
Abstract
Introduction
The practice and study of pain management pose myriad ethical challenges. There is a consensual opinion that adequate management of pain is a medical obligation rooted in classical Greek practice. However, there is evidence that patients often suffer from uncontrolled and unnecessary pain. This is inconsistent with the leges artis, and its practical implications merit a bioethical analysis. Several factors have been identified as causes of uncontrolled and unnecessary pain, which deprive patients from receiving appropriate treatments that theoretically they have the right to access. Important factors include (with considerable regional, financial, and cultural differences) the following: 1) failure to identify pain as a priority in patient care; 2) failure to establish an adequate physician–patient relationship; 3) insufficient knowledge regarding adequate prescription of analgesics; 4) conflicting notions associated with drug-induced risk of tolerance and fear of addiction; 5) concerns regarding “last-ditch” treatments of severe pain; and 6) failure to be accountable and equitable.
Objective
The aim of this article was to establish that bioethics can serve as a framework for addressing these challenging issues and, from theoretical to practical approaches, bioethical reflection can contextualize the problem of unrelieved pain.
Methods
This article is organized into three parts. First, we illustrate that pain management and its undertreatment are indeed ethical issues. The second part describes possible ethical frameworks that can be combined and integrated to better define the ethical issues in pain management. Finally, we discuss possible directions forward to improve ethical decision making in pain management.
Discussion
We argue that 1) the treatment of pain is an ethical obligation, 2) health science schools, especially medical training institutions, have the duty to teach pain management in a comprehensive fashion, and 3) regulatory measures, which prevent patients from access to opioid treatment as indicated in their cases, are unethical and should be reconsidered.
Conclusion
Developing an ethical framework for pain management will result in enhanced quality of care, linking the epistemic domains of pain management to their anthropological foundations, thereby making them ethically sound.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
The practice and study of pain management pose numerous ethical challenges.Citation1 Twenty years ago, CasselCitation2 described how medicine’s singular focus on curing the diseases of the body precluded it from being able to attend to the suffering of the individual. His core insight “persons suffer, bodies do not” has major explanatory power for medicine’s neglect of human pain. It is true that if medicine can delineate the physical/biological pain as its domain/responsibility and leave the rest to other professionals, then medicine can insulate itself from the responsibility to acknowledge and respond to pain and suffering resulting from a patient’s experience of illness.Citation3 Since such insulation is generally not possible, we are faced with an ethical dilemma.Citation4
Pain management faces a number of difficult ethical questions, which are perhaps too numerous to elucidate. The questions include: What importance does pain have in medicine? What role does pain management play in the clinical care of patients? What duties do health care professionals have concerning the pain of their patients? What other duties must be balanced against the duty to provide adequate analgesia?
This article posits that bioethics can make important contributions to solving these challenging issues. From theoretical to practical approaches, bioethical reflection can illuminate the problem of unrelieved pain. This article is organized into three parts. First, we illustrate that pain management and its neglect constitute ethical issues. Second, we describe potential ethical frameworks that can be combined and integrated to shape and organize some of the critical ethical issues in pain management. Finally, we discuss possible directions forward that will hopefully improve ethical decision making in pain management.
The facts
Pain is a common symptom in clinical practice, placing special demands on health care professionals as well as the patients they treat.Citation5 Knowledge of pain (as a symptom, disease, and/or illness and phenomenon, ie, total pain) must be the basis for all constructs in pain medicine.Citation6–Citation11 Due to the incredible complexity of pain, the treatment of patients with refractory pain is also complex and, accordingly, can be demanding. The clear articulation of pain medicine can be challenging, especially considering the current economic, legal, and social environments.
