
Abstract
Background
People with chronic low back pain experience myriads of problems from living with their condition. This study aimed to explore the lived experience of people with chronic low back pain in Ethiopia.
Design
This is a qualitative semi-structured study design which used an interpretative phenomenological analysis approach for data analysis.
Participants
Fifteen adults (10 women and 5 men) with chronic low back pain (duration ≥ 3 months) with age ranging from 19 to 66 years old were interviewed.
Setting
Participants were recruited from the outpatient departments of the University of Gondar hospital in Gondar, Ethiopia.
Methods
Data was collected through an in-depth semi-structured interview. Interviews were audio-recorded and transcribed verbatim. Data were analyzed through an iterative process, beginning with a line-by-line coding to identify the lived experience of chronic low back pain.
Findings
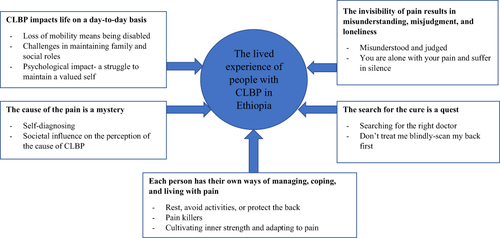
Five main themes related to the lived experience of people with chronic low back pain emerged: 1) CLBP impacts life on a day-to-day basis, 2) The invisibility of pain results in misunderstanding, misjudgment, and loneliness, 3) The cause of pain is a mystery, 4) The search for the cure is a quest, 5) Each person has their ways of managing, coping, and living with pain.
Conclusion
The findings from this study improve our understanding of the experience of people with chronic low back pain and its impact on their day-to-day life in Ethiopia. The findings from this study could inform the development of culturally centered chronic low back pain interventions such as self-management programs in the Ethiopian context.
Background
Chronic low back pain (CLBP) is often associated with longstanding or recurrent disability,Citation1–5 high socio-economic costs,Citation6–8 and psychosocial disruptions, including distorted self-image, shame, helplessness, social isolation, and perception of lowered self-esteem.Citation9,Citation10 CLBP is complex, and medical management rarely alleviates pain completely.Citation11 Moreover, people with low back injuries often experience pain despite evidence of tissue healing.Citation12 A substantial amount of evidence from previous studiesCitation10,Citation12–17 shows that people with CLBP not only suffer the impact of pain but also, as Smith & Osborn described it, “a cumulative failure of interventions” (p.518).Citation11
There is a scarcity of research related to CLBP in Ethiopia. However, a few available studies show that LBP is a prevalent musculoskeletal health condition impacting the lives of people living with the condition.Citation18–23 For instance, a recent study conducted by Beyera et al shows that LBP interfered with several activities of daily living of people with the condition, including, sleep disturbance, lack of productivity and time off work.Citation23 The authors also reported several biopsychosocial factors such as older age, level of education, rural residence, depressive symptoms, and negative pain beliefs associated with chronicity of LBP in Ethiopia.Citation23
A bulk of research on CLBP focuses on quantifying problems associated with the pain (eg, pain severity and magnitude of disability).Citation8,Citation24–27 However, pain is a subjective and experiential phenomenon that can be influenced by multitudes of spiritual, cognitive, cultural, and biomedical factors.Citation28,Citation29 These interconnected factors are difficult to capture with quantitative inquiry driven by a positivist paradigm. On the other hand, qualitative research adopts a different ontological and methodological approach suitable to explore the experiences and the meanings people with pain assign to their condition.Citation12,Citation29
Previous studies have explored the lived experience of people with low back pain (LBP) using an interpretative phenomenological analysis, a line of inquiry in qualitative psychological research.Citation11,Citation12,Citation30–34 These studies have highlighted the value of exploring the subjective experiences of living with CLBP by going beyond disease-specific beliefs to understand how people with the condition make sense of their world. Evidence from these studies indicates the process of living with pain for an extended time plays a significant role in how people with CLBP make sense of what is happening to them, which informs their lived experiences and the many meanings attached to it.Citation11
The existing qualitative studies on CLBP are primarily from developed countries reflecting experiences and meanings of pain from the Western perspective.Citation11,Citation12,Citation35–37 On the other hand, there is a shortage of such studies in developing countries such as Ethiopia. Evidence shows that people with diverse cultural backgrounds assign different meanings to their pain experiences,Citation35,Citation38 situated within their spiritual-cultural-social-personal setting.Citation29
The existing evidence in Ethiopia show people with low back pain receive inequitable and inaccessible health services.Citation21 There is also a substantive evidence-to-practice gap in the care provided to people with the condition. As demonstrated by Beyere et al, a significant number of people with low back pain received pharmacological or surgical interventions, as opposed to low back pain managements that align with the current clinical guidelines, such as receiving self-management support, exercises, psychological, or cognitive behavioral interventions.Citation21 Understanding the pain perceptions and the lived experiences of people with CLBP is essential to identify their health care needs.Citation37 It can also help the health care providers and health system planners to identify ways to offer care that is more tailored to the needs and expectations of people with CLBP within an Ethiopian cultural context.
However, there are no documented qualitative studies in Ethiopia with a focus on exploring the lived experiences of people with CLBP. It is unknown how people living with CLBP make sense of what it means to live with their pain in Ethiopia. This study aimed to explore the lived experience of adults living with CLBP from an idiographic phenomenological perspective in Ethiopia.
Methods
Study Design
This qualitative study employed an interpretative phenomenological analysis (IPA) approach to explore the lived experience of people with CLBP in Ethiopia.Citation38,Citation39 As an analytical process, IPA involves “double hermeneutics” as it involves a dual interpretation of the phenomena under study. The participants make meaning of their world, while the researcher interprets their meaning-making.Citation38,Citation39 IPA researchers attempt to understand what it means to be in “someone’s shoes” using an interpretative lens to give meaning to people’s experiences.Citation39 IPA enables an in-depth understanding of complex and difficult-to-articulate topics such as pain.Citation40 IPA also relies on an idiographic single-case in-depth analysis of individual’s experiences in their unique contexts.Citation30,Citation39 This study complies with the set of ethical principles recognized in the declaration of Helsinki.Citation41 Ethical approval was obtained from Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board (reference no.TRAQ#:6025614) and the Institutional Review Board of the University of Gondar (reference no.C/V/P/RCS/05/1046). All participants provided written consent to participate in this study and the publication of their anonymized responses. Furthermore, the names used in this manuscript to illustrate examples of individual accounts are pseudonyms.
Participants and Settings
A purposive sampling was employed to recruit 15 adults with CLBP from the University of Gondar Hospital medical and surgical outpatient departments, where they were attending care for their pain. The University of Gondar Hospital is a tertiary referral hospital located in Gondar town in Central Gondar Zone of the Amhara regional state in Northwest Ethiopia, which provides health services for over 5 million residents in the Amhara regional state and the neighbouring regions in the country. According to the recent census, Central Gondar Zone has 2,288,442 inhabitants,Citation42 with a predominantly Amhara ethnic group who speaks Amharic language with Orthodox Christian faith.
