
Abstract
Background
Improving pain and stress assessments in neonates remains important in preventing the short- and long-term consequences. We aimed to identify the relationships between different pain assessment parameters by simultaneously measuring changes in cortical, autonomic, hormonal, physiological, and behavioral evoked responses to venepuncture in healthy, full-term neonates.
Methods
This observational, prospective study (ancillary to the ACTISUCROSE trial) included 113 healthy, 3-day old, full-term neonates who underwent venepuncture for systematic neonatal screening, from July to October 2013, in a tertiary-level maternity ward of a university hospital. During venepuncture, we simultaneously measured the cortical single-channel near-infrared spectroscopy (NIRS) signals, foot skin conductance, salivary cortisol, physiological responses, and behavioral (Neonatal Facial Coding System [NFCS]) evoked responses.
Results
Regarding the NIRS analysis, the highest correlation was between the NFCS at venepuncture and the change in NIRS integrated values of total hemoglobin (r=0.41, P<0.001) or oxygenated hemoglobin (r=0.27, P<0.001). The NFCS at venepuncture was moderately positively correlated with changes in salivary cortisol (r=0.42, P<0.001) and skin conductance (r=0.29, P<0.001). Salivary cortisol and skin conductance changes were not correlated; the latter parameters were not correlated with heart rate, respiratory rate, or SpO2.
Conclusion
During venepuncture, NFCS was mildly or moderately correlated with salivary cortisol, skin conductance, and cortical NIRS changes.
Introduction
Hospitalized newborn infants undergo a significant number of clinically required stressful or painful procedures.Citation1 Carbajal et alCitation1 reported medians of 10 painful procedures per day during hospitalization and 75 during a 6-week study period in term and preterm newborns. Among these procedures, 79.2% did not include specific pre-procedural analgesia.Citation1 It is widely reported that the short- and long-term sequelae of repeated pain experiences can lead to altered brain architecture or neurodevelopmental impairments.Citation2–Citation4 Despite a large number of studies on the assessment and treatment of neonatal pain, among hospitalized newborns, pain management was reported to be highly heterogeneous, with low rates of pain assessment and treatment during painful procedures.Citation1,Citation5 Improving the assessment of neonatal pain during hospital stays remains highly important to prevent short- and long-term consequences.
Current clinical bedside pain scoring systems are essentially based on assessments of the neonate’s behavioral and physiological responses, such as facial expression, body movements, heart rate, and oxymetry. Of the large number of existing pain scales, five have been rigorously evaluated: the Neonatal Facial Coding System (NFCS), Douleur Aiguë du Nouveau-né [Acute Pain of the Neonate], Neonatal Pain and Sedation Scale, Behavioral Indicators of Infant Pain, and Premature Infant Pain Profile (PIPP).Citation6–Citation11 However, discrepancies have been reported between the pain severity determined with these scales and the pain-specific cortical activity measured with electroencephalogram (EEG) or near-infrared spectroscopy (NIRS) in term and preterm newborns.Citation12–Citation14 In some situations, behavioral observation-based scales could be limited to measurements of the subcortical somatic and autonomic motor pathways; consequently, they were not suitable for diagnosing the pain experience with accuracy in neonates.Citation13,Citation15
Even when all is not known about the mechanisms of pain experience in the non-verbal infant, different nociceptive responses have been well described. These responses are present as early as 25 weeks of gestation.Citation16–Citation18 Thus, neonatal pain experiences could be assessed with different measurements, including cortical, behavioral, physiological, autonomic, or hormonal measurements, and more accurately, with multidimensional assessments.Citation14,Citation19 For example, cortical pain responses to painful events can be measured with NIRS and EEG in full-term and preterm newborn infants.Citation16,Citation17,Citation20 Specific, noxious-evoked neural activity was recorded with EEG by Slater et al in term and preterm newborn infants.Citation12,Citation21 The EEG could be considered the most specific instrument for assessing cortical responses to pain, but it is not readily applied in daily practice.Citation17 Cortical responses to pain were also recorded with NIRS. Those signals showed specific responses to painful events, compared to non-painful events, in term and preterm newborns even when associated with a withdrawal reflex, which implied hemodynamic changes.Citation16,Citation22 In particular, NIRS measurements of oxygenated hemoglobin [HbO2] showed pain-associated increases in the contralateral somatosensory cortex.Citation22
Other neurophysiological measurements, like skin conductance, heart rate variability, or hormonal assessments of salivary cortisol concentrations, have been reported to be potentially reliable tools for discriminating pain in neonates.Citation23–Citation26 Evaluations of skin conductance, as a reflection of autonomic function, were reported to assess pain accurately in neonates as early as 22 weeks of gestation.Citation27–Citation29 In addition, pain exposure causes hormonal modifications.Citation30 Thus, significant increases in salivary cortisol have been observed after a painful or stressful experience in term and preterm newborns.Citation26,Citation31
To date, in routine clinical practice, no gold standard has been identified for accurately quantifying pain in neonates. More research is needed to improve our knowledge in this field. In particular, pain can be assessed with a multidimensional approach, which includes measurements of cortical, behavioral, hormonal, and physiological responses.Citation32 Relationships between different pain assessment indices need to be first established in healthy full-term newborn infants, as a knowledge base, before moving to hospitalized full-term or preterm newborn infants. Correlations between pain responses have been reported but they were typically limited to a few measures such as behavioral or physiological parameters.
