
Abstract
Purpose
It is asserted that primary dysmenorrhea/menstrual cramps only occur in ovulatory menstrual cycles. Our first objective was to present detailed menstrual cramps information in normally ovulatory versus anovulatory cycles from a single-cycle cohort study during the SARS-CoV-2 Pandemic. Secondly, we reviewed the literature for cohort studies documenting both menstrual cramps and ovulation.
Participants and Methods
The Menstruation and Ovulation Study 2 recruited 108 women ages 19–35 years to a prospective, observational single-cycle study, recording cramps daily (0–4 scale) in the Menstrual Cycle Diary© and assessing normal ovulation (luteal length ≥10 days) by the validated Quantitative Basal Temperature© (Mean Temperature Method). We searched databases for « primary dysmenorrhea » / » menstrual cramps »; « menstrual cycles »; « anovulation », finding four valid publications.
Results
In 75 women/cycles during the Pandemic, mean age was 28.5, body mass index 23.5, and higher education (16 years); 40 normally ovulatory and 35 anovulatory cycles had similar lengths (29.5–30.0 days), respectively (P=0.571). However, anovulatory cycles recorded significantly worse menstrual cramps versus normally ovulatory cycles; anovulatory median intensity was 1.9 versus 1.6, and Cramp Score was 8 versus 6 in normally ovulatory cycles (P=0.017). Four publications in 273 women (991 cycles) showed cramps in both anovulatory and ovulatory cycles; three were in adolescent/young adult women, one of which documented a significantly greater percentage of cramps in ovulatory cycles. The 694 cycles in premenopausal women (20–41 years) showed similar percentages of symptomatic cramps in cycles of both ovulatory types. Meta-analysis documented significantly higher cramp prevalence in ovulatory cycles (OR 2.10; 95% CI 1.31, 3.37; P=0.002).
Conclusion
This is the first documentation of more intense and frequent cramps in anovulatory cycles. However, meta-analysis showing the presence of symptomatic cramps in both ovulatory and anovulatory cycles documented they were twice as prevalent in ovulatory menstrual cycles.
Plain Language Summary
“Worse Menstrual Cramps in Anovulatory Cycles”. Medicine has long believed that menstrual cramps only occur in ovulatory menstrual cycles that release an egg and have high progesterone levels that decrease before the next period. The notion was that dropping progesterone levels triggered release of prostaglandins that cause the pain and uterus muscle contractions of menstrual cramps. This research studied 75 community women aged 19–35 years for a single cycle during COVID-19. Forty women had normally ovulatory cycles and 35 had anovulatory cycles with a similar mean cycle length of 29.7 days. Women in both groups were similar in age, weight, education and other reproductive characteristics. Women recorded Menstrual Cycle Diary© daily experiences for cramp presence and intensity (scored 0–4). Ovulation was documented by daily first morning temperatures analyzed by the valid Quantitative Basal Temperature© method. Results showed menstrual cramps occurred in both normally ovulatory and anovulatory cycles. Surprisingly, anovulatory compared with ovulatory cycles had cramps that lasted longer (4 rather than 3 days), were more intense (1.9 versus 1.6) and with significantly higher Cramp Scores (of 8 versus 6). We also found four other published studies showing cramps occurred in both anovulatory and ovulatory cycles. A meta-analysis of these, however, showed that cramps were twice as frequent in ovulatory cycles. These results matter because they stimulate the search for more accurate understandings of why menstrual cramps occur. They will likely stimulate more effective therapies for the rare, intense menstrual cramps that currently are not effectively treated by anti-inflammatory medicines such as ibuprofen.
