Abstract
Among the multiple causes of chronic low back pain, axial and discogenic pain are common. Various modalities of treatments are utilized in managing discogenic and axial low back pain including epidural injections. However, there is a paucity of evidence regarding the effectiveness, indications, and medical necessity of any treatment modality utilized for managing axial or discogenic pain, including epidural injections. In an interventional pain management practice in the US, a randomized, double-blind, active control trial was conducted. The objective was to assess the effectiveness of lumbar interlaminar epidural injections of local anesthetic with or without steroids for managing chronic low back pain of discogenic origin. However, disc herniation, radiculitis, facet joint pain, or sacroiliac joint pain were excluded. Two groups of patients were studied, with 60 patients in each group receiving either local anesthetic only or local anesthetic mixed with non-particulate betamethasone. Primary outcome measures included the pain relief-assessed by numeric rating scale of pain and functional status assessed by the, Oswestry Disability Index, Secondary outcome measurements included employment status, and opioid intake. Significant improvement or success was defined as at least a 50% decrease in pain and disability. Significant improvement was seen in 77% of the patients in Group I and 67% of the patients in Group II. In the successful groups (those with at least 3 weeks of relief with the first two procedures), the improvement was 84% in Group I and 71% in Group II. For those with chronic function-limiting low back pain refractory to conservative management, it is concluded that lumbar interlaminar epidural injections of local anesthetic with or without steroids may be an effective modality for managing chronic axial or discogenic pain. This treatment appears to be effective for those who have had facet joints as well as sacroiliac joints eliminated as the pain source.
Introduction
Epidural injections are one of the most commonly utilized treatment modalities for managing chronic low back pain with or without lower extremity pain.Citation1–Citation12 Despite increasing utilization of lumbar epidural injections, significant debate continues regarding their effectiveness, specifically any conditions other than disc herniation and compressive radiculitis. The pathophysiology of low back pain and radicular pain is the subject of ongoing research and controversy, with discogenic pain assuming a major role as a cause of non-specific low back pain, beyond disc herniation.Citation13–Citation16 In fact, soon after the description of intervertebral disc herniation by Mixter and BarrCitation17 in American medical literature in 1934 with their landmark description of the herniated nucleus pulposus, Mixter and AyersCitation18 showed that radicular pain can occur without disc herniation. Further, non-specific low back pain constitutes 80% or 90% of low back pain without identifiable causes with a large proportion having chronic axial low back pain secondary to progressive degenerative disc disease.Citation2,Citation19–Citation22 It has been shown that discs have innervation with deep ingrowth into degenerated intervertebral discs.Citation23–Citation26 Animal models have identified upregulation of various molecules such as calcitonin gene-related peptide and substance P in dorsal root ganglion neurons innervating degenerated intervertebral discs.Citation27,Citation28 Research also has detected high levels of inflammatory mediators in degenerated discs. While the majority of patients with axial low back pain improve with conservative management, various types of interventions have been described for chronic patients, but most interventions are highly variable and are associated with poor outcomes.Citation29–Citation40
In the past, all axial pain was attributed to disc degeneration. However, the development of controlled diagnostic blocks, and interventional techniques including discography, facet joint blocks, and sacroiliac joint blocks, have provided evidence that axial pain can also be caused by facet joints and sacroiliac joints. Utilizing provocation discography, the prevalence of pain due to internal disc disruption was reported to be 39% in patients suffering with chronic low back pain,Citation41 whereas primary discogenic pain was reported in 26%Citation42 when no other cause was suspected. In addition, facet joint pain has been shown to be present in 21%–41% of patients,Citation43 whereas sacroiliac joint pain has been established in 10%–38% of a selected population.Citation44
The underlying mechanism of action for epidurally administered local anesthetic and steroids has been described, though not well understood. However, historically it has been believed that epidural steroids function by reducing inflammation, thus limiting the indications to compressive radiculopathy or, at best, radiculitis secondary to chemical irritation. Much of the literature on lumbar interlaminar epidurals has been negative except in recent years when fluoroscopic guidance was utilized.Citation39,Citation45–Citation53 A variation of lumbar interlaminar injections, caudal epidural injections, have also been proven to be effective in multiple causes of low back pain with or without lower extremity pain.Citation38,Citation48,Citation54–Citation57 Recent evidence also has demonstrated effectiveness for fluoroscopically administered epidural injections in the cervical spineCitation58–Citation61 as well as the thoracic spine.Citation62 These evaluations have illustrated the effectiveness of epidural injections not only for disc herniation, but also for axial or discogenic pain after eliminating facet and sacroiliac joint pain, spinal stenosis, and post-surgery syndrome. In fact, in the published preliminary results of the current study, lumbar interlaminar epidural injections provided improvement in 74% of patients who received local anesthetic only, and 63% in the group who received local anesthetic and steroids.Citation39
The current report evaluates the role of lumbar interlaminar epidural injections for patients with chronic axial or discogenic low back pain in 120 patients with a 1-year follow-up.Citation39
Methods
This active control, randomized, double-blind trial was conducted in an interventional pain management practice, in a specialty referral center, with approval of the Institutional Review Board (IRB). It follows Consolidated Standards of Reporting Trials (CONSORT) guidelines.Citation63 The study is registered with the US Clinical Trial Registry with an assigned number of NCT00681447.