This study aimed to identify correlations between different pain assessment parameters. To that end, we measured the changes in cortical (NIRS), autonomic (skin conductance), hormonal (salivary cortisol), physiological (heart rate, oxygen saturation), and behavioral (NFCS) evoked responses during a venepuncture in healthy, full-term neonates simultaneously.
Methods
Design and procedures
We conducted an observational, prospective, monocentric study, which was ancillary to the ACTISUCROSE study. ACTISUCROSE was a prospective, randomized, controlled trial. From July to October 2013, we enrolled infants in a tertiary-level maternity ward of a university hospital.Citation33 The trial was primarily designed to evaluate differences in cortical responses to a painful procedure (venepuncture), measured with NIRS, between breastfed and sucrose-administered neonates.Citation33
The present study was nested within the ACTISUCROSE trial. We aimed to measure correlations between different methods of pain assessment. Healthy, 3-day-old, breastfed, full-term, newborn infants (>37 weeks of gestation) were assessed for inclusion, before they underwent venepuncture for systematic neonatal screening. Exclusion criteria were anatomic or chromosomal abnormality; treatment with opioids, barbiturates, or benzodiazepines during their first days of life; or maternal use of opioids.
Interventions
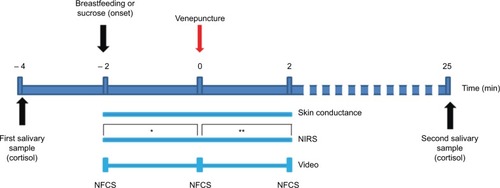
Our multidimensional equipment was set up at least 2 min before venepuncture. The neonates were placed in their mother’s arms in a private maternity room. The equipment included two optodes for NIRS, placed over the somatosensory cortex; three electrodes placed on the sole of the foot for skin conductance measurements; three ECG electrodes for monitoring heart signals; and an oxymeter for monitoring SpO2. The multidimensional assessment was recorded, starting 2 min before the venepuncture, continued throughout the procedure, and ended 2 min after the venepuncture. A video recording was included for analyzing the NFCS. In addition, for cortisol concentration measurements, salivary samples were collected 5 min before and 25 min after the equipment was set up.
We used a single-channel NIRS (NIRO 300, Hamamatsu, Japan) for monitoring oxygenated hemoglobin [HbO2] and total hemoglobin [HbT] concentrations. According to the 10–20 EEG system for identifying key landmarks, the two optodes were placed on the somatosensory cortex, contralateral to the venepuncture site, with an inter-optode distance of 4 cm.Citation22 Previous studies showed that [HbO2] and [HbT] were sufficiently reliable parameters for discriminating pain from non-noxious events in neonates.Citation13,Citation22 The NIRS recorded changes in both oxyhemoglobin [HbO2] and deoxyhemoglobin [HHb] concentrations. We also recorded changes in [HbT] concentrations ([HbO2]+[HHb]) throughout the procedure to compare our findings with previous studies reporting either [HbO2] or [HbT].
Foot skin conductance was monitored with the Med-Storm Pain Monitor. Three electrodes were placed on the sole of one foot. According to previous findings, the number of peaks per second showed the best reliability. Thus, we collected these data throughout the procedure, from 2 min before (−2 min) to 2 min after (+2 min) the venepuncture.Citation34,Citation35 For both skin conductance and NIRS recordings, the nurse researcher marked the starting time of venepuncture on the screens of both the devices.