Introduction
Primary dysmenorrhea refers to painful menstrual cramps that often begin in adolescence and are not caused by pelvic pathology.Citation1 Cramps usually start approximately 6–24 months after menarche,Citation1–3 with episodes beginning just before or at flow and with pain that can last for 8–72 hours.Citation1–3 Sometimes cramps are associated with vomiting, nausea, diarrhea, insomnia, and fatigue as well as pain radiating from the pelvis to the thighs and the lower back.Citation2
Australian population-based, cross-sectional data by Parker et al (2022)Citation4 quantified the impact of dysmenorrhea on 1051 senior high school students aged 15–19 years. Approximately 44.2% reported severe period pain, 35.7% reported a significant interference with daily activities and 13.7% missed school due to menstrual cramps.Citation4 An earlier population-based Canadian survey found that, of 291 public high school students aged 14–21 years, approximately 93% reported feeling menstrual discomfort, with 70% having tried over-the-counter medications to treat this discomfort.Citation5 Andersch and Milsom (1982)Citation6 studied a random sample of 656, 19-year-old women living in an urban Swedish population. They documented that 72% of women reported dysmenorrhea with 15% experiencing limitations to their daily activities and finding no improvement with analgesics.Citation6 Despite their young age of 19, the 15% whose activities were limited by pain that was nonresponsive to usual therapy may have had secondary dysmenorrhea, although most definitions require surgery or images documenting endometriosis or other pathology. Additionally, in this young Swedish population, dysmenorrhea was found to be significantly more severe in those who had an early menarche, experienced heavier menstrual flow, in nulliparous women as well as in those who had experienced a spontaneous or medical abortion.Citation6 Height, weight and regularity of menstrual cycles had no significant impact on the severity of dysmenorrhea.Citation6 Thus, population-based evidenceCitation4–6 shows that primary dysmenorrhea is common, often poorly treated, underrepresented in research and may be ignored by healthcare professionals despite being the most common gynecological condition among menstruating people.Citation1,Citation4–6
Pathogenesis of Primary Dysmenorrhea/Menstrual Cramps
Currently, overproduction of prostaglandins by the myometrium and endometrium is the explanation for primary dysmenorrhea for which there is the most evidence.Citation1,Citation7 Cells released during endometrial sloughing produce prostaglandin F2α and prostaglandin E2.Citation1,Citation7 These prostaglandins cause myometrial hypercontractility resulting in ischemia of the uterine muscle, as well as increased sensitivity of nociceptive nerve endings, respectively.Citation1,Citation7
Prostaglandins are synthesized from arachidonic acid, a process that is controlled by cyclic adenosine phosphate.Citation8 Prostaglandin production is increased through cyclic adenosine phosphate stimulation by a myriad of signals which include tissue trauma and mechanical stimuli as well as the ovarian hormones (such as estradiol and progesterone), epinephrine and peptide hormones.Citation9 Arachidonic acid is a derivative of phospholipids released by phospholipase A2, an enzyme found in lysosomes.Citation9 Lysosomal activity is adjusted by multiple factors; increased progesterone levels stabilize lysosomal activity, but decreasing progesterone removes that stabilizing effect, releasing lysosomal enzymes.Citation9 During the late luteal phase, the corpus luteum regresses alongside a decrease in progesterone and estradiol levels.Citation10 This decrease results in the release of phospholipase A2 from lysosomes in the endometrium ultimately raising arachidonic acid (the limiting factor for prostaglandin synthesis) by hydrolyzing phospholipids in the cell membrane.Citation11 Increased arachidonic acid in conjunction with tissue trauma and intracellular sloughing during menstruation results in an overproduction of prostaglandins during menstruation.Citation11
A prospective study conducted by Wilson and Kurzrok (1938)Citation12 first asserted that menstrual cramps occur only in ovulatory cycles. The data were based on 20 tracings from three women who had ovulatory bleeding, 14 tracings in one woman who had anovulatory bleeding and 38 tracings from 14 women with dysmenorrhea.
We have always noted [dysmenorrhea’s] association with an ovulatory cycle as shown by the presence of a secretory endometrium…we now believe the presence of functional dysmenorrhea indicates the occurrence of ovulation. (page 84)Citation12
This was repeated by Dawood (1981)Citation7 “The only proven endocrine factor is the occurrence of primary dysmenorrhea in ovulatory cycles”. (page 45).Citation7 However, since those important publications, there have been few studies to investigate and support that widely accepted hypothesis. Thus, there is a need to gather data and examine the role of progesterone and normal ovulation in the pathophysiology of primary menstrual cramps.
An experimental investigation by Eldering et al (1990)Citation10 used a primate model (rhesus monkey) to study the roles of progesterone and estradiol in prostaglandin release both in vivo and in vitro. This study documented, as is true in human cycles, that both estradiol and progesterone levels decrease prior to flow. They also found that endometrium obtained under the influence of high levels of estrogen produced more prostaglandins in vivo. However, the addition of estrogen in vitro did not stimulate prostaglandin production in the endometrium. These data either suggest that a potential factor(s) in the plasma works synergistically with estrogen to increase prostaglandin production or that the prostaglandin production is from the myometrium. In addition, this study abstract summarized:
Physiological concentrations of P (progesterone 5.0 ng/mL) added to cycle day 23 (luteal phase, secretory) cultures in both the absence and presence of low or high E (estradiol) markedly inhibited the high levels of PGs (prostaglandins) found in day 23 cultures (P = 0.01)Citation10
This basic animal research demonstrated that both estradiol and progesterone, plus likely other factors, are involved in stimulating prostaglandin production leading to menstrual cramps. These data emphasize the need for further research.