The internal resources of the practice were used to conduct the study. There was no external funding, either from industry or from elsewhere.
Interventions
Patients were assigned into one of two groups. Group I patients received lumbar interlaminar epidural injections with 6 mL of lidocaine 0.5% preservative free; Group II patients received lumbar interlaminar epidural injections with 5 mL of lidocaine 0.5% preservative-free mixed with 6 mg or 1 mL of non-particulate betamethasone.
Participants
All patients were recruited from new patients presenting to the center who met the inclusion criteria. The IRB-approved protocol and informed consent, which described in detail all aspects of the study and its process, were provided to all participating patients.
Pre-enrollment data collection
The data collected included Numeric Rating Scale (NRS) for pain, Oswestry Disability Index 2.0 (ODI) for functional status, medical and surgical history of any co-existing disease(s), radiologic investigations, physical examination, work status, and opioid intake.
Inclusion criteria
Inclusion criteria included only the patients with a diagnosis of lumbar axial or discogenic pain; over the age of 18 years; a history of chronic function-limiting low back pain of at least 6 months duration; and the ability to understand the study protocol and provide voluntary, written informed consent, and participate in outcome measurements.
Additional criteria were a failure to improve with conservative management, including, but not limited to, physical therapy, chiropractic manipulation, exercises, drug therapy, and bedrest.
Exclusion criteria were a positive response for lumbar facet joint or sacroiliac joint pain by means of controlled, comparative local anesthetic blocks; previous lumbar surgery; uncontrollable or unstable opioid use; uncontrolled psychiatric disorders; uncontrolled medical illness, either acute or chronic; any conditions that could interfere with the interpretation of the outcome assessments; pregnant or lactating women; and a history or potential for adverse reaction(s) to local anesthetics or steroids.
Description of interventions
All participating patients were evaluated with controlled, comparative local anesthetic lumbar facet joint nerve blocks or sacroiliac joint injections. The process started with diagnostic facet joint nerve blocks with 0.5 mL of 1% lidocaine, followed by the blockade of facet joint nerves with 0.25% bupivacaine on separate occasions. A positive response was 80% pain relief.Citation42–Citation44,Citation64 Controlled, comparative local anesthetic blocks were also performed for suspected sacroiliac joint pain, with 2 mL of 1% lidocaine and 0.25% bupivacaine.Citation42,Citation44
Lumbar interlaminar epidural procedures were performed by one physician (LM) in an ambulatory surgery setting, in a sterile operating room, utilizing fluoroscopy. Patients were in the prone position with intravenous access and sedation as indicated. The epidural space entry was confirmed by an injection of non-ionic contrast medium. All procedures were performed either between L5 and S1 or at a higher level based on the patient’s pain complaints. Following this, an injection of 6 mL of lidocaine hydrochloride 0.5% preservative-free, or 5 mL of lidocaine mixed with 6 mg of non-particulate betamethasone was given.
Additional interventions
If a patient required additional lumbar interlaminar epidural injections, these were provided based on the response to the previous injection, with deterioration of pain relief to less than 50%. Patients who were non-responsive and continued with conservative management were followed without further epidural injections with medical management, unless they requested unblinding.
Co-interventions
There was no specific physical therapy, occupational therapy, bracing, or other interventions offered other than the study intervention. In addition, if patients were improving significantly and the medical necessity for drugs was lacking, medications were stopped or dosages were decreased. For some patients, based on medical necessity, dosages were increased. However, all patients continued previously directed exercise programs, as well as their employment.
Objective
The study was designed to assess the effectiveness of lumbar interlaminar epidural injections containing local anesthetic with or without steroids in managing chronic axial low back pain of discogenic origin.
Outcomes
Primary outcome measures included the NRS on a scale of 0–10, and the ODI on a 0–50 scale. Secondary outcome measures included employment status, and opioid intake in terms of morphine equivalents. The value and validity of the NRS and ODI have been reported.Citation65,Citation66 Recently, previously established thresholds were questioned.Citation67,Citation68 Thus, significant pain relief or improvement and function were considered to be at least a 50% reduction in NRS and the ODI, which is similar to the measurements in other trials.Citation38,Citation46,Citation47,Citation54–Citation62,Citation69–Citation71
The opioid intake was converted into morphine equivalents.Citation72
Assessment of employment and work status were determined based on employability at the time of enrollment. Thus, they were classified into multiple categories such as employable, housewife with no desire to work outside the home, retired, or over the age of 65. Patients who were unemployed due to pain, employed but on sick leave, or made redundant were considered as employable.
The epidurals were considered to be successful if a patient obtained significant improvement for at least 3 weeks with the first and second procedures. All others were considered to be failures.
Sample size
The sample size was calculated based on significant pain relief. Considering a 0.05 two-sided significance level, a power of 80%, and an allocation ratio of 1:1, 55 patients in each group were estimated.Citation73 Allowing for a 10% attrition/ non-compliance rate, 60 patients were required.
Randomization
Sixty patients were randomly assigned into each group from a total of 120 patients who met inclusion criteria.
Sequence generation
Simple randomization was utilized to allocate patients into groups.
