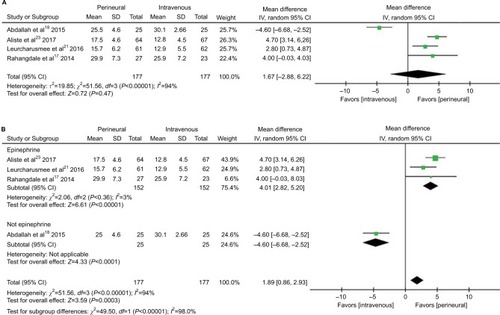
Four trials reported on duration of motor block. The effects on prolonging duration of motor block between the two modalities was statistically insignificant (MD 1.67 hours, I2=94%, 95% CI –2.88 to 6.22; P=0.47; ) as revealed by the random-effect model. However, subgroup analysis showed that in the presence of epinephrine, the perineural dexamethasone group had duration prolonged by 4 hours (95% CI 2.82–5.20, I2=3%; P<0.00001; ) when compared to the intravenous dexamethasone group.
Figure 3 Forest plots showing the duration of motor block.
Postoperative nausea and vomiting
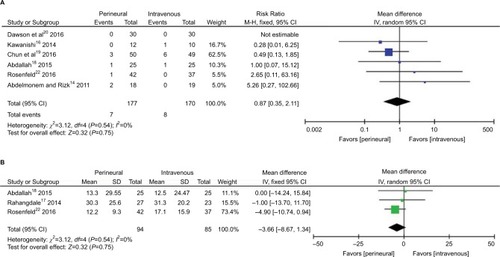
Six studies assessed the incidence of postoperative nausea and vomiting. The pooled analysis demonstrated that there was no difference between the perineural and intravenous dexamethasone groups (risk ratio 0.87, 95% CI 0.35–2.11; P=0.75; ), without heterogeneity (I2=0) or publication bias ().
Figure 4 Forest plots comparing perineural and intravenous groups at 24 hours.
Postoperative analgesic use at 24 hours
Postoperative opioid consumption (morphine equivalents) at 24 hours was evaluated by three trials. In this analysis, analgesic use was the same between the two groups (MD –3.66 mg, I2=0, 95% CI –8.67 to 1.34; P=0.15; ).
Grade quality
GradePro evaluation of the confidence of evidence is shown in .
Table 2 Summary of findings
Discussion
The results of our review and meta-analysis show that the two modalities of perineural and intravenous dexamethasone as local anesthetic additives can produce a similar effect on the duration of analgesia or sensory block. From the subgroup analysis, we found that the high heterogeneity in the data analysis stemmed from adding epinephrine or not, a well-known adjuvant in local anesthetics to prolong block duration.Citation26,Citation27 With epinephrine, prolongation of duration of analgesia and motor block were observed in the perineural dexamethasone group when compared to the intravenous dexamethasone method. Without epinephrine, both groups showed an equivalent effect on analgesia duration. In addition, the incidence of postoperative nausea and vomiting and postoperative analgesic consumption at 24 hours exhibited no statistical significant differences when comparing the two routes of administration.
Such adjuvants as midazolam,Citation28 ketamine,Citation29 clonidine,Citation30 dexmedetomidine,Citation31 epinephrine, or dexamethasone are coadministered with local anesthetics in order to enhance the effect of single-shot peripheral nerve block. Although several meta-analysesCitation4–Citation6 have demonstrated that dexamethasone given perineurally can extend the analgesic duration of common local anesthetics for brachial plexus block, the effectiveness of intravenous dexamethasone has been controversial.Citation12 Actually, in a meta-analysis of 38 studies, systemic dexamethasone (>0.1 mg·kg–1) reduced postoperative pain and analgesic consumption.Citation7 As such, the current paramount issue is to demonstrate that perineural dexamethasone has an extra effect on the duration of analgesia through a direct mechanism on nerve blocking.Citation32 In this meta-analysis, the pooled results from ten RCTs revealed that dexamethasone (4–10 mg) can produce similar duration of sensory or motor block when administered perineurally or intravenously without epinephrine. In other words, the viewpoint that dexamethasone has a direct inhibition of peripheral nerves needs to be considered carefully and examined again. However, limited evidence in our review and meta-analysis elucidates that there may be a synergistic effect between dexamethasone and epinephrine when given locally.
