
Abstract
Background
The chronic pain arising from knee osteoarthritis (KOA) is a prevalent clinical manifestation. As a traditional Chinese approach, electroacupuncture (EA) has a positive influence in relieving chronic pain from KOA. The study aims to explore functional connectivity (FC) and effective connectivity (EC) alterations induced by EA in anterior cruciate ligament transection (ACLT) rat model of KOA using resting-state functional magnetic resonance imaging (fMRI).
Methods
After the establishment of ACLT, rats were randomly divided into the EA group and the sham-EA group. The EA group received EA intervention while the sham-EA group received sham-intervention for 3 weeks. Mechanical pain threshold (MPT) assessment was performed before and after intervention, and fMRI was conducted after intervention.
Results
EA intervention effectively relieved pain in post-ACLT rats. Results of rest-state functional connectivity (rs-FC) analysis revealed that compared with the sham-EA group, the EA group had higher FC between the right raphe and the left auditory cortex, the left caudate_ putamen and the left internal capsule (IC), as well as the right zona incerta (ZI) and the left piriform cortex, but lower FC between the right raphe and the left hippocampus ventral, as well as the right septum and the left septum. Furthermore, Granger causality analysis (GCA) found the altered EC between the right septum and the left septum, as well as the left IC and the right septum.
Conclusion
The results confirmed the effect of EA on analgesia in post- ACLT rats. The alterations of FC and EC, mainly involving basal ganglia and limbic system neural connections, might be one of the neural mechanisms underlying the effect of EA, providing novel information about connectomics plasticity of EA following ACLT.
Introduction
Knee osteoarthritis (KOA) is known as a common clinical joint osteoarthritis caused by cartilage lesions and bone hyperplasia of the knee.Citation1 The main clinical manifestations are chronic pain and dysfunction that cause reduced life quality of the elderly and heavy economic burden.Citation2,Citation3 Acupuncture, one of the traditional Chinese treatments, is effective in relieving chronic pain from KOA.Citation4,Citation5 It has been reported that acupuncture generates positive effects in chronic pain in 50% to 85% of cases.Citation6 Electroacupuncture (EA) is a modified technique to apply pulse current to acupuncture needles, which plays a dual role of acupuncture and pulse electrotherapy.Citation7 EA has been proven to have significant effect on remarkably alleviating pain of diseases, including KOA.Citation8 A Cochrane review showed that EA had the characteristics of significant analgesic effect as well as a low untoward reaction risk.Citation9 Zhou et al treated 80 KOA subjects with low-frequency EA or Diclofenac Sodium Sustained Release Capsules for 28 days, indicating favored results of EA over Diclofenac Sodium Sustained Release Capsules for relieving pain.Citation10
It has been a research hotspot to study the pathogenesis of pain and the mechanism of acupuncture analgesia from the perspective of brain plasticity.Citation6,Citation11 It has been proven that resting-state functional connectivity (rs-FC) is powerful to explore the chronic pain’s neural basis.Citation12 In our previous study, we used resting-state functional magnetic resonance imaging (rs-fMRI) to investigate the changes of brain plasticity among people of end-stage KOA, and we found that KOA patients exhibited decreased rs-FC between the left middle temporal gyrus (left-MTG) and the left middle frontal gyrus, right dorsolateral superior frontal gyrus, as well as left medial superior frontal gyrus, indicating that patients’ intrinsic brain activity patterns were affected by pain-related pathological changes.Citation13
The pathological changes of KOA lead to peripheral nerve stimulation around the joint, resulting in activation of peripheral pain receptors, pain signal generation, and subsequent transmission to the subcortical centers, ultimately causing pain.Citation14 Pain involves structural and functional changes of brain neurons and it activates brain networks, affecting body feeling and emotion.Citation15,Citation16 Many brain nuclei forming a complex network play an important role on acupuncture analgesia, mainly including the periaqueductal grey (PAG), nucleus raphe magnus (NRM), caudate nucleus, septal area, accumbens nucleus (Acb), etc.Citation6
Most previous studies have mainly concentrated on functional connectivity (FC) in these brain regions, which can reflect indirect connections between brain regions.Citation17 However, FC does not provide insight into the specific causal relationships among brain regions, whereas effective connectivity (EC) provides a deep understanding of the brain activity of KOA by compensating for this deficit.Citation18 Recently, Granger causality analysis (GCA), which reflects the specific intensity and direction of information flow within a given brain region, has been applied on fMRI studies and is considered a suitable method to reveal causal effects among brain regions.Citation19–21 GCA has been applied in studies of chronic pain.Citation22–24 Chen et al showed that acupuncture might relieve migraine without aura (MwoA) by increasing the EC of superior lobe of left cerebellum, rostral ventromedial medulla, and right precuneus.Citation25 No investigations have been done to determine the direction of the altered connections, despite the possibility that the specific internal brain effective connectivity may potentially be affected after the EA intervention of KOA.