Salivary cortisol concentrations were assessed 4 min before (−4 min) and 25 min after (+25 min) the venepuncture. We collected saliva according to the method of Morelius et al.Citation25 Briefly, we used two cotton-tipped pins to absorb saliva and centrifuged the cotton pins to elute the saliva. These samples were frozen and stored at −70°C before analysis with radioimmunoassay. Because feeding might interfere with the cortisol concentrations, parents were told not to feed their neonates after the painful procedure, until the last collection of saliva.Citation25,Citation36
Heart rate and SpO2 (measured with oxymetry) were continuously monitored throughout the procedure.
The face and upper part of the infant’s body were continuously recorded on video, from 2 min before (−2 min) to 2 min after (+2 min) the venepuncture (video camera reference: HDR CX740VE; Sony, Tokyo, Japan). The recordings were used to assess the NFCS at −2 min, at venepuncture (0 min), and at +2 min.Citation37 We used the 4-item NFCS version, which included the brow bulge, eye squeeze, deepening of the nasolabial furrow, and opening of the lips. NFCS scores ranged from 0 (no pain) to 4 (severe pain). The video recordings were evaluated by two independent neonatal nurses, previously trained and blinded to the study aim.Citation37 The NFCS has shown good performance parameters, with a 91% inter-observer reliability.Citation37
Blood samples were collected with the venepuncture (23G, Safety blood collection set; Vacuette, Kremsmuenster, Austria), performed on the infant’s hand, according to a standardized procedure. Neonates received either breastfeeding or sucrose administration for a period of 2 min before the painful event ().Citation33
Figure 1 Timeline of the experimental procedure.
Abbreviations: NFCS, Neonatal Facial Coding System; NIRS, near infrared spectroscopy.
Statistical analyses
Group differences in demographic data were compared with the Wilcoxon or chi-square tests. Correlations between parameters were studied with the Pearson or Spearman method, depending on whether the variables were linearly or nonlinearly related.
To show statistical significance, based on the hypothesis of a high correlation of 0.8 with a precision of 0.10, this study would have required a sample of 56 neonates.Citation38 Multiple linear regression was performed for multivariate analyses to determine the multiple correlations between several outcomes. Significantly, the correlated parameters were integrated in a principal components analysis to identify clusters of pain responses.
According to previous studies, the pain response measured with NIRS was defined as the maximum change in hemoglobin ([Hb]), measured as either [HbO2] or [HbT]. These maximum changes were defined as follows: the difference between the maximum [Hb], measured during the 20 s after venepuncture (post-venepuncture), and the mean baseline [Hb], evaluated for over 20 s before the venepuncture (pre-venepuncture).Citation16 According to Bartocci et al and Ozawa et al, the pain response was analyzed as the mean change in [Hb], defined as the difference between the mean [Hb] evaluated during the post-venepuncture and the mean baseline [Hb]. Because [Hb] values can be influenced by body movements, data were excluded when values were more than two standard deviations (SDs) from the mean [Hb] measured post-venepuncture.Citation22,Citation39
Statistical analyses were performed with R 3.4.0 software. Statistical significance was set at P<0.05.
Ethics
The study was approved by the local Ethics Committee (Committee of Protection of Persons, CPP Ouest VI, Brest University Hospital). Written informed consent was obtained from the parents. The trial was registered at ClinicalTrials.gov, number NCT02109263.
Results
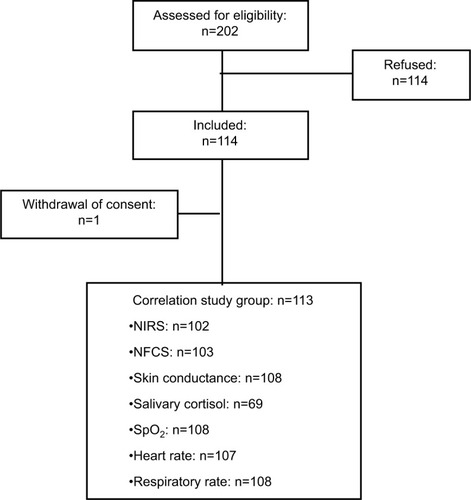
All 113 neonates from the ACTISUCROSE study were included in the correlation analysis (). Data were missing for 5–11 neonates, due to technical problems regarding NIRS, skin conductance, SpO2, NFCS, or heart and respiratory rate analyses. Data on salivary cortisol levels were missing for 39% of the enrolled neonates, due to an insufficient amount of saliva collected, particularly during the pre-venepuncture sampling.