Two phenomena regarding pain management are indisputable. First, health care professionals have an ethical obligation to relieve pain.Citation12 Second, this obligation has been largely neglected.Citation4 All types of pain (eg, traumatic, postoperative, chronic, non-cancer, cancer, and end of life) remain largely untreated and undertreated. Several studies have illuminated this problem: 80% of patients who undergo surgical procedures experience acute postoperative pain, and ~75% of those with postoperative pain report the severity as moderate, severe, or extreme.Citation13 An inordinately large proportion of nursing home residents are estimated to experience pain daily in nursing homes ranging from 40% to 85%, with as many as 25% of these older adults receiving no intervention for pain relief.Citation14 Pain is highly prevalent among nursing home residents with moderate-to-severe dementia (61.5%), and only 30.7% of patients were treated with analgesic drugs.Citation15 Even at the end of life, the data regarding adequate pain management remain discouraging; nearly one of two patients with cancer pain is undertreated;Citation16–Citation19 there is significant disparity in pain treatment adequacy with the odds of undertreatment twice as high for minority patients,Citation13 and more than 65% of nursing home residents with cancer had pain.Citation20 So widespread are the stories of unrelieved pain at the end of life that some believe that public support for euthanasia or physician-assisted suicide is driven by the fear of dying in pain.Citation4
Various barriers to effective pain management (relief of pain and suffering as well as improvement in function and quality of life) have been described in the literature: 1) failure of physicians to identify pain as a priority in patient care, which relates to the prevalence of the curative model over a person-centered care paradigm as well as the dominance of the scientific approach over the humanistic approach;Citation21 2) failure of physicians to develop adequate relationships with their patients, which threatens the possibility of understanding the subjective language of pain;Citation22 3) insufficient knowledge regarding pain management;Citation3,Citation23–Citation25 4) fears associated with opioid prescription and utilization for pain relief (eg, addiction, tolerance, dependence, and adverse side effects);Citation3,Citation25–Citation27 5) failure of health care systems to hold clinicians accountable for pain relief;Citation3,Citation26,Citation28 6) patients’ and family members’ resistance to using opioids;Citation23,Citation29 7) the “war on drugs and addiction”Citation4 and the consequent “pendulum swing”;Citation30,Citation31 and 8) cost constraints.Citation3,Citation26,Citation32
Diverse problems have been described in the pain management literature that, in our opinion, strengthens the importance of an ethical analysis. Evidence suggests the following: the undertreatment of pain is a realityCitation6 and the prevalence and societal burden of chronic pain are underestimated; treatment is not always instituted and/or adequate;Citation33 the inappropriate overutilization of pharmacologic agents and techniques without assuming a holistic approach toward pain management;Citation6,Citation33 and the tensions and conflicts that can occur between the stakeholders involved in pain medicine at all levels (micro–meso–macro).Citation34–Citation38
Ethical decision making in pain management
How we think about pain exerts an influence on the manner in which we respond to it. Our ability and willingness to hear, detect, trust, treat, and report which rely, to an extent, on our understanding of the essence and meaning of pain come ideally from a phenomenological perspective.Citation39,Citation40 Thus, how we think about pain is ideally guided by those unspoken and unconscious assumptions, myths, and metaphors that shape our understanding of the individual sufferer’s reality and experience of pain. Any effort to improve pain management will necessitate working not only at institutional, regulatory, and policy levels but also, simultaneously and explicitly, at the conceptual one.
The practice of medicine and, more broadly, health care is theoretically an ethical enterprise.Citation3 Indeed, the relief of all forms of pain and suffering is an ethical duty of health care professionals and societies as well and has been recognized throughout the world as an ethical demand and human right.Citation41–Citation44 The patient should be the primary interest of medicine and physicians are obliged to act first and foremost in the best interest of their patients.Citation45 Determining the “good” is the work of ethics, entailing the implementation of decision-making processes.Citation6
Nonetheless, there seems to be a failure of many health care systems to hold clinicians accountable for pain management.Citation3 Physicians and other health care professionals, organizations, systems, and societies fail to provide both effective pain management and holistic care. This denotes an alarming failure of medical professions to recognize the ethical implications of undertreated pain and the unnecessary suffering that it engenders.Citation3
From our perspective, an overview of the existing ethical theories is needed to ensure the sound ethical reasoning and judgment required for adequate pain management. Theories differ according to which aspect of the ethical situation they assume as the focus of their attention. The agent, the action itself, the consequences of the action, the relationships of the agent, and the specific characteristics of the situation have all been the focus of one or more ethical theories. Taking into consideration the specific case of pain management, integrating distinct approaches needs to be considered to better structure the main ethical dimension and framework of pain management: 1) an ethics of care, with a particular focus on the physician–patient relationship as a therapeutic alliance using a narrative-based ethics that takes into consideration the subjective dimensions of language pertaining to pain and 2) the ethical framework of the so-called principlism.
The importance of care-based ethics
Patient–physician relationships can be categorized into three main models: 1) paternalistic, deliberative, interpretive, informative;Citation46 2) paternalistic, shared, informed;Citation47 and 3) patient-active, collaborative, passive.Citation48 As physician and patient endeavor to exchange information, emotions can dominate the clinical encounter, and the traditional models may not address this emotional exchange. In fact, in a humanistic approach, this dialogical task is strongly about ethics; this ethics encounter fosters the capacity of physicians to see themselves as a character in others’ stories.Citation49 Thus, physicians relying on the traditional models of care may fail in treating those patients who have emotionally distressing symptoms.Citation50 Regardless of the model of patient–physician dyad, this relationship is ideally characterized by a therapeutic alliance between the one suffering (vulnerable) and the one caring (responsible). The development of such a relationship requires cognitive skills, emotional preparation, and reflective capacity. However, since the “curative model” in modern medical education and practice remains prominent, the development of these types of skills remains challenging and uncharacteristic. Therefore, an approach on care-basedCitation49,Citation51,Citation52 as well as virtue-based ethicsCitation53–Citation55 may be envisaged as potential guides for answers to this type of problem. In our opinion and as stated by Benner,Citation56 the major point of contrast between virtue- and care-based ethics lies in the manner in which virtues are manifested. In virtue-based ethics, the point of scrutiny lies in the inner character of the actor, whereas in care-based ethics, the focus is relational, ie, how virtues are lived out in specific relationships, particularly unequal relationships in which certain members are vulnerable. Accordingly, pain and its optimal management challenge the defiant straddling of the mind–body dualism characteristic of this curative model that persists in much of Western culture.