Allocation concealment
Patients were randomized into two groups by one of the three operating room nurses who were also study coordinators. The same person also prepared the drugs.
Blinding (masking)
The patients and physician were blinded to group assignment and both injectates were clear. In addition, the blinding was ensured by mixing the study patients with other patients receiving routine treatment. All patients chosen for 1-year follow-up were selected by a statistician not participating in provision of the patients’ care and the unblinding results were not disclosed to either the treating physician, other participants, or patients. Thus, the nature of blinding was not interrupted.
Statistical methods
Data analyses were carried out using SPSS software (v 9.01; SPSS Inc, Chicago, IL). For categorical and continuous data comparison, Chi-square (Fisher test where necessary) and t-tests were used, respectively. Because the outcome measures of the participants were measured at four points in time, repeated measures analysis of variance were performed with the post hoc analysis.
Intent-to-treat analysis
Either the last follow-up data or initial data were utilized in the patients who dropped out of the study and no other data were available for the intent-to-treat analysis.
Best case, worst case, and last follow-up score scenarios were used for sensitivity analysis.
Results
Participant flow
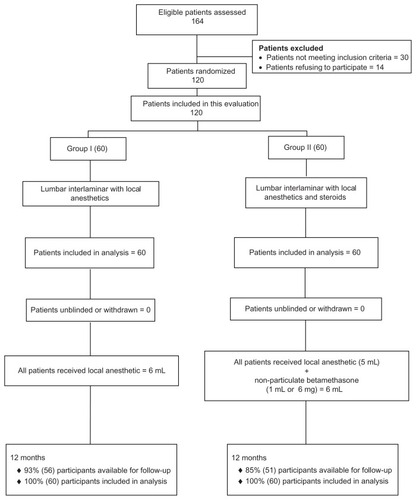
illustrates the participant flow. The recruitment period lasted from January 2008 through May 2010.
Figure 1 Schematic presentation of participant flow at 1-year follow-up of 60 patients.
Baseline data
shows the basic demographic characteristics, pain distribution, onset of the pain, numeric rating scale of pain, and ODI for functional status summary scores. There were no statistically significant differences between the two groups in terms of these baseline data (all P values > 0.05), except for weight (P = 0.000).
Table 1 Baseline demographic and clinical data
Pain relief and functional assessment
presents the results of repeated measures analysis. Regarding pain scores, there were significant differences within groups by time (P = 0.001). In the ODI for functional status, there were significant differences in summary scores within group by time (P = 0.001).
Table 2 Comparison of numeric rating scale for pain and Oswestry disability index score summaries at four time points
A post hoc analysis indicated that all the mean differences between baseline and with the scores at other time points were significant at the 0.05 level.
Pain relief and functional status improvement
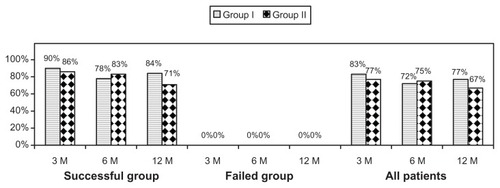
The percentage of patients with significant improvement is presented in . In Group I and II, 77% and 67% showed significant improvement, respectively. In the successful groups, significant improvement was seen in 84% in Group I and 71% in Group II.
Figure 2 Percentage of patients with a significant reduction in Numeric Rating Score and Oswestry disability index (≥50% reduction from baseline).
Therapeutic procedural characteristics
lists therapeutic procedural characteristics. Lumbar interlaminar procedures were performed in 91% of cases at L5/S1 and 9% of cases at L4/5.
Table 3 Therapeutic procedural characteristics with procedural frequency, average relief per procedure, and average total relief in weeks over a period of 1 year
Employment characteristics
lists employment characteristics in both groups. Among the patients eligible for employment, the total employed changed from 12 at baseline to 13 at the end of 12 months in Group I; it changed from 14 to 18 in Group II, a nonsignificant increase of 6% in Group I and 21% in Group II.
Table 4 Employment characteristics
Opioid intake
presents the results of repeated measures analysis for opioid intake. There were significant differences in opioid intake within group by time (P < 0.001). A post hoc analysis indicated that all the mean differences in scores between baseline and other time points were significant at the 0.05 level.
Table 5 Comparison of opioid intake (morphine equivalents in mg) summaries at four time points
Changes in weight
shows changes in weight, with no significant differences in changes among the groups.
Table 6 Characteristics of weight monitoring
Adverse events
Of the 454 lumbar epidural procedures performed, there were two subarachnoid punctures that did not result in headache. One patient experienced weight gain due to a high dose of steroid from an unrelated medical problem.
Discussion
This randomized, active control trial shows that carefully selected patients with axial or discogenic chronic low back pain can receive significant pain relief and functional status improvement with lumbar interlaminar epidural injections. Their pain was not caused by disc herniation, facet joints, or the sacroiliac joints. Significant pain relief and functional status improvement of ≥50% were seen in 77% of Group I and 67% of Group II. A better picture emerges when each group was divided into failed and successful outcomes. Significant pain relief and functional status improvement was seen in 84% of the successful outcomes in Group I; 71% in the successful outcomes in Group II. The average procedures per year and average weeks of total relief for the successful outcome patients were: Group I, 3.9 procedures and 40.0 ± 15.6 weeks; Group II, 4.0 procedures and 39.6 ± 12.4 weeks.