Women and menstruating people have an increased production of prostaglandins during the documented luteal phase relative to the follicular phase of the menstrual cycle.Citation1,Citation13 People with menstrual cramps tend to have higher levels of prostaglandins compared to people without menstrual cramps.Citation1,Citation13 These observations were confirmed through a study comparing endometrial biopsies, menstrual fluids and endometrial jet washings sampled during the luteal phase.Citation11 Although it is clear that uterine prostaglandins are related to menstrual cramps, the pathophysiology of the trigger to increased prostaglandin production remains unclear.
Evidence That Ovulatory Cycles are Necessary for Menstrual Cramps
Assuming that exposure to and a drop in luteal phase progesterone level is necessary for increased prostaglandin production, primary dysmenorrhea or menstrual cramps are thought to occur exclusively in ovulatory cycles.Citation7–11 However, there have now been four published investigations showing that the percentage of cycles with menstrual cramps does not vary between ovulatory and anovulatory cycles.Citation14–17 Each of these will be discussed in more detail below.
A cross-sectional study conducted by Espin Lopez et al, (2010)Citation14 in 166 undergraduate university students aged 17–23, demonstrated no difference in the severity of menstrual cramps as well as other symptoms between ovulatory and anovulatory cycles. This investigation utilized basal body temperature by the non-validated “smoothed curve method” to differentiate spontaneous anovulatory cycles from ovulatory cycles. A second study conducted by Seidman et al (2018)Citation15 recruited 39 adolescents and young adults experiencing primary dysmenorrhea (defined as NRS ≥4) and graded cramps using a numerical pain rating scale (NRS) of 0–10. They also studied as controls 52 women/people born with ovaries of reproductive age (PORA) with regular menstrual cycles aged 16–24 years (NRS ≤3). All participants had predictable, normal-length menstrual cycles. In this cross-sectional study, participants were asked to test urine for the luteinizing hormone (LH) surge that precedes ovulation (using either the OvuQuick® One-Step Ovulation Predictor, or the ClearBlue Digital Ovulation Test®) starting several days before predicted ovulation. They contacted investigators at the time of a positive result (meaning an LH surge of ≥40 mIU/mL). One hundred sixty-eight cycles were tracked among the 91 participants and results indicated that participants in the control group had an overall significantly higher incidence of anovulatory cycles at 37.1% compared to those with LH surge-positive ovulatory cycles (17.5%). However, within those with menstrual cramps, there was no significant difference in daily reporting of pain between anovulatory and ovulatory cycles.Citation15
A prospective cohort study conducted by Akman et al (2021)Citation16 assessed the presence of anovulation in healthy adolescent women/PORA experiencing primary dysmenorrhea or menstrual cramps. They reported regular menstruation and were between the ages of 11 to 18 years. Intensity of menstrual pain was assessed using the numerical rating scale (NRS). The control group included women/PORA experiencing grade 0 menstrual pain on the NRS. This was defined as menstruation causing no limitation to daily activities and no need for analgesic medications. Those with primary dysmenorrhea had an NRS ≥ 4, meaning a need for analgesics within the last 3 menstrual cycles, and moderate to severe primary dysmenorrhea. A suprapubic pelvic ultrasound was conducted in addition to luteal phase serum progesterone levels (with the ovulatory threshold set at 3 ng/mL) to determine whether ovulation had occurred. Results showed anovulatory cycle rates in the primary dysmenorrhea group of 31.7%, versus 44.4% in the control group. Despite this, the NRS intensity of cramps was similar during ovulatory and anovulatory cycles.
Similar results were collected in a prospective, 1-year observational community cohort study in 53 women (mean 13 cycles/woman) examining menstrual cramp occurrences and their relationship to ovulatory characteristics.Citation17 Participants in this study were healthy premenopausal women aged 21–41 years who were required to have two normal-length, normally ovulatory menstrual cycles prior to enrolment.Citation18 Each participant recorded cramp intensity in the Menstrual Cycle Diary©Citation19 (Diary) daily. To measure luteal phases and ovulation, a twice-validated Quantitative Basal Temperature©Citation20,Citation21 (QBT) analysis was used, with 10 being the minimal number of luteal phase days in a normally ovulatory cycle. Results showed that cramp intensity and duration did not vary within-woman among ovulatory and ovulatory disturbed (short luteal phase and anovulatory cycles).Citation17 In order to compare these data with the three previous studies, we have analyzed the 18 anovulatory cycles in this cohort versus all of the normally ovulatory cycles in this cohort for the presence or absence of menstrual cramps.
