
Abstract
Chronic musculoskeletal pain (CMP), defined as persistent discomfort in musculoskeletal tissues persisting for over 3 months, afflicts an estimated 1.71 billion people globally, leading to significant functional impairments and psychological distress, thereby detrimentally affecting individuals’ quality of life. The objective of this narrative review is to elucidate the complex relationship among dietary habits, sarcopenia, and gut microbiota composition, with an eye toward enhancing patient management and outcomes. Given the burgeoning interest in the influence of diet on CMP, a detailed examination of the current literature is warranted. Nutritional intake is a critical determinant of the gut microbiota profile, which, in turn, is linked to musculature integrity and performance, potentially leading to sarcopenia. The development of sarcopenia can aggravate CMP owing to diminished muscular strength and functionality. Additionally, disruptions in the gut microbiota may directly modulate nociception, intensifying CMP manifestations. Thus, nutritional optimization emerges as a viable approach to CMP management. Emphasizing a diet conducive to a healthy gut microbiome could forestall or mitigate sarcopenia, thereby attenuating CMP intensity. Nevertheless, the domain calls for further empirical exploration to unravel the nuances of these interactions and to forge efficacious dietary strategies for individuals with CMP. Beyond mere analgesia, comprehensive patient care for CMP requires acknowledgment of the complex and multifactorial nature of pain and its foundational elements. Embracing an integrative treatment model allows healthcare practitioners to promise better patient prognoses, enriched life quality, and a decrease in the sustained healthcare costs associated with CMP.
Plain Language Summary
Chronic musculoskeletal pain (CMP) is long-lasting pain in the bones, muscles, and joints, and it’s a common problem affecting over 1.7 billion people worldwide. This kind of pain can really disrupt someone’s daily life, making it hard to do everyday things and causing a lot of stress.
This review is like a deep dive into how eating habits, muscle loss, and the tiny organisms living in our guts all connect to this pain. As we are becoming more curious about how food affects CMP, it’s important to look closely at what we already know.
What we eat can change the tiny bugs in our guts, which has a big impact on our muscles. If our muscles get weak and shrink (a condition called sarcopenia), it can make CMP worse because weak muscles cannot support our bodies well. Also, if the balance of bugs in our gut is off, it might even make us feel pain more intensely. So, changing what we eat might be a good way to tackle CMP. Eating foods that keep our gut bugs happy might help prevent muscle loss and reduce pain. But we still need to do more research to understand this better and to figure out the best foods to eat for this purpose.
Treating CMP is not just about getting rid of the pain; it’s about looking at the whole picture and all the things that contribute to the pain. By considering everything — from our diet to our muscles to our gut bugs — doctors can help improve the lives of people with CMP, making them more comfortable and possibly reducing medical costs in the long run.
Introduction
Chronic musculoskeletal pain (CMP) is characterized by pain experienced in the musculoskeletal tissues for a duration of more than 3 months.Citation1,Citation2 CMP is accompanied by notable functional disability and emotional distress, significantly impacting an individual’s quality of life (QoL).Citation3
The prevalence of CMP is widespread, affecting approximately 1.71 billion individuals worldwide.Citation4 This condition places a substantial burden on personal well-being, social engagement, and healthcare systems. The pain is often linked to various musculoskeletal disorders, including osteoarthritis (OA), rheumatoid arthritis, and chronic low back pain (cLBP), among others.Citation5 Musculoskeletal conditions rank as the primary cause of disability on a global scale, with low back pain (LBP) standing out as the leading contributor to disability in 160 countries.Citation6
The economic implications of this condition are significant, with substantial healthcare expenditures, loss of productivity, and disability-related costs.Citation7 Aging demographics, sedentary lifestyles, and diverse lifestyle factors contribute to the steady rise in the prevalence of CMP.Citation8 This escalating prevalence has prompted growing concerns among healthcare professionals and researchers, leading them to explore innovative and comprehensive approaches to its management.Citation9 As a result, the search for alternative and complementary therapeutic strategies has gained traction in recent years.Citation10
In the ever-evolving field of pain management, nutrition has emerged as a central, modifiable factor influencing CMP.Citation11 Recent evidence highlights the profound impact of dietary choices and nutrient intake on the development, progression, and management of CMP. Unhealthy dietary behavior leading to overweight and obesity is a critical aspect of nutritional status in CMP patients.Citation12,Citation13 Emerging research into the microbiota, which is directly influenced by diet, highlights numerous possible mechanistic contributors to its potential role in pain.Citation14–16 Sarcopenia, a condition of muscle degeneration linked to nutritional imbalances, has also been associated with the presence of CMP.Citation14–16 Therefore, the impact of nutrition, along with the interplay regulated by factors such as the microbiota and sarcopenia, presents new avenues for therapeutic strategies that could complement traditional treatments.Citation9
With the growing interest in the potential impact of nutrition on CMP, there arises a need for a comprehensive review of the existing evidence. Although reviews on this topic can be found in the literature, recently published studies show the importance of this condition, and a different perspective on the topic may necessitate the need for a new review.Citation11,Citation17 This narrative review aims to shed light on the intricate interplay between nutrition, sarcopenia, and microbiota, paving the way for improved patient care and outcomes.
Chronic Pain as Bio-Psycho-Social Phenomenon
Chronic pain is increasingly understood as a complex interplay of biological, psychological, and social factors, moving away from the outdated notion that pain intensity directly correlates with tissue damage.Citation18 Introduced by George Engel in 1977, the biopsychosocial model has transformed our understanding of chronic conditions, such as musculoskeletal pain, emphasizing the intertwined roles of psychological states, societal influences, and biological mechanisms in pain perception and management.Citation19 Over the past few decades, this model has been extensively supported by research, leading to a more nuanced and holistic approach to pain treatment that considers the individual’s broader life context for more effective therapeutic outcomes.Citation20
Chronic Pain Impacts on Patient QoL
The burden and impact of CMP on an individual’s QoL warrant significant attention and should not be underestimated. Studies have shown that patients grappling with persistent pain often experience functional limitations that hinder daily activities and reduce their independence.Citation21 Moreover, it is noteworthy that these mobility restrictions, difficulties in performing household chores, and limitations in occupational activities can lead to frustration, loss of productivity, and social isolation for these patients,Citation22 further worsening their life situation.
Not only is the physical dimension of QoL affected by CMP, but the psychological toll is also significant.Citation23 CMP patients may grapple with anxiety, depression, and a sense of helplessness as they confront the challenges posed by unrelenting pain.Citation24 The emotional distress associated with chronic pain can further exacerbate the perception of pain itself, creating a vicious cycle that impairs both physical and mental well-being.Citation25
Chronic Pain is One of the Most Important Causes of Disability in the World and Loss of Productivity
According to the Global Burden of Disease Study 2019, CMP conditions rank as the foremost contributor to years lost due to disability on a global scale.Citation26 In this regard, it should also be highlighted that current data might potentially underrepresent the actual prevalence and subsequent burden of CMP conditions, suggesting an even higher incidence and burden than currently acknowledged.Citation27 This impact in disability, as noted in recent projections, is anticipated to escalate in the coming years, particularly in tandem with the ongoing trend of increasing life expectancy globally.Citation26 The economic repercussions of the health detriments linked to persistent CMP are substantial, not just for the afflicted individual but also for their familial circle, with significant implications for personal and societal well-being. Factors such as an inability to sustain consistent employment,Citation28 augmented absenteeism owing to ailments, and an uptick in inactivity stemming from disability or premature retirement all contribute to the financial strain associated with CMP.Citation29 The economic strain imposed by persistent CMP spans various facets, from diminished earnings at the individual level, reduced governmental tax inflows, and increased demand on state welfare provisions to expenses shouldered by healthcare systems.Citation30 Given that numerous occupational tasks necessitate optimal musculoskeletal function, CMP ailments are predominant culprits for work-related absences.Citation31 In addition, the fiscal ramifications of lost workdays and health-induced early retirements are considerable. Impairments related to CMP can significantly curtail work efficiency,Citation32 culminating in health-induced retirement for as many as 15% of the impacted populace.Citation33
Most Frequent Types of Chronic Pain: Focus on LBP OA
According to the Global Burden of Disease (GBD) 2019 study data, LBP is a prominent concern within the realm of musculoskeletal conditions, with an overwhelming 570 million cases documented globally.Citation34 This equates to 7.4% of the global years lived with disability (YLDs). Among other significant musculoskeletal conditions are OA, which affects 528 million individuals (accounting for 19 million YLDs), fractures with a prevalence in 440 million individuals (equivalent to 26 million YLDs), and neck pain, impacting 222 million individuals and contributing to 22 million YLDs.Citation34 The global burden is further compounded by amputations, rheumatoid arthritis, gout, and various other musculoskeletal conditions, which are represented by 180 million (5.5 million YLDs), 18 million (2.4 million YLDs), 54 million (1.7 million YLDs), and 453 million cases (38 million YLDs), respectively.Citation34
LBP not only signifies a considerable public health issue but also poses occupational challenges, leading to substantial professional, economic, and societal implications. Estimates suggest that up to 84% of the global population will experience at least one episode of LBP in their lifetime, characterized by a high recurrence rate.Citation35 Acute LBP is the second leading cause for seeking medical consultations in general practice, while its chronic form is ranked eighth.Citation35 One in every five LBP episodes culminates in sick leave, with LBP being accountable for 30% of extended sick leaves spanning over six months and 20% of work-related injuries.