Participants were invited to be approached by a researcher by their healthcare provider in the outpatient department. Patients were eligible to participate if they had LBP for three months or more, attend care for LBP at the university hospital, were eighteen years or older, reported the ability to communicate in Amharic, and were willing to participate in the study. Exclusion criteria included pregnant women, people with CLBP visiting the hospital primarily for other health problems, and people with specific pathology of the back such as cancer. There is no rule as to how many participants should be included in IPA studies. Previous studies have included samples that range from one to over 30 participants.Citation43 However, it is in the nature of IPA that researchers collect data from a small sample to allow an in-depth case-by-case analysis of the interview data.Citation30,Citation39 Unlike other qualitative research traditions, data “saturation” is not the focus of phenomenological research.Citation44,Citation45 Van Manen advises phenomenological researchers to consider how many examples of tangible, experiential descriptions are needed to explore the meaning instead of the number of interviews.Citation46
Data Collection
An in-depth semi-structured interviews were conducted to generate a detailed description of an individual’s lived experience of CLBP.Citation39 The guide allowed flexibility to explore relevant participant’s accounts as they arose (see Appendix A for a sample interview guide). Every interview began by collecting participant’s socio-demographic and clinical information, such as the duration of their LBP, followed by a broader question, “What is it like to live with CLBP?” Probes such as “what do you mean by that…”, were also used to explain further and clarify with the participants.Citation47
The interviews were conducted at one of the private offices in the University of Gondar hospital compound, where it was safe for the participants to share their personal experiences. The lead author conducted all interviews in Amharic (the primary language of the participants). All interviews were audio-recorded with a digital audio-recorder made visible to the study participants. Interviews lasted between 35 to 71 minutes. Observational data and field notes were also written down immediately at the end of interviews with the participants. Data were collected between April and June 2019.
Data Analysis
Data analysis followed the guidelines for interpretative phenomenological analysis suggested by Smith.Citation11,Citation38 Nvivo 12 software was used in the analytic process to assist in data management and coding.Citation48 There were six main steps to the analysis process as listed below.
Step 1: Immersing in the data through listening to the audio recording and reading the verbatim transcripts.
Step 2: Formulating initial notes and a free textual analysis of the data.
Step 3: Turning the initial notes and memos into emergent themes. The emergent themes were at the higher level of abstraction, rooted in the participant’s experiences.
Step 4: Finding connections between emergent themes and grouping them based on conceptual similarities. Specifically, attention was paid to participant’s cultural narratives to shed light on the local understanding.
Step 5: Moving to the next participant and repeated the same process outlined above to create an individual account of the experience while keeping an idiographic commitment.
Step 6: Finding connections between the main themes developed from each participant. A master table of themes and sub-themes was created, which was then transformed into a narrative account.
All the above steps in the analytic process were conducted in the Amharic language to minimize meaning loss and enhance the validity of the research.Citation49 Once the master table was created, the themes and participant’s quotes were translated to English to engage the rest of the research team (JM, CD, SG) who do not speak Amharic into the next step of the analysis.
Rigour and Trustworthiness
Sufficient participant quotes were presented to ensure the internal coherence and validity of the themes.Citation32 Two team members, MBC and AA independently coded four interviews to ensure rigour and systematic coding of the transcripts. They met multiple times to ensure uniformity in the coding process before moving to a subsequent transcript.Citation32 A series of peer debriefing meetings on the coding procedure was held with the larger research team. The first author coded all the remaining interviews for consistency while maintaining frequent discussions with the rest of the research team.
Additionally, phenomenological reflection was attained to explain specific meanings of living with CLBP.Citation50 We have provided a few excerpts from the reflexive journal in Appendix B. When clarifying complex meanings related to the phenomena under study was needed, colleagues who grew up in the participants’ culture were consulted. Lastly, the Consolidated Criteria for Reporting Qualitative Research checklist was used to report the study findings.Citation51
Findings
Ten females and five male participants (total n=15) with CLBP with ages ranging from 19 to 66 were interviewed. No participants declined the initial invitation to be invited to participate in the study, but one participant declined participation at the time of providing informed consent with the researcher. The median duration of LBP was five years (minimum =1.5, maximum 20 years). shows details of the socio-demographic characteristics of the study participants.
Table 1 Socio-Demographic Characteristics of the Participants (n=15)
A thorough analysis of the interviews and a phenomenological reflection resulted in five main themes related to the lived experience of people with CLBP in Ethiopia: 1) CLBP impacts life on a day-to-day basis, 2) The invisibility of pain results in misunderstanding, misjudgment, and loneliness, 3) The cause of pain is a mystery, 4) The search for the cure is a quest, 5) Each person has their ways of managing, coping, and living with pain.
The main themes and sub-themes about the lived experiences of people with CLBP are presented in . Selected participants’ quotes illustrating the sub-themes are also shown in the Appendix C section.
Figure 1 Main themes and sub-themes: the lived experience of people with CLBP in Ethiopia.
Chronic Low Back Pain Impacts Life on a Day-to-Day Basis
All participants in this study experienced pain that has impacted multiple dimensions of their lives. When asked about what it means to live with CLBP, almost all participants responded, “በጣም ከባድ ነው”, which means, “it is difficult to live with the pain” in English.
The findings show that CLBP hindered individual’s ability to lead their lives in their terms, which was expressed as “a loss.” Shegaw, a 30-year-old man, showed how frustrated he is with his pain frustration when he said,
It is tough to live with back pain. What more suffering can come more than this? The disease has been eating me for the past four or five years. The life that I lived during these four years was not life. I wish I could go back and take those years out of my life. It is a wasted life. Back pain is something you wouldn’t wish on to the wild beast, let alone on a human being.
Further data analysis resulted in the following experiential sub-themes portraying how pain impacted various dimensions of living with CLBP.
Loss of Mobility Means “Being Disabled”
The participants viewed their “back” as central to their health and wellbeing. According to them, any damage or pain in the back affected their mobility. Girma’s metaphor is an illustration of how people with CLBP make sense of what it means to live with a “damaged” back:
When you see a snake and want to kill it, you either hit its head or its back. If you first hit its back, there is no way it moves. It is the same. Our back is important for our movement. You can’t move if you have pain (Girma, 55 years old man)
A number of participants shared Girma’s sentiment and further explained their pain experience as confining and restrictive, which deterred them from moving around and conducting their day-to-day life. For Adanech, who works as a file sorter at a printing press, the captivity of the pain devoid her of the freedom to do her work. She described her experience as,
It feels like you are tied to something. It holds you down when you try to get up from sitting or moving around to work. (Adanech, 46-year-old woman)
Alemu, a 55-year-old farmer, also explained how the pain imposed restrictions on his farming activities. He said,
I feel pain all the time. It doesn’t let me farm. Let alone bending and pulling the “mofer” [a traditional plow drawn by oxen] out of the soil, I can’t even keep up with the speed of the oxen.
