Abstract
Introduction:
Review of opioid prescriptions in a hospital provides valuable information to health care professionals which may contribute to proper pain management; opioid utilization studies may help uncover factors that can be improved for better prescribing. To evaluate the use of opioid analgesics in a university hospital, a review of opioids prescribed in hospitalized patients was developed.
Methods:
Information was obtained from the pharmacy database and medical records. The study period was 1 month.
Results:
Medical records of 1156 patients admitted in July 2009 were analyzed. The most widely prescribed opioid was tramadol; the preferred administration route was intravenous; the main indication was severe pain; and major prescribers were from surgical departments.
Discussion:
Underutilization of potent opioids for acute and chronic pain seems to occur.
Conclusion:
Most prescribers prefer weak opioids, given intravenously to treat acute and chronic pain, while some patients may benefit from the prescription of more potent opioids.
Introduction
Despite having been used for many years, opioid analgesics remain essential in the control of severe pain. Hence, monitoring of opioid prescribing practices is a starting point for acquiring basic information regarding the treatment of pain. Several reports have indicated limited use of opioid analgesics in Colombia, but there has been a recent and important increase in the use of morphine nationwide, although supplies are insufficient and do not meet the national demand.Citation1 At a hospital level, review of prescriptions for opioid analgesics provides both prescribers and administrators with consolidated information on the routine use of these medications, and helps to ensure the quality and safety of prescriptions.Citation2,Citation3
Detailed information about prescriptions is particularly important in relation to opioid analgesics, because of the stigma attached to this family of medicines. This is due to biased overestimation of side effects, leading to reluctance to prescribe opioids. The result is underutilizationCitation4,Citation5 and unnecessary pain experience by patients.Citation6–Citation8
Currently, there is a trend toward greater opioid use due to increased attention paid to the treatment of acute, chronic, and cancer-related pain.Citation9–Citation11 Pain management can benefit the patient in different aspects. In cases of patients with acute postoperative pain treated with adequate analgesic schemes, improved outcomes have been found.Citation12 In patients with chronic pain, pain management can help maintain or improve quality of life.Citation13,Citation14
However, numerous reports indicate inadequate treatment of acute, chronic, and cancer-related pain. The purpose of this present research was to describe the opioid utilization profile in a university hospital and provide information that can be used in the future to compare patterns of opioid use over time.
Materials and methods
A retrospective review of opioid prescription (morphine, hydromorphone, pethidine, fentanyl, oxycodone, methadone, codeine, hydrocodone, and tramadol) during July 2009 at a multidisciplinary 190-bed university hospital in Bogota, Colombia was performed. During the study period, the monthly average occupancy rate was 83.41%. Inpatients were seen in all major subspecialties. Data concerning the opioids prescribed (prescribing physician, type of opioid, route of administration, and doses) as well as the patients’ medical records, were obtained from the hospital pharmacy. Three researchers collected data on relevant clinical variables (age, gender, diagnosis, reason for visit, type of pain, and duration of painful symptoms) from electronic medical records. To ensure accuracy, data were double-checked and recorded using Microsoft Excel. All prescriptions for opioids administered to hospitalized patients during the study period were included.
The inclusion criteria were adult inpatients that had been prescribed opioids. The exclusion criteria were: hospitalized patients who did not receive opioids, outpatients, and obstetric and pediatric patients. The institutional research ethics committee approved the study. It should be noted that treatment of pain in this hospital is an essential factor for accreditation by the Joint Commission on Accreditation.
Statistical analyses
For quantitative variables, means and standard deviations (SDs) were calculated. When variables were asymmetrically distributed, the median was calculated. Qualitative variables were expressed as absolute and relative percentage frequencies. The nonparametric Kruskal–Wallis test was used when appropriate. Bivariate analyses were performed to identify variables associated with the daily dose prescribed. All analyses were two-sided, and the alpha level was 0.05.
Results
The medical records of 1156 patients were reviewed; 705 (60.99%) were female and 451 (39.01%) were male. The mean age was 48.11 years (range, 18–99 years).
Patients were divided into four age groups. The group aged under 44 years was the largest (n = 545, 47.15%), followed by the group comprising patients over 65 years of age (n = 257, 22.23%), those between 45 and 54 years, and those between 55 and 64 years (n = 159, 13.75%). Most of the opioid analgesics were prescribed in the emergency unit (n = 580, 50.17%).