As stated, OA, a condition targeting synovial joints, is the second most prevalent CMP worldwide.Citation34 Population-based cohort studies revealed that the lifetime risk of symptomatic hand OA is 47.2% in women and 24.6% in men.Citation36 Concurrently, it has been estimated that one in four individuals may encounter symptomatic hip OA during their lifetime.Citation37 As a predominant source of disability among the elderly population, OA also incurs substantial societal costs.Citation38 The medical expenditure for OA in several high-income nations is estimated to constitute 1−2.5% of their gross domestic product, with surgeries, such as hip and knee joint replacements, accounting for the majority of these healthcare expenses.Citation38
Patient Profile with Chronic Pain Due to LBP and OA
CMP is linked to specific risk factors and patient demographics. In the case of cLBP, the prevalence appears to escalate with age, reaching its zenith between 35 and 55 years.Citation39 A recent systematic review has elucidated prognostic factors for pain chronicity in LBP cases.Citation40 Notably, heightened pain intensity, increased body weight, occupational heavy lifting, challenging work postures, and depression emerge as predominant risk factors for cLBP.Citation40 Additionally, maladaptive behavioral strategies, prevalent anxiety, functional impediments during episodes, smoking habits, and notably, physical labor have also been established as direct predictors of pain chronicity in LBP.Citation40
Although the primary symptom attributable to OA is joint pain, a comprehensive understanding of the determinants of joint-related pain in OA patients remains scant.Citation41 The degree to which structural abnormalities in OA influence pain perception has been a matter of debate.Citation42 Weak correlations were observed between the severity of radiographic OA and pain, though this discordance decreases with advanced radiographic stages.Citation42 It is well-known that radiographs do not provide specific insights into which structural damages contribute to pain.Citation42 However, MRI studies suggest that bone marrow lesions, synovitis, and effusions might be significant contributors.Citation42 In addition, different studies have found that other determinants, including higher BMI, pain hypervigilance, depressed mood, lack of weekly moderate-intensity activity, and unfavorable subjective health status are significant factors contributing to current arthritic pain in OA patients.Citation41
Nutrition and Chronic Pain
Why Nutrition/Diet Influence Chronic Pain
The association between nutrition and CMP has become a subject of increasing interest in recent years ().Citation11 Adequate nutritional intake plays a crucial role in modulating pain perception, managing inflammation, and promoting overall well-being.Citation43 Unhealthy dietary behaviors and a poor diet have been implicated in predicting, perpetuating, or contributing to CMP.Citation43 For instance, individuals with chronic pain often exhibit high levels of obesity, excessive calorie consumption, and diets rich in sugar, fat, sodium, and caffeine.Citation43 Adopting a healthier diet may have significant implications for managing chronic pain and reducing inflammation.Citation44 By promoting the consumption of nutrient-dense and anti-inflammatory foods, healthcare professionals can play a vital role in enhancing the overall well-being and QoL of patients with chronic musculoskeletal diseases.Citation45
Table 1 Impact of Diet on Chronic Musculoskeletal Pain
Numerous studies have explored the link between diet and the incidence of OA. Data from the Framingham cohort and the Osteoarthritis Initiative demonstrated a negative correlation between dietary fiber intake and the risk of symptomatic OA.Citation46,Citation47 Further analysis suggested that this association between fiber intake and OA risk was partly influenced by BMI and C-reactive protein (CRP) levels.Citation53 In this study, the authors found that a higher BMI, associated with lower fiber intake, leads to higher CRP levels, which could induce symptomatic OA according to the data analysis results.Citation53 Similarly, another longitudinal analysis, utilizing the Osteoarthritis Initiative database, revealed a significant reduction in the risk of worsening pain and symptomatic knee OA with higher adherence to the Mediterranean diet.Citation48 Two additional studies were conducted in this area, utilizing the dietary inflammatory index (DII®), a scoring algorithm that classifies individuals’ diets based on their inflammatory potential.Citation54 Both studies arrived at similar conclusions; Liu et al found that a higher inflammatory potential of the diet increased the risk of knee OA,Citation49 while Tonelli et al found significant associations between DII scores and an increased risk of OA symptoms (joint pain, aching, and stiffness) in the past year, low back pain, and any pain lasting longer than 24 hours, after adjusting for potential confounders.Citation50
In relation to cLBP, Pasdar et al discovered that greater adherence to a high protein dietary pattern, characterized by elevated intake of red and white meat, legumes, nuts, and eggs, was linked to a lower prevalence of chronic LBP in both crude and adjusted models.Citation51 Conversely, after accounting for the potential confounding factors mentioned, individuals in the highest category of an energy-dense diet were positively associated with chronic LBP compared to those in the lowest category.Citation51
Several studies have verified that implementing nutritional changes, such as modifying dietary patterns, consuming certain nutrients, and adjusting meal frequency, can offer considerable relief for individuals suffering from chronic pain ().Citation45 These interventions act through various molecular systems that enhance neural function and adaptability, leading to effects comparable to those of antidepressants.Citation55 Furthermore, nutritional interventions could provide relief for musculoskeletal conditions and also address their underlying causes, leading to improved overall health status for individuals.Citation56 These positive outcomes might be connected to clinical advantages and may be attributed to the dietary influence on central nervous system sensitization, which affects pain hypersensitivity.Citation57
Table 2 Specific Nutritional Interventions and Their Impact on Chronic Pain
In 2022, a systematic review examined the effectiveness of various dietary approaches, including intermittent fasting, time-restricted feeding, caloric restriction, the ketogenic diet, and the Mediterranean diet, as part of treatment plans for improving health and CMP.Citation52 The review analyzed 16 articles, consisting of 11 randomized controlled trials (RCTs) and five observational studies. Due to different inclusion criteria, the articles selected for this review are not repeated with those mentioned above.Citation56 Notably, six of these studies reported an improvement in pain assessment, while two indicated contrasting results. Four studies demonstrated a reduction in inflammation, with one study showing no significant change. Additionally, five studies indicated an improvement in the quality of life. This systematic review also concludes that, overall, the selected studies displayed good methodological quality in their assessment scales.Citation52
The previous reviews encompassed studies that focused on various CMP diseases. However, among these conditions, OA has received the most attention in terms of interventional nutritional studies, with a wealth of evidence available in the literature. In 2023, an umbrella review conducted a comprehensive analysis, synthesizing and comparing data from five systematic reviews and meta-analyses covering evidence-based dietary practices aimed at improving OA symptoms.Citation58 The findings of this umbrella review strongly supported the Mediterranean diet as an effective approach for enhancing OA-related outcomes.Citation58 These improvements include alleviating pain, reducing stiffness, mitigating inflammation, and even addressing biomarkers associated with cartilage degeneration.Citation58 Conversely, there was limited to no evidence supporting the beneficial effects of fruits and herbs on these OA-related symptoms.Citation58
Although the overall lack of homogeneity between the studies limits the conclusions of the reviews and highlights the need for quality research that can identify consumer-accessible foods to improve CMP symptoms,Citation52,Citation58 the vast body of evidence showcases promising findings. Diverse dietary approaches and specific food components have demonstrated the potential to reduce pain and inflammation while enhancing the overall health and well-being of affected individuals. As this field of study progresses, further investigations with larger sample sizes and rigorous methodologies will help solidify these findings and pave the way for more effective and personalized approaches to managing CMP through nutrition.