The results of this evaluation essentially illustrate that if patients are selected appropriately, lumbar epidural injections provide significant improvement. These results are in line with other studies separating the patients into failed and successful groups.Citation38,Citation46,Citation47,Citation54,Citation55,Citation58–Citation62 The results illustrate that both pain relief and improvement in functional status are clinically and statistically significant. Strict criteria were incorporated into the study and only participating patients judged not to have facet joint or sacroiliac joint pain were included, thus avoiding the criticism that including those with facet joint or sacroiliac joint pain in a study contributes to negative results. As confirmed in this report, epidural injections do not provide long-term relief. But, properly selected patients and appropriate procedures under fluoroscopy can provide long-term relief with judicious use.
Despite multiple publications, there is still significant debate regarding the medical necessity and indications for lumbar epidural injections, either by interlaminar approach, caudal approach, or transforaminal approach. Multiple systematic reviews, guidelines, and other reviews have identified weak indications for epidural injections, namely radicular pain from herniated lumbar intervertebral discs. However, there is a lack of evidence or recommended indications for other conditions. The preliminary report of the current manuscript showed positive results with interlaminar epidural injections.Citation39 Similarly, the previous results with caudal epidurals in appropriately selected patients were positive.Citation38
The results of this evaluation are similar to caudal epidural injections for axial or discogenic pain.Citation38 However, overall relief was superior in the present study, compared to the caudal study.Citation38 Steroids did not have any superiority over local anesthetic alone in either study.
There is a paucity of literature evaluating epidural injections for axial or discogenic pain. The role of caudal epidural injections for axial or discogenic pain, after ruling out facet joint pain or diagnosing it with provocation discography, was evaluated in three studies.Citation38,Citation74,Citation75 Only one studyCitation51 looked at lumbar interlaminar epidural injections other than the preliminary version of this study.Citation39 ButtermanCitation51 evaluated the role of interlaminar epidural steroids showing improvement only at the 3-month follow-up. All of the studies reported modest results.
The mechanism of action of steroids and local anesthetics continues to be debated. Multiple hypothesis have been emerging.Citation76–Citation84 The evidence shows that steroids, as well as local anesthetics, have significant effects on the modulation of noxious stimulation by various mechanisms. Long-term effects are provided by both local anesthetics and steroids or when in combination, in experimental as well as clinical studies.Citation38,Citation46,Citation47,Citation54–Citation56,Citation58–Citation61,Citation76–Citation84
Comparative effectiveness research and evidence-based medicine have been considered as pivotal to health care policy not only in the US, but across the world.Citation10,Citation11,Citation85–Citation89 In general, practical studies conducted in a generally applicable environment are considered more valuable than pragmatic or practical clinical trials with an active control group instead of a placebo group. Practical studies measure effectiveness, which is considered more appropriate than explanatory trials which measure efficacy.Citation90–Citation93 Thus, this study meets the criteria for a practical clinical trial, specifically in contemporary interventional pain management practices; it meets the appropriate selection criteria and repeats the procedures based upon the return of pain, rather than a predetermined schedule. The procedures were performed under fluoroscopy, only after conservative management had failed. The study also confirms the long-held belief that if the first two procedures do not provide at least a minimum of 3 weeks of relief, the procedures may not provide relief on a long-term basis. This was observed in the failed patients, suggesting that it may be futile to continue to repeat these procedures in these patients, unless there are compelling reasons to do so.
The present study may be criticized for not focusing on a placebo group. However, most studies have utilized inappropriate methodology with placebo groups with reference to interventional techniques.Citation88,Citation89,Citation94–Citation99 The only appropriately designed placebo trial by Ghahreman et alCitation99 showed a lack of significant effect when sodium chloride solution was injected into an inactive structure. Consequently, when sodium chloride solution or other agents such as local anesthetics, which are considered as placebo by some do not yield the same results, this leads to inaccurate methodology and conclusions.Citation100–Citation103
Some of the other weaknesses include differences in baseline demographic characteristics with respect to weight and sex; however, these differences were not considered to have caused any significant effect on the final results.
The implications of this trial are enormous in the health care arena. Studies with proper methodology in practical settings are not only crucial, but mandatory. Proper application of interventions will improve not only patients’ pain and function and reduce drug use, it may also return them to the workforce; however, by the same token, inappropriate provision of any type of intervention, specifically interventions with substantial expenses, will not provide any benefit. Instead, it can harm the patient, thus depleting resources and reducing access. Similarly, inappropriately performed evaluations in the name of methodology, leading to inaccurate conclusions, may reduce health care expenditures, and will also increase patient suffering and reduce function by impeding access to much needed medical care.
Conclusion
This study illustrates that overall significant improvement was seen in 77% of the patients in Group I and 67% of the patients in Group II. In the successful outcome groups, in those who received at least 3 weeks of relief with the first two procedures, the improvement was 84% in Group I and 71% in Group II. Pain relief and functional status improvement was achieved with an average procedures per year in the successful outcome groups of 3.9 in Group I and 4.0 in Group II, and an average total relief per year of 40.0 ± 15.6 weeks in Group I and 39.6 ± 12.4 in Group II.
