
Abstract
Background
Herpes zoster (HZ) typically manifests in the acute phase with distinct blisters and severe neuropathic pain. Remarkably, a subset of patients initially presents with only a mild skin rash and moderate pain that gradually intensifies, following a parabolic pattern. Despite being frequently observed in clinical settings, the underlying causes of this trajectory and its potential connection with post-herpetic neuralgia (PHN) remain unclear.
Methods
To investigate this phenomenon in-depth, we conducted a meticulous retrospective study involving 529 eligible HZ patients. All these patients sought medical care at the Third Central Hospital of Tianjin, China, between January 2020 and December 2023.
Results
The research identified that 14.6% of the sample (77 patients) experienced pain scores aligning with a parabolic curve. This trend was significantly more prevalent in patients aged 60 and above, accounting for 90.9% of this group, and demonstrated a positive correlation with age. Moreover, 87.0% of these patients had pre-existing medical conditions, highlighting the potential role of comorbidities in influencing the pain trajectory. A concerning 45.5% of patients sought medical attention more than seven days after the onset of symptoms, a delay that could exacerbate neurological damage. Notably, among those following a parabolic pain pattern, 66.2% eventually developed PHN, a considerably higher rate compared to the broader patient population.
Conclusion
We emphasize that healthcare practitioners meticulously assess patients who initially report lower pain scores for high-risk factors potentially leading to parabolic pain increases, including being over 60 years old, having comorbid conditions, and delaying medical consultation beyond seven days from symptom onset. Early implementation of supplementary pain management therapies may mitigate the risk of PHN development and enhance the quality of life for patients. This study furnishes clinicians with a deeper understanding of the variations in HZ-related pain trajectories, promising to improve treatment approaches and prognoses for HZ patients while paving the way for enriched clinical practice in the future.
Introduction
Herpes zoster (HZ), also known as shingles, arises from the varicella-zoster virus (VZV) reactivation, which lies dormant in the sensory ganglia following an initial chickenpox infection.Citation1 Typically, it presents as a painful rash along specific dermatomes, accompanied by acute neuropathic pain.Citation2,Citation3 A significant complication arising from HZ is post-herpetic neuralgia (PHN), a persistent neuropathic pain condition lasting three months or more and, in some cases, years, significantly diminishing the patient’s quality of life.Citation4
Recent advancements in vaccination against chickenpox have notably reduced the occurrence of VZV infections among adolescents, thus decreasing the risk of HZ development.Citation5 However, an age-related increase in the incidence of both HZ and PHN has been observed, establishing a direct association between aging and these conditions.Citation6,Citation7 The causes behind this uptick are multifaceted, possibly involving reduced vaccine effectiveness over time, decreased cellular immune function with age, and immune disruptions due to underlying health issues or the administration of immunosuppressive agents.Citation8
The initial 30 days following rash onset is the acute phase of HZ. Many patients endure nonspecific prodromal symptoms such as itching, burning sensations, headaches, and systemic manifestations like fever and fatigue.Citation9 These symptoms are swiftly followed by acute pain in the rash-affected area, characterized frequently as burning or stabbing and accompanied by other sensory disturbances such as altered tactile sensitivity and numbness.Citation10
Interestingly, some patients demonstrate a distinct clinical pathway, presenting initially with only a rash or mild discomfort and no apparent severe pain symptoms.Citation11 As time progresses, these individuals experience a surge in pain intensity, deviating from the conventional pain trajectory commonly seen in HZ patients. This delayed-onset pain is predominantly observed in middle-aged and elderly individuals and has been correlated positively with age. Moreover, this patient group is at a higher risk of developing PHN, underscoring a crucial pivot in our comprehension of HZ pathophysiology and its clinical management.
Given the profound impact of PHN as a persistent neural pain condition that significantly disrupts daily activities and emotional well-being, it is crucial to promptly identify acute-phase HZ patients exhibiting parabolic pain score patterns. By implementing proactive interventions for these individuals, we can reduce the risk of PHN development, thus mitigating the severity and duration of their suffering.
Materials and Methods
Study Population
We scrutinized the clinical and laboratory data of acute HZ patients to discern the percentage of individuals progressing to PHN and to evaluate the influence of HZ and PHN on pain experiences. The study encompassed patients who sought outpatient care at the Dermatology Department of Tianjin Third Central Hospital in China between January 2020 and December 2022.