Nutrition/Diet are Important for Microbiota
The microbiota refers to the community of microorganisms present in a specific environment.Citation59 In an average adult male, the human gut microbiome contains approximately 3.8×1013 microbes, surpassing the number of human host cells, which stands at about 3.0×1013.Citation60 To underscore its significance, while the human genome comprises around 23,000 genes, the microbiome encodes over three million, leading to the production of thousands of metabolites.Citation61 These metabolites effectively replace many of the host’s functions, playing pivotal roles in determining the host’s health, fitness, and phenotype.Citation61 Given this immense complexity, the gut microbiome is nowadays considered a virtual organ within the human body.
Gut microbes are instrumental in numerous aspects of human health, encompassing immune, metabolic, and neurobehavioral functions.Citation62 Notably, specific foods and dietary patterns can modulate the abundance and types of bacteria in the gut, which subsequently impacts health. A well-structured and diverse gut microbiota is paramount for sustaining optimal health. Conversely, dysbiosis—characterized by diminished diversity and compositional alterations in the gut microbiota—is correlated with conditions such as obesity, diabetes, and gastrointestinal diseases.Citation63 Notably, dietary choices heavily influence the human gut microbiota’s composition and function,Citation64 emphasizing the pivotal role of nutrition in gut health.
Dietary fiber emerges as a crucial nutrient for preserving gut microbiota diversity.Citation65 Interestingly, diets prevalent in industrialized nations, which are typically low in fiber but high in fats and protein, contribute significantly to the reduction of fiber-metabolizing microbes.Citation65 In addition, it is worth noting that certain minor dietary components, such as polyphenols and the micronutrient selenium, can promote the proliferation of beneficial bacterial species.Citation62 In contrast, numerous other components like specific food additives and alcohol might compromise the intestinal barrier, potentially triggering a leaky gut and leading to dysbiosis.Citation62
Microbiota and Its Impact on Chronic Pain
Emerging evidence suggests that the gut microbiota plays a significant role in modulating pain perception ().Citation15 Although still in its early stages, emerging research highlights the involvement of the gut microbiota in the release of signal molecules, such as metabolites, neurotransmitters, and neuromodulators, which play a direct role in pain transmission and modulation.Citation66 This has given rise to the concept of a microbiota-gut-brain axis, which involves a network of connections encompassing multiple biological systems that facilitate bidirectional communication between gut bacteria and the brain.Citation67 This axis is crucial for maintaining the homeostasis of the gastrointestinal, central nervous, and microbial systems in animals.Citation67 Although initially discovered for its involvement in visceral pain, recent findings have unveiled that the microbiota also plays a role in CMP.Citation68
Table 3 Microbiota and Its Role in Chronic Pain
Studies investigating the association between microbiota and pain have revealed intriguing findings. Gut dysbiosis, an imbalance in the composition of gut microorganisms, has been linked to an increased risk of developing chronic pain conditions.Citation69 Dysbiosis can lead to an altered gut barrier function and increased permeability, facilitating the translocation of bacteria and microbial products into the bloodstream.Citation69 This process triggers systemic inflammation and immune activation, potentially contributing to chronic pain.Citation69
In the domain of CMP, the link between the microbiome and OA has garnered considerable attention and investigation in the existing scientific literature. A Dutch study discovered significant correlations between gut microbiota composition and knee OA, even after adjusting for various factors such as smoking, alcohol intake, and BMI.Citation70 The study found an association between an increased presence of Streptococcus species in stool samples and the severity of knee OA along with heightened knee pain. While the precise mechanisms by which the Streptococcus species contribute to joint inflammation remain unidentified, the researchers hypothesized that the process could be mediated by metabolites or membrane vesicles produced by these bacteria in the gastrointestinal tract. Ultimately, the findings suggest that modulating gut microbiota could offer a novel therapeutic strategy for managing OA-related knee pain.
In a cohort study conducted by Huang et al,Citation71 involving 25 patients, the researchers investigated the relationship between lipopolysaccharide (LPS), a proinflammatory component of Gram-negative bacteria, and the severity of inflammation, symptoms, and radiographic abnormalities in knee OA. The study revealed the presence of LPS in both synovial fluid and serum of the knee, and it showed a significant correlation with the abundance of activated macrophages in the knee, the severity of radiographic OA, and joint symptoms.Citation71
In another study, a large cohort was compared to examine symptomatic vs asymptomatic hand OA.Citation72 The researchers found differences in the abundance of specific bacterial species in the symptomatic hand pain group, indicating potential gut microbiota-related metabolic dysfunction linking systemic inflammation to OA pain symptoms.
For obese subjects with and without low back pain, one study has explored the association between LBP and gut microbiota composition.Citation73 A significantly higher abundance of Adlercreutzia, Roseburia, and Uncl. Christensenellacae was found by Dekker Nitert et al in obese and overweight individuals with back pain compared to controls.Citation73 In the same line, Su and collaborators have performed a two-sample Mendelian randomization study, resulting in confirming the potential causal effect of specific gut microbiota and gut microbial metabolites on low back pain, therefore providing the theoretical basis for further explorations of targeted prevention strategies.Citation74
Nutrition/Diet as One of the Risk Factors for Sarcopenia
Sarcopenia, denoted by the age-associated decrease in muscle mass and strength, is notably prevalent among older adults, leading to substantial personal and economic implications.Citation75 Although the decline in muscle mass is an inherent component of aging, the variance in its progression across individuals points to the potential role of adjustable factors, primarily diet and lifestyle ().Citation76 Alarmingly, malnutrition, which includes both overnutrition and undernutrition, has gained global attention.Citation77 Present data indicates that approximately one-fourth of adults aged 65 years and above are either malnourished or at imminent risk.Citation78 The situation is even graver in hospital settings, with reported undernutrition rates soaring up to 72%.Citation79 These figures accentuate the pressing need to redress nutritional imbalances in seniors, which could be instrumental in the development of sarcopenia.
Table 4 Nutrition and Sarcopenia – Risk Factors and Impacts
Regarding the current state of dietary interventions, results from randomized controlled trials underscore the prospective advantages of dietary protein in combating sarcopenia and muscle deterioration.Citation80 Initial data also points to the potential efficacy of vitamin D in managing sarcopenia, although optimal dosing, administration protocols, and treatment durations are yet to be firmly established.Citation81 Other nutrients, including essential minerals, leucine, β-hydroxy-β-methylbutyric acid, vitamin C, vitamin E, omega-3 fatty acids, collagen peptides, creatine, inorganic nitrate, polyphenols omega-3 fatty acids and probiotics have also been studied, and are considered potential interventions in the management of sarcopenia.Citation82 Furthermore, adherence to a Mediterranean dietary pattern, along with augmented consumption of fruits and vegetables, has been linked to enhanced physical performance, potentially safeguarding against muscle atrophy, sarcopenia, and the onset of frailty.Citation86
Sarcopenia and His Impact on Chronic Pain
The discussion on musculoskeletal disorders and malnutrition would be incomplete without addressing the subject of sarcopenia. Sarcopenia, characterized by the depletion of muscle mass and strength, is an age-related condition frequently linked to reduced mobility and diminished quality of life in older individuals.Citation87 Malnutrition, whether due to insufficient calorie and protein intake (undernutrition) or excessive intake (overnutrition and obesity), is a common cause of sarcopenia.Citation88 In recent years, researchers have begun to unravel a potential relationship between sarcopenia and CMP, which represents a substantial public health burden worldwide.Citation89 Understanding the intricate interplay between sarcopenia and CMP is crucial for developing effective preventive and therapeutic interventions.
