
Abstract
Chronic pain is a significant and costly problem all over the world that negatively impacts the quality of life of sufferers. There are clear discrepancies between the prevalence of chronic pain in society and the low priority assigned to educating future physicians about the complexities of pain. This condition also occurs in other undergraduate health science students, although research in this area has not been studied as much as in medical schools. Based on the International Association for the Study of Pain (IASP) Pain Curriculum Outline, a systematic search of the available literature, and the authors’ own experiences, we highlight some relevant tips to educate health science trainees in the management of patients with chronic pain. These tips highlight current international recommendations for a comprehensive approach to this prevalent problem in society, which should be learnt during the university training of health professionals.
Video Abstract

Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Chronic pain is defined as pain that persists or recurs for longer than three months and negatively affects the quality of life of sufferers.Citation1
Currently, chronic pain is a significant global health problem that affects one in five European adults, representing 96 million afflicted people.Citation2 Its prevalence has been reported as 37.3% and 41.1% of the population in developed and developing countries, respectively, generating elevated social and economic costs (direct and indirect) for individuals and society.Citation3
Therefore, university and professional education on pain management should be a priority.Citation4 However, the International Association for the Study of Pain (IASP) reported that pain education in universities among health science students in many countries is alarmingly inadequate.Citation5 In a famous editorial, Loeser, a founding member of the IASP, described the
inadequate education of primary care providers about pain and how to treat it (p.111)
as one of five major crises in pain management.Citation6
The teaching of pain-related topics in medical schools throughout the world seems to be limited, fragmented, and variable.Citation7 Chronic pain is often relegated to brief lectures or seminars, and the time spent on this topic is generally low.Citation8 For example, in the UK, Shipton et al wrote that the median time spent on pain management by a medical student is 13 hours and sometimes as little as 6 hours.Citation9 This can create a potential social risk, since poor pain training will have a negative effect on the quality of future care for patients with this condition.Citation10 This educational and curricular lack, although to a lesser extent, has also been investigated in students of other health science degrees, especially in United States (EEUU), Canada, and the United Kingdom.Citation11,Citation12 These studies recognized that documented pain education in curricula is limited and fragmentary. Moreover, some of these identify different approaches that could be “successful”, related to pain education, across a range of health disciplines.Citation13,Citation14
On the other hand, chronic non-cancer pain has not been considered a priority within healthcare systems despite its consequences, as it is generally regarded as a symptom.Citation15 It lacks specific coding in the current version of the International Classification of Diseases (ICD-10). Fortunately, this will change soon since the new ICD revision will incorporate a chapter on all pain diagnostic codes, which represents a great step in the recognition of chronic pain as a public health problem.Citation1 In May 2019, the World Health Organisation (WHO) Assembly agreed to adopt ICD-11, which will come into effect in 2022.Citation16
This change should be quickly introduced in university pain education programmes to raise awareness among students and to emphasise the multidimensionality of the pain experience, highlighting the need for interdisciplinary collaboration to treat individuals with chronic pain.Citation5
Carr & Bradshaw declared the need to change the approach of the standard pain curriculum in university programmes, emphasising interpersonal, emotional, and social aspects rather than cellular processes, or shifting the paradigm from biopsychosocial to sociopsychobiological.Citation17
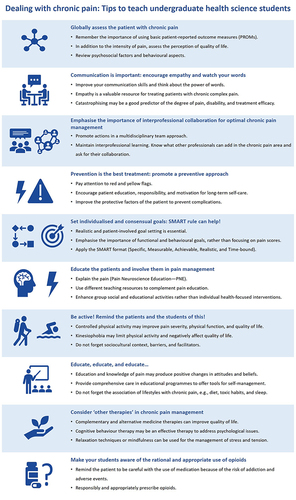
Therefore, based on the IASP Pain Curriculum outline, our expertise and after carrying out a systematic review of the existing literature, we want to highlight 10 practical tips about chronic pain management that should be addressed in university programmes and taught to undergraduate health science students, who, as future health professionals, will have to deal with this prevalent and challenging condition.