Figure 2 Flowchart of patient selection.
Abbreviations: NFCS, Neonatal Facial Coding System; NIRS, near infrared spectroscopy.
When we grouped the patients according to the analyzed parameter, the demographic characteristics were not different among the groups. Even the salivary cortisol group was similar to the other groups, in mean age, gestational age, birth weight, and sex ratio ().
Table 1 Demographic characteristics of the study sample, grouped by the type of measurement performed
The Hb analysis showed an increasing trend in all parameters analyzed, significantly for the maximum value of [HbO2] and [HbT] parameters during the 20 s post-venepuncture periods (). The NFCS scores were higher at the time of venepuncture compared to the NFCS scores at 2 min before or 2 min after the venepuncture (Wilcoxon test, P<0.01) (). The mean NFCS score assessed after the venepuncture was lower than that assessed 2 min before the event (Wilcoxon test, P=0.02).
Table 2 Parameter values analyzed to assess changes in responses measured before (–), during (0 s), and after (+) venepuncture
Mild to moderate increases in the heart rate and SpO2 values were observed with venepuncture, and a nonsignificant trend to a slight decrease in the respiratory rate was noted (). The mean salivary cortisol concentration measured 25 min after the venepuncture increased significantly from baseline (measured at −4 min) (). Mean number of peaks per second (skin conductance) was not different between the pre- and post-venepuncture periods ().
Due to the number of parameters included in the correlation analysis, only the correlation coefficients with P-values <0.01 were considered statistically significant, to avoid inflation of the alpha risk (). However, we showed the coefficients with P-values <0.05 in (gray values placed within parentheses). Significant correlations were most frequently found between NFCS assessed at the time of venepuncture and the NIRS parameters and during the change in salivary cortisol concentration and during the change in skin conductance.
Table 3 Correlation analysis: Pearson and Spearman correlation coefficients show associations between the different parameters analyzed
Changes in NIRS parameters were often significantly correlated to the NFCS assessed at the time of venepuncture. The parameter most significantly correlated with the NFCS at the time of venepuncture was the change between the post-venepuncture maximum and the baseline [HbT].
Despite significant differences between the mean NFCS scores assessed at the time of venepuncture and at 2 min after the venepuncture, a significant correlation was observed between these NFCS scores (0 min and +2 min). This positive correlation suggested that some neonates tended to maintain elevated NFCS scores for a few minutes after the painful event.
Some parameters, like the changes in SpO2 and the changes in heart rate, were found to be significantly correlated with the [HbO2] parameters. These correlations might be explained by the fact that general hemodynamic changes can influence NIRS measurements.
Multiple linear models were constructed to analyze the associations between NIRS changes ([HbO2] or [HbT]) and NFCS assessed at the time of venepuncture, SpO2 changes, and heart rate changes. Although SpO2 and heart rate parameters might be significantly associated with [HbO2], the NFCS at the time of venepuncture was independently associated with [HbO2] measurements. When both heart rate changes and NFCS were included in a multiple linear model for analyzing associations with [HbT] changes, only NFCS at the time of the venepuncture remained significantly associated. The most significant association was found between the [HbT] change (Δmax +20/mean −20 s) and the NFCS score of 4. These findings suggested that the association between NFCS and [HbT] was strongest when the neonates expressed behavioral signs that indicated the most severe pain.
Significant, moderately positive correlations were found between the NFCS assessed at the time of venepuncture and changes in salivary cortisol or skin conductance. These parameters were also significantly correlated with the NFCS assessed at 2 min after the venepuncture.
Finally, no significant correlations were found between salivary cortisol and skin conductance changes. Moreover, these parameters were not significantly correlated with heart rate, respiratory rate, or SpO2.
The most significant correlations are represented graphically (). The Pearson or Spearman analysis showed that the NFCS assessed at the time of venepuncture was moderately correlated with the [HbT] and [HbO2] changes. However, both the associations could be considered poor, based on the graphical representations; the R2 values (coefficient of determination), derived from simple linear regressions, were <0.20 in both the cases. We noted a high variability in the NIRS changes, particularly for neonates with NFCS scores of 0 or 4.