Inclusion and Exclusion Criteria
To be included in the study, individuals had to have a verified diagnosis of HZ, determined by a unilateral dermatomal rash with or without accompanying pain. In the case of atypical presentations, supplementary diagnostic approaches were employed, such as PCR analysis of VZV DNA in vesicular fluid and enzyme-linked immunosorbent assay (ELISA) of VZV-specific antibodies in serum. Patients who either passed away or could not be reached for follow-up were excluded from the study.
Data Collection
Qualifying participants were asked to complete a pain assessment survey at their first outpatient visit. Physicians were available to aid in this process, and comprehensive data, including contact details, medical histories, treatment logs, and laboratory test outcomes, were carefully documented. Follow-up sessions and further survey rounds were scheduled at 7, 14, 21, 28, and 90 days post-rash onset. For those unable to attend in person, follow-ups were conducted over the phone.
Pain Assessment Tool
We employed the HZ Brief Pain Inventory (ZBPI) scale for pain assessment.Citation6 This scale delineates pain into four grades: No pain (0), Mild pain (1–2), Moderate pain (3–6), and Severe pain (7–10). Beyond quantifying pain severity, the ZBPI scale analyzed the repercussions of pain on various aspects of patients’ daily life activities (ADL), encompassing areas like emotional well-being, mobility, work efficiency, interpersonal connections, sleep quality, and life interests, dispersed over seven items. An 11-point Likert scale facilitated the evaluation of each item, with 0 denoting no impact and 10 signifying the highest possible influence.
Underlying Diseases
The research considered the prevalence of underlying health conditions among participants, including but not restricted to diabetes, cancer, hypertension, cardiovascular ailments, gastrointestinal issues, renal disorders, liver complications, arthritis, and autoimmune diseases.
Statistical Analysis
This study will statistically analyze and examine the basic characteristics of the overall patient population, including gender, age (age distribution by segments), time to visit after onset, affected areas, underlying diseases, pain scores (in chronological order), and the prevalence of PHN (Post-herpetic Neuralgia). Using mathematical methods, the study will depict the pain score-time curve, identify patients with parabolic pain patterns, and compare them with the overall patient population to summarize their clinical characteristics. We utilized SPSS 29.0 software to construct a database for efficient data input, structuring, and statistical examination. Categorical data were represented as percentages (%) and analyzed using the chi-square test. Non-normally distributed continuous variables were depicted through medians (Q1, Q3), with group analyses being executed via the Wilcoxon rank-sum test (for two groups) and the Kruskal–Wallis H-test (for multiple groups). A two-tailed approach was adopted for all tests, setting the statistical significance threshold at α=0.05.
Results
Patient Characteristics
Sample Selection and Basic Features
Out of the 620 individuals who sought medical consultation, 91 were excluded — 85 due to loss to follow-up and 6 due to demise — resulting in a cohort of 529 patients for evaluation, encompassing 327 males and 202 females. The age distribution spanned from 15 to 93 years, with a median (IQR) of 62 years (48, 70). Noteworthily, a significant portion, 58.8% (311/529), were aged 60 or above. The prevalence of individuals with one or more underlying health conditions was 51.8% (274/529). In the early aftermath of symptom emergence, 35.3% (187/529) procured medical assistance within a 3-day frame, contrasted by 30.8% (163/529) who delayed until after 7 days. Dissecting the affected domains disclosed that 37.7% (200/529) were in the chest and back, 19.5% (103/529) in the waist and abdomen, 16.3% (86/529) in the head and face, 13.6% (72/529) in the neck, shoulders, and upper limbs, and 12.9% (68/529) in the buttocks and lower limbs. Additionally, 28.2% (149/529) of the study subjects were diagnosed with PHN ().
Table 1 Classification Characteristics of Herpes Zoster Patients and Pain Score Information
Pain Features and Site Distribution
Within the confines of the study, 77 patients delineated a parabolic trajectory in pain intensity, translating to 14.6% (77/529) of the total pool. This subset comprised 40 males and 37 females aged between 38 and 89, with a median age (IQR) of 71 years (62, 78). Strikingly, 90.9% (70/77) were 60 years or older, and a substantial fraction, 87.0% (67/77), reported having at least one underlying health ailment. Analyzing their medical care-seeking behavior revealed that 25.9% (20/77) accessed medical assistance within the first three days post-symptom onset, while a larger section, 45.5% (35/77), postponed it beyond seven days. The PHN diagnosis was confirmed in 66.2% (51/77) of this group, a vast majority of whom, 94.1% (48/51), acknowledged at least one existing health concern. A trend of escalating patient proportion with parabolic pain was witnessed with age augmentation, detailed in different age brackets in .