Overall, the challenges of not being able to move around and engage in essential daily living activities due to CLBP are equated with being “disabled”, as summed by Bekelech:
If you cannot move, you are a disabled person. After all, having this pain is nothing less than being disabled. (Bekelech, 24-year-old woman)
Challenges in Maintaining Family and Social Roles
The participants considered family and social roles foundational to their existence and loss of these roles emotionally difficult. For instance, Kebede’s account indicates that the inability to fulfill his kid’s needs due to his back pain was “damaging.” He said,
It is damaging when your kids cannot get what they deserve from you. One day, my daughter asked me, ‘papa why don’t you walk me to the school like other parents of my classmate friends?’ (Kebede, 66-year-old man)
Bekelech, a 24-year-old woman, who is the oldest daughter in the family, had difficulty accepting that she could not share the burden of household chores with her parents. She felt guilty for sitting around and watching her parents do the housework:
I feel bad for not assisting my parents with some chores. You know…you cannot do anything when the pain prevents you from getting up from the chair to move.
For our participants, one’s worth is measured by the ability to maintain social connections and contribute to social causes (eg, funerals, baptism, weddings). The participants had difficulties living up to the social expectations as a result of their CLBP. Specifically, it was more troubling for women who perceived their social expectations to be higher than men. When Askal was asked about the social impact of living with CLBP, she said,
You cannot conduct your social life like everyone else. When you have the pain, you are stuck at home. Even if I go [attend social events], I do nothing but sit, which is even hard as a woman. We have lots of social responsibilities compared to men. (Askal, 42-year-old woman)
She further elaborated that not maintaining social connection due to pain results in fear of outcast by the community. She said,
Your worth is dependent on your social connections- if you cannot maintain social connections, it means you are left out.
Psychological Impact- A Struggle to Maintain a “Valued Self”
For the interviewees, CLBP was considered a threat to their sense of valued self-identity. Data shows two major aspects where the participants struggled to maintain their “valued self.”
People with CLBP felt worthless when comparing themselves to others in their social circle who enjoy relative freedom to do whatever they like in life. As such, social comparison elicited negative emotions, which damaged their sense of valued self. Lamrot summed her feelings as:
There is nothing as bad as living with this pain; it makes you feel inferior to others, to your friends and neighbours. I see them go to a market without any problem and I don’t have a choice but to stay at home. That makes me feel sad and think less of myself. (Lamrot, 65-year-old woman)
The data also shows that people with CLBP witness an erosion of their previously perceived sense of personal identity. They considered their previous self a “strong and enduring person who could do anything”, which is now no longer accessible to them. The participants perceived their current self as “embodying a body weakened by pain”, which was undoubtedly frustrating.
Tizita, a 40-year-old female, explained her experience as
I used to walk far to fetch water. I gave birth to twins twice. You know, I used to be a very strong woman; I never felt defeated by anything. This one has broken me down.
Adanech also considered her present body as fragile as an “egg” that cannot withstand any pressure or load from work. She said,
I told you I used to carry lots of things to the market, things that weigh around 25 kg. I never needed any assistance from others. But now…hmm… I feel like I am an egg-that is how I think of my body. (Adanech, 46-year-old woman)
The Invisibility of Pain Results in Misunderstanding, Misjudgment, and Loneliness
Our interpretative phenomenological analysis of living with chronic low back pain shows that living with chronic pain as an invisible illness has several consequences impacting their ability to live their lives. The following sub-themes illustrate what it means to live with an invisible pain.
Misunderstood and Judged
Almost all the participants reported that others doubted them about their pain experiences. Bekelech said,
Isn’t it a must for us to be confined to bed to be understood? If people see you walking, they think you are well. But back pain is not like that. You are in pain. (Bekelech, a 24-year-old woman)
The above personal account of living with CLBP is a testimonial that the “invisibility of the pain” leads to being misunderstood by others.
At times, the participants wished that there are ways that they can objectify and make their “hidden and invisible pain” visible on their bodies so that others believe them. Asnaku’s account was an illustration of this conviction when she said:
I wish back pain is visible. You know I would be happy if back pain is as visible as a broken bone in my arm or my leg so that they see it. If they see a wound on your body, they sympathize with you. Otherwise, no one believes you. (Asnaku, 32-year-old woman)
People with CLBP are often misunderstood and judged in a social context with an expectation of social and cultural transactions. Askal’s account is a perfect example to illustrate this phenomenon. She said,
Those who do not know about my back problem do not understand me. Some even do not talk to me. There was a time when I could not go to a funeral of a friend whose husband passed away. And one day, she saw me walking on the street and disregarded me. She resented me. Of course, I heard about her husband’s death, but I could not go because I was in pain. I couldn’t even get out of my house at the time. (Askal, 42-year-old woman)
You are Alone with Your Pain and Suffer in Silence
Our participants expressed their experience of living with CLBP as isolating and lonely, which lead them to feel more negative emotions such as worry and suffering. Askal, a 42-year-old woman said:
It makes you feel lonely. It bothers you a lot, especially when you are alone.you are just alone with your pain.
Another participant also discussed how lonely it feels to live with CLBP when he said,
If your illness is something that you can see with your eyes, you will find a solution. Otherwise, you only feel it when it eats you from inside. It chews you from inside without you or others know it. (Shegaw, 30-year-old man)
Despite experiencing isolation and loneliness while living with CLBP, a few participants hesitated to disclose their situation to other people, including their bosses. Revealing their pain experience to those who may not comprehend what they were going through had repercussions such as judgment, stigmatization, and lack of validation of their pain experiences. Kebede’s account illustrates this notion when he said,
You keep it to yourself.there is a lot inside of you that you can say, but you won’t share that with those who do not understand your pain- some may think of you differently. When people ask me how I was doing, I always say ‘I am fine.’ (Kebede, 66-year-old man)
Overall, fear of negative consequences is the main reason why people with CLBP conceal their pain experience and suffer in silence. For instance, Bekelech, a 24-year-old woman, said,
when my pain gets higher, I take a break and sit in the middle of work, and my boss is not happy about that. I do not even try to make her understand what I am going through. Because she does not understand such a thing. So, no, I do not try to tell her.
The Cause of the Pain is a Mystery
Our findings show that the cause of the pain is confusing and mysterious to people with CLBP. Their perception of what caused the pain was often incongruent with what their health care providers tell them. In such times, the participants relied on their own or societal beliefs to make sense of the reason for their pain.