Several studies have covered the association between sarcopenia and CMP. In patients diagnosed with lumbar spinal stenosis, sarcopenia has shown correlations with an increased degree of vertebral slippage, heightened intensity of lower back pain, and a higher incidence of dyslipidemia and cardiovascular disease.Citation83,Citation84 In the same line, a retrospective cohort study underscored that grip strength values, a widely-used parameter to diagnose sarcopenia, are associated with the risk of falls among patients undergoing decompression and fusion procedures for lumbar spinal stenosis.Citation85 Moreover, another investigation has revealed an elevated risk of shoulder pain in individuals diagnosed with sarcopenia. However, it is less likely to be associated with severe rotator cuff pathology, such as tendon tears.Citation89 Additionally, an investigation involving older adults with multimorbidity demonstrated a meaningful association between sarcopenia and CMSP.Citation90 In this study, sarcopenia patients were observed to experience more painful sites. They reported greater pain severity and interference scores, further elucidating the potential impact of sarcopenia on musculoskeletal health, with implications for pain-related outcomes and functional decline in those affected.Citation90
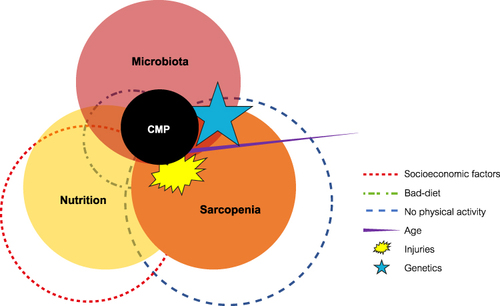
Both sarcopenia and CMP share a number of risk factors, such as advanced age, physical inactivity, and comorbidities.Citation40,Citation91 These shared risk factors may act synergistically to exacerbate the clinical manifestations of both conditions. Furthermore, emerging evidence suggests that certain pathophysiological mechanisms, including inflammation and oxidative stress, may underlie the simultaneous occurrence of sarcopenia and CMP.Citation9,Citation40,Citation91 ()
Figure 1 Interrelation of sarcopenia, malnutrition, and chronic musculoskeletal pain and their risk factors.
Management of the Patient with CMP
The Importance of the Therapeutical Goal: Not Only Pain Reduction
In CMP management, the clinical goal is not always complete pain elimination, as some underlying conditions may not be entirely curable.Citation92 Instead, the focus is on achieving an acceptable level of pain that allows the patient to lead a functional life with a satisfactory QoL.Citation92 The patient-acceptable symptom state (PASS) has been introduced as a means of addressing partial symptomatic remission.Citation93 It involves a clinically significant threshold, determined from the patient’s perspective, which allows for the classification of patients as either being in an “acceptable state” (with the outcome score meeting the PASS) or not (with the outcome score not meeting the PASS).Citation92 This approach permits the inclusion of the patient’s opinion on their health status, both at the group level and in daily clinical practice, providing insights into their perceived well-being and allowing differentiation between treatment responders and non-responders.Citation94 Consequently, the PASS is a pertinent and research-worthy concept that encompasses low disease activity, well-being, and partial symptom remission.Citation94
Focus on Multi-Modal Approach and Interdisciplinarity
CMP often requires a collaborative and integrated approach involving various healthcare professionals.Citation95 Multidisciplinary and interdisciplinary pain management teams may include pain specialists, physical therapists, psychologists, nutrition specialists, and other relevant experts.Citation96 Although similar in some aspects, it is essential to highlight the key differences between multidisciplinarity and interdisciplinarity in patient management.Citation97 Multidisciplinarity involves the incorporation of diverse professionals, each contributing their expertise within the confines of their respective fields.Citation97 In contrast, interdisciplinarity entails the coordination and collaboration of these various disciplines toward a unified and coherent approach.Citation97 Both multidisciplinarity and interdisciplinarity imply a multi-modal management approach that involves using multiple treatment modalities to address the complexities of CMP effectively.Citation97 Integrating various therapeutic strategies, such as pharmacological interventions, physical therapy, psychological support, and lifestyle changes, can lead to a more comprehensive and patient-centered model of healthcare.Citation20 Considering the intricate and multifaceted nature of CMP, an integrated approach to patient management is highly recommended.Citation9
Role of the Pharmacological Therapy
Pharmacological interventions play a significant role in managing CMP, but they are rarely used as stand-alone treatments.Citation95
Integrative management strategies, encompassing both pharmacological and non-pharmacological modalities, are essential in the therapeutic approach to pain. Within the scope of CMP, it is recommended that initial interventions prioritize non-pharmacological options, such as patient-engaged home exercise regimens and comprehensive rehabilitation programs involving multiple disciplines. Should these non-pharmacological strategies prove insufficient, the introduction of pharmacological agents, specifically nonsteroidal anti-inflammatory drugs (NSAIDs), ought to be contemplated as the principal therapeutic recourse, which may be supplemented with or without additional adjunct therapies.Citation9
Opioids are commonly prescribed for moderate to severe pain.Citation98,Citation99 Nonetheless, their prescription should be reserved exclusively for specific chronic non-cancer pain syndromes when conventional non-pharmacological and pharmacological therapeutic strategies have proven ineffective in carefully monitored individuals within the framework of a comprehensive, multi-modal, and interdisciplinary treatment approach.Citation98,Citation99 However, their potential for dependence, tolerance, and adverse effects warrants cautious use and close monitoring.Citation98,Citation99 The role of pharmacological treatments is often functional to the activity of other non-pharmacological therapeutic approaches.Citation100 For instance, medications may be utilized to provide pain relief and facilitate patients’ participation in non-pharmacological interventions like physiotherapy and exercise programs.Citation100 Conversely, successful non-pharmacological interventions may reduce the need for high-dose medications, mitigating their potential side effects.Citation95
Role of the Non-Pharmacological Therapy
Non-pharmacological approaches form an integral part of comprehensive pain management for chronic musculoskeletal conditions.Citation101 Physiotherapy plays a crucial role in improving mobility, strength, and flexibility while reducing pain and disability.Citation102 Exercise programs tailored to the individual’s needs can enhance the patient’s functional capacity and contribute to long-term pain relief.Citation103
Psychological interventions, such as cognitive-behavioral therapy (CBT), aim to modify maladaptive thought patterns and coping strategies, empowering patients to better manage their pain and emotional well-being.Citation104 Additionally, patient education on pain management, including nutritional education, equips individuals with self-management skills and fosters a sense of empowerment in their journey toward recovery.Citation105
Attention to Nutrition as an Important Factor for Microbiota and Muscle
In the intricate web of human physiology, nutrition stands out as a foundational pillar influencing various bodily systems. Among these, the connection between nutrition, gut microbiota, and muscle health has sparked significant interest in the medical and scientific communities. Our daily dietary choices, ranging from the macronutrients we consume to the micronutrients we might overlook, can profoundly impact the gut microbial community. This diverse ecosystem, comprising trillions of microorganisms, not only aids in digestion but also contributes to our overall health in ways we are still unraveling. Moreover, the balance of our gut microbiota is directly linked to muscle health and function. An imbalance, or dysbiosis, can lead to increased inflammation, which has been associated with muscle atrophy and weakness. Conversely, a balanced gut microbiota, achieved through optimal nutrition, can support muscle protein synthesis, enhance muscle growth, and improve physical performance.
Nutrition plays a pivotal role in supporting tissue repair, reducing inflammation, and optimizing overall physical and mental well-being.Citation106 Poor nutrition is a recognized precursor to dysbiosis and sarcopenia,Citation107 both of which may predispose individuals to the onset and exacerbation of CMP.Citation9,Citation40,Citation69,Citation91 Hence, a strategically devised nutritional plan becomes paramount. From a nutritional perspective, while diet plays an undeniable role, it may not be adequate in isolation due to mechanisms of metabolic decay that remain elusive and lead to sarcopenia.Citation108 Emphasizing early muscle preservation is vital, which can be achieved through early detection, utilizing tools like the SARC-Calf scale, and incorporating appropriate supplementation when indicated. Proper dietary choices, along with potential supplementation when indicated, can complement other therapeutic interventions and enhance treatment outcomes in chronic pain patients.Citation109
By integrating nutrition into the management plan, healthcare professionals can foster a comprehensive and patient-centered approach that addresses the diverse needs of individuals with CMP.Citation11 This integration underscores the importance of considering the CMP as a whole, recognizing the interconnectedness of biological, psychological, and social aspects, and paving the way for improved patient outcomes and enhanced overall well-being.Citation95
Diet Integration in the Multi-Modal Treatment: Proper Diet for Less Inflammation/Pain: Focus on Microbiota and Sarcopenia
Microbiota: Maintain the Right Equilibrium with Probiotic and Prebiotic
Probiotics and prebiotics are among the most commonly used substances in attempts to alter the microbiota.Citation110 Probiotics are defined as live microorganisms that confer health benefits to the host when administered in adequate amounts, while prebiotics are substances that promote the growth or function of beneficial microorganisms, including bacteria and fungi.Citation110 The use of both pre- and pro-biotics has been explored in the field of CMP treatment.