The majority of patients could be grouped into four diagnostic categories based on the pain source: musculoskeletal system, gastrointestinal system, wounds and injuries, and urogenital system (n = 631, 54.58%) (). Most patients were treated for acute pain (n = 1010, 87.37%). Treatment of chronic pain and cancer pain was performed in 89 (7.70%) and 49 (4.24%) patients, respectively. Type of pain was unknown in eight patients due to missing data.
Table 1 Distribution of patients according to diagnosis
Tramadol
The most widely prescribed opioid analgesic was tramadol, prescribed to 606 patients (52.42%) (); 305 (50.33%) were under 44 years, and 113 (18.65%) were over 65 years.
Table 2 Distribution of prescribed opioid analgesics
Tramadol was the most widely prescribed opioid for acute pain (n = 528, 52.28%). Tramadol was also the most frequently used analgesic for chronic pain, with 64 patients (71.91%) being prescribed this medication; 10 (20.41%) out of 49 cancer pain patients were prescribed tramadol.
Tramadol was most frequently administered intravenously (73.80%). The starting intravenous dose for tramadol was 50 mg (SD 6.09) by emergency unit prescribers, 70 mg (SD 56.62) by pain service prescribers, 45 mg (SD 11.03) by inpatient medical services prescribers, and 120 mg (SD 14.49) by inpatient surgical services prescribers (). Tramadol was the preferred opioid analgesic among emergency unit prescribers ().
Figure 1 Opioid analgesic prescribed (%) according to prescribing physician.
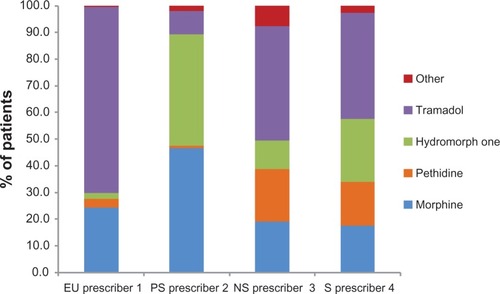
Table 3 Daily doses (milligrams) according to type of pain
Morphine
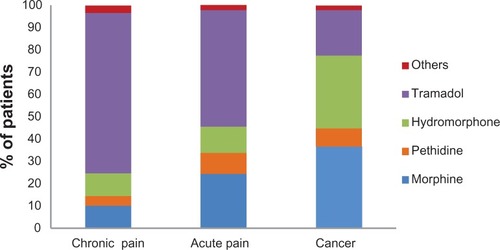
Morphine was the second most prescribed medication (n = 274, 23.70%) (). The most frequent indication for its prescription was acute pain (88.64%). Of the 274 patients prescribed morphine, the largest number was given the drug by emergency unit prescribers (n = 141, 51.46%), followed by inpatient surgical services prescribers (n = 53, 20.87%), then pain service prescribers (n = 48, 17.52%) and inpatient medical services (n = 32, 11.68%). Differences were found for morphine with regard to the type of pain endured by the patient and the daily dose prescribed. The daily dose for chronic pain patients was 5.68 mg (SD 2.95), compared with 8.96 mg (SD 11.08) for patients with acute pain and 24.06 mg (SD 39.86) for cancer pain patients (P = 0.017, nonparametric Kruskal–Wallis test) (). For patients with cancer pain, morphine was the most frequently prescribed analgesic (n = 18, 36.73%) (). Most doses of morphine were administered intravenously (98.60%).
Figure 2 Opioid analgesic prescribed according to type of pain.
Hydromorphone
The most frequent indication for prescription of hydromorphone was acute pain (80.65%). The daily dose of hydromorphone given to acute pain patients (3.77 mg, SD 11.75) was similar to the dose given to patients with chronic pain (3.45 mg, SD 2.32) and cancer pain (4.86 mg, SD 6.95) (P = 0.067, nonparametric Kruskal–Wallis test) (). Approximately one-third of cancer pain patients were prescribed hydromorphone (n = 16, 32.65%). Of the hydromorphone prescriptions, 99.20% were administered intravenously.