Acknowledgments/ethics approval
Dr Manchikanti and Dr Benyamin designed the study; Mr Pampati performed the statistical analysis, and Ms Cash and Ms McManus were two of the three coordinators. The study was approved by the IRB and was registered in the US Clinical Trial Registry. All ethical guidelines were followed.
Disclosure
The authors report no conflicts of interest in this work.
References
- ManchikantiLPampatiVBoswellMVSmithHSHirschJAAnalysis of the growth of epidural injections and costs in the Medicare population: a comparative evaluation of 1997, 2002, and 2006 dataPain Physician201013319921220495584
- ManchikantiLBoswellMVSinghVASIPP-IPMComprehensive evidence-based guidelines for interventional techniques in the management of chronic spinal painPain Physician200912469980219644537
- StaalJBde BieRAde VetHCHildebrandtJNelemansPInjection therapy for subacute and chronic low back pain: an updated Cochrane reviewSpine (Phila Pa 1976)2009341495919127161
- ChouRHuffmanLGuideline for the Evaluation and Management of Low Back Pain: Evidence ReviewGlenview, ILAmerican Pain Society2009 Available at: http://www.ampainsoc.org/pub/pdf/LBPEvidRev.pdfAccessed on May 14, 2012
- ManchikantiLSinghVCarawayDLBenyaminRMHirschJAMedicare physician payment systems: impact of 2011 schedule on interventional pain managementPain Physician2011141E5E3321267048
- BogdukNChristophidisNCherryDEpidural use of steroids in the management of back painReport of working party on epidural use of steroids in the management of back painNational Health and Medical Research Council. Commonwealth of AustraliaCanberra1994176
- FriedlyJChanLDeyoRIncreases in lumbosacral injections in the Medicare population: 1994 to 2001Spine (Phila Pa 1976)200732161754176017632396
- ManchikantiLPampatiVSinghVBoswellMVSmithHSHirschJAExplosive growth of facet joint interventions in the Medicare population in the United States: a comparative evaluation of 1997, 2002, and 2006 dataBMC Health Serv Res2010108420353602
- ManchikantiLSinghVHirschJASaga of payment systems of ambulatory surgery centers for interventional techniques: an updatePain Physician201215210913022430649
- ManchikantiLDattaSDerbyRWolferLRBenyaminRMHirschJAA critical review of the American Pain Society clinical practice guidelines for interventional techniques: part 1. Diagnostic interventionsPain Physician2010133E141E17420495596
- ManchikantiLDattaSGuptaSA critical review of the American Pain Society clinical practice guidelines for interventional techniques: part 2. Therapeutic interventionsPain Physician2010134E215E26420648212
- AbbottZINairKVAllenRRAkuthotaVRUtilization characteristics of spinal interventionsSpine J2012121354322138113
- WheelerAHMurreyDBChronic lumbar spine and radicular pain: pathophysiology and treatmentCurr Pain Headache Rep2002629710511872180
- HadjipavlouAGTzermiadianosMNBogdukNZindrickMRThe pathophysiology of disc degeneration: a critical reviewJ Bone Joint Surg Br200890101261127018827232
- McCarronRFWimpeeMWHudkinsPGLarosGSThe inflammatory effects of nucleus pulposus: a possible element in the pathogenesis of low back painSpine (Phila Pa 1976)19871287607642961088
- OlmarkerKNordborgCLarssonKRydevikBUltrastructural changes in spinal nerve roots induced by autologous nucleus pulposusSpine (Phila Pa 1976)19962144114148658242
- MixterWJBarrJSRupture of the intervertebral disc with involvement of the spinal canalN Eng J Med1934211210215
- MixterWJAyersJBHerniation or rupture of the intervertebral disc into the spinal canalN Engl J Med1935213385395
- ManchikantiLBoswellMVSinghVASIPPComprehensive review of neurophysiologic basis and diagnostic interventions in managing chronic spinal painPain Physician2009124E71E12019668292
- HancockMJMaherCGLatimerJSystematic review of tests to identify the disc, SIJ or facet joint as the source of low back painEur Spine J200716101539155017566796
- PengBWuWHouSThe pathogenesis of discogenic low back painJ Bone Joint Surg20058716267
- MiyagiMIshikawaTOritaSDisk injury in rats produces persistent increases in pain-related neuropeptides in dorsal root ganglia and spinal cord glia but only transient increases in inflammatory mediators: pathomechanism of chronic diskogenic low back painSpine (Phila Pa 1976)201136262260226621228748
- CoppesMHMaraniEThomeerRTGroenGJInnervation of “painful” lumbar discsSpine (Phila Pa 1976)19972220234223499355214
- FreemontAJPeacockTEGoupillePHoylandJAO’BrienJJaysonMINerve ingrowth into diseased intervertebral disc in chronic back painLancet199735090721781819250186
- EdgarMAThe nerve supply of the lumbar intervertebral discJ Bone Joint Surg200789911351139
- OzawaTOhtoriSInoueGAokiYMoriyaHTakahashiKThe degenerated lumbar intervertebral disc is innervated primarily by peptide-containing sensory nerve fibers in humansSpine (Phila Pa 1976)200631212418242217023849
- AokiYOhtoriSInoHDisc inflammation potentially promotes axonal regeneration of dorsal root ganglion neurons innervating lumbar intervertebral disc in ratsSpine (Phila Pa 1976)200429232621262615564910