Probiotic supplementation has been associated with reduced pain severity and improved functional outcomes in patients with CMP.Citation111 In a clinical trial with individuals with knee OA, Lei et al found that after 6 months of Lactobacillus casei Shirota supplementation, pain scores were significantly reduced, suggesting the potential use of this supplement as a new option for knee OA therapy.Citation112 In another study, Lyu et al conducted a trial using Streptococcus thermophilus (TCI633), and although there were no significant changes in certain biomarkers, the distinct pain scores indicated that TCI633 might slow the progression of knee OA.Citation113 Furthermore, Taye et al showed in an N-of-1 trial that probiotic intervention was associated with lower pain scores, suggesting the role of probiotics in pain relief for OA patients.Citation114 Research on probiotics and other CMP conditions was also conducted.
Regarding prebiotics, in the context of CMP, Coulson et al conducted a study to analyze the impact of green-lipped mussel extract (GLM) and glucosamine sulfate (GS) supplementation on the gut microbiome of knee OA patients.Citation115 Both groups showed significant improvements in OA symptoms and gastrointestinal symptoms after 12 weeks of intervention. Although changes in the gut microbiome were not significant, there was a notable decrease in Clostridia sp., which correlated with reduced inflammation and improvement in OA and gastrointestinal symptoms.Citation115
Sarcopenia: Prevention, Early Diagnosis, Less Severity
Prevention and treatment of sarcopenia could lead to a positive impact on CMP symptoms. Reducing muscle mass may cause more prolonged pain, leading to further reductions in activity and, therefore, sustained pain, creating a vicious cycle. In this context, several diagnostic scales for sarcopenia are available and should be considered for the early diagnosis of CMP patients.Citation116 In this regard, a recent study by Tsuji et al has shown that both SARC-F and SARC-CalF demonstrated moderate diagnostic capabilities in a CMP population.Citation117 SARC-CalF, however, exhibited higher diagnostic power compared to SARC-F. Moreover, both SARC-F and SARC-CalF scores correlated with Psychotic Depression Assessment Scale (PDAS) scores, signifying pain-related disability. This suggests that they can serve as screening tools for sarcopenia and also as simple tools to assess disability in patients with CMP. Another recent study by Tsuji and collaborators found that the phase angle may be a valid discriminator of sarcopenia in patients with CMP. They even indicated established cutoff points that clinicians can follow.Citation118 In this study, the phase angle showcased high accuracy in differentiating sarcopenia in men and moderate accuracy in both genders and women. Moreover, although data has not been published yet for CMP patients, other instruments to identify sarcopenia can be used, including the Asian Working Group for Sarcopenia (AWGS) criteria for sarcopenia diagnosis,Citation119 and those proposed by the European Working Group for Sarcopenia in Older People 2 (EWGSOP2),Citation87 or the International Working Group on Sarcopenia (IWGS).Citation120
It’s important to highlight the importance of early diagnosis in CMP patients. In patients with CMP, sarcopenia was identified even in those under 65 years of age.Citation117 This implies that muscle deterioration is not exclusively a concern for the elderly. Recognizing sarcopenia at an earlier stage could lead to better management and interventions. With several instruments and scales available to diagnose sarcopenia, there is a strong argument for their adoption in routine screenings for sarcopenia in patients with CMP. Implementing these scales during the early diagnosis phases will allow healthcare providers to offer timely interventions, potentially improving the quality of life and management outcomes for CMP patients.
In managing CMP patients diagnosed with sarcopenia, a multifaceted intervention approach is crucial to address both pain and muscle wasting. Amino acids play a pivotal role in muscle protein synthesis, with essential amino acids, particularly leucine, being shown to stimulate muscle growth and prevent muscle protein breakdown. Incorporating protein powders, whether from vegetable or dairy origins, can help meet the elevated protein requirements of these patients. Vegetable-based proteins, such as pea or rice protein, offer an alternative for those with lactose intolerance or those who prefer plant-based sources, while dairy-derived proteins like whey and casein are known for their high biological value and rich amino acid profiles. Additionally, superoxide dismutase (SOD) has been researched for its potential antioxidative properties. Superoxide dismutase aids in the dismutation of superoxide radicals in the body, potentially combating oxidative stress, which is believed to play a role in muscle degeneration. Thus, the integration of these nutritional supplements, in conjunction with physical therapy and medical management, can be an effective strategy to mitigate the effects of sarcopenia in CMP patients.
Conclusion
In conclusion, the management of CMP demands a multi-modal and multidisciplinary approach, underlining the paramount importance of nutrition in treatment management. The relationship between nutrition, microbiota, and sarcopenia plays a pivotal role in CMP patients. Nutritional patterns influence gut microbiota composition, which in turn affects muscle health and function, leading to sarcopenia. The onset of sarcopenia can exacerbate CMP due to decreased muscle strength and function. Moreover, gut microbiota imbalance can directly influence pain perception, amplifying the effects of CMP. Therefore, optimizing nutrition could serve as a potential strategy for managing CMP. Focusing on a balanced diet that supports a healthy gut microbiome may prevent or alleviate sarcopenia and, in turn, reduce the severity of CMP. However, this field necessitates further research to fully understand the complex interplay and to develop effective nutritional interventions for CMP patients. In addition, it is to be highlighted that effective patient management with CMP encompasses more than just pain control. It is imperative to understand the multifaceted nature of pain and its underlying components. Comprehensive care involves recognizing the physical, emotional, and psychological aspects of pain. Additionally, addressing the unique needs and concerns of the patient is crucial. By adopting a holistic approach, healthcare providers can ensure improved patient outcomes, enhanced quality of life, and a reduction in long-term healthcare burdens.
Expert opinions stress the value of a practical approach that factors in nutrition’s pivotal role, along with the gut microbiota and other determinants, in influencing pain perception and overall health. Healthcare professionals should prioritize nutrition as a central element of comprehensive patient care and seamlessly integrate it into standard practice. The forward-thinking idea of modulating gut microbiota through dietary and pharmabiotic measures heralds promising avenues for optimizing CMP management. By delving into these cutting-edge strategies, we can amplify the efficacy of pharmacological treatments and enrich patient outcomes. Committing to an in-depth appreciation of nutrition’s influence in CMP, coupled with a patient-centric stance, will lay the groundwork for more adept and all-encompassing pain management protocols. As our expertise in this realm grows, we eagerly anticipate shaping the future of chronic pain management and elevating the well-being of those afflicted by CMP.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
Medical writing and Editorial Assistance was provided by Jesús Loureiro Álvarez, PhD, Flavia Nicora MD, Aashni Shah, BSc, and Massimiliano Pianta (Polistudium srl, Italy).
Additional information
Funding
References
- Treede R-D, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–1007. doi:10.1097/j.pain.0000000000000160
- Treede R-D, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
- Wittkopf PG, Zomkowski K, Cardoso FL, Sperandio FF. The effect of chronic musculoskeletal pain on several quality of life dimensions: a critical review. Int J Ther Rehabil. 2017;24(8):327–336. doi:10.12968/ijtr.2017.24.8.327
- Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2021;396(10267):2006–2017. doi:10.1016/S0140-6736(20)32340-0
- Bonanni R, Cariati I, Tancredi V, Iundusi R, Gasbarra E, Tarantino U. Chronic pain in musculoskeletal diseases: do you know your enemy? J Clin Med. 2022;11(9):2609. doi:10.3390/jcm11092609
- Musculoskeletal health. Available from: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions. Accessed July 25, 2023.
- Woolf A. Musculoskeletal health, wealth and business, and wider societal impact. Eur J Public Health. 2022;32(5):831–833. doi:10.1093/eurpub/ckac087
- Blyth FM, Briggs AM, Schneider CH, Hoy DG, March LM. The global burden of musculoskeletal pain-where to from here? Am J Public Health. 2019;109(1):35–40. doi:10.2105/AJPH.2018.304747
- El-Tallawy SN, Nalamasu R, Salem GI, LeQuang JAK, Pergolizzi JV, Christo PJ. Management of musculoskeletal pain: an update with emphasis on chronic musculoskeletal pain. Pain Ther. 2021;10(1):181–209. doi:10.1007/s40122-021-00235-2
- Johnson MA, Cosgrove CD. Complementary and alternative medicine for chronic musculoskeletal pain. Fed Pract. 2015;32(9):31–36.