Thus, there are growing primary data documenting that menstrual cramps may occur in both ovulatory and anovulatory cycles.Citation14–17 Since there are suggestions that the current understanding that cramps require an ovulatory cycle is not correct, it is critical to conduct more detailed, evidence-based research.
Our primary purpose in this investigation of the relationship of primary dysmenorrhea to ovulatory characteristics was to report the intensity, duration and a Cramp Score integrating both measures in women in the Menstruation and Ovulation Study 2 (MOS2) that documented one cycle per participant, examining all normally ovulatory versus all anovulatory cycles. Our secondary purposes were to tabulate and provide a meta-analysis of data from the previously published studies on menstrual cramps and ovulation or anovulation to examine the prevalence of cramps in the two cycle types.
Materials and Methods
Study Design
This was a cross-sectional, single-cycle, community-based study of 108 menstrual cycles and ovulation with data collection (February 2020-September 2021) primarily during the lockdowns and socio-economic local restrictionsCitation22 related to the first 19 months of the SARS-CoV-2 pandemic (Pandemic).
Ethical Considerations
Each participant read and signed a consent form and passed a brief telephone screening questionnaire before being enrolled. Following faxing or email of a photo of the signed final page of the consent form participants were sent several blank copies of the Diary, a digital thermometer, plus printed instructions and links to instructional videos by postal mail. They then completed an interviewer administered questionnaire in person or via video-conferencing that collected information on demographics, health and reproductive histories, lifestyles and any medication or supplement use. The first visit, if in person, used standard methods to measure height in stocking feet, and weight on a balance beam while wearing light, indoor clothing. If they were participating remotely, participants were sent a recording form and instructions on how to record their weight and height and measure their waist circumference (using a provided paper tape).
This study protocol and its modifications to allow it to continue during the Pandemic (https://dx.doi.org/10.14288/1.0395296) were initially approved by the Clinical Research Ethics Board of the University of British Columbia (H19-02983) in October, 2019. All participants understood that what they recorded in the Menstrual Cycle Diary© (which included the menstrual cramps investigated in this study) would be analyzed. In the recruitment, conduct and recording of this research, we have complied with the principles of the Declaration of Helsinki.
Participants
Participants were 108 women with complete data, they were aged 19–35, had menstruated in the past three months prior to the study with cycles between 21 and 35 days in length. Exclusions included participants who had taken exogenous hormones within the past 3 months including estrogen, progesterone, progestin or combined hormonal contraception, or did not have approximately month-apart menstruations.
Assessment and Grading of Menstrual Cramps
Participants were provided with paper copies of the data collection tool – the Menstrual Cycle Diary©Citation19 (Diary©). This tool is organized to include the actual date and cycle day. Each woman was asked to make daily entries in the evening before bed. Menstrual cycle teaching was conducted by providing personalized written instructions as well as access to three online 10-minute videos (https://www.youtube.com/watch?v=6K9LB6afKxE).
All days within the single cycle with cramps scored as non-zero were counted to obtain the duration (including during flow and before the next flow). Data for cramp intensity were scored on a 0–4 scale, (0 = no cramps, 1 = minimal, 2 = moderate, 3 = moderately intense, 4 = very intense). The median cramp intensity was multiplied by the cramp duration (days per cycle) to obtain a Cramp Score.
Quantitative Basal Temperature© (QBT©) Analysis for Ovulation Documentation
Participants were provided with a digital thermometer with which they measured their daily first oral morning temperature. Temperatures were to be obtained first thing in the morning without any activity other than going to the washroom. The twice validated QBT©Citation20,Citation21 was analyzed using the Mean Temperature MethodCitation20 to determine if the cycle were normally ovulatory, had a short luteal phase or were anovulatory. Thus, the QBT©Citation20,Citation21 method can also assess luteal phase length which is determined as the length of time with temperatures higher than the mean.Citation20 In this method all the temperature records in a given cycle are averaged and the days of temperature above that average (if they remain consistently above until the day before flow) are considered the luteal phase length. On average, this temperature shift occurs approximately 24–36 hours following the LH surge.Citation20 A cycle is also determined to be anovulatory if the QBT©Citation20,Citation21 shows fewer than four days of temperatures above the cycle’s temperature average. Throughout this research, a normally ovulatory cycle is defined by our QBT© method as having a luteal phase length of ≥10 days.
Statistical Analyses
Since the purpose of this investigation was to study cramp experiences in participants who differed most in progesterone exposure, we excluded 33 short luteal phases that were part of the MOS2 data. This study analyzed ordinal menstrual cramp data using the Mann–Whitney U-test in two extreme ovulation-related groups: participants with ovulatory cycles and normal luteal phase lengths (defined as ≥10 days) and those with anovulatory cycles.