- HayashiYOhtoriSYamashitaMDirect single injection of p38 mitogen-activated protein kinase inhibitor does not affect calcitonin gene-related peptide expression in dorsal root ganglion neurons innervating punctured discs in ratsSpine (Phila Pa 1976)2009242622952299
- HelmSHayekSMBenyaminRMManchikantiLSystematic review of the effectiveness of thermal annular procedures in treating discogenic low back painPain Physician200912120723219165305
- BlondelBTropianoPGuadartJHuangRCMarnayTClinical results of lumbar total disc arthroplasty in accordance with Modic signs, with a 2-year-minimum follow-upSpine (Phila Pa 1976)201136262309231521252824
- OhWSShimJCA randomized controlled trial of radiofrequency denervation of the ramus communicans nerve for chronic discogenic low back painClin J Pain2004201556014668658
- TsouPMYeungCAYeungATPosterolateral transforaminal selective endoscopic discectomy and thermal annuloplasty for chronic lumbar discogenic pain: a minimal access visualized intradiscal surgical procedureSpine J20044556457315363430
- PengBPangXZhaoCSongXA randomized placebo-controlled trial of intradiscal methylene blue injection for the treatment of chronic discogenic low back painPain2010149112412920167430
- OhtoriSKinoshitaTYamashitaMResults of surgery for discogenic low back pain: A randomized study using discography versus discoblock for diagnosisSpine (Phila Pa 1976)200934131345134819440168
- OhtoriSKoshiTYamashitaMSurgical versus nonsurgical treatment of selected patients with discogenic low back pain: a small-sized randomized trialSpine (Phila Pa 1976)201136534735420838371
- MadanSGundannaMHarleyJMBoereeNRSampsonMDoes provocative discography screening of discogenic back pain improve surgical outcome?J Spinal Disord Tech200215324525112131428
- Maghout-JuratliSFranklinGMMirzaSKWickizerTMFulton-KohoeDLumbar fusion outcomes in Washington state workers’ compensationSpine (Phila Pa 1976)200631232715272317077741
- ManchikantiLCashKAMcManusCDPampatiVSmithHSOne year results of a randomized, double-blind, active controlled trial of fluoroscopic caudal epidural injections with or without steroids in managing chronic discogenic low back pain without disc herniation or radiculitisPain Physician2011141253621267039
- ManchikantiLCashKAMcManusCDPampatiVBenyaminRMPreliminary results of a randomized, double-blind, controlled trial of fluoroscopic lumbar interlaminar epidural injections in managing chronic lumbar discogenic pain without disc herniation or radiculitisPain Physician2010134E279E29220648214
- VallejoRManuel ZevallosLLoweJBenyaminRIs spinal cord stimulation an effective treatment option for discogenic pain?Pain Pract201212319420121797964
- SchwarzerACAprillCNDerbyRFortinJKineGBogdukNThe relative contributions of the disc and zygapophyseal joint in chronic low back painSpine (Phila Pa 1976)19941978018068202798
- ManchikantiLSinghVPampatiVEvaluation of the relative contributions of various structures in chronic low back painPain Physician20014430831616902676
- DattaSLeeMFalcoFJEBryceDAHayekSMSystematic assessment of diagnostic accuracy and therapeutic utility of lumbar facet joint interventionsPain Physician200912243746019305489
- RupertMPLeeMManchikantiLDattaSCohenSPEvaluation of sacroiliac joint interventions: a systematic appraisal of the literaturePain Physician200912239941819305487
- ParrATDiwanSAbdiSLumbar interlaminar epidural injections in managing chronic low back and lower extremity pain: a systematic reviewPain Physician200912116318819165302
- ManchikantiLSinghVFalcoFJECashKAPampatiVEvaluation of the effectiveness of lumbar interlaminar epidural injections in managing chronic pain of lumbar disc herniation or radiculitis: a randomized, double-blind, controlled trialPain Physician201013434335520648203
- ManchikantiLCashKAMcManusCDDamronKSPampatiVFalcoFJELumbar interlaminar epidural injections in central spinal stenosis: preliminary results of a randomized, double-blind, active control trialPain Physician2012151516322270738
- AckermanWE3rdAhmadMThe efficacy of lumbar epidural steroid injections in patients with lumbar disc herniationsAnesth Analg200710451217122217456677
- CandidoKDRaghavendraMSChinthagadaMBadieeSTrepashkoDWA prospective evaluation of iodinated contrast flow patterns with fluoroscopically guided lumbar epidural steroid injections: the lateral parasagittal interlaminar epidural approach versus the transforaminal epidural approachAnesth Analg2008106263864418227326
- GhariboCVarlottaGRhameELiuECJBendoJPerloffMInterlaminar versus transforaminal epidural steroids for the treatment of sub-acute lumbar radicular pain: a randomized, blinded, prospective outcome studyPain Physician201114649951122086091
- ButtermanGRThe effect of spinal steroid injections for degenerative disc diseaseSpine J20044549550515363419
- AmrYMEffect of addition of epidural ketamine to steroid in lumbar radiculitis: one-year follow-upPain Physician201114547548121927052