Figure 3 Graphic representations (boxplots) of the significant correlations between NFCS, assessed at the time of the venepuncture (0 min), and changes in various parameters. (A) Change in [HbO2] (Δ: max [HbO2] at +20 s − mean [HbO2] at −20 s); (B) change in [HbT] (Δ: max [HbT] at +20 s − mean [HbT] at −20 s); (C) change in salivary cortisol concentrations (Δ: [cortisol] at +25 min − at −4 min); and (D) change in skin conductance (Δ: peaks/s at +2 min − peaks/s at −2 min).
Abbreviations: HbO2, oxygenated hemoglobin; HbT, total hemoglobin; NFCS, Neonatal Facial Coding System.
![Figure 3 Graphic representations (boxplots) of the significant correlations between NFCS, assessed at the time of the venepuncture (0 min), and changes in various parameters. (A) Change in [HbO2] (Δ: max [HbO2] at +20 s − mean [HbO2] at −20 s); (B) change in [HbT] (Δ: max [HbT] at +20 s − mean [HbT] at −20 s); (C) change in salivary cortisol concentrations (Δ: [cortisol] at +25 min − at −4 min); and (D) change in skin conductance (Δ: peaks/s at +2 min − peaks/s at −2 min).](/cms/asset/cc60c5fa-5bbb-462f-8b18-353cce1fdbd4/djpr_a_165810_f0003_b.jpg)
The graphical representations also show the associations between NFCS assessed at the time of venepuncture and the changes in skin conductance or changes in salivary cortisol concentrations. However, again, the R2 values were <0.20.
Finally, we found no significant positive correlations between the changes in respiratory rate and the other parameters. Similarly, we found no significant correlations between salivary cortisol changes or skin conductance changes and [HbT] or [HbO2] changes ().
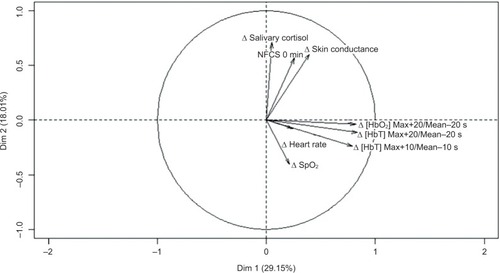
Our principal component analysis revealed two dimensions accounting for almost half of the variance (). The first dimension integrated the NFCS at the time of venepuncture and salivary cortisol concentrations and skin conductance changes. The second dimension integrated the changes in NIRS measurements and in physiological parameters (heart rate, SpO2).
Figure 4 Variable factor map representing the two main dimensions (Dim 1, Dim 2) from the principal components analysis.
Abbreviations: Dim, dimension; HbO2, oxygenated hemoglobin; HbT, total hemoglobin; NFCS, Neonatal Facial Coding System.
Discussion
This study showed that the NFCS assessed at the time of venepuncture was mildly to moderately correlated with salivary cortisol and skin conductance changes in healthy, full-term neonates. Regarding the cortical responses to venepuncture, the parameters highly correlated to NFCS were the NIRS measurements which integrated the [HbT] and evaluated the change between the maximum value measured post-venepuncture and the baseline value measured pre-venepuncture.
To date, this study was the first to simultaneously analyze the changes in NIRS, skin conductance, salivary cortisol, heart rate, oxygen saturation, and NFCS responses to a venepuncture in healthy, full-term neonates.
The parameters that were chosen in this study for analyzing the changes in NIRS, skin conductance, and salivary cortisol were based on the literature and according to how they are used routinely.Citation16,Citation26,Citation35
Our study was an ancillary study, and the sample size was not initially designed to identify the correlations between all the parameters measured. However, all neonates were studied in the same conditions during a standardized venepuncture on the third day of life in healthy full-term neonates. Moreover, our study sample was larger than the theoretical sample calculated and than many other studies reporting neonatal pain assessments.Citation13,Citation22,Citation24,Citation34,Citation40
Our study had some limitations. First, for the NIRS analysis, previous studies have reported that this technique could discriminate between responses to painful versus non-painful stimulations, particularly in the contralateral somatosensory cortex in term and preterm newborn infants.Citation16,Citation22 Thus, our findings could have been limited by the use of a single NIRS device. Second, subsequent studies could investigate more precisely the correlations between the different parameters by assessing the NFCS more continuously (eg, every 30 s) to provide more details about how different parameters were associated with the behavioral responses during the entire procedure.
Our study included full-term, healthy neonates who underwent a unique painful procedure. As a result, these findings cannot be extrapolated to non-healthy neonates or premature infants, who must undergo multiple acute painful or stressful procedures.