On the one hand, whether or not dexamethasone has a direct effect on nerve conduction has been disputed. In isolated rat sciatic nerves, neither dexamethasone nor buprenorphine can inhibit the compound action potentials from A and C fibers.Citation33 In vivo, an animal study demonstrated that bupivacaine plus 67 μg dexamethasone did not increase block duration more than bupivacaine alone.Citation34 In contrast, in a mouse sciatic nerve-blockade model, high-dose (0.5 mg·kg–1) perineural dexamethasone added to bupivacaine prolonged the duration of sensory and motor block, while low-dose (0.14 mg·kg–1) dexamethasone did not. However, these results should be considered with skepticism, because of the unblinded procedure in that study.Citation35 Despite the fact that sciatic nerves are commonly used to evaluate the effect of local anesthetic, we cannot directly extrapolate the results from rodents to humans. In addition, the period of block conduction can differ due to the neurobiology of acute postoperative pain in clinical patients. Acute postoperative pain includes not the conduction of nociception, but direct nerve damage and inflammatory mediator release, which activate peripheral nociceptors to deliver information to the central nervous system.Citation1 Dexamethasone, a long-effective glucocorticoid, has the appropriate anti-inflammatory property by increasing the production of anti-inflammatory substances and decreasing the release of inflammatory mediators.Citation36 This characteristic may be responsible for its systematic mechanism in prolonging block duration. Overall, further studies are needed to find and prove the precise indirect mechanism of dexamethasone and also its interaction with epinephrine perineurally.
On the other hand, dexamethasone is prescribed “off-label” for perineural administration. Neurotoxicity is a serious problem for local anesthetics and additives that we have to consider. Dexamethasone 133 μg·mL–1 combined with ropivacaine increased neurotoxicity for isolated sensory neurons. As such, the author advised that much attention be paid to the time- and concentration-dependent toxicity when dexamethasone is combined with ropivacaine.Citation37 In agreement with previous results,Citation38,Citation39 in a preliminary animal experiment, we found that solutions of commonly used local anesthetics (bupivacaine, ropivacaine) in combination with nonparticulate dexamethasone sodium phosphate could crystallize, even in physiological pH (unpublished data). Therefore, the patient’s safety might be compromised when crystalliferous solution is unintentionally injected into the subarachnoid space or into the blood vessels.
Considering potential neurotoxicity or hazards from crystallization, the unknown mechanism of action, and the fact that both methods have a similar effect on block duration, controlling nausea and vomiting, and sparing opioid consumption, we conclude that intravenous dexamethasone is preferable to perineural dexamethasone, as it carries fewer risks to the patient. Moreover, a recent published meta-analysisCitation40 proved that a combination of intravenous dexamethasone with other antiemetics showed more efficacy than a single antiemetic in preventing nausea and vomiting after laparoscopic cholecystectomy.
There are some limitations of this analysis. Firstly, post-operative blood glucose levels and long-term neurological sequelae were not analyzed. Only two of the ten trialsCitation15,Citation19 chosen here reported blood glucose concentrations after surgery. In these two studies, data demonstrated that there were no significant differences in blood glucose levels between the two routes of administration. Also, no serious relevant neurologic symptoms were found in these clinical trials. Secondly, although heterogeneity was low or inexistent among the four outcomes, there was a risk of bias in some of the studies. Thirdly, this review did not evaluate the interaction between the dosage of dexamethasone and block duration. However, Albrecht et alCitation41 elucidated that no inconclusive evidence was found between different concentrations of dexamethasone (4–10 mg) and analgesic duration by subgroup analysis.
Knowledge on many aspects of the two modalities is not clear, and further clinical studies are required to explore and determine their mechanism of action. A large-scale, multicenter, prospective, double-blinded RCT is needed to be performed to prove which is the most effective adjuvant, the best method of delivery (local anesthetic, perineural, or intravenous dexamethasone), and whether dexamethasone has a synergistic or additive effect with epinephrine when administered locally. If the most efficient route of administration proves to be additive, then the optimal dose of dexamethasone has to be determined. Finally, prospective studies should investigate the safety of dexamethasone at higher doses (>133 μg·mL–1), when administered perineurally with local anesthetics.
Conclusion
Our systematic review and meta-analysis suggests that local epinephrine and dexamethasone have a synergistic effect. However, without epinephrine, intravenous dexamethasone and perineural dexamethasone share similar effects on block duration, postoperative nausea and vomiting, and postoperative analgesic consumption at 24 hours. At present, and considering the potential risk of the off-label use of dexamethasone perineurally and its as yet unknown mechanism of action, the route of intravenous administration is thus preferable. Further animal and human studies are needed to explore the definite relationship and the potential synergistic mechanism between local dexamethasone and epinephrine and to select the most effective route of administration required to guide clinical practice.