Self-Diagnosing
Most participants associated the cause of their back pain with damages to some structures in their back, such as discs or ligaments, due to manual labor or engaging in strenuous activities. For example, Shegaw said:
Maybe it could be related to the heavy load of woods I used to carry when I was a little boy.maybe that damaged my back. (Shegaw,30-year-old man)
A few women participants speculated the cause of their back pain to giving birth to lots of children and long labor during delivery. Ergoye said,
Giving birth to so many children.the long labour during birth which may sometimes take up to three or four days can tear our body- our back apart. That can cause back pain. We had no option other than to give birth at our homes. These days, women go to the hospital and give birth instantly. (Ergoye, 39-year-old woman)
A few of the participants found the doctor’s diagnosis conflicting with their beliefs of the cause of their back pain. When the doctor’s diagnosis was not compelling, people with CLBP opted for their views of what caused their pain.
Girma, 55-year-old man:
…on that day they told me, ‘something has slipped out of your back.’ Hmm, they said something like a ‘disc.’ But I do not think it is from a disc. Isn’t this thing called ‘disc,’ something we are born with? Well, I never had any problem with that before. So, I do not think it is from that. I think my back pain could either be from dryness or thinning of the bones. Or maybe from my sleeping position.
Societal Influence on the Perception of People with CLBP on the Cause of the Pain
When self-diagnosing is not sufficient to make sense of the cause of their back pain, the participants relied on socio-cultural-related beliefs (eg, supernatural beliefs) to make sense of the cause of their back pain. Adanech- A 46-year-old woman, said:
Initially, I thought it is from my muscles, and I went to the healer. He tried so many things for me. It did not work. When it got worse, some people told me it could be from her [evil spirit], and they advised me to make some sacrifices for her. Hmm, I don’t know, but who knows?
The Search for the Cure is a Quest
People with CLBP have spent a great deal of their time looking for answers for their back problems. Their expectation of curative treatment has not been realized. For the participants, the search for a cure is a quest with no resultant outcome. The following two sub-themes exemplify this phenomenon.
Searching for the Right Doctor
People with CLBP are constantly searching for the right health care provider who could offer solutions for their pain. Kebede explained that he had exhausted all his options, and seeing multiple specialists at different health care institutions did not resolve his pain:
I tried everything. I saw lots of doctors in Addis Ababa and Gondar. I even consulted those with big names- Dr. Y and Dr. L [both names replace] and received lots of treatments. But it [the pain] keeps coming back. What I haven’t tried yet is ‘behalawi wegesha’ (a traditional healer). (Kebede-66-year-old man)
Several participants expressed dissatisfaction with their health care provider’s diagnosis and approach to pain management. Kelemua, who lived with LBP for six years, said,
They did not understand my problem. They keep giving me painkillers. When I went back and told them that I wasn’t getting better, they gave me a different kind of medicine. That did not help either. I went to see a doctor at a private clinic. Still, it is the same- nobody knows what to do for me. (Kelemua-48-year-old woman)
A few participants also revealed that their concerns were not taken seriously by their health care providers. Instead, the providers used scary language and recommended an invasive management option for their back pain. One participant said:
He (a surgeon) scared me that I am in danger and I must have surgery for my back problem. He even asked me whether I have children or not as if I will not be able to have kids after surgery. It was worrying, and I asked him if there are other options. He said, ‘that is the only thing I can do for you.’ He didn’t even look at me as if I am something. I left his clinic and never went back again. (Tadese-36-year-old man)
Do Not Treat Me Blindly- Scan My Back first
The participants felt that having diagnostic imaging for their back problems is essential for solving the puzzle. Such beliefs came from the assumption that “knowing the exact cause of the pain means getting their back problems fixed easily.”
Kelemua, a 48-year-old woman, said:
In our village, many people complain of back pain. Some of them told me the doctors could see it [her back pain] on the x-ray. That is why I came here. I believe that they can see this thing with an X-ray and find a solution for my pain.
For some of our participants, getting their low back scanned was the first step to validate their belief that their pain is genuine. Even more, it gave them a sense of closure related to the cause of their pain, as if all their problems would be visible with imaging. A participant said:
Before the scan, they used to treat me blindly. Having the scan gave me mental satisfaction. At least I am not treated blindly. (Adanceh, 46-year-old woman)
Each Person Has Their Ways of Managing, Coping, and Living with Pain
Our findings suggest that people with CLBP use different strategies to manage, cope, and live with their pain. The following five sub-themes explain these strategies.
Rest, Avoid Activities, or Protect the Back
In the immediacy of pain, the participants primarily preferred to rest or refrain from engaging in any activities that demanded their back movement. For instance, Bekelech’s account shows that rest is the most accessible technique to minimize pain flare up during activities. She said:
I rest. otherwise it is very painful. I rest or minimize workload. That is what I do. (Bekelech-24-year-old woman)
A few women participants indicated using traditional back support to protect their back and minimize pain during work. Ergoye, a 39-year-old woman, said:
Oh yea.there is a huge difference. I feel much better when I tie my back with ‘meqenet’ [a piece of cloth]. I feel like a load is taken off my back when I do that. I have lots of pain if I take it off. I must tie my back when I work.
Pain Killers
The participants also used pain killers as a viable strategy to manage their pain, especially when they think their pain may interfere with their instrumental activity of daily living, such as attending social events. Tadese said:
Sitting for a longer duration makes me miserable. So, I always take Advil before leaving the house- especially when I plan to meet my friends or plan on going to any event that requires me to sit for a long time. (Tadese, 37-year-old man)
On the contrary, a few participants were hesitant to take pain medications for a long duration, fearing the side effects. Instead, they opted for traditional remedies to manage their pain. A female participant said,
Some people told me that medicine is not good; It is bad for a liver. So, I tell my kids to massage my back. I sometimes go to a healer. He [the healer] thought something was wrong with the bones, and he used a glass and fire [cupping] to lift it for me. I got temporary relief from it. (Adanech-46-year-old woman)
Cultivating Inner Strength and Adapting to Pain
When the effort to cure the pain failed and no foreseeable timeline to see themselves pain-free, the participants turned their attention inward and cultivated resilience to cope with their back pain. Tizita’s experience exemplifies how people with CLBP focus on adapting and developing an inner strength to cope with their pain. She said,
I lived with my pain for…hmm…eleven years now. Sometimes I think of myself as a woman who has two husbands. I have my real husband and then this pain, and I don’t know if it will ever leave me [the pain]. So, I never sit around and wait until it goes away. Rather, I withstand it and focus on my work. I consider myself a strong woman. I think that is why I usually feel better. (Tizita-40-year-old woman)
Furthermore, a few participants accepted, normalized, and adapted to their pain. One participant used a metaphor discussing how he adapted to his pain experience. He said,
When you live with your pain for a very long time, you adapt to it, and it becomes normal. You do not even think of seeing a doctor. Hmm, they say, ‘when you live with your illness for long, it becomes a health!’ (Shegaw, 30-year-old man)
Submit to God, Pray, and Ask for Mercy
The findings show that people with CLBP used several religious and spiritual strategies to cope with their pain. In particular, in the absence of a likely biological explanation for the cause of the pain (eg, injury to the back), the participants had an alternative explanation of the cause of their pain using spiritual and religious beliefs. As a result, they turned to religious and spiritual practices for healing and coping with pain. The following statement by Birtukan, a 19-year-old woman, shows how she considered her pain as a “gift from God”, and he is the only one who can take her pain away from her. She said,
He [God] sent this to me. It is a gift from him. There is nothing to complain about, and I think there is a reason why God sent this [LBP] to me. I only ask him for mercy.