- RadosISakicKFinglerMKapuralLEfficacy of interlaminar vs transforaminal epidural steroid injection for the treatment of chronic unilateral radicular pain: prospective, randomized studyPain Med20111291316132121914118
- ManchikantiLSinghVCashKAPampatiVDamronKSBoswellMVA randomized, controlled, double-blind trial of fluoroscopic caudal epidural injections in the treatment of lumbar disc herniation and radiculitisSpine (Phila Pa 1976)201136231897190521897343
- ManchikantiLSinghVCashKAPampatiVDattaSManagement of pain of post lumbar surgery syndrome: one-year results of a randomized, double double-blind, active controlled trial of fluoroscopic caudal epidural injectionsPain Physician201013650952121102963
- ManchikantiLCashRAMcManusCDPampatiVFellowsBFluoroscopic caudal epidural injections with or without steroids in managing pain of lumbar spinal stenosis: One year results of randomized, double-blind, active-controlled trialJ Spinal Disord201225226234
- DashfieldAKTaylorMBCleaverJSFarrowDComparison of caudal steroid epidural with targeted steroid placement during spinal endoscopy for chronic sciatica: a prospective, randomized, double-blind trialBr J Anaesth200594451455915695544
- ManchikantiLCashKAPampatiVWargoBWMallaYCervical epidural injections in chronic discogenic neck pain without disc herniation or radiculitis: preliminary results of a randomized, double-blind, controlled trialPain Physician2010134E265E27820648213
- ManchikantiLCashKAPampatiVWargoBWMallaYThe effectiveness of fluoroscopic cervical interlaminar epidural injections in managing chronic cervical disc herniation and radiculitis: preliminary results of a randomized, double-blind, controlled trialPain Physician201013322323620495586
- ManchikantiLMallaYCashKAMcManusCDPampatiVFluoroscopic epidural injections in cervical spinal stenosis: preliminary results of a randomized, double-blind, active control trialPain Physician2012151E59E7022270749
- ManchikantiLMallaYCashKAMcManusCDPampatiVFluoroscopic cervical interlaminar epidural injections in managing chronic pain of cervical post-surgery syndrome: preliminary results of a randomized, double-blind active control trialPain Physician2012151132622270734
- ManchikantiLCashKAMcManusCDPampatiVBenyaminRMA preliminary report of a randomized double-blind, active controlled trial of fluoroscopic thoracic interlaminar epidural injections in managing chronic thoracic painPain Physician2010136E357E36921102973
- AltmanDGSchulzKFMoherDCONSORT GROUPThe revised CONSORT statement for reporting randomized trials: explanation and elaborationAnn Intern Med2001134866369411304107
- ManchukondaRManchikantiKNCashKAPampatiVManchikantiLFacet joint pain in chronic spinal pain: an evaluation of prevalence and false-positive rate of diagnostic blocksJ Spinal Disord Tech200720753954517912133
- ManchikantiLHirschJASmithHSEvidence-based medicine, systematic reviews, and guidelines in interventional pain management: part 2: Randomized controlled trialsPain Physician200811671777319057624
- FairbankJCTPynsentPBThe Oswestry Disability IndexSpine (Phila Pa 1976)200025222940295311074683
- CarrageeEJThe rise and fall of the “minimum clinically important difference”Spine J201010428328420362245
- CarrageeEJChenIMinimum acceptable outcomes after lumbar spinal fusionSpine J201010431332020362247
- ManchikantiLSinghVFalcoFJECashKAPampatiVEvaluation of lumbar facet joint nerve blocks in managing chronic low back pain: a randomized, double-blind, controlled trial with a 2-year follow-upInt J Med Sci20107312413520567613
- ManchikantiLSinghVFalcoFJECashKAPampatiVFellowsBComparative effectiveness of a one-year follow-up of thoracic medial branch blocks in management of chronic thoracic pain: a randomized, double-blind active controlled trialPain Physician201013653554821102966
- ManchikantiLSinghVFalcoFJCashKAFellowsBComparative outcomes of a 2-year follow-up of cervical medial branch blocks in management of chronic neck pain: a randomized, double-blind controlled trialPain Physician201013543745020859313
- PereiraJLawlorPViganoADorganMBrueraEEquianalgesic dose ratios for opioids. A critical review and proposals for long-term dosingJ Pain Symptom Manage2001222672687 Narcotic analgesic converterGlobalRPh Inc http://www.globalrph.com/narcotic.cgi
- BrownerWSNewmanTBCummingsSRHulleySBEstimating sample size and powerHulleySBCummingsSRBrownerWSGradyDHearstNNewmanTBDesigning Clinical Research: An Epidemiologic Approach2nd edPhiladelphia, PALippincott, Williams and Wilkins20016584
- ManchikantiLSinghVRiveraJJEffectiveness of caudal epidural injections in discogram positive and negative chronic low back painPain Physician200251182916896354
- ManchikantiLPampatiVRiveraJJBeyerCDDamronKSBarnhillRCCaudal epidural injections with Sarapin or steroids in chronic low back painPain Physician20014432233516902678