Acknowledgments
The authors show much gratitude to Robert McCarthy for supplying the raw data presented in their studies.
Supplementary materials
Figure S1 Risks of bias for the ten included studies by all authors’ judgment.
Notes: Red, high risk of bias; yellow, unclear risk of bias; green, low risk of bias.
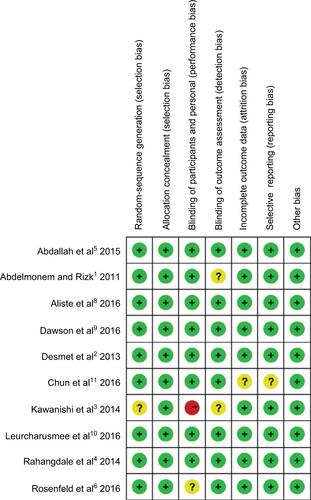
Figure S2 Funnel plots of duration of analgesia: adding epinephrine (left) and not adding epinephrine (right).
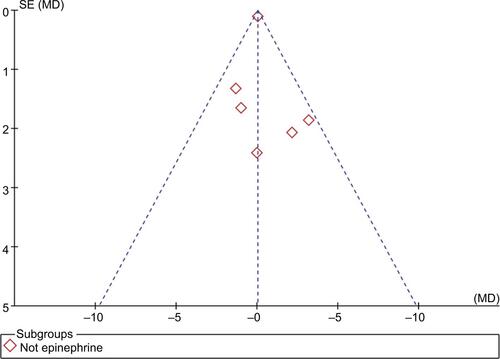
Figure S3 Funnel plot of postoperative nausea and vomiting.
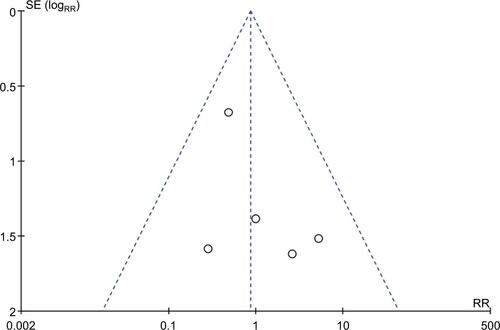
Table S1 Search strategy
Table S2 Definitions
Disclosure
The authors report no conflicts of interest in this work.
References
- AbdelmonemARizkSNComparative study between intravenous and local dexamethasone as adjuvant to bupivacaine in perianal blockEgypt J Anaesth2011273163168
- DesmetMBraemsHReynvoetMI.V. and perineural dexamethasone are equivalent in increasing the analgesic duration of a single-shot interscalene block with ropivacaine for shoulder surgery: a prospective, randomized, placebo-controlled studyBr J Anaesth2013111344545223587875
- KawanishiRYamamotoKTobettoYPerineural but not systemic low-dose dexamethasone prolongs the duration of interscalene block with ropivacaine: a prospective randomized trialLocal Reg Anesth201475924817819
- RahangdaleRKendallMCMcCarthyRJThe effects of perineural versus intravenous dexamethasone on sciatic nerve blockade outcomes: a randomized, double-blind, placebo-controlled studyAnesth Analg201411851113111924686045
- AbdallahFWJohnsonJChanVIntravenous dexamethasone and perineural dexamethasone similarly prolong the duration of analgesia after supraclavicular brachial plexus block: a randomized, triple-arm, double-blind, placebo-controlled trialReg Anesth Pain Med201540212513225629321
- RosenfeldDMIvancicMGHattrupSJPerineural versus intra-venous dexamethasone as adjuncts to local anaesthetic brachial plexus block for shoulder surgeryAnaesthesia201671438038826899862
- ChunEHKimYJWooJHWhich is your choice for prolonging the analgesic duration of single-shot interscalene brachial blocks for arthroscopic shoulder surgery? Intravenous dexamethasone 5 mg vs. perineural dexamethasone 5 mg randomized, controlled, clinical trialMedicine (Baltimore)20169523e382827281084
- AlisteJLeurcharusmeePEngsusophonPA randomized comparison between intravenous and perineural dexamethasone for ultrasound-guided axillary blockCan J Anaesth2017641293627663451
- DawsonRLMcLeodDHKoerberJPPlummerJLDracopoulosGCA randomised controlled trial of perineural vs intravenous dexamethasone for foot surgeryAnaesthesia201671328529026682721
- LeurcharusmeePAlisteJVan ZundertTCA multicenter randomized comparison between intravenous and perineural dexamethasone for ultrasound-guided infraclavicular blockReg Anesth Pain Med201641332833327015546
- ChunEHKimYJWooJHWhich is your choice for prolonging the analgesic duration of single-shot interscalene brachial blocks for arthroscopic shoulder surgery? Intravenous dexamethasone 5 mg vs. perineural dexamethasone 5 mg randomized, controlled, clinical trialMedicine (Baltimore)20169523e382827281084
References
- MillerRDMiller’s Anesthesia7th edPhiladelphiaChurchill Livingstone2009
- CandidoKDKnezevicNNAll adjuvants to local anesthetics were not created equal: animal data evaluating neurotoxicity, thermal hyperalgesia, and relevance to human applicationReg Anesth Pain Med201136321121221508791
- KirkseyMAHaskinsSCChengJLiuSSLocal anesthetic peripheral nerve block adjuvants for prolongation of analgesia: a systematic qualitative reviewPloS One2015109e013731226355598