- Elma Ö, Yilmaz ST, Deliens T, et al. Chronic musculoskeletal pain and nutrition: where are we and where are we heading? PM R. 2020;12(12):1268–1278. doi:10.1002/pmrj.12346
- Mendonça CR, Noll M, de Carvalho Santos ASEA, Rodrigues APDS, Silveira EA. High prevalence of musculoskeletal pain in individuals with severe obesity: sites, intensity, and associated factors. Korean J Pain. 2020;33(3):245–257. doi:10.3344/kjp.2020.33.3.245
- Cooper L, Ells L, Ryan C, Martin D. Perceptions of adults with overweight/obesity and chronic musculoskeletal pain: an interpretative phenomenological analysis. J Clin Nurs. 2018;27(5–6):e776–e786. doi:10.1111/jocn.14178
- Tonelli Enrico V, Vo N, Methe B, Morris A, Sowa G. An unexpected connection: a narrative review of the associations between Gut Microbiome and Musculoskeletal Pain. Eur Spine J. 2022;31(12):3603–3615. doi:10.1007/s00586-022-07429-y
- Defaye M, Gervason S, Altier C, et al. Microbiota: a novel regulator of pain. J Neural Transm. 2020;127(4):445–465. doi:10.1007/s00702-019-02083-z
- Sahin UK, Şentürk AY. Investigation of the relationship between chronic musculoskeletal pain and sarcopenia risk in community-dwelling older adults: a cross-sectional study. Ann Geriatr Med Res. 2023;27(3):250–257. doi:10.4235/agmr.23.0081
- Elma Ö, Yilmaz ST, Deliens T, et al. Do nutritional factors interact with chronic musculoskeletal pain? A systematic review. J Clin Med. 2020;9(3):702. doi:10.3390/jcm9030702
- Meints SM, Edwards RR. Evaluating psychosocial contributions to chronic pain outcomes. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(Pt B):168–182. doi:10.1016/j.pnpbp.2018.01.017
- Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–136. doi:10.1126/science.847460
- Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581–624. doi:10.1037/0033-2909.133.4.581
- Results - A meta-ethnography of patients’ experience of chronic non-malignant musculoskeletal pain - NCBI Bookshelf. Available from: https://www.ncbi.nlm.nih.gov/books/NBK262991/. Accessed July 25, 2023.
- Dueñas M, Ojeda B, Salazar A, Mico JA, Failde I. A review of chronic pain impact on patients, their social environment and the health care system. J Pain Res. 2016;9:457–467. doi:10.2147/JPR.S105892
- Crofford LJ. Psychological aspects of chronic musculoskeletal pain. Best Pract Res Clin Rheumatol. 2015;29(1):147–155. doi:10.1016/j.berh.2015.04.027
- Woo AK. Depression and Anxiety in Pain. Rev Pain. 2010;4(1):8–12. doi:10.1177/204946371000400103
- Turk DC, Wilson HD. Fear of pain as a prognostic factor in chronic pain: conceptual models, assessment, and treatment implications. Curr Pain Headache Rep. 2010;14(2):88–95. doi:10.1007/s11916-010-0094-x
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
- Tada Y, Iversen L, Koo J. Early efficacy and safety data with fixed-dose combination calcipotriol/betamethasone dipropionate foam attributed to mechanism of absorption and steroid potency. J Eur Acad Dermatol Venereol. 2021;35(Suppl 1):5–9. doi:10.1111/jdv.17027
- Ackerman IN, Ademi Z, Osborne RH, Liew D. Comparison of health-related quality of life, work status, and health care utilization and costs according to Hip and knee joint disease severity: a national Australian study. Phys Ther. 2013;93(7):889–899. doi:10.2522/ptj.20120423
- Laires PA, Canhão H, Rodrigues AM, Eusébio M, Gouveia M, Branco JC. The impact of osteoarthritis on early exit from work: results from a population-based study. BMC Public Health. 2018;18(1):472. doi:10.1186/s12889-018-5381-1
- Phillips CJ. The Cost and Burden of Chronic Pain. Rev Pain. 2009;3(1):2–5. doi:10.1177/204946370900300102
- Briggs AM, Shiffman J, Shawar YR, Åkesson K, Ali N, Woolf AD. Global health policy in the 21st century: challenges and opportunities to arrest the global disability burden from musculoskeletal health conditions. Best Pract Res Clin Rheumatol. 2020;34(5):101549. doi:10.1016/j.berh.2020.101549
- Palmer KT, Goodson N. Ageing, musculoskeletal health and work. Best Pract Res Clin Rheumatol. 2015;29(3):391–404. doi:10.1016/j.berh.2015.03.004
- Conaghan PG, Porcheret M, Kingsbury SR, et al. Impact and therapy of osteoarthritis: the Arthritis Care OA Nation 2012 survey. Clin Rheumatol. 2015;34(9):1581–1588. doi:10.1007/s10067-014-2692-1
- Global Burden of Disease (GBD). Available from: https://www.healthdata.org/research-analysis/gbd. Accessed May 28, 2024.
- Airaksinen O, Brox JI, Cedraschi C, et al. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006;15(Suppl 2):S192–300. doi:10.1007/s00586-006-1072-1
- Qin J, Barbour KE, Murphy LB, et al. Lifetime risk of symptomatic hand osteoarthritis: the Johnston County Osteoarthritis Project. Arthritis Rheumatol. 2017;69(6):1204–1212. doi:10.1002/art.40097
- Murphy LB, Helmick CG, Schwartz TA, et al. One in four people may develop symptomatic Hip osteoarthritis in his or her lifetime. Osteoarthr Cartil. 2010;18(11):1372–1379. doi:10.1016/j.joca.2010.08.005
- Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–1759. doi:10.1016/S0140-6736(19)30417-9
- Grabovac I, Dorner TE. Association between low back pain and various everyday performances: activities of daily living, ability to work and sexual function. Wien Klin Wochenschr. 2019;131(21–22):541–549. doi:10.1007/s00508-019-01542-7
- Nieminen LK, Pyysalo LM, Kankaanpää MJ. Prognostic factors for pain chronicity in low back pain: a systematic review. Pain Rep. 2021;6(1):e919. doi:10.1097/PR9.0000000000000919
- Lee KM, Chung CY, Sung KH, et al. Risk factors for osteoarthritis and contributing factors to current arthritic pain in South Korean older adults. Yonsei Med J. 2015;56(1):124–131. doi:10.3349/ymj.2015.56.1.124
- Neogi T. The epidemiology and impact of pain in osteoarthritis. Osteoarthr Cartil. 2013;21(9):1145–1153. doi:10.1016/j.joca.2013.03.018
- Elma Ö, Brain K, Dong H-J. The importance of nutrition as a lifestyle factor in chronic pain management: a narrative review. J Clin Med. 2022;11(19):5950. doi:10.3390/jcm11195950
- Brain K, Burrows TL, Bruggink L, et al. Diet and chronic non-cancer pain: the state of the art and future directions. J Clin Med. 2021;10(21):5203. doi:10.3390/jcm10215203
- Dragan S, Șerban M-C, Damian G, Buleu F, Valcovici M, Christodorescu R. Dietary patterns and interventions to alleviate chronic pain. Nutrients. 2020;12(9):2510. doi:10.3390/nu12092510
- Dai Z, Lu NA, Niu J, Felson DT, Zhang Y. Dietary fiber intake in relation to knee pain trajectory. Arthritis Care Res. 2017;69(9):1331–1339. doi:10.1002/acr.23158
- Dai Z, Niu J, Zhang Y, Jacques P, Felson DT. Dietary intake of fibre and risk of knee osteoarthritis in two US prospective cohorts. Ann Rheum Dis. 2017;76(8):1411–1419. doi:10.1136/annrheumdis-2016-210810
- Veronese N, Koyanagi A, Stubbs B, et al. Mediterranean diet and knee osteoarthritis outcomes: a longitudinal cohort study. Clin Nutr. 2019;38(6):2735–2739. doi:10.1016/j.clnu.2018.11.032
- Liu Q, Hebert JR, Shivappa N, et al. Inflammatory potential of diet and risk of incident knee osteoarthritis: a prospective cohort study. Arthritis Res Ther. 2020;22(1):209. doi:10.1186/s13075-020-02302-z
- Tonelli Enrico V, Hébert JR, Mugford G, et al. Assessing diet and musculoskeletal pain in adults: results from a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES). Am J Lifestyle Med;2023. 15598276231189682. doi:10.1177/15598276231189682
- Pasdar Y, Hamzeh B, Karimi S, et al. Major dietary patterns in relation to chronic low back pain; a cross-sectional study from RaNCD cohort. Nutr J. 2022;21(1):28. doi:10.1186/s12937-022-00780-2
- Cuevas-Cervera M, Perez-Montilla JJ, Gonzalez-Muñoz A, Garcia-Rios MC, Navarro-Ledesma S. The effectiveness of intermittent fasting, time restricted feeding, caloric restriction, a ketogenic diet and the Mediterranean diet as part of the treatment plan to improve health and chronic musculoskeletal pain: a systematic review. Int J Environ Res Public Health. 2022;19(11):6698. doi:10.3390/ijerph19116698
- Dai Z, Jafarzadeh SR, Niu J, et al. Body mass index mediates the association between dietary fiber and symptomatic knee osteoarthritis in the osteoarthritis initiative and the Framingham Osteoarthritis Study. J Nutr. 2018;148(12):1961–1967. doi:10.1093/jn/nxy231
- Shivappa N, Steck SE, Hurley TG, Hussey JR, Hébert JR. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014;17(8):1689–1696. doi:10.1017/S1368980013002115
- Manchishi SM, Cui RJ, Zou XH, Cheng ZQ, Li BJ. Effect of caloric restriction on depression. J Cell Mol Med. 2018;22(5):2528–2535. doi:10.1111/jcmm.13418
- Mendonça CR, Noll M, Castro MCR, Silveira EA. Effects of nutritional interventions in the control of musculoskeletal pain: an integrative review. Nutrients. 2020;12(10):3075. doi:10.3390/nu12103075
- Nijs J, Elma Ö, Yilmaz ST, et al. Nutritional neurobiology and central nervous system sensitisation: missing link in a comprehensive treatment for chronic pain? Br J Anaesth. 2019;123(5):539–543. doi:10.1016/j.bja.2019.07.016
- Buck AN, Vincent HK, Newman CB, et al. Evidence-based dietary practices to improve osteoarthritis symptoms: an umbrella review. Nutrients. 2023;15(13):3050. doi:10.3390/nu15133050
- Berg G, Rybakova D, Fischer D, et al. Microbiome definition re-visited: old concepts and new challenges. Microbiome. 2020;8(1):103. doi:10.1186/s40168-020-00875-0
- Sender R, Fuchs S, Milo R. Revised estimates for the number of human and bacteria cells in the body. PLoS Biol. 2016;14(8):e1002533. doi:10.1371/journal.pbio.1002533
- Bull MJ, Plummer NT. Part 1: the human gut microbiome in health and disease. Integr Med. 2014;13(6):17–22.