We aimed to identify the correlations among different methods for assessing an acute, procedural, and painful event. A correlation analysis of these methods applied during a non-painful event could have been useful in discussing our findings.
The cortisol reactivity to painful events in young infants has been well described, and it appeared to be strongest in the first weeks of life and in preterm infants.Citation31 In one systematic review, non-painful stressors were found to be unlikely to provoke a cortisol reaction. Indeed, Mörelius et al found no correlation between PIPP or Neonatal Infant Pain Scale and salivary cortisol changes after stressful events, like diaper changes in preterm and full-term, healthy neonates.Citation41 In the present study, we reported a significant, moderate correlation between the NFCS and the salivary cortisol change in full-term infants after a painful event. Finally, salivary cortisol changes seemed to be associated more with painful events than with stressful experiences, and the potential marker of an intense physiological response was not necessarily well-correlated with behavioral responses in newborn infants. This correlation continues to be of interest, for example, in studies of sedated newborn infants subject to painful actions and under conditions where behavioral modifications are not expected.
To date, no previous study has evaluated the associations between NFCS and skin conductance assessments. A specific association between skin conductance and the PIPP score was described in full-term infants during painful stimulations, compared to tactile stimulations.Citation24 Those findings led to the hypothesis that skin conductance could serve as a discriminating factor for acute pain. But we found a dissociation between skin conductance and NIRS measurements. Our results suggested that some infants responded acutely to a painful event, which could be measured in a short window with NIRS, but others responded in a prolonged manner that could be measured with skin conductance; thus, the latter response might reflect stress more than pain.
As previously reported, we showed that the changes in NIRS measurements could reflect cortical responses to painful or stressful events. These measurements could be assessed differently; we could either evaluate the changes in NIRS (differences between pre-venepuncture and post-venepuncture values) or evaluate the maximum NIRS values, to discriminate pain in full-term or preterm neonates.Citation16,Citation22,Citation39 By studying these different changes in NIRS measurements, we found the highest correlations between the NFCS and the changes in NIRS parameters. The highest correlation was between NFCS and the difference between the maximum (post-venepuncture) and baseline [HbT] values, measured in the contralateral somatosensory cortex, as described by Slater et al.Citation16 Our choice of a single-channel NIRS recording of activity in the contralateral somatosensory cortex was based on the study by Slater et al, which showed that a double-channel NIRS device provided a good discrimination of pain with a single contralateral channel.Citation16 Nevertheless, although a mono-channel device is more practical in routine clinical practice, we suspect that a multichannel NIRS device might provide better accuracy in analyzing correlations between behavioral and cortical responses.
A previous study showed that an increase in heart rate was associated with an increase in [HbO2] in the somato-sensory cortex after a painful event in preterm infants.Citation22 In that same study, a reduction in SpO2 was observed while [HbO2] increased. Conversely, we found a positive correlation between SpO2 and [HbO2], which indicated a trend toward an increase in the SpO2 with increases in [HbO2]. This discrepancy between studies might be because Bartocci et al studied neonates born between 28 and 36 weeks of gestation. Compared to our full-term neonates, those preterm infants were more likely to exhibit apnea and/or desaturation in response to a stressful or painful event.
Interestingly, Morison et al found a moderate, significant correlation between NFCS and the change in heart rate, based on Pearson correlation coefficients, which ranged from 0.41 to 0.62, depending on the gestational age of the infant (range 23–32 weeks).Citation42 They used the 10-item NFCS, but only the facial expressions were used to study the correlation with the change in heart rate. In contrast, we found no correlation between the NFCS and changes in heart rate among our sample of full-term neonates. This discrepancy pointed out the lack of sensitivity to changes in heart rate among neonates, compared to premature neonates, due to the more mature autonomic system of full-term neonates.
Finally, the correlations that we found between parameters (NIRS, NFCS, salivary cortisol, skin conductance, and physiological parameters) were not remarkably high. Hence, we concluded that these parameters were essentially dissociated with each other during a procedural painful event in full-term neonates. Despite this dissociation, we did find that salivary cortisol and skin conductance were moderately associated with NFCS assessed at 0 or +2 min and that NIRS changes were moderately associated with NFCS assessed at 0 min. By definition, these parameters do not measure the same dimensions of physiological responses to a painful event. Thus, this dissociation may not be interpreted as superior to one parameter over another. The most probable explanation is that full-term neonates have different response profiles to painful or stressful events. The principal component analysis tended to confirm this hypothesis by identifying two clusters of pain responses. Hence, we concluded that some infants showed acute responses, which were more likely to be detected with NIRS and physiological parameters, and others showed prolonged stress responses, which were more likely to be detected with skin conductance and changes in salivary cortisol measurements. This dissociation highlighted the importance of applying an integrated, multidimensional assessment, when attempting to determine neonate responses during or after a painful and/or stressful event.