In the present study, after we established the anterior cruciate ligament transection (ACLT) rat model of KOA, we utilized EA intervention in the EA group for 3 weeks, comparing to the sham-intervention group. Meanwhile, rs-fMRI was conducted to analysis the alternation of FC and EC induced by EA in post-ACLT rats. It was hypothesized that EA might ameliorate pain caused by ACLT by modulating both functional and effective connectivity. We aim to provide novel information about resting-state connectomics plasticity of effect of EA following ACLT.
Materials and Methods
Animals
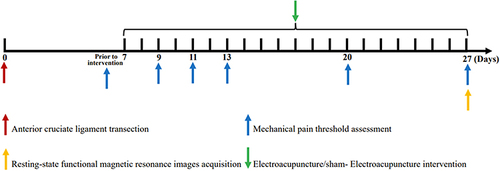
All the experimental procedures and animal care were approved by the Ethical Committee of Guanghua Hospital of Integrative Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine (Approval No. 2022-K-30). National Institutes of Health Guide for the Care and Use of Laboratory Animals were followed in the entire process. A total number of 16 Sprague-Dawley (SD) rats weighing between 180 and 200 g (female, clean-grade) were provided by Guanghua Hospital of Integrative Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine.Citation26,Citation27 The rats were divided randomly into the EA group (n=8) and the sham-EA group (n=8). The diagram of the entire experimental process was depicted in .
Figure 1 The diagram of the experimental process.
Rat Model of Knee Osteoarthritis of the Right Knee with Anterior Cruciate Ligament Transection (ACLT)
The pentobarbital sodium (40mg/kg) through intraperitoneal injection was used to anesthetize the rats until their respiration was shallow and slow, the limbs were weak, and the corneal reflex was weakened or disappeared. The electric shaver shaved the hair and prepared the skin. The rats were fixed on an operating table in supine position. The routine iodophor was used for disinfection and the aseptic gauze was covered around the surgical area. Subsequently, the ACLT rat model of KOA was performed.Citation28
Electroacupuncture Intervention
In the EA group, Futu (ST32) and Zusanli (ST36) acupoints on the left side (the unaffected side) were stimulated by EA after 7 days of modeling. Two 0.25*40 mm disposable sterile stainless needles were, respectively, inserted to a penetration depth of 5 mm at ST32, located in upper one-third of the line connecting the anterior superior iliac spine and lateral patella, and ST36, located on the lateral posterior position of the knee, 5 mm below the capitulum fibulae.Citation29,Citation30 Electroacupuncture instrument (SDZ-V Hwato brand) was then used to provide electrical stimulation pulses at a frequency of sparse and dense waves of 2 Hz, 0.2 ms pulse width and 2 mA intensity.Citation31 The positive electrode was connected with ST36 and the negative electrode was connected with ST32. The current intensity was adjusted until the muscle twitched slightly. EA stimulation was applied for 20 min each time, once a day, 5 times a week, continuously lasting 3 consecutive weeks.
In the sham-EA group, same as the EA group, two same needles were inserted, respectively, into ST32 and ST36 on the left side. But the connected EA instrument did not deliver electrical stimulation pulses. The sham intervention was also maintained 20 minutes each time, once a day, 5 times a week, continuously lasting 3 consecutive weeks.