- Zhang P. Influence of foods and nutrition on the gut microbiome and implications for intestinal health. Int J Mol Sci. 2022;23(17). doi:10.3390/ijms23179588
- DeGruttola AK, Low D, Mizoguchi A, Mizoguchi E. Current understanding of dysbiosis in disease in human and animal models. Inflamm Bowel Dis. 2016;22(5):1137–1150. doi:10.1097/MIB.0000000000000750
- Nova E, Gómez-Martinez S, González-Soltero R. The influence of dietary factors on the gut microbiota. Microorganisms. 2022;10(7):1368. doi:10.3390/microorganisms10071368
- Cronin P, Joyce SA, O’Toole PW, O’Connor EM. Dietary fibre modulates the gut microbiota. Nutrients. 2021;13(5):1655. doi:10.3390/nu13051655
- Guo R, Chen L-H, Xing C, Liu T. Pain regulation by gut microbiota: molecular mechanisms and therapeutic potential. Br J Anaesth. 2019;123(5):637–654. doi:10.1016/j.bja.2019.07.026
- Morais LH, Schreiber HL, Mazmanian SK. The gut microbiota–brain axis in behaviour and brain disorders. Nat Rev Microbiol. 2021;19(4):241–255. doi:10.1038/s41579-020-00460-0
- Minerbi A, Gonzalez E, Brereton NJB, et al. Altered microbiome composition in individuals with fibromyalgia. Pain. 2019;160(11):2589–2602. doi:10.1097/j.pain.0000000000001640
- Garvey M. The association between dysbiosis and neurological conditions often manifesting with chronic pain. Biomedicines. 2023;11(3):748. doi:10.3390/biomedicines11030748
- Boer CG, Radjabzadeh D, Medina-Gomez C, et al. Intestinal microbiome composition and its relation to joint pain and inflammation. Nat Commun. 2019;10(1):4881. doi:10.1038/s41467-019-12873-4
- Huang ZY, Stabler T, Pei FX, Kraus VB. Both systemic and local lipopolysaccharide (LPS) burden are associated with knee OA severity and inflammation. Osteoarthr Cartil. 2016;24(10):1769–1775. doi:10.1016/j.joca.2016.05.008
- Wei J, Zhang C, Zhang Y, et al. Association between gut microbiota and symptomatic hand osteoarthritis: data from the Xiangya Osteoarthritis Study. Arthritis Rheumatol. 2021;73(9):1656–1662. doi:10.1002/art.41729
- Dekker Nitert M, Mousa A, Barrett HL, Naderpoor N, de Courten B. Altered gut microbiota composition is associated with back pain in overweight and obese individuals. Front Endocrinol. 2020;11:605. doi:10.3389/fendo.2020.00605
- Su M, Tang Y, Kong W, Zhang S, Zhu T. Genetically supported causality between gut microbiota, gut metabolites and low back pain: a two-sample Mendelian randomization study. Front Microbiol. 2023;14:1157451. doi:10.3389/fmicb.2023.1157451
- Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39(4):412–423. doi:10.1093/ageing/afq034
- Robinson S, Cooper C, Aihie Sayer A. Nutrition and sarcopenia: a review of the evidence and implications for preventive strategies. J Aging Res. 2012;2012:510801. doi:10.1155/2012/510801
- Lepre B, Laur C, Johnsen JT, et al. A 2020 evaluation of global knowledge networks in the UN decade of action on nutrition (2016–2025). In: Proceedings of the 6th International Summit on Medical and Public Health Nutrition Education and Research; 2022.