- ArulkumarSElnagarIHamiltonCFoxCDexamethasone as an adjunct for brachial plexus blockade: meta-analysis2014 Available from: http://www.lsuhscshreveport.edu/Assets/uploads/LSUHealthShreveport/Documents/Anesthesiology/Posters/DexamethasoneRegionalAnesthesiaIARS2014.pdfAccessed June 13, 2017
- HuynhTMMarretEBonnetFCombination of dexamethasone and local anaesthetic solution in peripheral nerve blocks: A meta-analysis of randomised controlled trialsEur J Anaesthesiol2015321175175825774458
- ChoiSRodsethRMcCartneyCJEffects of dexamethasone as a local anaesthetic adjuvant for brachial plexus block: a systematic review and meta-analysis of randomized trialsBr J Anaesth2014112342743924413428
- De OliveiraGSJrAlmeidaMDBenzonHTMcCarthyRJPerioperative single dose systemic dexamethasone for postoperative pain: a meta-analysis of randomized controlled trialsAnesthesiology2011115357558821799397
- LeeSChoiSIntravenous and perineural dexamethasone in peripheral nerve block: are they truly equivalent?Anesth Analg20151211251
- SondekoppamRVUppalVGanapathySIntravenous or perineural dexamethasone for interscalene brachial plexus block: the equivalence not yet provenBr J Anaesth20141121175176
- TigheSQPerineural or intravenous dexamethasone: do we still need catheters?Anaesthesia201671898398427396259
- BolinEDWilsonSPerineural versus systemic dexamethasone: questions remain unansweredReg Anesth Pain Med201540439339426079360
- AlbrechtEKernCKirkhamKRPerineural vs intravenous administration of dexamethasone: more data are availableBr J Anaesth20151141160
- HozoSPDjulbegovicBHozoIEstimating the mean and variance from the median, range, and the size of a sampleBMC Med Res Methodol200551315840177
- AbdelmonemARizkSNComparative study between intravenous and local dexamethasone as adjuvant to bupivacaine in perianal blockEgypt J Anaesth2011273163168
- DesmetMBraemsHReynvoetMI.V. and perineural dexamethasone are equivalent in increasing the analgesic duration of a single-shot interscalene block with ropivacaine for shoulder surgery: a prospective, randomized, placebo-controlled studyBr J Anaesth2013111344545223587875
- KawanishiRYamamotoKTobettoYPerineural but not systemic low-dose dexamethasone prolongs the duration of interscalene block with ropivacaine: a prospective randomized trialLocal Reg Anesth201475924817819
- RahangdaleRKendallMCMcCarthyRJThe effects of perineural versus intravenous dexamethasone on sciatic nerve blockade outcomes: a randomized, double-blind, placebo-controlled studyAnesth Analg201411851113111924686045
- AbdallahFWJohnsonJChanVIntravenous dexamethasone and perineural dexamethasone similarly prolong the duration of analgesia after supraclavicular brachial plexus block: a randomized, triple-arm, double-blind, placebo-controlled trialReg Anesth Pain Med201540212513225629321
- ChunEHKimYJWooJHWhich is your choice for prolonging the analgesic duration of single-shot interscalene brachial blocks for arthroscopic shoulder surgery? Intravenous dexamethasone 5 mg vs. perineural dexamethasone 5 mg randomized, controlled, clinical trialMedicine (Baltimore)20169523e382827281084
- DawsonRLMcLeodDHKoerberJPPlummerJLDracopoulosGCA randomised controlled trial of perineural vs intravenous dexamethasone for foot surgeryAnaesthesia201671328529026682721
- LeurcharusmeePAlisteJVan ZundertTCA multicenter randomized comparison between intravenous and perineural dexamethasone for ultrasound-guided infraclavicular blockReg Anesth Pain Med201641332833327015546
- RosenfeldDMIvancicMGHattrupSJPerineural versus intravenous dexamethasone as adjuncts to local anaesthetic brachial plexus block for shoulder surgeryAnaesthesia201671438038826899862