Materials and Methods
Search Strategy and Study Selection Criteria
In order to get information to write the results, the bibliographic search was carried out between January 2021 and July 2021 in the PubMed/MEDLINE electronic database. In this review we searched among electronic and manual documents covering a 22-yr period, between 2000 and 2021. Search terms included combinations of the following MeSH keywords in the title/abstract fields: “pain management” and “chronic pain” and “curriculum” or “medical education” or “health sciences” and “students” or “undergraduate”. All types of studies were included in this review such as systematic review, randomized trials, descriptive and analytic studies, review articles, guidelines and protocols. Non-English publications were excluded.
The search identified 1137 documents. After that, under the focus of chronic pain management by undergraduate health science students, results were evaluated to look for topics related to treatment of chronic pain education by the 1st and 2nd authors, independently, based on the information provided on the titles, abstracts, and MeSH terms (). All the discrepancies between reviewers were discussed and resolved, subsequently.
Box 1 Checklist of Topics in Chronic Pain Education
A selection of topics on chronic pain management was elaborated, using the IASP pain curriculum outline and the experience of the authors. shows a list summarizing these terms.
Figure 1 Check list of specific points to improve chronic pain education in undergraduate health science students.
Finally, 171 articles were obtained, of which 68 articles were selected to make targeted recommendations based on the major gaps on education chronic pain. Therefore, the approach presented here focuses on the main areas to improve the training of undergraduate health science students in the management of patients with chronic pain. A list summarising and a descriptive section is offered for each area ().
Results and Discussion
Globally Assess the Patient with Chronic Pain
Patients with chronic pain require a holistic assessment, including information about the intensity and quality of pain, psychological, and behavioural aspects, as well as the sociocultural context where patients interact.Citation18
Students should learn to use basic patient-reported outcome measures (PROMs) for pain assessment and to analyse the results derived from these tools. The interpretation of their scores can help plan an early intervention and propose the incorporation of other members of a multidisciplinary team for pain management.Citation19
In addition to the intensity or quality of pain, other related factors with the pain experience, such as the psychosocial factors (depression, mood, anxiety), fear of movement (kinesiophobia) and catastrophisation, should be assessed using PROMs because they are important prognostic factors correlated with disability and a decrease in the perception of the quality of life.Citation20
Clinical training and the incorporation of clinical simulation activities in faculties of health sciences are excellent training for students to develop skills related to the clinical interview, assessment, and the use of standardised PROMs.Citation21
Another relevant aspect is to encourage students to pay attention to “red and yellow flags.” For patients with chronic pain, the use of the “red flags” system can be helpful to detect serious underlying conditions and to determine if additional investigation is warranted, although their use in isolation is not recommended.Citation22 The most usual and useful red flags are a previous history of malignancies or cancer, weight loss, increased pain at night or continuous pain at rest, drug addiction, and severe or progressive neurological deficit, among others.
However, yellow flags are clinical indicators that warn about psychosocial factors that may contribute to long-term distress, disability, and chronic pain.Citation23 Some examples of frequently observed yellow flags are sickness behaviours, tendencies towards low moods and withdrawal from social interaction, fear-avoidant behaviour, and reduced activity levels.
In the future, students should be able to detect both situations when treating a patient with chronic non-cancer pain. For this reason, university training programmes should emphasise simulated activities that allow them to transfer these experiences to real practice. For undergraduate health science students, learning experiences to identify red flags in a relevant clinical problem in a simulated practice context have been reported as positive.Citation24
Communication is Important: Encourage Empathy and Watch Your Words
Good communication skills are essential for clinicians, and health science students need special training in this when treating chronic pain patients.Citation25 Clinicians and health science students should train and use effective communication skills to reinforce positive health behaviours and the internal locus of control in patients.Citation26 Empathy is valuable for clinicians who treat patients with chronic complex pain. Indeed, a highly empathic clinician may bring a more balanced approach to the treatment of patients with chronic pain.Citation27 Therefore, it is important to train health science students in a patient-centred approach and empathic communication to improve the quality of attention to patients who suffer from this condition.