Demographic, anthropomorphic, reproductive health, and exercise variables were assessed for normal distribution, with results expressed as mean (95% confidence interval) or median (range) across the two extreme ovulatory-status groups in women. All baseline characteristics were compared between the two groups of women/PORA with cycles at the extremes of ovulation. Statistically appropriate tests were conducted to identify differences between the normally ovulatory (LL≥10 days) and anovulatory groups using the independent sample t-Test and Mann–Whitney U-test in normally distributed data versus data that are not, respectively. Statistical analyses were performed with SPSS version 29 (IBM Corp. 2022. IBM SPSS Statistics for Windows, New York).
We identified that two participants in MOS2 reported being diagnosed with endometriosis. Since endometriosis and secondary dysmenorrhea are etiologically associated, we performed a sensitivity analysis excluding those two cycles. A probability of, or less than, 0.05 was considered likely important.
We have also identified four publications documenting the proportion of cycles with problematic menstrual cramps (NRS ≥4),Citation15,Citation16 upper quartile of the Menstrual Symptom Questionnaire,Citation14 or cramp intensity of 2–4Citation17) in ovulatory and anovulatory cycles. We extracted data from these sources to allow a comprehensive meta-analysis on cramp occurrences (in percentages) across all ovulatory (including short luteal phases) and all anovulatory cycles. Utilizing the Cochrane analysis tool Review Manager (RevMan; Computer program), Version 5.4, we computed the pooled odds ratio along with a 95% confidence interval [CI]. Our analysis employed a random-effects model, and statistical heterogeneity was assessed using the I2 statistic.
Results
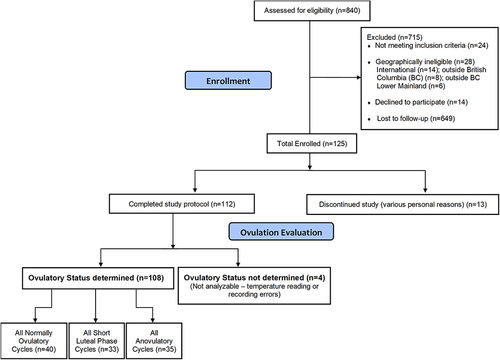
The flow of participants each with a single cycle, from recruitment to documentation of ovulatory characteristics in 108 women, is shown in . All normally ovulatory and anovulatory cycles are compared for menstrual cramp characteristics in this analysis. Participant characteristics, including demographics, anthropomorphic and reproductive measures, were examined in the 40 women with normally ovulatory cycles and the 35 women with anovulation cycles (). In general, the women participants (since they so gender self-identified) averaged aged 28.6 ± 3.9 years, had a normal weight for height (body mass index, BMI) of 23.7 ± 4.0, were very well educated (median of 16 years) with just fewer than half being non-White. Two participants in MOS2 reported being diagnosed with endometriosis, making it likely their cramps were not primary dysmenorrhea. Menstrual cycle lengths were similar (at 29.5 days in ovulatory and 30 days in anovulatory cycles). Likewise, parity, age at menarche and past months of combined hormonal contraceptive use were all similar.
Table 1 Demographic, Anthropomorphic, and Reproductive Characteristics of Women in Menstrual and Ovulation Study 2 Who Experienced Normally Ovulatory (Luteal Phase Length ≥10 Days) and Anovulatory Cycles
Figure 1 This Diagram shows the Flow of Participants in the Menstruation Ovulation Study 2 from first Contact to the Cramp Analyses in only the Normally Ovulatory and Anovulatory Cycles.
Menstrual Cramp Variables by Normally Ovulatory versus Anovulatory Cycles in MOS2
summarizes three menstrual cramp variables including cramp duration (days per cycle), cramp intensity (0–4) and the resulting Cramp Score (duration times intensity). Results showed that all three menstrual cramp parameters were significantly more frequent, more intense and had higher Cramp Scores in the anovulatory cycles compared with normally ovulatory ones. Cramp duration was longer by one day in anovulatory cycles (P = 0.04). Cramp intensity was also higher in anovulatory cycles with a median value of 1.9 (1.0–3.0) compared to 1.6 (0.0–3.0) (P = 0.026). The Cramp Score was also significantly higher (P = 0.017) in anovulatory cycles; normally ovulatory cycles had a Cramp Score of 6.0 (0.0–25.0) versus the 8.0 (1.0–54.0) in anovulatory ones.