Mechanical Pain Threshold (MPT) Assessment
To investigate the analgesic effect of EA for post-ACLT rats, MPT assessment was carried out within 8 rats from each group prior to intervention (T0) and on 3, 5, 7, 14, 21 days after the intervention (T1, T2, T3, T4 and T5, respectively). The rats were placed on a wire grid covered by a transparent and perforated plexiglass box and given 30 minutes for adaptation. Von Frey filaments which were buckled for 5 s each with a 10 s interval, 5 cycles on the plantar surface of right hind paws were used to observe paw withdrawal responses. A thicker filament was applied if less than three paw withdrawal responses occurred. Paw withdrawal threshold (PWT) referred to the thinnest filament that caused paw withdrawal responses at least 3 times.
fMRI Image Acquisition
rs-fMRI was obtained by a 7 T animal fMRI scanner (Bruker Corporation, Germany) after 3-week intervention (T5). The rats were fixed in the scanner after receiving 4% isoflurane anesthetic effect. Continuously input of 1.5–2% isoflurane was used to ensure that the rats were anesthetized during the entire scanning process and a ventilator was used for respiratory monitoring of the rats. Using a Gradient Echo-Echo Planar Imaging (GRE-EPI) sequence, fMRI images were acquired by the following particular parameters: field of vision= 32*32 mm2, flip angle= 90°, repetition time = 3000 ms, echo time= 20ms, slice number=43, and slice thickness = 0.5 mm. After scanning, it was necessary to visually check data quality.
fMRI Data Preprocessing
We carried out image preprocessing using the statistical parametric mapping 12 (SPM12) toolbox (http://www.fil.ion.ucl.ac.uk/spm/) and the Data Processing Assistant for Resting-State fMRI (DPARSF) v4.5 (http://rfmri.org/DPARSF) on MATLAB platform. At the beginning of the preprocessing, the images were enlarged by 10 times to make their size approximate to the human brain, so that the data processing algorithm originally developed for human research could work normally for rats. The preprocessing was mainly composed of the following procedure: format conversion of the images from DICOM to NIfTI format, removal of non-brain tissue, data screening, slice timing, realignment, spatial normalization to the standard template, smooth with a full width at half maximum triploid as the voxel size, detrend, filtering with a bandpass filtering at 0.01–0.1 Hz and regressing out nuisance covariates.Citation32
Functional Connectivity Analysis
Based on the atlas of the rat’s brain, 96 regions of interest (ROIs) were automatically divided in the whole rat brain.Citation32 The seed-based FC was performed between ROIs by calculating the Pearson’s correlation coefficients of the average value of the time series from all voxels in each ROI. In addition, the FC value was standardized to zFC value using Fisher’s z-transformation. Subsequently, comparison of zFC values between the two groups was conducted. Multiple comparison correction was made using false discovery rate (FDR) (α=0.05, two-tailed).
Granger Causality Analysis
In order to obtain the direction of connectivity in the brain regions, EC analysis was performed on the brain regions, which showed statistical significance through FC analysis between the two groups and then were defined as ROIs. In this research, GCA was performed to analyze EC on RESTplus software (http://restfmri.net/forum/RESTplus). According to the extended vector autoregressive model of Hamilton’s as follows:Citation19
Xt and Yt respectively represent time series. Ai and A'i represent signed-path coefficients, Bi and B'i represent autoregression coefficients, ε and ε' represent residual, and Zt represent covariates. Xt is the Granger cause of Yt if Ai is significantly higher or lower than zero. Similarly, Yt is the Granger cause of Xt if A'i is significantly higher or lower than zero. The signed-path coefficients are used for further group comparison.
Statistical Analysis
SPSS software (v 22.0, IBM, Armonk, New York) was used to carry out statistical analysis. The MPT data in the EA group and the sham-EA group at different time points was analyzed using two-way repeated-measures analysis of variance (ANOVA), with the intervention (EA and sham-EA) as the between-subject factor and time (T0, T1, T2, T3, T4 and T5) as the within-subject factor. If the interaction effect between intervention and time of the MPT data was significant, simple effect analysis was performed, followed by Bonferroni’s post hoc tests to determine the between-group and within-group differences. In the post hoc test, a Bonferroni adjustment was applied for multiple comparisons with the significance level set at p<0.05/k, where k represented the number of comparisons. Additionally, two-sample t-test was used to access differences in zFC values and GCA signed-path coefficients between the two groups at T5. Multiple comparison correction was made using false discovery rate (FDR). The statistical p-value was set at p<0.05(two-tailed).