Clinicians and undergraduate health science students will likely remain unaware of the potential harm that their words may cause. They need to talk about the real possibilities of therapy and pathoanatomical features in a way that patients can understand, mainly avoiding terms that can induce catastrophism. Catastrophizing is a large field of study in chronic pain, and it has been identified as a predictor of the degree of pain, disability, and treatment efficacy in most studies.Citation28 The findings suggest that specific subset of chronic pain patients with a high level of catastrophising tend to magnify the threat value of pain, develop feelings of helplessness, and have a higher risk for prescription opioid misuse or even with suicide risk.Citation29,Citation30 Remember the power of words and that they can elicit emotions and prompt actions that can lead to positive or negative behavioural change. Knowing the influence and consequences that language can have on the management of chronic pain is of paramount importance.Citation31
Emphasise the Importance of Interprofessional Collaboration for Optimal Chronic Pain Management
Considering the complexity of chronic pain, different disciplines must be involved in its assessment and management. In this case, a multidisciplinary team approach is considered the optimal therapeutic paradigm for most adult chronic pain sufferers.Citation32 For it, so-called interprofessional learning (IPL), based on the interaction of members of more than one profession learning together to improve patient therapeutic outcomes, is essential to properly educate undergraduate health science students. When IPL is appropriately applied, the comprehensive multidisciplinary management of chronic pain has repeatedly been shown to be a clinically effective and cost-efficient alternative to single-discipline treatment or usual care.Citation33
However, despite the known benefits, the incorporation of IPL in university curricula is limited, and collaborative practice is not yet an integral part of all health education programmes.Citation34 Therefore, future professionals in health sciences should be guided to promote interdisciplinary meetings on the treatment of these patients, both in the hospital and primary care. In both cases, it will be important that all members know what other professionals can contribute. Moreover, all professionals must be aware of the information and care that the patient should receive and of how to manage or guide the patient. Kassutto et al and Boet et al proposed interesting tips for creating IPL opportunities with medical students at university based on collaborative practice in real and simulated healthcare settings. In these multidisciplinary teams, different subspecialties of physicians (primary care, surgeons, neurologists, anesthetists, etc.) and other health care specialties (physiotherapy, nursing, psychology, and social workers, among others) should be included.Citation35,Citation36
Prevention is the Best Treatment: Promote a Preventive Approach
Despite the serious consequences of chronic pain, efforts to prevent chronic non-cancer pain are significantly less than those carried out in other conditions.Citation37 Clinical practice guidelines usually focus on specific clinical conditions and the prescription of opioids.Citation38 This high dependence on pharmacological treatment shows, in part, the failure of the chronic pain prevention model in primary care.
An approach that encourages patient responsibility and motivation for long-term self-care, as well as education to improve protective factors, is key to preventing complications in chronic pain.Citation39
The incorporation of cross-cutting activities in health undergraduate degrees will allow students to improve their ability to assess the progression of acute to chronic pain and from chronic to intractable pain. As mentioned, the knowledge and identification of the yellow flags as predictors of long-term disability are considered essential for early intervention for vulnerable people.Citation19
Set Individualised and Consensual Goals: SMART Rule Can Help!
Realistic goal setting is essential in patients with chronic pain. Patients and clinicians can prioritise different management goals for chronic pain. Therefore, asking people to nominate their goals and involve patients in goal setting is very relevant.Citation40 Moreover, rather than focusing on a pain score, it may be more beneficial to emphasise the importance of functional and behavioural goals.Citation41
Applying the Specific, Measurable, Achievable, Realistic, and Time-bound (SMART) format to patient goals is a good and easy starting point to increase the chances of achieving a positive outcome.Citation42 Therefore, it is very important to train students in goal setting.
To achieve an optimal result, consider the following aspects: avoid abstract sentences, be as specific as possible so there is no misunderstanding, and use replace them with more specific functional goals. The goal must be reasonable, based on the patient’s current health status and limitations. By ensuring that each goal is achievable, the likelihood of success can increase. One goal may be that all patients with chronic pain end up knowing and having information about the causes of their pain. In undergraduate health science students, promoting the creation of infographics or videos that explain the chronic pain process and the main ways to fight it can be an interesting learning tool.
Then, some specific parameters are set to make the goal measurable and consider the relevance of the planned goals for the patient. Setting unrealistic goals makes the situation worse. Finally, put a frame on each goal. This is important, as it encourages the patient to track their progress and not just their pain. In this case, the final person-centred goals might sound like this:
be able to walk 2 kilometres at a good pace without stopping in 2 months, completing this with minimal pain (<3/10), to go out with my friends again for a walk and recover part of my social activity.