Table 2 Menstrual Cramp Variables in Women with Normally Ovulatory and Anovulatory Cycles from the Menstrual Cycle and Ovulation Study 2 (MOS2)
Given that endometriosis is associated with secondary dysmenorrhea, the two participants with endometriosis were eliminated and a sensitivity analysis was performed; both were in the anovulatory menstrual cycle group. The sensitivity analysis results showed that cramp duration remained statistically significantly worse in anovulatory cycles (P = 0.046) as did the Cramp Score (P = 0.032); cramp intensity, however, became non-significantly different between anovulatory and normally ovulatory cycles (P = 0.056) (Supplemental Table 1).
Literature Prevalence of Primary Menstrual Cramps in Ovulatory and Anovulatory Cycles
Four previously published studies (), and 991 cycles reported by 273 women/PORA, as described earlier, reported symptomatic menstrual cramps by the ovulatory characteristics of the menstrual cycles. Three reported primary dysmenorrhea in adolescent cross-sectional or prospective cohortsCitation14–16 and one described prospective menstrual cramp experiences over approximately one year (mean of 13 cycles/woman) in 53 adult women ages 20–41.Citation17 All of the studies used different methods to document ovulation (smoothed basal body temperature curves, the presence of a urine LH surge, a 3rd week serum progesterone level of ≥3 ng/mL or QBT©). The three adolescent studies showed 47% of problematic cramps occurred in ovulatory cycles but a mean of 29% were documented in anovulatory ones. The prospective one-year study in 53 premenopausal women documented that symptomatic cramps occurred in 56% of anovulatory cycles. Thus, all studies showed that symptomatic menstrual cramps occurred in both ovulatory and anovulatory studies.
Table 3 Literature Documenting the Percentage of Cycles by Their Ovulatory Status Having Symptomatic Primary Dysmenorrhea in Adolescent and Premenopausal Menstrual Cycles
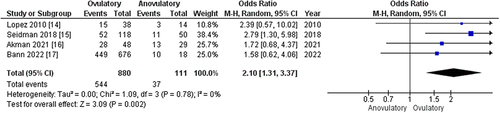
A meta-analysis of the percentage of cycles with menstrual cramps in those that were ovulatory versus anovulatory (), showed that symptomatic menstrual cramps, occurred in a statistically higher percentage in ovulatory compared with anovulatory cycles. The ovulatory cycles had an overall higher Odds Ratio of 2.10 (95% CI 1.31, 3.37; P = 0.002) for having problematic cramps.
Figure 2 This Forest Plot Illustrates the Meta-analysis of Four Publications that have Documented Symptomatic Primary Menstrual Cramps in both Ovulatory and Anovulatory Menstrual Cycles.
Discussion
In this two-part investigation we have shown that menstrual cramps are worse in anovulatory than in normally ovulatory cycles in a single-cycle cohort study in 75 women, as well as documenting in a meta-analysis of almost 1000 cycles that, although cramps are more than twice as prevalent in ovulatory cycles, they also consistently occur in anovulatory ones.Citation14–17 These two types of data about menstrual cramps call into serious question the assertion that primary dysmenorrhea only occurs in ovulatory menstrual cycles.
To the best of our knowledge, no other primary menstrual cramp data have documented menstrual cramps by the ovulatory characteristics of the menstrual cycles in which they occurred. To support these new observations, we need, but cannot yet provide, an alternate physiological explanation for the relationship of dysmenorrhea with ovarian hormone levels and their changes. The “cramps only in ovulatory cycles” concept rested on an understanding that progesterone blocked lysosomal enzymes that were released as progesterone decreased before flow, and that these lysosomal enzymes triggered prostaglandin release. However, both estradiol and progesterone levels drop prior to the onset of menstruation. Also, primate data show that high estradiol levels, at least in vitro, are associated with increased prostaglandin production.
The original investigation in 1938Citation12 did not provide mean cycle lengths for the anovulatory cycles (although it implied that they were similar in length to ovulatory ones). If these anovulatory cycles were substantially longer than the normally ovulatory ones, it is possible that estradiol levels were lower and that this related to the absence of cramps. It is clear that future studies are needed in which the potential hormonal and other variables related to prostaglandin release as well as menstrual cramp duration, intensity and Cramp Score are all documented.