Table 2 Classification Characteristics and Pain Score Profiles of Patients Exhibiting Parabolic Pain Changes
Comparison of Patients with Parabolic Pain to the Overall Patient Population
Upon closer scrutiny, a statistically significant disparity (P<0.01) emerged when contrasting average age, the incidence of underlying health complications, the time-lapse to medical consultation post symptoms onset, and PHN occurrence between individuals with parabolic pain dynamics and the general patient populace. Older individuals, those harboring one or more underlying health disorders, and those demonstrating procrastination in seeking medical intervention post-symptom emergence were correlated with an escalated probability of undergoing parabolic pain and a greater prevalence of PHN. Accentuated delineations of these distinctions were captured when the parabolic pain patient group was partitioned into age categories of ≥75, 60–74, and ≤59.
Assessment of Patients’ Pain Using the ZBPI Scale
Initial Pain Scores
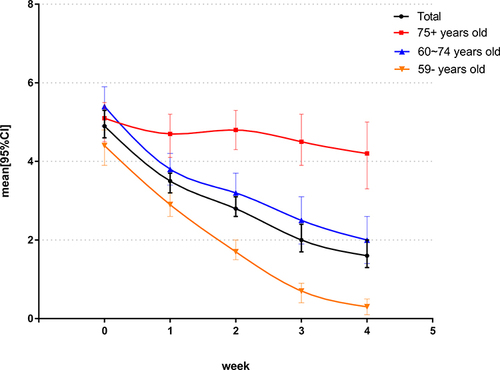
Utilizing the ZBPI scale, the study investigated the primary pain ratings in 529 HZ patients. The entire group had a median (IQR) score of 5 (3, 7) and an average score with a 95% confidence interval of 4.9 (4.6, 5.3). When grouped by age, the initial pain scores for different age groups were as follows: 75 years and above group: Median initial pain score (IQR) was 5 (4, 7), with a mean (95% CI) of 5.1 (4.5, 5.5); 60–74 years’ group: Median initial pain score (IQR) was 5 (4, 8), with a mean (95% CI) of 5.4 (4.9, 5.9); below 59 years’ group: Median initial pain score (IQR) was 4 (3, 6), with a mean (95% CI) of 4.4 (3.9, 4.8). For more detailed information regarding pain severity scores, please refer to .
Initial Pain Scores for Patients Exhibiting Parabolic Pain Patterns
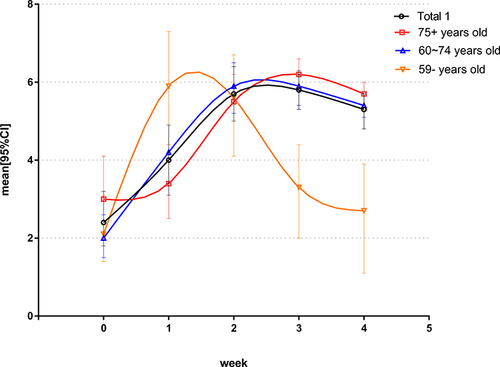
If we describe the relationship mathematically, with the pain score of the patient as the y-axis and the duration of the illness as the x-axis, we find that the pain score-time curve remarkably aligns with a parabola. Therefore, we term it the parabolic pain pattern. Focusing on the 77 patients demonstrating parabolic pain patterns, their median (IQR) initial score was considerably lower at 2 (1, 3), and an average score with a 95% confidence interval was recorded at 2.4 (1.8, 3.2). When categorized by age, the initial pain scores for different age groups were as follows: 75 years and above group: Median initial pain score (IQR) was 3 (1, 4), with a mean (95% CI) of 3.0 (2.0, 4.1); 60–74 years’ group: Median initial pain score (IQR) was 2 (1, 2), with a mean (95% CI) of 2.0 (1.5, 2.6); below 59 years’ group: Median initial pain score (IQR) was 2 (1, 2), with a mean (95% CI) of 2.1 (1.4, 3.1). For more detailed information regarding pain severity scores, please refer to .
Overall Observation of Pain Trends in HZ Patients
The HZ patient group showed a diminishing trend in weekly pain scores. Nevertheless, the descent was more gradual for individuals aged 75 and above, while those below 59 years initiated with relatively subdued pain scores. The variations in these trends are graphically represented in .
Figure 1 In the overall population (Total), pain severity scores exhibit a weekly declining trend, with a slower decline observed in the 75 and above age group and slightly lower initial pain scores in the 59 and below age group.