Educate the Patients and Involve Them in Pain Management
“Explain the pain” is important for changing the understanding of the biological processes that underpin pain. For this purpose, Pain Neuroscience Education (PNE) uses the current understanding of neuroscience to help reconceptualise the experience of pain.Citation43,Citation44 Translating this for the targeted culture is also important. In fact, PNE has become key to the successful management of chronic pain. When it is combined with other pain interventions, this approach has been associated with health-related cost reduction.Citation45,Citation46 Furthermore, PNE has demonstrated a positive effect on kinesiophobia, pain intensity, disability, or catastrophising, which are predictors of negative clinical evolution in chronic pain patients.Citation47
Therefore, it is essential to Training health science students in teach this patient-centred therapeutic approach is essential for improving care of future patients. The focus of such educational interventions is the understanding of the biological processes that are thought to underpin pain as a mechanism for reducing pain itself. A combination of different teaching resources to complement in-person pain education can be used, such as prepared pictures, presentation slides, drawings, infographics, metaphors, and books.Citation48 Research demonstrates that education, as part of multidisciplinary programmes, is likely to improve self-management and self-efficacy in people with chronic pain.Citation49
When educating patients is a goal, research indicates that the most effective health promotional programmes for adults are social and educational group activities rather than individual health-focused interventions.Citation50,Citation51 Educational group actions can help improve aspects such as differences in coping strategies illness perceptions, self-efficacy, fear-avoidant beliefs, locus of control, and pain attitudes in different populations. However, when these actions are carried out, ethnic and cultural patient characteristics should be considered because these affect the pain beliefs, cognitions, and behaviours in those with chronic pain.Citation52
Be Active! Remind the Patients and the Students of This!
Given that physical activity can influence the experience of pain, a relevant aspect of self-managing pain is that the patient remains physically active, avoiding prolonged sedentary behaviour that leads to greater disability.Citation53
“Physical activity on prescription” in patients with chronic pain may improve pain severity, physical function, and consequently quality of life, with few adverse events.Citation54 Therefore, it is essential to teach health science students the importance of considering exercise in their prescriptions for chronic pain. It is also important to know the role of physiotherapists in this area and to maintain a relationship of trust and continuous dialogue with them to achieve the best results.Citation55
It is essential to consider the patients’ circumstances, context, symptoms, preferences, and current activity level when prescribing physical activity and therapeutic exercise because some patients need extra support to overcome barriers.Citation56
Everything possible must be done to avoid or reduce kinesiophobia, which is a frequently related condition in patients with chronic pain that limits their physical activity and negatively affects their quality of life.Citation57
Educate, Educate, and Educate …
Therapists must provide educative and comprehensive care in educational programmes to offer tools to patients for the self-management of chronic pain.Citation58 Pain education for various healthcare providers has been associated with significant improvements in the knowledge of pain and with positive changes in attitudes and beliefs regarding persistent pain.Citation59
Due to the association of lifestyles with chronic pain, healthcare professionals should educate patients on some factors that potentially affect the pain experience.Citation60 For example, reducing and avoiding toxic habits (smoking and alcohol intake), highlighting the importance and the positive effect of whole-food diets on pain,Citation61 and explaining the intrinsic relationship between pain and sleep.Citation62
Consider “Other Therapies” in Chronic Pain Management
Complementary and alternative medicine therapies can improve the quality of life in patients with chronic pain.Citation63 Although these therapies are not widely accepted, there is an increasing demand for them by patients. Practitioners are beginning to realise the importance of understanding their benefits, and they have even been offered in medical schools.Citation64 Techniques such as acupuncture, biofeedback, massage, and osteopathic and spinal manipulation can be considered complementary treatments for chronic pain, and they are already a reality in many chronic pain units.
Regarding behavioural therapies, cognitive behaviour therapy, which replaces maladaptive thoughts, may be an effective therapy for addressing psychological concerns in patients with chronic pain.Citation65 In addition, relaxation or mindfulness techniques can be useful for the management of stress and tension generated by pain in the long term, but the research is not overwhelming, and follow-up data suggests that its usefulness is reduced over time.