Several participants also used bathing in holy water to cope with their pain, find comfort and inner peace. See Lamrot’s account below:
I can say Wanzaye [a holy water place] is my home. I often go there for healing, and it made me stand on my two feet and walk. I feel at peace when I go there. There are lots of people who give testimony about that place-all of them say ‘they were healed’. (Lamrot, 65-year-old woman)
Maintaining Positive Social Connection
The participants discussed the importance of maintaining a positive and supportive social connection as an antidote to the isolating nature of CLBP. For instance, Askal, a 42-year-old woman with CLBP, explained how a visit by friends distracted her from focusing on the pain. She said:
When they [her friends and colleagues] come to visit me, I am completely detached from my pain. We talk about different things-good things, and I would forget about my pain. They are terrific friends- if I have nothing at home, they share what they have with me.
Discussion
This is the first interpretive phenomenological study that has explored the lived experience of people with CLBP in Ethiopia. The findings from this study provide an important insight into the “lived world” of people with the condition from an Ethiopian perspective.
As illustrated in the participants’ narratives, living with CLBP is challenging as it affected every dimension of their lives. The participants made sense of their CLBP experiences based on a belief that the back is the cornerstone of any movement; hence, any damage or pain means a compromised life. In other words, the structural and functional importance of the back for people with CLBP is the beginning of their sense-making as to what it means to live with a painful low back.Citation17,Citation52
The impact of CLBP on people living with the condition is multidimensional, affecting every facet of their lives. In this study, the physical impact (eg, restriction in mobility), the social impact (eg, difficulty in maintaining social roles), and psychological impact (eg, loss of valued sense of self) are intertwined. The physicality of pain affected participants’ engagement in activities of daily living (eg, farming) and restricted them from participating in valued social life (eg, attending a funeral). The compounding physical and social impacts of pain further resulted in significant psychological problems.Citation53 Participants in this study experienced a loss of valued sense of self which is embedded in their social and cultural values. In particular, the collectivist culture called ‘mahiberawi nuro’ which means, collective life in Ethiopia,Citation54,Citation55 shaped the pain experience of the participants. Consistent with symbolic interactionism,Citation56,Citation57 the “self” is not independent of the social interaction in the collectivist life, hence shaping one’s identity. In the Ethiopian collectivist life, one becomes a valued member of the society by contributing to the social causes (eg, attending a funeral, visiting the sick) and providing social, emotional, or financial support for those in need. This study showed that the inability to contribute to these social causes due to pain damaged the participants’ sense of self, resulting in loneliness, isolation, and a perception of unworthiness. Our results underscore the importance of assessing and managing the multiple dimensions of CLBP, with a particular focus on capturing the psychosocial dimension of pain.
The findings from this study indicate that the invisibility of pain contributes to stigma and judgmental attitudes towards people with CLBP. In particular, people with CLBP felt judgmental attitudes were encountered in the workplace and in social settings. Participants asserted they would prefer to have a visible illness (eg, broken bone) over CLBP to avoid misunderstanding by others. Most participants discussed that they would prefer to keep their pain experience secret from others due to fear of stigma and social disapproval. Previous studies also documented that the invisibility of pain resulted in overt and subtle stigmatization among people with CLBP.Citation58–66 There are several implications of stigma related to people with CLBP in the Ethiopian context. Stigma can be a significant barrier to social participation, resulting in social isolation, loneliness, depression, further intensifying chronicity, and disability related to CLBP.Citation63 The invisible nature of the pain could also reinforce several pain-related behaviours such as playing sick roles and attending to biomedical beliefs (eg, imaging) to validate and legitimize their pain experience. The findings from this study show the need to explore further the impact of stigma related to people with CLBP in Ethiopia.
Most participants attributed the cause of their pain to dysfunction to their spine due to physical causes such as overworking without protecting their back. This perspective of the participants indicates that the biomedical belief related to the cause of LBP is not exclusive to a specific population but a universal phenomenon.Citation35,Citation53 Interestingly, the participants did not associate the cause of their pain with a punitive punishment from God. Instead, in the absence of a likely etiological explanation, people with CLBP used societal and cultural beliefs to justify the cause of their pain. Evidence indicates that people use cultural explanatory models to make sense of their illness in medically unexplained symptoms.Citation67,Citation68 This finding has clinical implications in Ethiopia. The belief that the cause of back pain is dysfunction in the spine may motivate patients to seek biomedically oriented care (eg, fixing damaged back).Citation53 On the contrary, people with non-biomedical beliefs use different coping mechanisms (eg, spiritual and religious rituals).Citation69 Regardless, an improved understanding of patients’ perceived cause of CLBP using a socio-cultural lens would enable health care providers and the broader health system to align services with patient beliefs and expectations of care.
As seen from the results in this study, participants were dissatisfied with the diagnosis and pain management they received from their care providers, showing the unmet health care needs of people with CLBP.Citation12,Citation35,Citation63 The participants placed particular emphasis on receiving proper diagnoses guided with diagnostic imaging. They believed that diagnostic imaging not only legitimizes their pain experience but also guides their pain management. This biomedical belief contradicts guidelines that recommend against the use of low-value health care.Citation70 Regarding pain management, most participants felt that their providers did not address their pain-related concerns during their clinical encounters, showing discordant care for people with CLBP in Ethiopia.Citation71 That led people with CLBP to continue engaging in “health shopping”Citation53 to find satisfactory answers for their pain by visiting various health care providers and traditional healers. These findings highlight the urgent need for a comprehensive patient-centered pain management strategy that emphasizes patient values and preferences. Our findings also indicate the need to address patients’ diagnostic uncertainty and beliefs about their back pain during their clinical encounter.Citation72
Interestingly, most participants in this study relied on spiritual and religious rituals to cope with the adversity of pain. This finding is consistent with previous studies that suggest that spiritual and religious beliefs influence pain perception, tolerance, and coping.Citation69,Citation73–75 Spirituality and religious beliefs are at the center of many Ethiopians, and Christian believers use prayers and bathing in tsebel (holy water) to cure major illnesses.Citation76,Citation77 In addition, participants in our study also depended on social support to overcome the day-to-day challenges of living with the pain. They valued the emotional and material supports and assistance with household chores they received from their social network. This finding is closely related to the concept of social capital, where individuals who have trustworthy social support have an improved sense of belonging and have better-coping strategies when confronted with health challenges.Citation56,Citation78,Citation79 These findings have relevance in designing future patient-centred pain management in Ethiopia. CLBP management interventions (eg, self-management) could capitalize on the existing social and religious structures to address the psychosocial needs of people with the condition.