Pethidine
Pethidine was prescribed to 103 (8.91%) of the 1156 patients studied. The most frequent indication was acute pain (92.23%). The largest group of prescribers was surgical inpatient services physicians, with 49 patients (47.57%) prescribed pethidine. About half of the patients prescribed pethidine (n = 52, 50.49%) were less than 44 years old, and 21 (20.39%) were over 65.
The daily dose of pethidine given to cancer related pain patients was 52.32 mg (SD 38.88). Of the pethidine prescriptions, 100% were administered intravenously.
Fentanyl
Twelve fentanyl prescriptions were issued. The most frequent indication for its use was acute pain (n = 9, 75.00%). The mean initial dose was 96.67 μg. Most doses were administered intravenously (83.33%). No patches were prescribed during the study period, and no cancer pain patients were prescribed fentanyl.
Other opioid analgesics
With respect to the other opioid analgesics, four (codeine, methadone, oxycodone, and hydrocodone) were prescribed to a small number of patients (n = 14, 1.21%). All of them were taken orally.
Prescribers profile
Overall, the prescription of potent opioid agonists (morphine, hydromorphone, and fentanyl) was different for each group of prescribers. The pain service prescribers utilized this group of potent analgesics the most; of a total of 103 patients given prescriptions by the pain service prescribers, these medications were given to 93 (90.29%). In the surgical inpatient service (n = 301), 127 patients (42.19%) were prescribed these drugs; in the medical inpatient service (n = 168), 55 patients (32.74%) were prescribed potent opioids; of the emergency unit patients (n = 580), 156 patients (26.90%) were prescribed these medicines.
Approximately one-third of the patients (n = 404, 34.95%) were prescribed acetaminophen, whereas other nonsteroidal anti-inflammatory drugs were prescribed to 23.70% of patients (n = 274).
Discussion
The analysis of the treatment of pain using opioid analgesics in 1156 patients admitted to a university hospital in Colombia shows that tramadol was the most frequently prescribed medication for acute and chronic pain, while morphine was most often prescribed for cancer-related pain.
Several factors may explain the popularity of tramadol. First, the results indicate the knowledge of the prescribers regarding tramadol’s effectiveness. Indeed, its efficacy in acute postoperative pain control has been demonstrated following intravenous administration.Citation15 When compared with morphine in the treatment of acute musculoskeletal pain, tramadol has similar efficacy and is an alternative treatment.Citation16 The findings of this present study are consistent with the wide variability in opioid analgesic requirements observed among individuals treated for pain. In relation to its efficacy for chronic pain, a systematic review on chronic low back pain showed that tramadol was more effective than placebo in pain relief assessed after 4 weeks of treatment,Citation17 with a frequency of adverse events similar to that of placebo. In short, if one considers only analgesic efficacy, tramadol prescriptions would be well indicated in patients with acute and chronic pain. The preference for tramadol can also be explained by the lower incidence of respiratory depressionCitation18 as compared with other opioid agonists, a fact that generates greater confidence in the prescriber; it has been acknowledged that fear of respiratory depression is a barrier for morphine prescription. The number of prescriptions may also be explained by the fact that tramadol is not subject to any “special control” by the Ministry of Health because it is an over-the-counter opioid analgesic in Colombia, unlike the other potent opioid analgesics evaluated (morphine, methadone, hydromorphone, pethidine, fentanyl), which are strictly regulated. This government regulation requires doctors to complete special forms and mandates a review of prescriptions by authorities, which hinders the medical use of opioid analgesics.Citation19 In addition, tramadol is marketed by private pharmaceutical companies, whereas the other opioids are distributed noncommercially by the Ministry of Health. This situation favors tramadol use since commercial interests in the consumption of tramadol only have to compete with a very limited state interest regarding the availability of opioids in Colombia.Citation20 Finally, cancer pain studies have also demonstrated tramadol’s efficacy to curb moderate pain.Citation21 However, reports of adverse effects may lead to the increased use of other opioid agonists that cause fewer serious pharmacological reactions than tramadol.Citation22
The factors underlying the morphine prescription results detailed in this study include morphine’s well established efficacy in moderate to severe painCitation23,Citation24 and the fact that morphine is the opioid analgesic that has been used for the longest period of time at the hospital where the research was conducted. On the other hand, the comparatively lower number of morphine prescriptions in comparison to tramadol may be due to a limitation in the knowledge required to prescribe it, or an opioid-phobic attitude of doctors and paramedical staff, which has been documented for opioids for acute pain.Citation25 A notable finding in the treatment of pain in cancer patients is the preference for powerful opioid agonists, as proven by the fact that most prescriptions in this group were for morphine and hydromorphone (). Another interesting finding from the acute pain group is the low number of prescriptions for oral painkillers, a result that contrasts those of a previous study,Citation26 showing that up to 57.0% of patients who took an oral opioid did so to control acute pain. Apart from the natural comfort offered by oral administration, it is recognized to be effective in controlling acute pain after analgesic titration and when gastrointestinal function has recovered. The marked preference for intravenous administration (98.60%) could represent a lack of knowledge of the advantages of oral administration.