In addition to the recent development of a multichannel NIRS that is potentially suited to clinical practice, some new devices are currently available. In particular, one new device uses a high frequency analysis to evaluate the heart rate variability index, which serves as a reflection of pain. The reliability of these devices must be assessed in full-term and preterm neonates in a multidimensional assessment of responses during and after painful or stressful events.
Conclusion
NFCS was mildly or moderately correlated with salivary cortisol, skin conductance, and cortical NIRS changes during venepuncture in healthy full-term neonates. Two clusters of pain response profiles were identified. Some neonates presented acute responses measured by NIRS and physiological parameters, and others presented prolonged stressful responses measured by skin conductance, salivary cortisol, and NFCS. These different pain response profiles should be considered in future randomized controlled trials aiming to compare different analgesics by using multimodal pain assessment including at least a scale based on behavioral assessment and the measurement of a physiological parameter like skin conductance changes.
Acknowledgments
The study was supported by grants from the “Institut UPSA de ladouleur” and the “Fondation de France” and was promoted by the Brest University Hospital.
Disclosure
The authors report no conflicts of interest in this work.
References
- CarbajalRRoussetADananCEpidemiology and treatment of painful procedures in neonates in intensive care unitsJAMA20083001607018594041
- GrunauREWhitfieldMFPetrie-ThomasJNeonatal pain, parenting stress and interaction, in relation to cognitive and motor development at 8 and 18 months in preterm infantsPain20091431–213814619307058
- RangerMChauCMGargANeonatal pain-related stress predicts cortical thickness at age 7 years in children born very pretermPLoS One2013810e7670224204657
- VinallJGrunauREImpact of repeated procedural pain-related stress in infants born very pretermPediatr Res201475558458724500615
- American Academy of Pediatrics Committee on Fetus and Newborn, American Academy of Pediatrics Section on Surgery, Canadian Paediatric Society Fetus and Newborn CommitteeBattonDGBarringtonKJWallmanCPrevention and management of pain in the neonate: an updatePediatrics200611852231224117079598
- HummelPLawlor-KleanPWeissMGValidity and reliability of the N-PASS assessment tool with acute painJ Perinatol201030747447819924132
- HolstiLGrunauREInitial validation of the Behavioral Indicators of Infant Pain (BIIP)Pain2007132326427217382473
- JonsdottirRBKristjansdottirGThe sensitivity of the premature infant pain profile – PIPP to measure pain in hospitalized neonatesJ Eval Clin Pract200511659860516364113
- PetersJWKootHMGrunauRENeonatal Facial Coding System for assessing postoperative pain in infants: item reduction is valid and feasibleClin J Pain200319635336314600535
- CarbajalRPaupeAHoennELenclenROlivier-MartinMAPN: evaluation behavioral scale of acute pain in newborn infantsArch Pediatr1997476236289295899
- Committee on Fetus and Newborn and Section on Anesthesiology and Pain MedicinePrevention and management of procedural pain in the neonate: an updatePediatrics20161372e2015427126810788
- SlaterRCornelissenLFabriziLOral sucrose as an analgesic drug for procedural pain in newborn infants: a randomised controlled trialLancet201037697481225123220817247
- SlaterRCantarellaAFranckLMeekJFitzgeraldMHow well do clinical pain assessment tools reflect pain in infants?PLoS Med200856e12918578562
- BenoitBMartin-MisenerRNewmanALatimerMCampbell-YeoMNeurophysiological assessment of acute pain in infants: a scoping review of research methodsActa Paediatr201710671053106628326623
- GokuluGBilgenHOzdemirHComparative heel stick study showed that newborn infants who had undergone repeated painful procedures showed increased short-term pain responsesActa Paediatr201610511e520e52527557529
- SlaterRCantarellaAGallellaSCortical pain responses in human infantsJ Neurosci200626143662366616597720
- FabriziLSlaterRWorleyAA shift in sensory processing that enables the developing human brain to discriminate touch from painCurr Biol201121181552155821906948