Finally, we believe that this study adds value to the existing literature on the understanding of chronic low back pain from an Ethiopian perspective, which could be of great importance to a broader scientific community who are interested in this topic. As documented in previous studies, there is a disparity in the number and nature of pain related research between developed and developing countries, including from Africa.Citation26,Citation80 Such pain related research and knowledge gap between developed and developing countries could result in biases with regards to the understanding of pain and treatment recommendation in the underrepresented population. In that sense, the present study addresses a research and knowledge gap in the literature by illuminating the lived experience of people with chronic low back pain from the Ethiopian perspective. As such, our findings contribute to the growing science of pain by reflecting subtle socio-cultural, religious, and spiritual factors that shape the experience of people with chronic low back pain.
This study has a few limitations. Participants were recruited from a hospital setting, and the findings cannot be transferable to people with CLBP in a community setting, who may have different lived experiences. This study was conducted on participants from one geographic location who share the same cultural and religious values. Therefore, we do not claim that the findings of this study are applicable to all people with CLBP in Ethiopia. It would be helpful to include people with CLBP from different socio-cultural backgrounds (eg, age, religion, ethnicity) in future studies to better understand the impact of CLBP and the broader applicability of the findings.
Conclusion
This study provided insight into the lived experiences of people with chronic low back pain in Ethiopia. The data suggest CLBP is a complex health problem which impacted participants’ lives in many ways. The findings could also inform the design of context specific patient-centered pain management approaches that addresses the physical, psychological, and social aspects of the lived experience of people living with the condition. Finally, empirical studies are needed to deepen our understanding of contextual social and cultural factors that influence the experience of living with CLBP in Ethiopia.
Disclosure
The authors declare no conflicts of interest in this work.
Acknowledgment
The authors would like to thank all the participants for taking the time to share their lived experiences of living with chronic low back pain in this study.
Additional information
Funding
References
- de Vet HCW, Heymans MW, Dunn KM, et al. Episodes of low back pain: a proposal for uniform definitions to be used in research. Spine. 2002;27(21):2409–2416. doi:10.1097/01.BRS.0000030307.34002.BE
- Pankey J, Hayes SC. Acceptance and commitment therapy for psychosis. Int J Psychol Psychol Ther. 2003;3:311–328.
- Koes BW, van Tulder MW, Ostelo R, Kim Burton A, Waddell G. Clinical guidelines for the management of low back pain in primary care. Spine. 2001;26(22):2504–2513. doi:10.1097/00007632-200111150-00022
- Airaksinen O, Brox JI, Cedraschi C, et al. Chapter 4: European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006;15(SUPPL. 2):192–300. doi:10.1007/s00586-006-1072-1
- Hayden Jill A, Tougas Michelle E, Riley R, et al. Individual Recovery Expectations and Prognosis of Outcomes in Non-Specific Low Back Pain: Prognostic Factor Exemplar Review. Hayden JA, ed.. Chichester, UK: John Wiley & Sons, Ltd; 2014. doi:10.1002/14651858.CD011284
- Weiner SS, Nordin M. Prevention and management of chronic back pain. Best Pract Res Clin Rheumatol. 2010;24(2):267–279. doi:10.1016/j.berh.2009.12.001
- Aranjan Lionel K. Risk factors for chronic low back pain. J Community Med Health Educ. 2014;4(2). doi:10.4172/2161-0711.1000271
- Freburger JK, Holmes GM, Agans RP, et al. The rising prevalence of chronic low back pain. Arch Intern Med. 2009;169(3):251. doi:10.1001/archinternmed.2008.543
- Reid MC, Williams CS, Concato J, Tinetti ME, Gill TM. Depressive symptoms as a risk factor for disabling back pain in community-dwelling older persons. J Am Geriatr Soc. 2003;51(12):1710–1717. doi:10.1046/j.1532-5415.2003.51554.x
- Snelgrove S, Liossi C. Living with chronic low back pain: a metasynthesis of qualitative research. Chronic Illn. 2013;9(4):283–301. doi:10.1177/1742395313476901
- Smith JA, Osborn M. Pain as an assault on the self: an interpretative phenomenological analysis of the psychological impact of chronic benign low back pain. Psychol Health. 2007;22(5):517–534. doi:10.1080/14768320600941756
- Snelgrove S, Liossi C. An interpretative phenomenological analysis of living with chronic low back pain. Br J Health Psychol. 2009;14(Pt 4):735–749. doi:10.1348/135910709X402612
- Tavafian SS, Gregory D, Montazeri A. The experience of low back pain in Iranian women: a focus group study. Health Care Women Int. 2008;29(4):339–348. doi:10.1080/07399330701876356
- Lin IB, O’Sullivan PB, Coffin JA, Mak DB, Toussaint S, Straker LM. ‘I am absolutely shattered’: the impact of chronic low back pain on Australian Aboriginal people. Eur J Pain. 2012;16(9):1331–1341. doi:10.1002/j.1532-2149.2012.00128.x
- Scheermesser M, Bachmann S, Schämann A, Oesch P, Kool J. A qualitative study on the role of cultural background in patients’ perspectives on rehabilitation. BMC Musculoskelet Disord. 2012;13:5. doi:10.1186/1471-2474-13-5
- Lin IB, O’Sullivan PB, Coffin JA, Mak DB, Toussaint S, Straker LM. Disabling chronic low back pain as an iatrogenic disorder: a qualitative study in Aboriginal Australians. BMJ Open. 2013;3(4):e002654. doi:10.1136/bmjopen-2013-002654
- Darlow B, Dean S, Perry M, Mathieson F, Baxter GD, Dowell A. Easy to harm, hard to heal: patient views about the back. Spine. 2015;40(11):842–850. doi:10.1097/BRS.0000000000000901