In fact, the curative model, immersed in the biases of dualism in medicine, has been the subject of critique, as it appears to create a hostile environment for the ideal care of severely ill and dying patients.Citation3 Often, the curative model of care is perceived as “competing” with that of person-centered care, as if these two models should or could represent completely separate and distinct realms.Citation3 More recent perspectives emphasize the need for integrationCitation57 with pain management and palliative care being considered simultaneously as an approach and a specialist area of care provision. The ideal paradigm requires the integration of the main principles, values, and practices of palliative care with those of person-centered care in all forms, areas, and settings.Citation58–Citation61
Commonly utilized diagnostic tests cannot communicate the intensity, duration, quality, and personal dimensions of pain, as they are something that only the sufferer can appreciate.Citation40 Ideally, physicians observe, listen to, and trust the patient’s narrative of pain and talk with the patients, which are skills that physicians are not necessarily taught in their formal training.
Physicians do not trust (hence, hear) the human voice[…] they in effect perceive the voice of the patient as an unreliable narrator of bodily events, a voice which must be bypassed as quickly as possible so that they can get around and behind it to the physical events themselves.Citation4
Therefore, an “ethics of care” is crucial to foster a relationship-based ethics, based on an “emotional commitment and willingness to act on behalf of persons with whom one has a significant relationship”Citation62 that focuses on empathic association rather than solely on individual rights. This “ethics of care” is relevant to pain management because it challenges impartiality and detachment, as well as universal principles in ethics, as an important component of the therapeutic alliance. Total pain and suffering, in particular, may be perceived best in an empathic relationship characterized by a rich narrative interchange, which calls attention to consideration of the importance of narrative-based ethics.
The importance of narrative-based ethics
Modern medical practices have, at times, abstracted the problem of pain from its context and story. Therefore, from our perspective, another important ethical theory through which to frame pain management is narrative-based ethical theory. In this article, the story of the individual case becomes of core importance and of paramount understanding. The subjectivity of pain makes communication essential to its management and relief.
“Physical pain – unlike any other state of consciousness – has no referential content. It is not of or for anything”.Citation63 The task of describing pain lends itself to the use of metaphors, allowing it to take the shape of something with a more familiar exterior, such as a “sharp nail” or “hot flame.”Citation4 Unless one is its “owner,” little about pain lends credence to its existence. Although people may display signs of pain (eg, a grimaced face, an absent appetite, and an irritable disposition), these remain signs of something interior and something not necessarily easily described by the one in pain nor easily believed by those who do not experience it. This is especially true if they, as care givers, are not familiar with the practical guides for the assessment of the existence of pain and its accurate evaluation. Pain has been described as having an invisible geography that has no reality because it has not yet manifested itself on the visible surface of the earth.Citation39 The experiential gap between the bearer of pain and the observer is so wide that it is said to have an epistemic impact. In other words, as stated by ScarryCitation63 that “to have pain is to have certainty; to hear about it is to have doubt.” The believability of pain is confounded by its subjectivity, as it is often the case with subjective experience. Pain cannot be generalized on the basis of objective factors that signal a particular therapeutic response. Each individual experiences pain quite differently, depending on factors as variable as neurobiology, culture, religious beliefs, previous experiences of pain, and current psychological and spiritual states of feeling.
Narrative medicineCitation64 stands out as a logical pathway for integration in pain management, as it aims to address each individual patient’s experience as a source of data and a resource through which to better attend and understand the pain condition. It requires the collection of patients’, caregivers’ and health care professionals’ stories both to provide patients with more effective care and foster shared decision making. The stories told by all stakeholders and the practice of reflective writing and closed reading set up a common ground of shared expectations, fears, and doubts. These can provide privileged access to the inner world of those who suffer and those who care.Citation65 By emphasizing this first-person narrative, the entirety of the person in pain can be considered, rather than simply focusing on signs and symptoms.