Pain Trends in Patients Exhibiting Parabolic Pain Patterns
Patients presenting parabolic pain trajectories illustrated a unique pattern marked by an initial surge in pain intensity followed by a consistent decline. This trend was especially noticeable in the sub-59 age group, witnessing a substantial pain elevation at the one-week mark before a swift descent. Conversely, those in the 75 and above bracket experienced a notable spike in pain at the fortnight mark, enduring a gradual mitigation in pain intensity. These trends are illustrated in .
Figure 2 Among individuals displaying a parabolic change in pain scores (Total 1), pain severity scores exhibit a parabolic trend characterized by an initial increase followed by a decrease. In the 59 and below age group, there is a notable upward trend at 1 week, followed by a rapid decline, whereas the 75 and above age group shows a prominent upward trend at 2 weeks with evident delayed onset, followed by a gradual decrease.
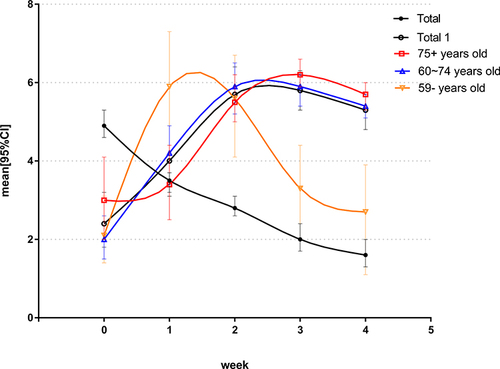
Comparison of Pain Scores in HZ Patients Exhibiting Parabolic Patterns and the Overall Patient Cohort
Comparative scrutiny of the HZ patients with parabolic pain patterns and the larger patient cohort unveiled substantial disparities in their pain scores, as showcased in .
Figure 3 Pain severity scores show significant differences when compared to the overall population.
Discussion
PHN is a type of nerve pain, and recent studies have shown its strong association with the neuroimmune and peripheral immune systems and the inflammatory substances they produce.Citation12 When the VZV virus becomes active again, it prompts an immune response that stirs up neuroimmune cells. These cells then release inflammation-causing agents and draw other immune cells to the nervous system. This action results in nerve inflammation, unprovoked pain, and increased sensitivity to pain. The interplay between different immune cells and imbalances in inflammation-causing and inflammation-reducing agents leads to a continuous cycle, keeping the nerve inflammation alive and perpetuating the nerve pain.Citation13–16
Clinical symptoms of PHN vary widely among individuals. Some patients might only show skin rashes without noticeable pain or mild discomfort.Citation17 In certain instances, pain appears later and is marked by a curve-like shift in pain ratings. Our research indicated that of those patients who demonstrated this trend, nearly 91% (70 out of 77) were 60 years old or older, with notable variations between different age categories. Among those aged 75 and above, 37.6% (32/85) exhibited parabolic changes, compared to 16.8% (38/226) in the 60–74 age group and only 3.2% (7/218) in the under 59 age group. Furthermore, 87.0% (67/77) of these patients had underlying health conditions. Individuals of older age with concurrent comorbidities are more prone to this phenomenon. Several factors may contribute to this phenomenon: as individuals age, both the quantity and activity of immune cells decrease, and innate and adaptive immunity weaken, possibly delaying or attenuating neuroinflammatory immune responses and resulting in delayed pain.Citation18,Citation19 Underlying health conditions may similarly inhibit immune system activity, reducing immune cell activity. Certain painful underlying conditions may interfere with a patient’s perception and assessment of shingles-associated neuralgia. Additionally, age-related neurological decline may contribute to diminished pain perception.Citation20–23 This study highlights that older age plays a decisive role in the duration of pain delay, whereas underlying health conditions are a significant factor among younger patients.
Our research also revealed a significantly elevated incidence of PHN (66.2%) among patients with pain scores exhibiting parabolic changes. There were differences in the proportions among different age groups, with higher proportions observed in older age groups. Among those aged 75 and above, 75.0% (24/32) developed PHN, while 60.5% (23/38) did in the 60–74 age group and 57.1% (4/7) in the under 59 age group. Notably, a vast majority, 94.1% (48/51), of these individuals had pre-existing health conditions. A further contributing factor is the considerable fraction, 45.5% (35/77), who pursued medical assistance only after a delay of over seven days post-symptom onset, potentially escalating the nerve damage sustained. Thus, it is deduced that older age and immunosuppression are key high-risk factors predisposing to PHN, further exacerbated by delayed medical intervention. This emphasizes a pertinent clinical inference: Early and proactive medical engagement can be critical in mitigating the risk of PHN, especially in older demographics with underlying health concerns.Citation7,Citation24
This phenomenon can be explained by two primary factors: First, the variability in viral activity. HZ arises from the VZV that can remain latent within the body for extended periods. Upon reactivation, the virus targets nerve cells, instigating neural inflammation and subsequent pain. Such reactivation could be instrumental in the observed parabolic pain trajectory. Second, the dynamic nature of immune responses. At the onset, the immune system might muster a robust defense, curbing the viral propagation and correlating with milder pain intensities. However, as the immune response attenuates over time, the virus may proliferate more aggressively within the nervous system, culminating in a pronounced spike in pain—thus delineating a parabolic pattern.