- AlisteJLeurcharusmeePEngsusophonPA randomized comparison between intravenous and perineural dexamethasone for ultrasound-guided axillary blockCan J Anaesth2017641293627663451
- Morales-MuñozCSánchez-RamosJLDiaz-LaraMDGonzález-GonzálezJGallego-AlonsoIHernández-del-CastilloMSAnalgesic effect of a single-dose of perineural dexamethasone on ultrasound-guided femoral nerve block after total knee replacementRev Esp Anestesiol Reanim2017641192627372380
- RückerGCarpenterJRSchwarzerGDetecting and adjusting for small-study effects in meta-analysisBiom J201153235136821374698
- NiemiGBreivikHAdrenaline markedly improves thoracic epidural analgesia produced by a low-dose infusion of bupivacaine, fentanyl and adrenaline after major surgery: a randomised, double-blind, crossover study with and without adrenalineActa Anaesthesiol Scand19984288979099773133
- SakaguchiYSakuraSShinzawaMSaitoYDoes adrenaline improve epidural bupivacaine and fentanyl analgesia after abdominal surgery?Anaesth Intensive Care200028552252611094667
- BoussofaraMCarlesMRaucoules-AimeMSellamMRHornJLEffects of intrathecal midazolam on postoperative analgesia when added to a bupivacaine-clonidine mixtureReg Anesth Pain Med200631650150517138191
- KazemeiniARahimiMFazeliMSThe effect of local injections of bupivacaine plus ketamine, bupivacaine alone, and placebo on reducing postoperative anal fistula pain: a randomized clinical trialScientificWorldJournal2014201442415225544955
- TrifaMEngelhardtTKhalifaSBThe addition of clonidine to bupivacaine in saphenous/sciatic nerve blocks in childrenPaediatr Anaesth201626332132226814039
- XiangQHuangDYZhaoYLCaudal dexmedetomidine combined with bupivacaine inhibit the response to hernial sac traction in children undergoing inguinal hernia repairBr J Anaesth2013110342042423161357
- MartinezVFletcherDDexamethasone and peripheral nerve blocks: on the nerve or intravenous?Br J Anaesth2014113333834024907282
- Yilmaz-RastoderEGoldMSHoughKAGebhartGFWilliamsBAEffect of adjuvant drugs on the action of local anesthetics in isolated rat sciatic nervesReg Anesth Pain Med201237440340922430023
- BuvanendranAKroinJSLiJMoricMTumanKJRelative contribution of adjuvants to local anesthetic for prolonging the duration of peripheral nerve blocks in ratsReg Anesth Pain Med201641558959227483415
- AnKElkassabanyNMLiuJDexamethasone as adjuvant to bupivacaine prolongs the duration of thermal antinociception and prevents bupivacaine-induced rebound hyperalgesia via regional mechanism in a mouse sciatic nerve block modelPloS One2015104e012345925856078
- BarnesPJAnti-inflammatory actions of glucocorticoids: molecular mechanismsClin Sci (Lond)19989465575729854452
- WilliamsBAHoughKATsuiBYIbinsonJWGoldMSGebhartGFNeurotoxicity of adjuvants used in perineural anesthesia and analgesia in comparison with ropivacaineReg Anesth Pain Med201136322523021519308
- WatkinsTWDupreSCoucherJRRopivacaine and dexamethasone: a potentially dangerous combination for therapeutic pain injectionsJ Med Imaging Radiat Oncol201559557157726076198
- HwangHParkJLeeWKCrystallization of local anesthetics when mixed with corticosteroid solutionsAnn Rehabil Med2016401212726949665
- AwadKAhmedHAbushoukAIDexamethasone combined with other antiemetics versus single antiemetics for prevention of postoperative nausea and vomiting after laparoscopic cholecystectomy: an updated systematic review and meta-analysisInt J Surg201636Pt A15216327793640
- AlbrechtEKernCKirkhamKRA systematic review and meta-analysis of perineural dexamethasone for peripheral nerve blocksAnaesthesia2015701718325123271