However, narrative-based ethical theories are not without limitations. Because they are so rich with respect to the individual case, it becomes more difficult to generalize across cases. How does one develop policies tied to narratives?Citation24 Principle-based ethical theories, that are further described, can offer a structured means of solving conceptual and bio-ethical problems, creating a template to aid in the making of complex and difficult decisions. Nonetheless, they need some bottom-up, case-based supplementation through casuistry narrative methods.Citation24 These top (principles) to/from the bottom (narratives) can indeed only be realized through a care approach between the physician and the patient. In fact, as previously claimed by other authors (including Vanlaere and GastmansCitation51), care can hardly be the only point of departure of an ethical perspective and needs to be complemented with universal principles to possess the normativity that is characteristic of a full ethical perspective; care starts from a sentiment, which is required for one to act in an ethically responsible way. However, without the addition of principles that link this sentiment to a “universal ethical standard” (such as justice), arbitrariness and favoritism will lurk.
Relevant ethical principles in pain management
Health care professionals must seek to provide biomedical, technical, and scientific goods in ways that allow adequate appreciation for patients’ values, goals, and choices and convey respect for the patient as a person.Citation6,Citation66 An applied ethics of pain medicine must be pragmatic and therefore cannot rely upon or be reduced to a single principle or ethical system.Citation6
There exists a broadly based humanistic ethics, which applies to the domain of medical care giving patients a strong prima facie right to freedom from unnecessary pain. Such an approach places two concomitant moral obligations toward patients upon medical professionals. First, there is a responsibility not to inflict additional pain and suffering beyond that which is absolutely necessary (primum non nocere).Citation55 Second, there is the responsibility to do all than can be performed within the current limits of knowledge and available resources to relieve pain and suffering.Citation67 Responsibility and accountability at micro (individual, health care professionals), meso (interprofessionals, teams, health care and education organizations), and macro (health care systems, education systems, policies such as pain as the fifth vital sign) levels are paramount. Indeed, personal and professional responsibility/accountability for failing to treat patients competently and compassionately is critical, as it is to create environments that make effective care for patients in pain the norm.Citation68 This dual connection between responsibility and accountability must take other bioethical principles into consideration, as well: autonomy, vulnerability, integrity, dignity, and justice.
Unrelieved pain may leave patients extremely vulnerable, speechless, changed, and even destroyed. In common medical ethics parlance, unrelieved pain can compromise a person’s autonomy and increase vulnerability,Citation69 whereas providing pain relief can potentially protect a person’s integrity and promote dignity. The consent process, for example, demonstrates respect for patients’ values and decision-making capacities. However, autonomy can be compromised in a suffering person when provider goals are directed by the immediate needs of the sick body or by the compulsion to address what is perceived to be the source of suffering. This issue should be taken into account when caring for a patient in pain.Citation2 Regrettably, the term “vulnerable” too often is used without any concrete meaning. Given the absence of commonly accepted standards for the identification and solution to the issue of vulnerability, a list of six types of vulnerability has been proposed: cognitive, juridical, deferential, medical, allocational, and infrastructural.Citation63 These six types of vulnerability might also represent an ethically relevant feature that bespeaks vulnerability in the context of pain care.Citation70,Citation71
Physicians have a duty to take positive steps to help others, which goes beyond simply refraining from harmful acts. In fact, health care professionals who witness unnecessary pain have an ethical (and also a deontological) responsibility toward those patients, even if they are not clinically responsible for them.Citation72 Thus, the further notion that moderate-to-severe pain can be physically and psychologically harmful, treating patients in a holistic fashion will be a more fruitful approach.Citation37,Citation39 Patients with pain often become vulnerable and despaired, and therefore at risk of trying anything that all-too-willing health and non-health practitioners might recommend. When is an aggressive intervention a compassionate and understandable effort as opposed to taking advantage of a vulnerable patient? Given the large multitude of interventions available today for pain management, desperate individuals with unremitting pain may find unqualified and/or greedy practitioners who may take advantage of a patient by performing unnecessary or overly extensive procedures. The practitioner, on the other hand, may believe that he or she is acting in the best interest of the patient, even if the primary motivation of the practitioner is financial. This severely challenges the principle of non-maleficence.Citation67
We may recognize the existence of other “vulnerable” groups of patients with pain, such as those who cannot communicate verbally (children, older people, and unconscious patients), end-of-life patients, and socioeconomically disadvantaged patients. This latter group, in particular, tests the ethical principle of justice, conceived as the fair distribution and access to health care for all persons/citizens who need it.Citation62
In addition to respecting autonomy, considering vulnerability, preventing harm, and promoting good for patients, physicians have an obligation to promote justice in the distribution of these goods/services. Distributive justice refers to fair, equitable, and appropriate distribution of a privilege, benefit, or service within a society. Problems of distributive justice arise under conditions of scarcity and competition in which there is not enough to provide all that each needs or desires.Citation39 As an example, we may argue that currently, financial constrains make it more difficult in almost all systems to provide necessary monitoring of patients (eg, due to work overload, time pressure, and resource shortages), therefore hindering the humanistic and relational approaches is needed to effectively assess, manage, and control pain. In fact, evidence suggests that access to pain control and palliative care is currently grossly inequitable.Citation43 Furthermore, the likelihood that the lack of equity will continue to increase, particularly in societies in which medicine has become corporatized, ought not to be underestimated.Citation73
Western health care systems are dominated by a paradigm that emphasizes “disease” as the basic element of pathology and health care provision.Citation74 However, as OslerCitation75 recognized, it is more important to know “what sort of patient has a disease (risk factor or adverse effect) than to know what sort of disease a patient has.”Citation76,Citation77 A person-focused or population group-focused (rather than a disease-focused) view of morbidity and pain can ethically reveal and address inequity (ie, the presence of systematically and potentially remediable differences among population groups defined racially, culturally, socially, economically, or geographically). There exists therefore the need to further develop and implement guidelines and approaches that are appropriate to person-focused care rather than to disease-focused care. Obtaining information on the current impact of inequities on access to pain care is a critical initial step toward action, since equitable access to care is of vital importance in all health care systems.