- Crichton M, Craven D, Mackay H, Marx W, de van der Schueren M, Marshall S. A systematic review, meta-analysis and meta-regression of the prevalence of protein-energy malnutrition: associations with geographical region and sex. Age Ageing. 2019;48(1):38–48. doi:10.1093/ageing/afy144
- Heersink JT, Brown CJ, Dimaria-Ghalili RA, Locher JL. Undernutrition in hospitalized older adults: patterns and correlates, outcomes, and opportunities for intervention with a focus on processes of care. J Nutr Elder. 2010;29(1):4–41. doi:10.1080/01639360903574585
- Hickson M. Nutritional interventions in sarcopenia: a critical review. Proc Nutr Soc. 2015;74(4):378–386. doi:10.1017/S0029665115002049
- Uchitomi R, Oyabu M, Kamei Y. Vitamin D and sarcopenia: potential of vitamin D supplementation in sarcopenia prevention and treatment. Nutrients. 2020;12(10):3189. doi:10.3390/nu12103189
- Liu S, Zhang L, Li S. Advances in nutritional supplementation for sarcopenia management. Front Nutr. 2023;10:1189522. doi:10.3389/fnut.2023.1189522
- Matsuo S, Kawakami M, Minetama M, et al. Clinical features of sarcopenia in patients with lumbar spinal stenosis. Spine. 2020;45(17):E1105–E1110. doi:10.1097/BRS.0000000000003498
- W-t W, Lee T-M, Han D-S, Chang K-V. The prevalence of sarcopenia and its impact on clinical outcomes in lumbar degenerative spine disease-a systematic review and meta-analysis. J Clin Med. 2021;10(4). doi:10.3390/jcm10040773
- Kwon J-W, Lee BH, Lee S-B, et al. Hand grip strength can predict clinical outcomes and risk of falls after decompression and instrumented posterolateral fusion for lumbar spinal stenosis. Spine J. 2020;20(12):1960–1967. doi:10.1016/j.spinee.2020.06.022
- Papadopoulou SK, Detopoulou P, Voulgaridou G, et al. Mediterranean diet and sarcopenia features in apparently healthy adults over 65 years: a systematic review. Nutrients. 2023;15(5):1104. doi:10.3390/nu15051104
- Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
- AlMohaisen N, Gittins M, Todd C, Burden S, Hussain SM. What is the overlap between malnutrition, frailty and sarcopenia in the older population? Study protocol for cross-sectional study using UK Biobank. PLoS One. 2022;17(12):e0278371. doi:10.1371/journal.pone.0278371
- Han D-S, W-T W, Hsu P-C, Chang H-C, Huang K-C, Chang K-V. Sarcopenia is associated with increased risks of rotator cuff tendon diseases among community-dwelling elders: a cross-sectional quantitative ultrasound study. Front Med. 2021;8:630009. doi:10.3389/fmed.2021.630009
- Sit RWS, Zhang D, Wang B, et al. Sarcopenia and chronic musculoskeletal pain in 729 community-dwelling Chinese older adults with multimorbidity. J Am Med Dir Assoc. 2019;20(10):1349–1350. doi:10.1016/j.jamda.2019.04.009
- Papadopoulou SK. Sarcopenia: a contemporary health problem among older adult populations. Nutrients. 2020;12(5):1293. doi:10.3390/nu12051293
- Tubach F, Ravaud P, Martin-Mola E, et al. Minimum clinically important improvement and patient acceptable symptom state in pain and function in rheumatoid arthritis, ankylosing spondylitis, chronic back pain, hand osteoarthritis, and Hip and knee osteoarthritis: results from a prospective multin. Arthritis Care Res. 2012;64(11):1699–1707. doi:10.1002/acr.21747
- Tubach F, Ravaud P, Baron G, et al. Evaluation of clinically relevant states in patient reported outcomes in knee and Hip osteoarthritis: the patient acceptable symptom state. Ann Rheum Dis. 2005;64(1):34–37. doi:10.1136/ard.2004.023028
- Wariaghli G, Allali F, Berrada K, et al. The patient acceptable symptom state of chronic musculoskeletal pain measured on a Visual Analog Scale in Moroccan patients. Pain Med. 2013;14(1):103–109. doi:10.1111/j.1526-4637.2012.01529.x
- Mallick-Searle T, Sharma K, Toal P, Gutman A. Pain and function in chronic musculoskeletal pain-treating the whole person. J Multidiscip Healthc. 2021;14:335–347. doi:10.2147/JMDH.S288401
- Giusti EM, Castelnuovo G, Molinari E. Differences in multidisciplinary and interdisciplinary treatment programs for fibromyalgia: a mapping review. Pain Res Manag. 2017;2017:7261468. doi:10.1155/2017/7261468
- Choi BCK, Pak AWP. Multidisciplinarity, interdisciplinarity and transdisciplinarity in health research, services, education and policy: 1. Definitions, objectives, and evidence of effectiveness. Clin Invest Med. 2006;29(6):351–364.
- Häuser W, Morlion B, Vowles KE, et al. European* clinical practice recommendations on opioids for chronic non-cancer pain–Part 1: role of opioids in the management of chronic non-cancer pain. Eur J Pain. 2021;25(5):949–968. doi:10.1002/ejp.1736
- Krcevski–škvarc N, Morlion B, Vowles KE, et al. European clinical practice recommendations on opioids for chronic non-cancer pain–part 2: special situations. Eur J Pain. 2021;25(5):969–985. doi:10.1002/ejp.1744
- Services USD of H and H. Pain management best practices inter-agency task force report: updates, gaps, inconsistencies, and recommendations. Washington, DC: US Department of Health and Human Services; 2019.
- Nijhof LN, Nap-van der Vlist MM, van de Putte EM, van Royen-Kerkhof A, Nijhof SL. Non-pharmacological options for managing chronic musculoskeletal pain in children with pediatric rheumatic disease: a systematic review. Rheumatol Int. 2018;38(11):2015–2025. doi:10.1007/s00296-018-4136-8
- Trulsson Schouenborg A, Rivano Fischer M, Bondesson E, Jöud A. Physiotherapist-led rehabilitation for patients with chronic musculoskeletal pain: interventions and promising long-term outcomes. BMC Musculoskelet Disord. 2021;22(1):910. doi:10.1186/s12891-021-04780-x
- Booth J, Moseley GL, Schiltenwolf M, Cashin A, Davies M, Hübscher M. Exercise for chronic musculoskeletal pain: a biopsychosocial approach. Musculoskeletal Care. 2017;15(4):413–421. doi:10.1002/msc.1191
- Cheng JOS, Cheng S-T, Pasin L. Effectiveness of physical and cognitive-behavioural intervention programmes for chronic musculoskeletal pain in adults: a systematic review and meta-analysis of randomised controlled trials. PLoS One. 2019;14(10):e0223367. doi:10.1371/journal.pone.0223367
- Marris D, Theophanous K, Cabezon P, Dunlap Z, Donaldson M. The impact of combining pain education strategies with physical therapy interventions for patients with chronic pain: a systematic review and meta-analysis of randomized controlled trials. Physiother Theory Pract. 2021;37(4):461–472. doi:10.1080/09593985.2019.1633714
- Sears B, Saha AK. Dietary Control of Inflammation and Resolution. Front Nutr. 2021;8:709435. doi:10.3389/fnut.2021.709435
- Bilski J, Pierzchalski P, Szczepanik M, Bonior J, Zoladz JA. Multifactorial mechanism of sarcopenia and sarcopenic obesity. role of physical exercise, microbiota and myokines. Cells. 2022;11(1):160. doi:10.3390/cells11010160
- Rubio-Ruiz ME, Guarner-Lans V, Pérez-Torres I, Soto ME. Mechanisms underlying metabolic syndrome-related sarcopenia and possible therapeutic measures. Int J Mol Sci. 2019;20(3):647. doi:10.3390/ijms20030647
- Nijs J, Tumkaya Yilmaz S, Elma Ö, et al. Nutritional intervention in chronic pain: an innovative way of targeting central nervous system sensitization? Expert Opin Ther Targets. 2020;24(8):793–803. doi:10.1080/14728222.2020.1784142
- Cunningham M, Azcarate-Peril MA, Barnard A, et al. Shaping the future of probiotics and prebiotics. Trends Microbiol. 2021;29(8):667–685. doi:10.1016/j.tim.2021.01.003
- Morreale C, Bresesti I, Bosi A, et al. Microbiota and pain: save your gut feeling. Cells. 2022;11(6):971. doi:10.3390/cells11060971
- Lei M, Guo C, Wang D, Zhang C, Hua L. The effect of probiotic Lactobacillus casei Shirota on knee osteoarthritis: a randomised double-blind, placebo-controlled clinical trial. Benef Microbes. 2017;8(5):697–703. doi:10.3920/BM2016.0207
- Lyu J-L, Wang T-M, Chen Y-H, et al. Oral intake of Streptococcus thermophil us improves knee osteoarthritis degeneration: a randomized, double-blind, placebo-controlled clinical study. Heliyon. 2020;6(4):e03757. doi:10.1016/j.heliyon.2020.e03757
- Taye I, Bradbury J, Grace S, Avila C. Probiotics for pain of osteoarthritis; An N-of-1 trial of individual effects. Complement Ther Med. 2020;54:102548. doi:10.1016/j.ctim.2020.102548
- Coulson S, Butt H, Vecchio P, Gramotnev H, Vitetta L. Green-lipped mussel extract (Perna canaliculus) and glucosamine sulphate in patients with knee osteoarthritis: therapeutic efficacy and effects on gastrointestinal microbiota profiles. Inflammopharmacology. 2013;21(1):79–90. doi:10.1007/s10787-012-0146-4
- Nishikawa H, Asai A, Fukunishi S, et al. Screening tools for sarcopenia. In Vivo. 2021;35(6):3001–3009. doi:10.21873/invivo.12595
- Tsuji H, Tetsunaga T, Tetsunaga T, et al. Evaluation of SARC-F and SARC-CalF for sarcopenia screening in patients with chronic musculoskeletal pain: a prospective cross-sectional study. Medicine. 2022;101(29):e29568. doi:10.1097/MD.0000000000029568
- Tsuji H, Tetsunaga T, Misawa H, Nishida K, Ozaki T. Association of phase angle with sarcopenia in chronic musculoskeletal pain patients: a retrospective study. J Orthop Surg Res. 2023;18(1):87. doi:10.1186/s13018-023-03567-1
- Chen L-K, Woo J, Assantachai P, et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(3):300–307.e2. doi:10.1016/j.jamda.2019.12.012
- Fielding RA, Vellas B, Evans WJ, et al. Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopenia. J Am Med Dir Assoc. 2011;12(4):249–256. doi:10.1016/j.jamda.2011.01.003