There are some limitations to this research. First, only one menstrual cycle was collected per participant in the MOS2 data and thus we potentially have captured menstrual cramps during both flow and prior to the next cycle’s flow. Second, these adult data were collected while participants were experiencing the multidimensional stressors of the Pandemic, which can influence menstrual cycles,Citation22 and also increase the risk for short luteal phase and anovulatory cycles.Citation23 However, Diary© entries and temperature measurements were conducted daily which allowed for consistency across all participants. Also, in order to test the extreme range of progesterone production related to the postulated cramp etiology, we have omitted analysis of the MOS2 cramp data from the 33 ovulatory cycles with short luteal phase lengths. It is a limitation that we did not eliminate secondary dysmenorrhea in this cohort with imaging or other methods. However, we did systematically ask all participants in the baseline questionnaire if they had been diagnosed with endometriosis. We believe that these are valid diagnoses based on the Shafrir data.Citation24
Two participants reported being diagnosed with endometriosis. We have performed a sensitivity analysis in which we excluded their data. In women who had the opportunity to say they had endometriosis and did not, they presumably had primary menstrual cramps. Excluding women with endometriosis showed similar results as the primary analysis but cramp intensity became just non-significant although the cramp duration and Cramp Score remained statistically higher in anovulatory cycles. Despite this, we cannot ensure that these data are uniform in reflecting primary dysmenorrhea.
There are also limitations in the literature search and meta-analysis portion of this investigation. The four studies varied in the life phase studied (three in adolescent/young adultCitation14–16 and one in mature premenopausal womenCitation17). In addition, these studies used varying methods to document ovulation, and differently assessed symptomatic or problematic cramps. Finally, we have used revised data in this analysis; note that we have identified to editors that there was a database error and requested revision of data in a published studyCitation17 but the revision is not yet published. We compared the percentage of problematic cramps (intensity 2–4 out of 4) in all ovulatory (normally ovulatory and short luteal phase cycles) with all anovulatory cycles so that these adult, premenopausal cramp data would be similar to those in adolescents.
This study also has strengths. This is the first analysis of primary data to show that menstrual cramps or primary dysmenorrhea are more intense and frequent in anovulatory than in normally ovulatory menstrual cycles. Sensitivity analysis eliminating the two participants with diagnosed endometriosis still showed that cramp duration and Cramp Score were significantly greater in anovulatory cycles. It will be important for future studies of secondary dysmenorrhea to determine the intensity and duration of these cramps and whether or not these also occur in both ovulatory and anovulatory cycles. Additionally, our meta-analysis integrated previously published data showing that symptomatic menstrual cramps occur in both ovulatory and anovulatory cycles although remaining significantly more prevalent in ovulatory ones.
Conclusions
Previous research has asserted that ovulation is required for the presence of primary dysmenorrhea.Citation7,Citation12 However, there is now substantial evidence showing that it is possible to have menstrual cramps during anovulatory cycles.Citation14–17 Ultimately, it is likely that the progesterone-prostaglandin relationship is not the major factor related to primary dysmenorrhea. Thus, primary menstrual cramp characteristics are all significantly greater in same-length anovulatory compared with normally ovulatory menstrual cycles in well-educated community women in their late 20s and early 30s. This prompts a new era of scientific investigation into the relationships of ovarian hormones, the balance of estradiol and progesterone levels and their menstrual cycle-related changes in association with the pathophysiology of primary dysmenorrhea. These new understandings are likely to lead to more accurate physiological etiology, better prevention and more effective treatment of menstrual cramps that are a significant issue for many, especially younger women/PORA.
Abbreviations
95% CI, 95% Confidence Interval; Anovulation, absence of egg release and high progesterone levels; BMI, Body Mass Index; LH, Luteinizing Hormone; Diary©, Menstrual Cycle Diary©; MOS2, Menstruation and Ovulation Study 2; NRS, Numerical Rating Scale; PORA, People with Ovaries of Reproductive Age; QBT©, Quantitative Basal Temperature©; Pandemic, SARS-CoV-2 Pandemic.
Consent for Publication
All authors contributed importantly to this manuscript and have approved this version for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Data Sharing Statement
The MOS2 data related to menstrual cramps are available in their entirety in this manuscript. The Menstruation and Ovulation Study 2 from which these data were derived has not yet been published; these data will not be more widely available until that occurs. The literature search and meta-analysis data are included here in full.
Additional information
Funding
References
- Iacovides S, Avidon I, Baker FC. What we know about primary dysmenorrhea today: a critical review. Hum Reprod Update. 2015;21(6):762–778. doi:10.1093/humupd/dmv039
- Hofmeyr GJ, Bassin J. Dysmenorrhoea. Topic Obstetr Gynaecol. 1996;1996:269–274.