The way forward
As discussed earlier, the barriers to high-quality pain management are numerous and complex. Often-cited impediments include 1) the lack of education and training on state-of-the-art pain management, 2) the lack of institutional mechanisms for standardizing the assessment and treatment of pain, 3) the lack of accountability for the undertreatment of pain, and 4) federal and state statutes and regulations designed to fight a “war on drugs and addiction” that negatively affect the legitimate use of controlled substances.Citation4 There is an uncomfortable irony in Blacksher’sCitation4 prophecy of the deleterious impact of this “war” on patients with pain in 2001, ie, at a time at which the severity of the harms that are currently being performed to patients by the “war” was not yet being realized. Further strategic actions are needed to improve pain management and provide answers to these problems from an ethical perspective. Three ethical approaches have accordingly been presented in this article. The first pertains to reflection on and analysis of the nature of pain itself. The second is related to pain’s personal dimensions. The third refers to the intersubjectivity embedded in the assessment and treatment of pain. All converge on one essential feature of good pain management: attending to the person in pain.Citation4
From our perspective, educational interventions that consider the specific nature of pain and the issues previously detailed must be designed for “both” patients and health care professionals to enhance the ethical robustness of pain management. Basic undergraduate education and postgraduate education programs are needed to stimulate cognitive skill acquisition, emotional development, and the capacity of reflective insight.Citation78 Appropriate competencies for pain management can be promoted by encouraging clinicians to actively engage the humanistic dimensions of medicine and gain insight into their own feelings and attitudes. Even though knowledge does not necessarily translate into actions, using ethical arguments to establish “the good” is often the first step in motivating behavioral change toward such. Strategies for education regarding ethical issues in pain management can provide the proper balance between the essential knowledge and skills of the curative model and those of the person-centered care model.Citation3,Citation78–Citation80 This can ensure the development of a more comprehensive paradigm of pain management that recognizes the complexity of pain as a “total” phenomenon and experience. Consequently, this approach accounts for economic factors imposed upon health care systems and enables the articulation of any paradigmatic revision within the contemporary medicolegal environment.Citation6
A better understanding of what influences one’s interpretation of a person in pain is part of the process of cultivating an ethical sensitivity to the personal dimensions of pain and suffering. Because identifying with the pain of others does not necessarily come naturally to all health care professionals, the pedagogical tools used by medical humanity courses may be especially valuable in efforts to improve the state of pain care. The use of literature, movies, and other art forms can be considered an important tool, as all are designed to stimulate human emotions and the capacity to relate to those living in circumstances very different from one’s own.Citation4,Citation39,Citation79,Citation81
Dispelling the myriad myths associated with pain and its care will be no easy matter. Part of the solution depends on educating and training health care professionals in the state-of-the-art of pain management. In addition, ethics cases chosen for teaching settings need to reflect a broader array of pain management scenarios. Bioethics, as a field, has been accused of experiencing an aversion to such everyday evils.Citation4 Nevertheless, case-based ethics learning approaches might prove to be an invaluable tool in teaching developing professionals who will treat pain.
Conclusion
Anyone who has personally experienced severe acute or chronic pain will grasp its ethical dimensions and frameworks. However, the challenge to pain management lies on the other side of that experience: moving people not in pain to acknowledge, treat, and care for those who are in pain. In summary, a “patient-centered” view of pain is more accurate more efficient, safer, more equitable, and better aligned with the core principles and philosophy of medicine. To diminish inequity and the neglect and marginalization of pain care, health care systems and medicine need to be redefined.