PHN is characterized by lingering neural discomfort even after HZ has resolved. Thus, a parabolic trend in acute-phase HZ pain scores could signal an escalated propensity for neuralgia and act as a precursor to PHN.
Motivated by this captivating phenomenon, our research endeavor entailed an exhaustive clinical examination encompassing data acquisition, rigorous statistical scrutiny, and novel methodologies. We endeavored to decode the enigmatic mechanisms underlying this deferred pain onset, amplify our proficiency in gauging HZ severity, recalibrate therapeutic blueprints, earmark individuals with heightened susceptibility to PHN, and pioneer avant-garde early intervention tactics. Through this investigation, we aspire to unveil nuanced insights into the multifaceted landscape of HZ, thereby transforming our clinical strategy to address this debilitating ailment and optimize patient prognoses.
Our research spanned from January 2020 to December 2022, coinciding with the enactment of COVID-19 containment protocols by the Chinese government. Extended home confinement, perturbed daily rhythms, augmented psychological duress, and possible immune perturbations might have influenced a heightened HZ incidence during this epoch. Out of apprehension over acquiring COVID-19 during medical consultations, numerous patients postponed clinical engagement, inadvertently amplifying the latency in PHN diagnosis and intervention. The nexus between these behavioral shifts, psychological ramifications, and the observed parabolic pain trajectories in patients beckons further scholarly exploration.
From the results of this investigation, it is evident that regardless of the absence or presence of only minor pain during the initial phase of the disease, preemptive use of adjunctive analgesics might be beneficial for high-risk patients prone to a parabolic pain trajectory. This includes individuals aged 60 or older, those with underlying health conditions, or those who delay medical intervention for more than a week. Such a proactive approach could potentially mitigate the risk of evolving into PHN, a sentiment echoed by prior studies focusing on elderly patients who experienced moderate to intense pain associated with shingles.Citation25
It is paramount to prioritize clinical monitoring and immediate intervention for these demographics. Patient education should also be emphasized, ensuring individuals can promptly identify early symptoms, such as skin eruptions, and seek medical advice even if pain is absent or minimal.
This study has several limitations that warrant consideration: 1) It is a single-center retrospective study conducted over a short time frame, which may introduce bias due to loss of follow-up and missing data for some patients. 2) All patients received standardized antiviral treatment. However, the lack of a placebo control group hinders evaluating its specific effect on pain duration. 3) The sample size is limited, highlighting the need for larger-scale studies in the future to enhance the robustness of the findings. 4) Intra-rater and inter-rater reliability were not assessed, and variations between raters and patients could potentially influence the results.
Conclusion
Our research offers significant insights into the etiology of PHN. The unique parabolic pain trend could be a pivotal signpost for potential PHN onset, underlining the urgency for timely therapeutic interventions even when the initial pain indications are subdued. The efficacy of early adjunctive analgesic protocols in curbing PHN incidence is further corroborated by existing literature. Clinical alertness, swift medical actions, and patient education remain paramount. Future investigations could gain from collaborative efforts across multiple research centers, embracing larger participant cohorts and adopting more objective pain evaluation metrics to reinforce these conclusions.
Abbreviations
HZ, Herpes zoster; VZV, varicella-zoster virus; PHN, post-herpetic neuralgia; ELISA, enzyme-linked immunosorbent assay; ZBPI, HZ Brief Pain Inventory.
Ethics Approval and Informed Consent
This research was conducted per the principles of the Helsinki Declaration and the Chinese Guidelines for the Diagnosis and Treatment of HZ. The study received approval from the Ethics Committee of the Third Central Hospital of Tianjin (Approval No. SZX2020-005). All patients provided written informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there is no conflicts of interest regarding the publication of this article.