- Harel Z. Dysmenorrhea in adolescents. In: Annals of the New York Academy of Sciences. Vol. 1135. 2008. doi:10.1196/annals.1429.007
- Parker MA, Kent AL, Sneddon A, Wang J, Shadbolt B. The menstrual disorder of teenagers (MDOT) study no. 2: period impact and pain assessment (PIPPA) tool validation in a large population-based cross-sectional study of Australian teenagers. J Pediatr Adolesc Gynecol. 2022;35(1):30–38. doi:10.1016/j.jpag.2021.06.003
- Campbell MA, McGrath PJ. Use of medication by adolescents for the management of menstrual discomfort. Arch Pediatr Adolesc Med. 1997;151(9):905. doi:10.1001/archpedi.1997.02170460043007
- Andersch B, Milsom I. An epidemiological study of young women with dysmenorrhea. Am J Obstet Gynecol. 1982;144(6):655–660. doi:10.1016/0002-9378(82)90433-1
- Dawood MY. Dysmenorrhoea and Prostaglandins: pharmacological and Therapeutic Considerations. Drugs. 1981;22(1):42–56. doi:10.2165/00003495-198122010-00003
- Funk CD. Prostaglandins and leukotrienes: advances in eicosanoid biology. Science. 2001;294(5548):1871–1875. doi:10.1126/science.294.5548.1871
- Dawood MY. Dysmenorrhea. Clin Obstet Gynecol. 1990;33(1):168–178. doi:10.1097/00003081-199003000-00023
- Eldering JA, Nay MG, Hoberg LM, Longcope C, McCracken JA. Hormonal regulation of prostaglandin production by rhesus monkey endometrium. J Clin Endocrinol Metab. 1990;71(3):596–604. doi:10.1210/jcem-71-3-596
- Dawood MY. Primary dysmenorrhea: advances in pathogenesis and management. Obstetrics Gynecol. 2006;108(2):428–441. doi:10.1097/01.AOG.0000230214.26638.0c
- Wilson L, Kurzrok R. Studies on the motility of the human uterus in vivo. Endocrinology. 1938;23(1):79–86. doi:10.1210/endo-23-1-79
- Pickles VR. PROSTAGLANDINS AND DYSMENORRHEA: historical Survey. Acta Obstet Gynecol Scand. 1979;58(87 S):7–12. doi:10.3109/00016347909157782
- Espín López L, Carrillo Verdejo E, González Javier F, Ordoñana Martín JR, Gómez-Amor J. Incidence of anovulatory menstrual cycles among dysmenorrheic and non-non-dysmenorrheic [corrected] women: effects on symptomatology and mood. Psicothema. 2010;22(4):654–658.
- Seidman LC, Brennan KM, Rapkin AJ, Payne LA. Rates of anovulation in adolescents and young adults with moderate to severe primary dysmenorrhea and those without primary dysmenorrhea. J Pediatr Adolesc Gynecol. 2018;31(2):94–101. doi:10.1016/j.jpag.2017.09.014
- Akman AO, Bozdag G, Pehlivantürk-Kizilkan M, Akgul S, Derman O, Kanbur N. Menstrual cycle pain is independent of ovulation in adolescents with primary dysmenorrhea. J Pediatr Adolesc Gynecol. 2021;34(5):635–642. doi:10.1016/j.jpag.2021.04.001
- Bann S, Goshtasebi A, Shirin S, Prior JC. A one-year observational cohort study of menstrual cramps and ovulation in healthy, normally ovulating women. Sci Rep. 2022;12(1). doi:10.1038/s41598-022-08658-3
- Prior JC, Vigna YM, Schechter MT, Burgess AE. Spinal bone loss and ovulatory disturbances. N Engl J Med. 1990;323(18):1221–1227. doi:10.1056/nejm199011013231801
- Prior JC. Exercise associated menstrual disturbances. Reprod Endocrinol Surg Technol. 1996;1996:1077–1091.
- Prior JC, Vigna YM, Schulzer M, Hall JE, Bonen A. Determination of luteal phase length by quantitative basal temperature methods: validation against mid-cycle LH peak. Clin Invest Med. 1990;13(3):123–131.
- Bedford JL, Prior JC, Hitchcock CL, Barr SI. Detecting evidence of luteal activity by least-squares quantitative basal temperature analysis against urinary progesterone metabolites and the effect of wake-time variability. Eur J Obstet Gynecol Reprod Biol. 2009;146(1):76–80. doi:10.1016/j.ejogrb.2009.05.001
- Garcia de Leon R, Baaske A, Albert AY, et al. Higher perceived stress during the COVID-19 pandemic increased menstrual dysregulation and menopause symptoms. Women’s Health. 2023;19. doi:10.1177/17455057231199051
- Prior JC. Adaptive, reversible, hypothalamic reproductive suppression: more than functional hypothalamic amenorrhea. Front Endocrinol. 2022;13. doi:10.3389/fendo.2022.893889
- Shafrir AL, Wise LA, Palmer JR, et al. Validity of self-reported endometriosis: a comparison across four cohorts. Hum Reprod. 2021;36(5):1268–1278. doi:10.1093/humrep/deab012