In our opinion, decision-making practices informed by person-centered dimensions (patient as a person, characteristics of the physician, patient–physician communication and relationship) that take into account an array of ethical theories (eg, ethics of care and virtues, narrative medicine/approach ethics, and principle-based ethics) may constitute a constructive approach to an ethics framework for pain management. Accordingly, as we have proposed a novel ethics of care, this model places a particular focus on the physician–patient relationship as an ethics encounter, using narrative-based ethics approaches that take into consideration the subjective dimensions of language pertaining to pain, and the ethical principles of the so-called principlism. This is of particularly importance given the International Association for the Study of Pain’s consideration of 2018 as the global year for excellence in pain education. Accordingly, this framework, which is illustrated in , will hopefully contribute to this initiative, motivating and reskilling pain physicians on cognitive, emotional, and reflective skills, rather than just technical ones, with these “nontechnical” skills of particular importance to vulnerable patients with pain. This can be illustrated through a core philosophy of medicine as specific and focal to the uniqueness of pain, of the patient and of the health care professional.
Figure 1 Integrated ethical framework for pain management.
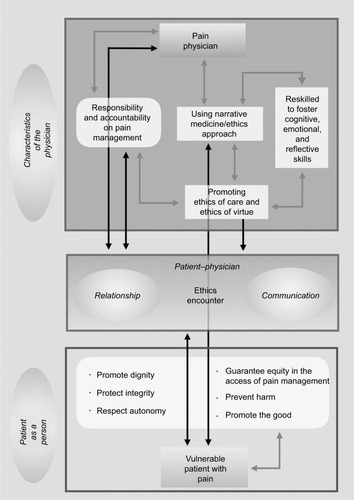
This ethical framework of pain management will allow us to 1) further respect ethical principles (integrity, autonomy, equity, non-maleficence, and beneficence) and, thus, patients’ dignity, 2) acknowledge and explain the vulnerabilities illuminated by pain and recognize the variability and subjectivity of its expression through narratives of both patients and physicians, 3) reduce asymmetries and thereby improve patient–clinician relationships and communication, and 4) be more fully responsible and accountable for the overall management of pain. Such will result in “good” care, linking the epistemic domains of pain management to its anthropological foundations, and accordingly will be ethically sound.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
This article was written during the period of the following projects: InPalIn (Integration of Palliative Care and Intensive Care), NOS (Narrar, Ouvir Sentir), and subproject ETHICS II of project ENSURE (Enhancing the Informed Consent Process: Supported decision-making and capacity assessment in clinical dementia study). Therefore, SMP, PHM, and ASC would like to thank Fundação Grünenthal and Fundação Merck, Sharpe, and Dohme for the funding provided for the project InPalIn. SM, CCG, JA, and ASC would like to thank Fundação Calouste Gulbenkian for the funding provided to the project NOS. PHM, JA, SMP, and ASC would like to thank the Portuguese Foundation for Science and Technology (Fundação para a Ciência e a Tecnologia – FCT) and the EU COFUND ERA-NET Program for the funding provided to the subproject ETHICS II of Project ENSURE. The authors would also like to thank Mr Diogo Morais for the graphical work of .
Disclosure
The authors declare that no funding was obtained to conduct this study. The authors report no conflicts of interest in this work.
References
- GallagherRMEthics in pain medicine: good for our health, good for the public healthPain Med200122878915102294
- CasselEThe nature of suffering and the goals of medicineN Engl J Med1982306116396457057823
- RichBAAn ethical analysis of the barriers to effective pain managementCamb Q Healthc Ethics200091547010721469
- BlacksherEHearing from pain: using ethics to reframe, prevent, and resolve the problem of unrelieved painPain Med20012216917515102307
- MurinsonBBAgarwalAKHaythornthwaiteJACognitive expertise, emotional development, and reflective capacity: clinical skills for improved pain careJ Pain200891197598318984501
- GiordanoJSchatmanMEAn ethical analysis of crisis in chronic pain care. Part 1. Facts, issues, and problems in pain medicinePain Physician200811448349018690277
- GiordanoJSchatmanMEA crisis in chronic pain care: an ethical analysis. Part two: proposed structure and function of an ethics of pain medicinePain Physician200811558959518850024
- GiordanoJChanging the practice of pain medicine writ large and small through identifying problems and establishing goalsPain Physician20069428328517066114
- SaundersCCare of the dying. Control of pain in terminal cancerNurs Times19592310311032
- SaundersCDrug treatment in the terminal stages of cancerCurr Med Drugs1960111628
- ClarkD‘Total pain’, disciplinary power and the body in the work of Cicely Saunders, 1958–1967Soc Sci Med199949672773610459885