The third most commonly used opioid was hydromorphone (12.72%). Its mechanism of action and safety profile are similar to those of morphine. However, it is less well known than morphine and pethidine in this study’s setting, having been available to prescribers for a shorter period of time. In fact, this medicine is not available in many regions of the country. It was administered intravenously in 99.20% of the cases. The most frequent indication for its prescription was acute pain (80.65%).
For pethidine (8.91% of all prescriptions), the most frequent indication was acute pain (92.23%). Currently, this medicine is less frequently prescribed due to its lower analgesic power and its potential for neurotoxicity in patients with impaired renal excretion.Citation27 This low percentage of prescriptions may represent the evolution of prescribers toward better treatment options.
Fentanyl, hydrocodone, oxycodone, codeine, and methadone were prescribed to very few patients (less than 2%). At the hospital where the study was conducted, fentanyl is used almost exclusively in operating rooms and intensive care units, a fact that explains the small number of prescriptions. However, the low number of transdermal fentanyl prescriptions is notable, and no cancer pain patient received fentanyl patches. One possible explanation is the limited number of cancer pain patients in the study sample. Another possible impediment is the clinical skill needed for fentanyl patch prescription. The other three drugs are commonly given orally, which is reflected in their very limited use in this hospital setting.
The low number of prescribed oral analgesics could be due to the absence of a postoperative home-based analgesia program. The great majority of opioid-treated patients were medicated intravenously, possibly because of hospital tradition or the underestimation of the effectiveness of other routes of administration.
This review of the use of opioid analgesics reveals the profile of use of these medicines and can help to identify areas of possible improvement in prescription. Since the type of prescription forms a part of an effective treatment plan for pain, these studies can help to improve analgesia in the hospital. These studies are especially useful in settings with limited resources to improve pain control.
Due to incomplete records, detailed analysis of the use of nonopioid analgesics was not possible. However, it was possible to establish that paracetamol was the analgesic most commonly co-administered with opioid analgesics.
As previously mentioned, a limitation in interpreting these results is that scores for pain intensity (possibly the variable of greatest interest to patients) were not included, and side effects were not recorded. Consequently, analysis of analgesic use partially depended on the dose received, which did not allow us to evaluate the result of the use of specific medications in an integral fashion. Thus, this present study could be a pilot to direct future research to support prescribers in practice. Nevertheless, the data provide useful information that will assist health care professionals working in similar hospitals, such as those in developing countries. In fact, after the completion of this study, the hospital began to record pain intensity in all hospitalized patients and began efforts to avoid duplication of analgesic treatments.
Conclusion
Opioids were most commonly prescribed for acute pain. Overall, prescribers in the hospital studied preferred tramadol to treat acute and chronic pain; however, morphine was the preferred opioid for cancer pain. Pain service prescribers preferred potent opioid agonists for the treatment of all types of pain. Monitoring of opioid prescriptions is recommended as a useful tool that provides clinicians relevant and meaningful feedback to determine optimal treatments for patients.
Disclosure
The authors report no conflicts of interest in this work.