- CornelissenLFabriziLPattenDPostnatal temporal, spatial and modality tuning of nociceptive cutaneous flexion reflexes in human infantsPLoS One2013810e7647024124564
- SlaterRFitzgeraldMMeekJCan cortical responses following noxious stimulation inform us about pain processing in neonates?Semin Perinatol200731529830217905184
- VerriotisMFabriziLLeeACooperRJFitzgeraldMMeekJMapping cortical responses to somatosensory stimuli in human infants with simultaneous near-infrared spectroscopy and event-related potential recordingeNeuro201632
- SlaterRFabriziLWorleyAMeekJBoydSFitzgeraldMPremature infants display increased noxious-evoked neuronal activity in the brain compared to healthy age-matched term-born infantsNeuroimage201052258358920438855
- BartocciMBergqvistLLLagercrantzHAnandKJPain activates cortical areas in the preterm newborn brainPain20061221–210911716530965
- FayePMde JonckheereJLogierRNewborn infant pain assessment using heart rate variability analysisClin J Pain201026977778220973153
- ErikssonMStormHFremmingASchollinJSkin conductance compared to a combined behavioural and physiological pain measure in newborn infantsActa Paediatr2008971273018052991
- MoreliusENelsonNTheodorssonESalivary cortisol and administration of concentrated oral glucose in newborn infants: improved detection limit and smaller sample volumes without glucose interferenceScand J Clin Lab Invest200464211311815115248
- MöreliusEHeHGShoreySSalivary cortisol reactivity in preterm infants in neonatal intensive care: an integrative reviewInt J Environ Res Public Health2016133337
- StormHChanges in skin conductance as a tool to monitor nociceptive stimulation and painCurr Opin Anaesthesiol200821679680418997532
- HernesKGMørkridLFremmingAØdegårdenSMartinsenØGStormHSkin conductance changes during the first year of life in full-term infantsPediatr Res200252683784312438658
- MunstersJWallströmLAgrenJNorstedTSindelarRSkin conductance measurements as pain assessment in newborn infants born at 22-27 weeks gestational age at different postnatal ageEarly Hum Dev2012881212621764228
- GitauRFiskNMTeixeiraJMCameronAGloverVFetal hypothalamic-pituitary-adrenal stress responses to invasive procedures are independent of maternal responsesJ Clin Endocrinol Metab200186110410911231985
- JansenJBeijersRRiksen-WalravenMde WeerthCCortisol reactivity in young infantsPsychoneuroendocrinology201035332933819651476
- HartleyCSlaterRNeurophysiological measures of nociceptive brain activity in the newborn infant – the next stepsActa Paediatr2014103323824224180281
- RioualenSDurierVHervéDMiseryLSizunJRouéJMCortical pain response of newborn infants to venepuncture: a randomized controlled trial comparing analgesic effects of sucrose versus breastfeedingClin J Pain201834765065629298184
- Pereira-da-SilvaLVirellaDMonteiroISkin conductance indices discriminate nociceptive responses to acute stimuli from different heel prick procedures in infantsJ Matern Fetal Neonatal Med201225679680121726181
- StormHThe development of a software program for analyzing skin conductance changes in preterm infantsClin Neurophysiol200111281562156811459697
- NelsonNArbringKTheodorssonENeonatal salivary cortisol in response to heelstick: method modifications enable analysis of low concentrations and small sample volumesScand J Clin Lab Invest200161428729111465342
- GrunauREOberlanderTHolstiLWhitfieldMFBedside application of the Neonatal Facial Coding System in pain assessment of premature neonatesPain19987632772869718246
- MoinesterMGottfriedRSample size estimation for correlations with pre-specified confidence intervalQuant Methods Psychol2014102124130
- OzawaMKandaKHirataMKusakawaISuzukiCInfluence of repeated painful procedures on prefrontal cortical pain responses in newbornsActa Paediatr2011100219820320860706
- KarpeJMisiołekADaszkiewiczAMisiołekHObjective assessment of pain-related stress in mechanically ventilated newborns based on skin conductance fluctuationsAnaesthesiol Intensive Ther201345313413724092508
- MöreliusEHellström-WestasLCarlénCNormanENelsonNIs a nappy change stressful to neonates?Early Hum Dev2006821066967616507341
- MorisonSJGrunauREOberlanderTFWhitfieldMFRelations between behavioral and cardiac autonomic reactivity to acute pain in preterm neonatesClin J Pain200117435035811783816