- The American Academy of Pain Medicine Council on EthicsThe American Academy of Pain Medicine Ethics Charter: American Academy of Pain Medicine2003 Available from http://www.painmed.org/files/ethics-charter.pdfAccessed December 21, 2017
- American Pain SocietyGuidelines on the management of postoperative painJ Pain201617213115726827847
- RussellTLMadsenRWFlesnerMRantzMJPain management in nursing homes: what do quality measure scores tell us?J Gerontol Nurs201036124956
- MiuDKYChanKCUnder-detection of pain in elderly nursing home residents with moderate to severe dementiaJ Clin Gerontol Geriatr2014512327
- DeandreaSMontanariMMojaLApoloneGPrevalence of under-treatment in cancer pain. A review of published literatureAnn Oncol200819121985199118632721
- FischMJLeeJWeissMProspective, observational study of pain and analgesic prescribing in medical oncology outpatients with breast, colorectal, lung, or prostate cancerJ Clin Oncol201230161980198822508819
- van den Beuken-van EverdingenMHJde RijkeJMKesselsAGSchoutenHCvan KleefMPatijnJPrevalence of pain in patients with cancer: a systematic review of the past 40 yearsAnn Oncol20071891437144917355955
- Te BoveldtNVernooij-DassenMLeppinkISamwelHVissersKEngelsYPatient empowerment in cancer pain management: an integrative literature reviewPsychooncology201423111203121124816749
- PimentelCBBriesacherBAGurwitzJHRosenABPimentelMTLapaneKLPain management in nursing home residents with cancerJ Am Geriatr Soc201563463364125900481
- QuinteroGAMedical education and the healthcare system – why does the curriculum need to be reformed?BMC Med201412121325387484
- BuchmanDZHoAIllesJYou present like a drug addict: patient and clinician perspectives on trust and trustworthiness in chronic pain managementPain Med20161781394140626759389
- KressHGAhlbeckKAldingtonDManaging chronic pain in elderly patients requires a CHANGE of approachCurr Med Res Opin20143061153116424450746
- SchreiberJACantrellDMoeKAImproving knowledge, assessment, and attitudes related to pain management: evaluation of an interventionPain Manag Nurs201415247448123419934
- ManchikantiLFalcoFJBoswellMVHirschJAFacts, fallacies, and politics of comparative effectiveness study: part 2-implications for interventional pain managementPain Physician2009131E55E79
- KingNBFraserVUntreated pain, narcotics regulation, and global health ideologiesPLoS Med2013104e100141123565063
- TaylorALLawrenceOGKatrinaAPEnsuring effective pain treatment: a national and global perspectiveJAMA20082991899118167410
- PaseroCMcCafferyMComfort-function goals: a way to establish accountability for pain reliefAm J Nurs200410497781
- McPhersonCJHadjistavropoulosTDevereauxALobchukMMA qualitative investigation of the roles and perspectives of older patients with advanced cancer and their family caregivers in managing pain in the homeBMC Palliat Care20141313925140119
- SchatmanMEDarnallBDA pendulum swings awry: seeking the middle ground on opioid prescribing for chronic non-cancer painPain Med2013145617
- AtkinsonTJSchatmanMEFudinJThe damage done by the war on opioids: the pendulum has swung too farJ Pain Res2014726526824872719
- AndrewRDerrySTaylorRSStraubeSPhillipsCJThe costs and consequences of adequately managed chronic non-cancer pain and chronic neuropathic painPain Pract2014141799423464879
- KressHGAldingtonDAlonEA holistic approach to chronic pain management that involves all stakeholders: change is neededCurr Med Res Opin20153191743175426172982
- SchatmanMELebovitsAHOn the transformation of the “profession” of pain medicine to the “business” of pain medicine: an introduction to a special seriesPain Med201112340340521332931
- FerrellBDeanGEEthical issues in pain managementJ Palliat Care199410367727844648
- BornemanTFerrelBEthical issues in pain managementClin Geriatr Med19961236156288853949
- FerrellBRNovyDSullivanMDAmerican Pain Society/American Academy of Pain Ethics Task ForceEthical dilemmas in pain managementJ Pain20012317118014622827
- BernhoferEEthics and pain management in hospitalized patientsOnline J Issues Nurs20111711122320876
- SullivanMEthical principles in pain managementPain Med20001327427915101894
- SchatmanMEPsychological assessment of Maldynic pain: the need for a phenomenological approachGiordanoJMaldynia: Inter-Disciplinary Perspectives on the Illness of Chronic PainNew YorkInforma Healthcare2010157182
- World Health Organization [webpage on the Internet]WHO Definition of Palliative Care2002 Available from: www.who.int/cancer/palliative/definition/en/Accessed January 2014
- Worldwide Palliative Care AllianceGlobal Atlas of Palliative Care at the End of LifeLondonWorldwide Palliative Care Alliance2014