References
- MoyanoJRFiguerasAThe medical consumption of opioids in Colombia, 1997–2007J Pain Palliat Care Pharmacother201024436737321133745
- FigueirasACaamanoFGestal OteroJJMetodología de los estudios de utilización de medicamentos en Atención Primaria. [Methodology of drug utilization studies in primary care.]Gac Sanit200314Suppl 3719 Spanish11459556
- CapellàDLaporteJRMétodos aplicados en estudios descriptivos de utilización de medicamentos. In: JR Laporte y G Tognoni. [Methods used in descriptive studies of drug use. In: Principles of drug epidemiology]Principios de Epidemiología de Medicamentos2nd edBarcelonaMasson-Salvat19936787 Spanish
- Gonzalez-EscaladaJRCreencias, actitudes y percepciones de médicos, farmacéuticos y pacientes acerca de la evaluación y el tratamiento del dolor crónico no oncológicoRev Soc Esp Dolor2009161720 Spanish
- RincónDValeroFPrevención de la náusea y el vómito postoperatoriosRev Col Anest200735293300 Spanish
- AguilarJPeláezREsteveNFernándezSLimitaciones en el uso de opiáceos mayores en dolor crónico no oncológico: ¿”errare humanum est” o procrastinación médica? [Limitations in the use of opioids in chronic noncancer pain: “errare humanum est” or medical procrastination?]Rev Soc Esp Dolor20091646 Spanish
- DavisMPWalshDEpidemiology of cancer pain and factors influencing poor pain controlAm J Hosp Palliat Care20042113714215055515
- BreivikHCollettBVentafridaVCohenRGallacherDSurvey of chronic pain in Europe: prevalence, impact on daily life, and treatmentEur J Pain200610428733316095934
- KehletHMultimodal approach to control postoperative pathophysiology and rehabilitationBr J Anesth199778606617
- MacintyrePEWalkerSMThe scientific evidence for acute pain treatmentCurr Opin Anaesthesiol201023562362820811175
- WuCLRajaSNTreatment of acute postoperative painLancet201137797842215222521704871
- Elvir-LazoOLWhitePFThe role of multimodal analgesia in pain management after ambulatory surgeryCurr Opin Anaesthesiol201023669770320847690
- WonALapaneKLVallowSScheinJMorrisJNLipsitzLALong-term effects of analgesics in a population of elderly nursing home residents with persistent nonmalignant painJ Gerontol A Biol Sci Med Sci200661216516916510860
- PayneRMathiasSDPastaDJWankeLAWilliamsRMahmoudRQuality of life and cancer pain: satisfaction and side effects with transdermal fentanyl versus oral morphineJ Clin Oncol199816158815939552070
- WangFShenXXuSLiuYPreoperative tramadol combined with postoperative small-dose tramadol infusion after total abdominal hysterectomy: a double-blind, randomized, controlled trialPharmacol Rep20096161198120520081257
- VergnionMDegesvesSGarcetLMagotteauxVTramadol, an alternative to morphine for treating posttraumatic pain in the prehospital situationAnesth Analg20019261543154611375843
- ChouRHuffmanLHfor the American Pain Society and American College of PhysiciansMedications for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guidelineAnn Intern Med2007147750551417909211
- PattinsonKTOpioids and the control of respirationBr J Anaesth2008100674775818456641
- DahlJLHow to reduce fears of legal/regulatory scrutiny in managing pain in cancer patientsJ Support Oncol20053538438816218263
- De LimaLSakowskiJAStratton HillCBrueraELegislation analysis according to WHO and INCB criteria on opioid availability: a comparative study of 5 countries and the state of TexasHealth Policy20015629911011275300
- LeppertWTramadol as an analgesic for mild to moderate cancer painPharmacol Rep200961697899220081232
- GillmanPKMonoamine oxidase inhibitors, opioid analgesics and serotonin toxicityBr J Anaesth200595443444116051647
- TrescotAMGlaserSEHansenHBenyaminRPatelSManchikantiLEffectiveness of opioids in the treatment of chronic non-cancer painPain Physician2008112 SupplS181S20018443639
- WuCLCohenSRRichmanJMEfficacy of Postoperative patient-controlled and continuous infusion epidural analgesia versus intravenous patient-controlled analgesia with opioids: a meta-analysisAnesthesiology200510351079108816249683
- MotovSMKhanANProblems and barriers of pain management in the emergency department: are we ever going to get better?J Pain Res2008251121197290
- ChooCYOngCYChanSYOxycodone – an audit of its prescription in a local hospitalAnn Acad Med Singapore2009381194795119956816
- MurtaghFEChaiMODonohoePEdmondsPMHigginsonIJThe use of opioid analgesia in end-stage renal disease patients managed without dialysis: recommendations for practiceJ Pain Palliat Care Pharmacother200721251617844723