- Abebe A, Gebrehiwot EM, Lema S, Abebe TW. Prevalence of low back pain and associated risk factors among Adama Hospital Medical College Staff, Ethiopia. Eur J Prevent Med. 2015;3(6):188. doi:10.11648/j.ejpm.20150306.15
- Abraha TH, Demoz AT, Moges HG, Ahmmed AN. Predictors of back disorder among Almeda textile factory workers, North Ethiopia. BMC Res Notes. 2018;11(1):304. doi:10.1186/s13104-018-3440-4
- Belay MM. Epidemiology of low back pain among nurses working in public hospitals of Addis Ababa, Ethiopia. J Nov Physiother. 2016;6(5). doi:10.4172/2165-7025.C1.009
- Beyera GK, O’Brien J, Campbell S. Determinants of healthcare utilisation for low back pain: a population‐based study in Ethiopia. Health Soc Care Community. 2020;28(3):1058–1070. doi:10.1111/hsc.12939
- Arero AG, Arero G, Mohammed SH, Eftekhari S. Prevalence of low back pain among working Ethiopian population: a systematic review and meta-analysis. medRxiv. 2020. doi:10.1101/2020.11.29.20238170
- Beyera GK, O’Brien J, Campbell S. Profile of individuals with low back pain and factors defining chronicity of pain: a population-based study in Ethiopia. Qual Life Res. 2022;31(9):2645–2654. doi:10.1007/s11136-022-03148-5
- Arthur L, Rolan P. A systematic review of western medicine’s understanding of pain experience, expression, assessment, and management for Australian Aboriginal and Torres Strait Islander Peoples. PAIN Rep. 2019;4(6):e764. doi:10.1097/PR9.0000000000000764
- Calvo-Muñoz I, Gómez-Conesa A, Sánchez-Meca J. Prevalence of low back pain in children and adolescents: a meta-analysis. BMC Pediatr. 2013;13(1):14. doi:10.1186/1471-2431-13-14
- Morris LD, Daniels KJ, Ganguli B, Louw QA. An update on the prevalence of low back pain in Africa: a systematic review and meta-analyses. BMC Musculoskelet Disord. 2018;19(1):196. doi:10.1186/s12891-018-2075-x
- Fatoye F, Gebrye T, Odeyemi I. Real-world incidence and prevalence of low back pain using routinely collected data. Rheumatol Int. 2019;39(4):619–626. doi:10.1007/s00296-019-04273-0
- Van Rysewyk S. Meanings of Pain. Springer International Publishing; 2017. doi:10.1007/978-3-319-49022-9
- Osborn M, Rodham K. Insights into pain: a review of qualitative research. Rev Pain. 2010;4(1):2–7. doi:10.1177/204946371000400102
- Smith JA, Osborn M. Psychology and Health Pain as an assault on the self: an interpretative phenomenological analysis of the psychological impact of chronic benign low back pain. Psychol Health. 2007;22(5):517–534. doi:10.1080/14768320600941756
- Darlow B, Dowell A, Baxter GD, Mathieson F, Perry M, Dean S. The enduring impact of what clinicians say to people with low back pain. Ann Fam Med. 2013;11(6):527–534. doi:10.1370/afm.1518
- Osborn M, Smith JA. The personal experience of chronic benign lower back pain: an interpretative phenomenological analysis. Br J Health Psychol. 1998;3(1):65–83. doi:10.1111/j.2044-8287.1998.tb00556.x
- Snelgrove S, Edwards S, Liossi C. A longitudinal study of patients’ experiences of chronic low back pain using interpretative phenomenological analysis: changes and consistencies. Psychol Health. 2013;28(2):121–138. doi:10.1080/08870446.2011.630734
- Snelgrove S, Edwards S, Liossi C. Psychology & Health A longitudinal study of patients’ experiences of chronic low back pain using interpretative phenomenological analysis: changes and consistencies. Psychol Health. 2011. doi:10.1080/08870446.2011.630734
- Singh G, Newton C, O’Sullivan K, Soundy A, Heneghan NR. Exploring the lived experience and chronic low back pain beliefs of English-speaking Punjabi and white British people: a qualitative study within the NHS. BMJ Open. 2018;8(2):1–11. doi:10.1136/bmjopen-2017-020108
- Stensland ML, Sanders S. “It has changed my whole life”: the systemic implications of chronic low back pain among older adults. J Gerontol Soc Work. 2018;61(2):129–150. doi:10.1080/01634372.2018.1427169
- Osborn M, Smith JA. Living with a body separate from the self. The experience of the body in chronic benign low back pain: an interpretative phenomenological analysis. Scand J Caring Sci. 2006;20(2):216–222. doi:10.1111/j.1471-6712.2006.00399.x
- Smith JA, Larkin M, Flowers P, Larkin M. Interpretative Phenomenological Analysis: Theory, Method and Research. Los Angeles: SAGE; 2009.
- Pietkiewicz I, Smith JA, Pietkiewicz I, Smith JA. A practical guide to using Interpretative Phenomenological Analysis in qualitative research psychology. Cz Psych Psychol J. 2014;20(1):7–14. doi:10.14691/cppj.20.1.7
- Smith JA, Osborn M. Interpretative phenomenological analysis as a useful methodology for research on the lived experience of pain. Bri J Pain. 2015;9(1):41–42. doi:10.1177/2049463714541642
- World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/JAMA.2013.281053
- Nigusie A, Azale T, Yitayal M, Derseh L, Ortega JA. Institutional delivery and associated factors in rural communities of Central Gondar Zone, Northwest Ethiopia. PLoS One. 2021;16(7):e0255079. doi:10.1371/JOURNAL.PONE.0255079
- Hale ED, Trehame GJ, Kitas GD. Qualitative methodologies II: a brief guide to applying Interpretative phenomenological analysis in musculoskeletal care. Musculoskelet Care. 2008;6(2):86–96. doi:10.1002/msc.113
- Van Manen M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy. Routledge; 1990.
- Stensland M, Sanders S. Living a life full of pain: older pain clinic patients’ experience of living with chronic low back pain. Qual Health Res. 2018;28(9):1434–1448. doi:10.1177/1049732318765712
- Van Manen M. Phenomenology of practice: meaning-giving methods in phenomenological research and writing (developing qualitative inquiry); 2014. Available from: https://ocul-qu.primo.exlibrisgroup.com/discovery/openurl?institution=01OCUL_QU&vid=01OCUL_QU:QU_DEFAULT&url_ver=Z39.88-2004&rft.genre=book&rfr_id=info:sid%2Fliteratum:sage&rft.aulast=vanManen&rft.aufirst=M&rft.date=2014&rft.btitle=Phenomenologyofpract. Accessed February 21, 2021.