- ByrodGOtaniKBrisbyHRydevikBOlmarkerKMethylprednisolone reduces the early vascular permeability increase in spinal nerve roots induced by epidural nucleus pulposus applicationJ Orthop Res200018698398711192260
- HayashiNWeinsteinJNMellerSTLeeHMSprattKFGebhartGFThe effect of epidural injection of betamethasone or bupivacaine in a rat model of lumbar radiculopathySpine (Phila Pa 1976)19982388778859580954
- LeeHMWeinsteinJNMellerSTHayashiNSprattKFGebhartGFThe role of steroids and their effects on phospholipase A2: an animal model of radiculopathySpine (Phila Pa 1976)19982311119111969636970
- MinamideATamakiTHashizumeHYoshidaMKawakamiMHayashiNEffects of steroids and lipopolysaccharide on spontaneous resorption of herniated intervertebral discs: an experimental study in the rabbitSpine (Phila Pa 1976)19982388708769580953
- PasqualucciAVarrassiGBraschiAEpidural local anesthetic plus corticosteroid for the treatment of cervical brachial radicular pain: single injection verus continuous infusionClin J Pain200723755155717710003
- MaoJChenLLSystemic lidocaine for neuropathic pain reliefPain200087171710863041
- PasqualucciAExperimental and clinical studies about the preemptive analgesia with local anesthetics. Possible reasons of the failureMinerva Anestesiol199864104454579857627
- TachiharaHSekiguchiMKikuchiSKonnoSDo corticosteroids produce additional benefit in nerve root infiltration for lumbar disc herniationSpine (Phila Pa 1976)200833774374718379400
- SatoCSakaiAIkedaYSuzukiHSakamotoAThe prolonged analgesic effect of epidural ropivacaine in a rat model of neuropathic painAnesth Analg2008106131332018165597
- ManchikantiLFalcoFJEBoswellMVHirschJAFacts, fallacies, and politics of comparative effectiveness research: part 2. Implications for interventional pain managementPain Physician2010131E55E7920119475
- ManchikantiLFalcoFJBenyaminRMHelmS2ndParrATHirschJAThe impact of comparative effectiveness research on interventional pain management: Evolution from Medicare Modernization Act to Patient Protection and Affordable Care Act and the Patient-Centered Outcomes Research InstitutePain Physician2011143E249E28221587337
- ManchikantiLFalcoFJEBoswellMVHirschJAFacts, fallacies, and politics of comparative effectiveness research: part 1. Basic considerationsPain Physician2010131E23E5420119474
- ChouRAtlasSJLoeserJDRosenquistRWStanosSPGuideline warfare over interventional therapies for low back pain: can we raise the level of discourse?J Pain201112883383921742563
- ManchikantiLBenyaminRMFalcoFJECarawayDLDattaSHirschJAGuidelines warfare over interventional techniques: Is there a lack of discourse or straw man?Pain Physician2012151E1E2622270745
- HotopfMThe pragmatic randomized controlled trialAdv Psychiatr Treat20028326333
- TunisSRStryerDBClancyCMPractical clinical trials. Increasing the value of clinical research for decision making in clinical and health policyJAMA2003290121624163214506122
- RolandMTorgersonDJWhat are pragmatic trials?BMJ199831671272859472515
- International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human UseICH Harmonised Tripartite GuidelineChoice of Control Group and Related Issues in Clinical TrialsE107202000
- IversenTSolbergTRomnerBEffect of caudal epidural steroid or saline injection in chronic lumbar radiculopathy: multicentre, blinded, randomised controlled trialBMJ2011343d527821914755
- CaretteSLeclaireRMarcouxSEpidural corticosteroid injections for sciatica due to herniated nucleus pulposusN Engl J Med199733623163416409171065
- KarppinenJMalmivaaraAKurunlahtiMPeriradicular infiltration for sciatica: a randomized controlled trialSpine (Phila Pa 1976)20012691059106711337625
- ManchikantiLGiordanoJFellowsBHirschJAPlacebo and nocebo in interventional pain management: a friend or a foe – or simply foes?Pain Physician2011142E157E17521412379
- SmuckMLevinJHRE: Manchikanti L, et al. Cervical medial branch blocks for chronic cervical facet joint pain: A randomized double-blind, controlled trial with one-year follow-up. Spine (Phila Pa 1976). 2008;33(17):1813–1820Spine (Phila PA 1976)200934101116111719404184
- GhahremanAFerchRBogdukNThe efficacy of transforaminal injection of steroids for the treatment of lumbar radicular painPain Med20101181149116820704666
- IndahlAKaigleAMReikeräsOHolmSHInteraction between the porcine lumbar intervertebral disc, zygapophysial joints, and paraspinal musclesSpine (Phila Pa 1976)19972224283428409431619
- IndahlAKaigleAReikeräsOHolmSElectromyographic response of the porcine multifidus musculature after nerve stimulationSpine (Phila Pa 1976)19952024265226588747243
- Pham DangCLelongAGuilleyJEffect on neurostimulation of injectates used for perineural space expansion before placement of a stimulating catheter: normal saline versus dextrose 5% in waterReg Anesth Pain Med200934539840319920414
- TsuiBCKropelinBGanapathySFinucaneBDextrose 5% in water: fluid medium maintaining electrical stimulation of peripheral nerve during stimulating catheter placementActa Anaesthesiol Scand200549101562156516223407