Data Sharing Statement
The datasets utilized and/or analyzed in the present study are available upon reasonable request from the corresponding author.
References
- Yin D, Van Oorschot D, Jiang N, et al. A systematic literature review to assess the burden of herpes zoster disease in China. Expert Rev Anti Infect Ther. 2021;19(2):165–179.
- Camargo K. Correction: in the Clinic-Herpes Zoster. Ann Intern Med. 2018;169(7):516.
- John AR, Canaday DH. Herpes Zoster in the Older Adult. Infect Dis Clin North Am. 2017;31(4):811–826.
- Khadem T, Stevens V. Therapeutic options for the treatment of post-herpetic neuralgia: a systematic review. J Pain Palliat Care Pharmacother. 2013;27(3):268–283.
- Wutzler P, Bonanni P, Burgess M, Gershon A, Safadi MA, Casabona G. Varicella vaccination - The global experience. Expert Rev Vaccines. 2017;16(8):833–843.
- Johnson RW, Rice AS. Clinical practice. Post-herpetic neuralgia. N Engl J Med. 2014;371(16):1526–1533.
- Forbes HJ, Thomas SL, Smeeth L, et al. A systematic review and meta-analysis of risk factors for post-herpetic neuralgia. Pain. 2016;157(1):30–54.
- Gershon AA, Gershon MD. Pathogenesis and current approaches to control of varicella-zoster virus infections. Clin Microbiol Rev. 2013;26(4):728–743.
- Johnson RW, Bouhassira D, Kassianos G, Leplege A, Schmader KE, Weinke T. The impact of herpes zoster and post-herpetic neuralgia on quality-of-life. BMC Med. 2010;8:37.
- Garcia-Gonzalez AI, Rosas-Carrasco O. Herpes zoster and post-herpetic neuralgia in the elderly: particularities in prevention, diagnosis, and treatment. Gac Med Mex. 2017;153(1):92–101.
- Patil A, Goldust M, Wollina U. Herpes zoster: a Review of Clinical Manifestations and Management. Viruses. 2022;14(2).
- Devor M. Rethinking the causes of pain in herpes zoster and post-herpetic neuralgia: the ectopic pacemaker hypothesis. Pain Rep. 2018;3(6).
- Lowy DB, Makker PGS, Moalem-Taylor G. Cutaneous Neuroimmune Interactions in Peripheral Neuropathic Pain States. Front Immunol. 2021;12:660203.
- Bachiller S, Jimenez-Ferrer I, Paulus A, et al. Microglia in Neurological Diseases: a Road Map to Brain-Disease Dependent-Inflammatory Response. Front Cell Neurosci. 2018;12:488.
- Malcangio M. Role of the immune system in neuropathic pain. Scand J Pain. 2019;20(1):33–37.
- Kuhn JA, Vainchtein ID, Braz J, et al. Regulatory T-cells inhibit microglia-induced pain hypersensitivity in female mice. Elife. 2021;10.
- Huang J, Li Y, Xie H, et al. Abnormal Intrinsic Brain Activity and Neuroimaging-Based fMRI Classification in Patients With Herpes Zoster and Post-herpetic Neuralgia. Front Neurol. 2020;11:532110.
- Castelo-Branco C, Soveral I. The immune system and aging: a review. Gynecol Endocrinol. 2014;30(1):16–22.
- Montecino-Rodriguez E, Berent-Maoz B, Dorshkind K. Causes, consequences, and reversal of immune system aging. J Clin Invest. 2013;123(3):958–965.
- Finnerup NB, Kuner R, Jensen TS. Neuropathic Pain: from Mechanisms to Treatment. Physiol Rev. 2021;101(1):259–301.
- St John Smith E. Advances in understanding nociception and neuropathic pain. J Neurol. 2018;265(2):231–238.
- Rosenberger DC, Blechschmidt V, Timmerman H, Wolff A, Treede RD. Challenges of neuropathic pain: focus on diabetic neuropathy. J Neural Transm (Vienna). 2020;127(4):589–624.
- Ghione S. Hypertension-associated hypalgesia. Evidence in experimental animals and humans, pathophysiological mechanisms, and potential clinical consequences. Hypertension. 1996;28(3):494–504.
- Gruver C, Guthmiller KB. Post-Herpetic Neuralgia. Treasure Island (FL) ineligible companies; 2023.
- Xing X, Sun K, Yan M. Delayed Initiation of Supplemental Pain Management is Associated with Post-herpetic Neuralgia: a Retrospective Study. Pain Physician. 2020;23(1):65–72.