Results
Difference of Mechanical Pain Threshold Between the Two Groups Before and After Intervention
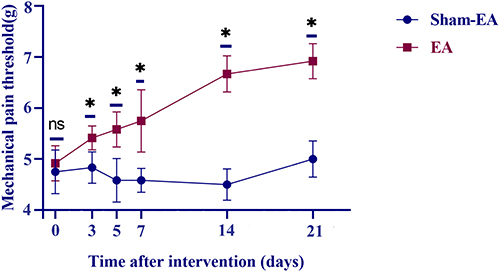
As shown in , the interaction effect between intervention and time of the MPT data was statistically significant (F=18.272, p<0.001). The results of the simple effect analysis showed that there was no significant difference in MPT between the EA group and the sham-EA group at T0 (F=0.737, p=0.405) and there were significant differences at T1, T2, T3, T4 and T5 (F=18.053, p<0.001; F=26.526, p<0.001; F=25.407, p<0.001; F=169.000, p<0.001; F=119.452, p<0.001, respectively). No significant difference was found between the different time points in the sham-EA group (F=1.906, p=0.180). Furthermore, a significant difference was found between different time points in the EA group (F=33.283, p < 0.001). Bonferroni’s post hoc test revealed that in the EA group, there existed significant differences between T0 and T1, T2, T3, T4,T5 (all p < 0.05), T1 and T4, T5 (all p<0.05), T2 and T4, T5 (all p < 0.05) as well as T3 and T4, T5 (all p < 0.05).
Figure 2 Comparison of mechanical pain threshold between the EA group and the sham-EA group.
Difference of Functional Connectivity Between the Two Groups After 3-Week Intervention
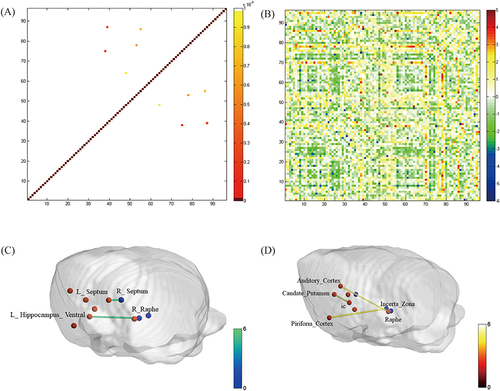
The between-group comparison of FC was shown in . The p-value diagram (p<0.001) and the t-value diagram by two-sample t-test were depicted in and , respectively. Specifically, the FC analysis revealed that the zFC values between the right raphe and the left hippocampus ventral (t=−5.584, p<0.001), as well as the right septum and the left septum (t=−5.470, p<0.001) were significantly lower in the EA group in comparison with the sham-EA group (). And the zFC values between the right raphe and the left auditory cortex (t=3.722, p<0.001), the left caudate_putamen and the left internal capsule (IC) (t=4.939, p<0.001), as well as the right zona incerta (ZI) and the left piriform cortex (t=4.607, p<0.001) were significantly higher in the EA group ().
Figure 3 Comparison of functional connectivity between the EA group and the sham-EA group.
Difference of Effective Connectivity Between the Two Groups After 3-Week Intervention
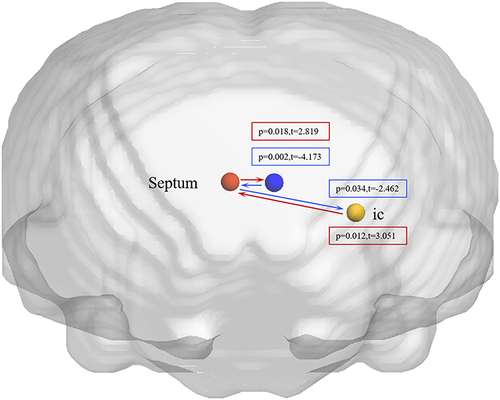
The rats following 3-week EA intervention exhibited significantly higher EC from the right septum to the left septum (t=2.819, p=0.018), higher EC from the left IC to the right septum (t=3.051, p=0.012), lower EC from the right septum to the left IC (t=−4.173, p=0.002) and lower EC from the left septum to the right septum (t=−2.462, p=0.034) in comparison with the sham-EA group ().