- Given L. Probes and Probing. In: The SAGE Encyclopedia of Qualitative Research Methods. SAGE Publications, Inc.; 2012. doi10.4135/9781412963909.n340
- Côté A-M, Durand M-J, Tousignant M, Poitras S. Physiotherapists and use of low back pain guidelines: a qualitative study of the barriers and facilitators. J Occup Rehabil. 2009;19(1):94–105. doi:10.1007/s10926-009-9167-2
- van Nes F, Abma T, Jonsson H, Deeg D. Language differences in qualitative research: is meaning lost in translation? Eur J Ageing. 2010;7(4):313–316. doi:10.1007/s10433-010-0168-y
- Van Manen M. Hermeneutic Phenomenological Reflection. In: Researching Lived Experience: Human Science for an Action Sensitive Pedagogy. Routledge; 2018.
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
- Bunzli S, Smith A, Schütze R, Lin I, O’Sullivan P. Making Sense of low back pain and pain-related fear. J Orthop Sports Phys Ther. 2017;47(9):628–636. doi:10.2519/jospt.2017.7434
- Bunzli S, Watkins R, Smith A, Schütze R, O’Sullivan P. Lives on hold: a qualitative synthesis exploring the experience of chronic low-back pain. Clin J Pain. 2013;29(10):907–916. doi:10.1097/AJP.0b013e31827a6dd8
- Abebe T. The Ethiopian “Family Collective” and Child Agency’. Barn Nr. 2008;3:89–108.
- Ethiopian culture - core concepts. Cultural Atlas. Available from: https://culturalatlas.sbs.com.au/ethiopian-culture/ethiopian-culture-core-concepts. Accessed May 17, 2021.
- Charmaz K. Loss of self: a fundamental form of suffering in the chronically ill. Sociol Health Illn. 1983;5(2):168–195. doi:10.1111/1467-9566.ep10491512
- Benzies KM, Allen MN. Symbolic interactionism as a theoretical perspective for multiple method research. J Adv Nurs. 2001;33(4):541–547. doi:10.1046/j.1365-2648.2001.01680.x
- Jackson JE. Stigma, liminality, and chronic pain: mind-body borderlands. Am Ethnol. 2005;32(3):332–353. doi:10.1525/ae.2005.32.3.332
- Cohen M, Quintner J, Buchanan D, Nielsen M, Guy L. Stigmatization of patients with chronic pain: the extinction of empathy. Pain Med. 2011;12(11):1637–1643. doi:10.1111/j.1526-4637.2011.01264.x
- Bowman JM. Reactions to chronic low back pain. Issues Ment Health Nurs. 1994;15(4):445–453. doi:10.3109/01612849409006920
- Campbell C, Guy A. “Why can’t they do anything for a simple back problem?” A qualitative examination of expectations for low back pain treatment and outcome. J Health Psychol. 2007;12(4):641–652. doi:10.1177/1359105307078171
- Holloway I, Sofaer B, Walker J. The transition from well person to “pain afflicted” patient: the career of people with chronic back pain. Illn Crisis Loss. 2000;8(4):373–387. doi:10.1177/105413730000800403
- Slade SC, Molloy E, Keating JL. Stigma experienced by people with nonspecific chronic low back pain: a qualitative study. Pain Med. 2009;10(1):143–154. doi:10.1111/j.1526-4637.2008.00540.x
- Ware NC. Suffering and the social construction of illness: the delegitimation of illness experience in chronic fatigue syndrome. Med Anthropol Q. 1992;6(4):347–361. doi:10.1525/maq.1992.6.4.02a00030
- Naushad N, Dunn LB, Muñoz RF, Leykin Y. Depression increases subjective stigma of chronic pain. J Affect Disord. 2018;229:456–462. doi:10.1016/j.jad.2017.12.085
- Corbett M, Foster NE, Ong N. Living with low back pain-Stories of hope and despair. Soc Sci Med. 2007;65:1584–1594. doi:10.1016/j.socscimed.2007.06.008
- Kirmayer LJ, Sartorius N. Cultural models and somatic syndromes. Psychosom Med. 2007;69:832–840. doi:10.1097/PSY.0b013e31815b002c
- LaCaille L, Patino-Fernandez AM, Monaco J, et al. Explanatory models of illness. In: Encyclopedia of Behavioral Medicine. Springer New York; 2013:733–734. doi:10.1007/978-1-4419-1005-9_1400
- Dedeli O, Kaptan G. Spirituality and religion in pain and pain management. Health Psychol Res. 2013;1(3):29. doi:10.4081/hpr.2013.e29
- Chenot JF, Greitemann B, Kladny B, Petzke F, Pfingsten M, Schorr SG. Clinical practice guideline: non-specific low back pain. Dtsch Arztebl Int. 2017;114(51–52):883–890. doi:10.3238/arztebl.2017.0883
- Underwood MR, Harding G, Klaber Moffett J. Patient perceptions of physical therapy within a trial for back pain treatments (UK BEAM) [ISRCTN32683578]. Rheumatology. 2006;45(6):751–756. doi:10.1093/rheumatology/kei254
- Paulo HF, Ferreira ML, Maher CG, Refshauge KM, Latimer J, Adams RD. The therapeutic alliance between clinicians and patients predicts outcome in chronic low back pain. Phys Ther. 2013;93(4):470–478. doi:10.2522/ptj.20120137
- Dezutter J, Wachholtz A, Corveleyn J. Prayer and pain: the mediating role of positive re-appraisal. J Behav Med. 2011;34(6):542–549. doi:10.1007/s10865-011-9348-2
- Wachholtz AB, Pearce MJ. Does spirituality as a coping mechanism help or hinder coping with chronic pain? Curr Pain Headache Rep. 2009;13(2):127–132. PMID: 19272278. doi:10.1007/s11916-009-0022-0
- Koenig HG. Religion, spirituality, and health: the research and clinical implications. ISRN Psychiatry. 2012;2012:1–33. doi:10.5402/2012/278730
- Olsen M, Jensen NK, Tesfaye M, Holm L. Conceptual equivalence of WHOQOL-HIV among people living with HIV in Ethiopia. Qual Life Res. 2013;22(2):361–367. doi:10.1007/s11136-012-0141-7
- Hussen SA, Tsegaye M, Argaw MG, Andes K, Gilliard D, Del Rio C. Spirituality, social capital and service: factors promoting resilience among Expert Patients living with HIV in Ethiopia. Glob Public Health. 2014;9(3):286–298. doi:10.1080/17441692.2014.880501
- Chen X, Stanton B, Gong J, Fang X, Li X. Personal Social Capital Scale: an instrument for health and behavioral research. Health Educ Res. 2008;24(2):306–317. doi:10.1093/her/cyn020
- Eriksson M. Social capital and health--implications for health promotion. Glob Health Action. 2011;4:5611. doi:10.3402/gha.v4i0.5611
- Onyeka TC, Chukwuneke FN. Pain research in Africa: a ten-year bibliometric survey. J Anesth. 2013;28(4):511–516. doi:10.1007/S00540-013-1767-5