As a result, it is advisable to include information in the curricular training programmes so that students can be clear about what these techniques can actually achieve and refer patients to treatment-specific units.Citation66
Make Your Students Aware of the Rational and Appropriate Use of Opioids
Opioids are useful and powerful medications for treating pain, although their use is not exempt from the risk of addiction and adverse events.Citation15 Currently, the United States of America suffers a crisis caused by a dramatic increase in the chronic use of opioid therapy, and its misuse and abuse has become a first-order problem.Citation67
Tobin et al found an unmet learning need in undergraduate training on opioid use disorder,Citation68 and Singh & Pushkin described how
currently, medical education about the ethical dimensions of opioid prescribing lacks clarity, consistency and structure (p. 640).Citation69
Therefore, it is important to improve awareness and opioid-related education to address the knowledge gaps reported by students.Citation70 Academic sessions and implementing curricula on responsible opioid prescribing should be interactive and case-based, while offering clinical pearls.Citation15 Pedagogical methods recommended for this purpose include the use of standardised patients, team-based learning exercises, internet-based modules, and lectures followed by an objective structured clinical examination.Citation71
Conclusion
Chronic pain is a major public health problem, a silent epidemic that needs, among other things, improvements in health science education and an alteration in how pain education is integrated into the regular university curricula. The literature highlights the importance of teamwork through communication, patient education as well as the patient involvement in pain management. It also emphasizes the importance of goal setting, the promotion of physical activity as a way to reduce pain, the avoidance of opioid use and, above all, the prevention by identifying those patients with a higher risk of suffering from of chronic pain.
By improving knowledge, attitudes, and skills in pain management in our universities, we can contribute to the training of future professionals sensitised to this condition, which will be transferred to their future work with patients. We forget that part of the change starts in the classrooms of our faculties, and we have the responsibility to promote it. Let us be consistent with current evidence and promote a modern approach that improves care for patients with chronic pain.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work..
Additional information
Funding
References
- Treede RD, Rief W, Barke A, et al. The IASP Taskforce for the Classification of Chronic Pain. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the international classification of diseases ICD-11. Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
- Breivik H, Collett B, Ventfridda V, et al. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10:287–333. doi:10.1016/j.ejpain.2005.06.009
- Mills SEE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br J Anaesth. 2019;123(2):e273–e283. doi:10.1016/j.bja.2019.03.023
- Loeser JD, Schatman ME. Chronic pain management in medical education: a disastrous omission. Postgrad Med. 2017;129(3):332–335. doi:10.1080/00325481.2017.1297668
- International Association for the Study of Pain [IASP]. Interprofessional pain curriculum outline; 2018. Available from: www.iasp-pain.org/Education/CurriculumDetail.aspx?ItemNumber=2057. Accessed February 8, 2021.
- Loeser JD. Five crises in pain management. Pain Clinical Updates. 2012;19(3):111–116.
- Briggs EV, Battelli D, Gordon D, et al. Current pain education within undergraduate medical studies across Europe: Advancing the Provision of Pain Education and Learning (APPEAL) study. BMJ Open. 2015;5(8):e006984. doi:10.1136/bmjopen-2014-006984
- Vadivelu N, Mitra S, Hines RL. Undergraduate medical education on pain management across the globe. Virtual Mentor. 2013;15(5):421–427. doi:10.1001/virtualmentor.2013.15.5.medu1-1305
- Shipton EE, Bate F, Garrick R, et al. Systematic review of pain medicine content, teaching, and assessment in medical school curricula internationally. Pain Ther. 2018;7(2):139–161. doi:10.1007/s40122-018-0103-z
- Kodama Y, Fukahori H, Tse M, et al. Pain prevalence, pain management, and the need for pain education in healthcare undergraduates. Pain Manag Nurs. 2020;S1524–S9042(20):30197. doi:10.1016/j.pmn.2020.09.008
- Watt-Watson J, Hunter J, Pennefather P, et al. An integrated undergraduate pain curriculum, based on IASP curricula, for six health science faculties. Pain. 2004;110(1–2):140–148. doi:10.1016/j.pain.2004.03.019
- Carr ECJ, Watt-Watson J, McGillion M, et al. The quest of pain education leaders in Canada and the United States: a qualitative study. J Adv Nurs. 2016a;72(11):2728–2737. doi:10.1111/jan.13050
- Carr ECJ, Briggs EV, Briggs M, et al. Understanding factors that facilitate the inclusion of pain education in undergraduate curricula: perspectives from a UK survey. Br J Pain. 2016b;10(2):100–107. doi:10.1177/2049463716634377
- Wong ML, Kirk-Sanchez N. Moving from strategy to process: an iterative and formative approach to integrating the IASP pain curriculum guidelines into an established physical therapy program. J Allied Health. 2021;50(3):213–220.