Figure 4 Comparison of effective connectivity between the EA group and the sham-EA group after 3-week intervention.
Discussion
KOA is a common chronic joint disease characterized by chronic pain, swelling and knee joint dysfunction or degeneration.Citation33 EA has been reported as an effective method to alleviate joint pain.Citation34 Consequently, further research is necessary to understand the underlying mechanism of EA in treating KOA. This study investigated the changes of connectivity involved in the effects of EA at ST 32 and ST 36 acupoints in post-ACLT rats. To our knowledge, this study is the first study to integrate FC and EC analyses to explore the brain functional connectivity alteration in post-ACLT rats. Consistent with previous findings, we found a significant improvement in MPT in the EA group compared to the sham-EA group. And the rs-fMRI results showed that EA can induce significant alterations in FC and EC in the brain of post-ACLT rats, mainly involving basal ganglia and limbic system neural connections.
In the EA treatment strategy, we utilized ST32 and ST36 as EA acupoints ground on both traditional and contemporary practices. Firstly, as per the ancient Traditional Chinese Medicine text “Huangdi Neijing”, treatment for flaccidity focuses on the yangming meridian (ST).Citation35,Citation36 Those acupoints used most generally are tightly arranged in the stomach channel of foot-Yangming.Citation35,Citation36 The main mechanism of KOA is kidney deficiency, qi stagnation and blood stasis.Citation37 In the theory of traditional Chinese medicine, spleen qi is the biochemical source of human qi and blood.Citation37 ST32 and ST36 acupoints are believed to have a significant impact on promoting the operation of qi and blood caused by KOA. Secondly, our choice is supported by contemporary research as well. ST36 was one of the most frequently used acupoints for the treatment of pain.Citation38
The present research indicated a significant increase in MPT in post-ACLT rats after EA treatment. This behavioral change corresponds with alterations in the FC of key brain regions, notably those involved in processing sensation and emotion. These findings underscore the multidimensional nature of pain experience and its modulation by EA.
FC focuses on the temporal correlation among the activity of different brain regions.Citation12 Compared with the sham-EA group, our research observed significantly increased FC between the right raphe and the left auditory cortex, the left caudate_putamen and the left IC in the EA group. According to the three dimensions of pain, pain includes sensation, emotion and cognition.Citation39 The pathogenesis of chronic pain caused by KOA is closely related to the subcortical structures of subcortical nucleus.Citation40 Raphe nuclei (RPN), located in the brainstem, can integrate relevant contextual information and trigger the release of pain-related neurotransmitters in the central neural system, thus making it a significant structure associated with chronic pain.Citation6,Citation41 Auditory cortex is a critical region for sound processing as well as involved in all phases of emotional learning and memory.Citation42 The neural mechanism of perception and regulation of dorsal RPN on pain in neuroimaging is based on the research results showing that acupuncture enhanced FC between cortex or subcortical areas and dorsal RPN in chronic pain patients.Citation43 Consistent with these findings, Gao et al (2022) reported that the increased FC between the right putamen and the dorsal RPN was related to chronic pain severity in KOA patients after acupuncture invention.Citation3 Additionally, the striatum, comprising caudate and putamen, is part of the basal ganglia.Citation44 Caudate and putamen are associated with pain processing.Citation45 The IC is a bidirectional tract for information transmission to and from the cerebral cortex and is a critical brain region responsible for emotion processing and regulation.Citation46 We also found a significant increase in FC between the right ZI and the left piriform cortex in the EA group. ZI is a largely inhibitory subthalamic area that extensively connects with brain.Citation47 It influences sensory processing and transmits pain information.Citation34,Citation48 The piriform cortex is a key brain region of the olfactory cortex. The synaptic plasticity in the piriform cortex encodes olfactory information, associative memory and sensory processing.Citation49 EA intervention increased FC of brain regions involved in processing sensation and emotion, indicating that pain experience was multidimensional.