- KnaulFMFarmerPEBhadeliaABermanPHortonRClosing the divide: the Harvard Global Equity Initiative–Lancet Commission on global access to pain control and palliative careLancet2015386999572272425762055
- BrennanFCarrDBCousinsMPain management: a fundamental rightAnesth Analg2007105120522117578977
- SchoffermanJPRF: too good to be true?Pain Med20067539517014597
- EmanuelEJEmanuelLFour models of the physician-patient relationshipJAMA199226716222122261556799
- CharlesCGafniAWhelanTDecision-making in the physician-patient encounter: revisiting the shared treatment decision-making modelSoc Sci Med199949565166110452420
- DegnerLFSloanJADecision-making during serious illness: what role do patients really want to play?J Clin Epidemiol19924599419501432023
- AustinWThe ethics of everyday practice: healthcare environments as moral communitiesANS Adv Nurs Sci2007301818817299287
- FoxEPredominance of the curative model of medical care. A residual problemJAMA199727897617639286838
- VanlaereLGastmansCA personalist approach to care ethicsNurs Ethics2001182161173
- FrySTThe philosophical foundations of caringLeiningerMMEthical and moral dimensions of careDetroitWayne State University Press19901324
- SulmasyDPDignity and bioethics: history, theory, and selected applicationsHuman Dignity and Bioethics Essays Commissioned by the President’s Council on BioethicsPresident’s Council on BioethicsWashington, DC2008476480
- OakleyJCockingDVirtue Ethics and Professional RolesCambridgeCambridge University Press2001
- PellegrinoEDThomasmaDCVirtues in Medical PracticeOxfordOxford University Press1993
- BennerPA dialogue between virtue ethics and care ethicsTheor Med1997181–247619129392
- World Health OrganizationStrengthening of palliative care as a component of integrated treatment throughout the life courseJ Pain Palliat Care Pharmacother201428213013424779434
- Hernández-MarreroPMartins PereiraSA valence issue or a transformational definition: is palliative care no more, no less than high-quality care?MałeckaKGibbsRAnd Death Shall Have Dominion: Interdisciplinary Perspectives on Dying, Caregivers, Death, Mourning and the BereavedOxfordInter-Disciplinary Press20156171
- NelsonJECortezTBCurtisJRIntegrating palliative care in the ICU: the nurse in a leading roleJ Hosp Palliat Nurs2011132899421874122
- BrueraEHuiDConceptual models for integrating palliative care at cancer centersJ Palliat Med201215111261126922925157
- BeiderSAn ethical argument for integrated palliative careEvid Based Complement Alternat Med20052222723115937565
- BeauchampTLChildressJFPrinciples of Biomedical Ethics5th edNew YorkOxford University Press2001
- ScarryEThe Body in PainOxfordOxford University Press1985
- CharonRNarrative medicine: form, function, and ethicsAnn Intern Med20011341838711187429
- CharonRNarrative and medicineN Engl J Med2004350986286414985483
- PellegrinoEDThe healing relationship: the architectonics of clinical medicineShelpEEThe Clinical Encounter The Moral Fabric of the Patient-Physician RelationshipDordrechtSpringer1983153172
- LebovitsAEthics and pain: why and for whom?Pain Med200122929615102296
- JohnsonMCollettBCastro-LopesJMThe challenges of pain management in primary care: a pan-European surveyJ Pain Res2013639340123723719
- TaitRCVulnerability in clinical study with patients in pain: a risk analysisJ Law Med Ethics2009371597219245603
- KipnisKVulnerability in study subjects: a bioethical taxonomyEthical and Policy Issues in Study Involving Human Participants. Volume II: Commissioned PapersRockville, MDNational Bioethics Advisory Commission (NBAC)2001G1G13
- ten HaveHVulnerability: Challenging BioethicsNew YorkRoutledge2016
- ShapiroRSHealth care providers’ liability exposure for inappropriate pain managementJ Law Med Ethics19962443603649180522
- SchatmanMEPain and corporatization: more special interests, more disparities, more vulnerabilityPain Med201112463263321463473
- KaplanBEcholsM‘One Health’ – the Rosetta stone for 21st century health and health providersVet Ital200945337738220391400
- OslerWRemarks on specialismBoston Med Surg J1892126457459
- GoldenRLRolandCGSir William OslerSan FranciscoNorman Publishing1988
- JohnMFrom Osler to the cone techniqueHSR Proc Intensive Care Cardiovasc Anesth201351575823734290
- LoeserJDSchatmanMEChronic pain management in medical education: a disastrous omissionPostgrad Med2017129333233528276788
- AraújoJGomesCCJácomoAMartins PereiraSTeaching bioethics in high schoolsHealth Educ J2017764507513
- Martins PereiraSTeixeiraCMCarvalhoASHernández-MarreroPInPalInCompared to palliative care, working in intensive care more than doubles the chances of burnout: results from a nationwide studyPLoS One2016119e016234027612293
- MagalhãesSNarrative in medicine and history: how fiction reminds us of who we areAdv Soc Sci Res J201637176183