- Webster F, Bremner S, Oosenbrug E, et al. From opiophobia to overprescribing: a critical scoping review of medical education training for chronic pain. Pain Med. 2017;18(8):1467–1475. doi:10.1093/pm/pnw352
- World Health Organization [WHO]. World health assembly update, 25 May 2019; 2019. Available from: https://www.who.int/news-room/detail/25-05-2019-world-health-assembly-update. Accessed January 15, 2021.
- Carr DB, Bradshaw YS. Time to flip the pain curriculum? Anesthesiology. 2014;120(1):12–14. doi:10.1097/ALN.0000000000000054
- Gatchel RJ, Peng YB, Peters ML, et al. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581–624. doi:10.1037/0033-2909.133.4.581
- Veirman E, Van Ryckeghem DM, De Paepe A, et al. Multidimensional screening for predicting pain problems in adults: a systematic review of screening tools and validation studies. Pain Rep. 2019;4(5):e775. doi:10.1097/PR9.0000000000000775
- Walankar PP, Panhale VP, Patil MM. Psychosocial factors, disability and quality of life in chronic shoulder pain patients with central sensitization. Health Psychol Res. 2020;8(2):8874. doi:10.4081/hpr.2020.8874
- Miller RM, Kaiser RS. Psychological characteristics of chronic pain: a review of current evidence and assessment tools to enhance treatment. Rev Curr Pain Headache Rep. 2018;22(3):22. doi:10.1007/s11916-018-0663-y
- Ramanayake RP, Basnayake BM. Evaluation of red flags minimizes missing serious diseases in primary care. J Family Med Prim Care. 2018;7(2):315–318. doi:10.4103/jfmpc.jfmpc_510_15
- Herndon CM, Zoberi KS, Gardner BJ. Common questions about chronic low back pain. Am Fam Physician. 2015;91(10):708–714.
- Lytton K, Woolley T, Rasalam R, et al. Benefits of simulated general practice clinics in the preparation of medical students for primary healthcare. Educ Prim Care. 2019;30(5):275–281. doi:10.1080/14739879.2019.1623087
- Linton SJ, Flink IK, Nilsson E, et al. Can training in empathetic validation improve medical students’ communication with patients suffering pain? A test of concept. Pain Rep. 2017;2(3):e600. doi:10.1097/PR9.0000000000000600
- Gupta A. The importance of good communication in treating patients’ pain. AMA J Ethics. 2015;17(3):265–267. doi:10.1001/journalofethics.2015.17.3.sect1-1503
- Tait RC. Empathy: necessary for effective pain management? Curr Pain Headache Rep. 2008;12(2):108–112. doi:10.1007/s11916-008-0021-6
- Wertli MM, Burgstaller JM, Weiser S, et al. Influence of catastrophizing on treatment outcome in patients with nonspecific low back pain: a systematic review. Spine. 2014;39(3):263–273. doi:10.1097/BRS.0000000000000110
- Martel MO, Wasan AD, Jamison RN, et al. Catastrophic thinking and increased risk for prescription opioid misuse in patients with chronic pain. Drug Alcohol Depend. 2013;132(1–2):335–341. doi:10.1016/j.drugalcdep.2013.02.034
- Legarreta M, Bueler E, DiMuzio J, et al. Predicting risk for opioid misuse in chronic pain with a single-item measure of catastrophic thinking. J Nerv Ment Dis. 2018;206(3):217–222. doi:10.1097/NMD.0000000000000799
- Stewart M, Loftus S. The impact of language in musculoskeletal rehabilitation. J Orthop Sports Phys Ther. 2018;48(7):519–522. doi:10.2519/jospt.2018.0610.32
- Joos B, Uebelhart D, Michel BA, et al. Influence of an outpatient multidisciplinary pain management program on the health-related quality of life and the physical fitness of chronic pain patients. Biomedicine. 2004;3:1–10. doi:10.1186/1477-5751-3-1
- Danilov A, Danilov A, Barulin A, et al. Interdisciplinary approach to chronic pain management. Postgrad Med. 2020;132(sup3):5–9. doi:10.1080/00325481.2020.1757305
- Hassan S, Carlin L, Zhao J, et al. Promoting an interprofessional approach to chronic pain management in primary care using Project ECHO. J Interprof Care. 2020a;9:1–4. doi:10.1080/13561820.2020.1733502
- Kassutto S, Seam N, Carlos WG, et al. Twelve tips for conducting successful interprofessional teaching rounds. Med Teach. 2020;42(1):24–29. doi:10.1080/0142159X.2018.1545086
- Boet S, Bould MD, Layat Burn C, et al. Twelve tips for a successful interprofessional team-based high-fidelity simulation education session. Med Teach. 2014;36:853–857. doi:10.3109/0142159X.2014.923558
- Fricton J. The need for preventing chronic pain: the “big elephant in the room” of healthcare. Glob Adv Health Med. 2015;4(1):6–7. doi:10.7453/gahmj.2014.075
- Smith BH, Hardman JD, Stein A, et al. Managing chronic pain in the non-specialist setting: a new SIGN guideline. Br J Gen Pract. 2014;64(624):462–464. doi:10.3399/bjgp14X680737
- Badiola IJ. Can chronic pain be prevented? Anesthesiol Clin. 2016;34:303–315. doi:10.1016/j.anclin.2016.01.008
- Glattacker M, Dudeck A, Dibbelt S, et al. Evaluation of a collaborative goal setting intervention in patients with chronic back pain. Rehabilitation. 2013;52(4):257–265. doi:10.1055/s-0032-1327724
- Filoramo MA. Improving goal setting and goal attainment in patients with chronic noncancer pain. Pain Manag Nurs. 2007;8(2):96–101. doi:10.1016/j.pmn.2007.03.005
- Costantino RC. Setting realistic goals for patients with chronic pain. Pharmacy Today. 2017;23(9):45–46. doi:10.1016/j.ptdy.2017.09.002
- Moseley GL, Butler DS. Fifteen years of explaining pain: the past, present, and future. J Pain. 2015;16(9):807–813. doi:10.1016/j.jpain.2015.05.005
- Maguire N, Chesterton P, Ryan C. The effect of pain neuroscience education on sports therapy and rehabilitation students’ knowledge, attitudes, and clinical recommendations toward athletes with chronic pain. J Sport Rehabil. 2019;28(5):438–443. doi:10.1123/jsr.2017-0212
- Aguirrezabal I, Pérez de San Román MS, Cobos-Campos R, et al. Effectiveness of a primary care-based group educational intervention in the management of patients with migraine: a randomized controlled trial. Prim Health Care Res Dev. 2019;20:e155. doi:10.1017/S1463423619000720
- Luciano JV, Sabes-Figuera R, Cardeñosa E, et al. Cost-utility of a psychoeducational intervention in fibromyalgia patients compared with usual care: an economic evaluation alongside a 12-month randomized controlled trial. Clin J Pain. 2013;29(8):702–711. doi:10.1097/AJP.0b013e318270f99a
- Romm MJ, Ahn S, Fiebert I, et al. A meta-analysis of therapeutic pain neuroscience education, using dosage and treatment format as moderator variables. Pain Pract. 2020;9:1201. doi:10.1111/papr.12962
- Louw A, Zimney K, Puentedura EJ, et al. The efficacy of pain neuroscience education on musculoskeletal pain: a systematic review of the literature. Physiother Theory Pract. 2016;32(5):332–355. doi:10.1080/09593985.2016.1194646
- Joypaul S, Kelly F, McMillan SS, et al. Multi-disciplinary interventions for chronic pain involving education: a systematic review. PLoS One. 2019;14(10):e0223306. doi:10.1371/journal.pone.0223306
- McClive-Reed KP, Gellis ZD. Psychological distress and help-seeking by residents of a Neighborhood Naturally Occurring Retirement Community (NNORC). J Gerontol Soc Work. 2016;59(7–8):572–586. doi:10.1080/01634372.2016.1222474
- Lemieux J, Abdollah V, Powelske B, Kawchuk G. Comparing the effectiveness of group-based exercise to other non-pharmacological interventions for chronic low back pain: a systematic review. PLoS One. 2020;15(12):e0244588. doi:10.1371/journal.pone.0244588
- Orhan C, Van Looveren E, Cagnie B, et al. Are pain beliefs, cognitions, and behaviors influenced by race, ethnicity, and culture in patients with chronic musculoskeletal pain: a systematic review. Pain Physician. 2018;21(6):541–558.
- Smith BE, Hendrick P, Bateman M, et al. Musculoskeletal pain and exercise-challenging existing paradigms and introducing new. Br J Sports Med. 2019;53(14):907–912. doi:10.1136/bjsports-2017-098983
- Geneen LJ, Moore RA, Clarke C, et al. Physical activity and exercise for chronic pain in adults: an overview of Cochrane reviews. Cochrane Database Syst Rev. 2017;1(1):CD011279. doi:10.1002/14651858.CD011279.pub2
- Ambrose KR, Golightly YM. Physical exercise as non-pharmacological treatment of chronic pain: why and when. Best Pract Res Clin Rheumatol. 2015;29:120–130. doi:10.1016/j.berh.2015.04.022
- Joelsson M, Bernhardsson S, Larsson ME. Patients with chronic pain may need extra support when prescribed physical activity in primary care: a qualitative study. Scand J Prim Health Care. 2017;35(1):64–74. doi:10.1080/02813432.2017.1288815
- Luque-Suarez A, Martinez-Calderon J, Falla D. Role of kinesiophobia on pain, disability and quality of life in people suffering from chronic musculoskeletal pain: a systematic review. Br J Sports Med. 2019;53(9):554–559. doi:10.1136/bjsports-2017-098673
- Siegler M, Frange C, Andersen ML, et al. Sleep, pain and exercise: an integrative perspective on neuroscience education: comments on article titled “Exercise therapy for chronic musculoskeletal pain: innovation by altering pain memories. Man Ther. 2015;20(1):e1–2. doi:10.1016/j.math.2014.10.016
- Louw A, Vogsland R, Marth L, et al. Interdisciplinary pain neuroscience continuing education in the veterans affairs. Clin J Pain. 2019;35(11):901–907. doi:10.1097/AJP.0000000000000756
- Micheletti JK, Bláfoss R, Sundstrup E, et al. Association between lifestyle and musculoskeletal pain: cross-sectional study among 10,000 adults from the general working population. BMC Musculoskelet Disord. 2019;20(1):609. doi:10.1186/s12891-019-3002-5
- Field R, Pourkazemi F, Turton J, et al. Dietary interventions are beneficial for patients with chronic pain: a systematic review with meta-analysis. Pain Med. 2020;21:1–21. doi:10.1093/pm/pnaa378
- Nijs J, Lluch Girbés E, Lundberg M, et al. Exercise therapy for chronic musculoskeletal pain: innovation by altering pain memories. Man Ther. 2015;20(1):216–220. doi:10.1016/j.math.2014.07.004
- Hassan S, Zheng Q, Rizzolo E, et al. Does integrative medicine reduce prescribed opioid use for chronic pain? A systematic literature review. Pain Med. 2020b;21(4):836–859. doi:10.1093/pm/pnz291
- Lin YC, Wan L, Jamison RN. Using integrative medicine in pain management: an evaluation of current evidence. Anesth Analg. 2017;125(6):2081–2093. doi:10.1213/ANE.0000000000002579
- Thomas DA, Maslin B, Legler A, et al. Role of alternative therapies for chronic pain syndromes. Curr Pain Headache Rep. 2016;20(5):29. doi:10.1007/s11916-016-0562-z
- Dunford E, Thompson M. Relaxation and mindfulness in pain: a review. Rev Pain. 2010;4(1):18–22. doi:10.1177/204946371000400105
- Stoicea N, Costa A, Periel L, et al. Current perspectives on the opioid crisis in the US healthcare system: a comprehensive literature review. Medicine. 2019;98(20):e15425. doi:10.1097/MD.0000000000015425
- Tobin H, Klimas J, Barry T, et al. Opiate use disorders and overdose: medical students’ experiences, satisfaction with learning, and attitudes toward community naloxone provision. Addict Behav. 2018;86:61–65. doi:10.1016/j.addbeh.2017.11.028
- Singh R, Pushkin GW. How should medical education better prepare physicians for opioid prescribing? AMA J Ethics. 2019;21(8):E636–641. doi:10.1001/amajethics.2019.636
- Chouinard S, Prasad A, Brown R. Survey assessing medical student and physician knowledge and attitudes regarding the opioid crisis. WMJ. 2018;117(1):34–37.
- Wallace PM, Warrier S, Kahn MJ, et al. Developing an opioid curriculum for medical students: a consensus report from a national symposium. Subst Abus. 2020;41(4):425–431. doi:10.1080/08897077.2019.1635971