In addition, the results suggested decreased FC between the left hippocampus ventral and the right raphe in the EA group compared with the sham-EA group. Chronic pain is considered a type of long-term learning, distinguished by the accumulation of nociceptive memories and the inability to overcome negative emotional association.Citation50,Citation51 It is suggested that the negative emotion can aggravate the feeling of chronic pain in turn and become a vicious circle.Citation52 The hippocampus, a central structure of the limbic system, plays an important role in controlling emotion, learning, and memory.Citation53 Disrupting hippocampal function can reverse persistent nociception in rats.Citation54 The previous neuroimaging research has suggested that increased PAG–hippocampus connectivity was associated with worse pain symptoms in patients with KOA.Citation54 Collectively, based on the previous research, we speculated that decreased connectivity between the left hippocampus ventral and the raphe, which was exerted by EA in the current study, could reduce the information flow and result in analgesic effect. Furthermore, we found decreased FC between the right septum and the left septum. The septum is an important part of the limbic system and related to emotion and motivation.Citation53 Further analysis revealed a decrease in FC within regions associated with emotional and cognitive regulation, particularly in the limbic system. This observation aligns with the increased MPT. Based on the above results, we speculated that the analgesic effect of EA was a result of the decreased FC of brain regions closely related to emotional and cognitive regulation in the limbic system.
The study also highlights altered EC, particularly between the left septum, the left IC and the right septum. A study regarding neuropathic pain suggested that acupuncture intervention reduced EC from hypothalamus and amygdala to somatosensory cortex which might be one of the mechanisms underlying the pain relief.Citation55 We discovered that compared to the sham-EA group, the right septum to the left septum-directed connectivity was increased, whereas the left septum to the right septum-directed connectivity was decreased in the EA group. The results extended connectivity findings by delineating the direction of influence between the right septum and the left septum. We also found that the left IC to the right septum-directed connectivity was increased, whereas the right septum to the left IC-directed was decreased in the EA group. The anterior limb of the internal capsule (ALIC) is a part of the IC and has structural integration into limbic system.Citation56 It is implicated in mediating emotional distress. The results may indicate emotion regulation in KOA rats. Taken together, the mechanism for EA analgesia may be related to the alterations in directional EC between these brain regions.
It is known that chronic pain also causes psychological changes.Citation57 The research discovered that patients in the late stage of KOA had higher Beck Depression Inventory (BDI) scores compared with those in the early stage.Citation57 Wang et al found that more positive expectation, lower extraversion and more attention to emotion were associated with better effect in relieving pain in KOA patients after 4-week acupuncture intervention.Citation58 However, the subjective experience cannot be evaluated in rat study. Zhang et al carried out open field test (OFT) to evaluate anxiety of chronic migraine rats and found that anxious rats preferred to stand in a safer location.Citation59 Light/dark box or elevated plus-maze tests are also used to assess anxiety-like behaviors.Citation60 It is a challenge to conduct the sensory and emotion assessment of pain experience caused by KOA and then translate findings from animal models to human conditions.Citation61 We emphasize that while our study provides valuable insights into the neural mechanisms of pain relief through electroacupuncture, as evidenced by changes in functional and effective connectivity, it does not fully encapsulate the subjective experience of pain.
One of the pivotal strengths of using fMRI in the study is its ability to localize pain-specific brain regions and neural circuits.Citation62 This specificity is crucial in understanding the complexities of pain and the effects of EA on these pathways. By pinpointing pain-specific brain regions and neural circuits, we can design experiments to explore these areas in greater depth. This approach allows us to delve into the intricate mechanisms at a cellular and molecular level, providing a comprehensive view of how acupuncture influences pain processing pathways.
However, there are several existing limitations in this research. Firstly, while this study primarily focused on MPT to assess pain alleviation, we recognize the significance of incorporating comprehensive behavioral assessments in future research. Such evaluations will enrich our understanding of EA’s overall therapeutic impacts, including improvements in mobility and exploratory behavior, providing a fuller picture of the treatment outcomes in post-ACLT rats. Secondly, the time frame of the study was sufficient to observe significant results, however, assessing the longer-term durability of the induced brain changes in rats would have been beneficial. Thirdly, it is highly meaningful to conduct a clinical study on KOA volunteers to evaluate the efficacy of EA in relieving pain and related mechanism. Furthermore, the sample size will be expanded for further research in the future.
Conclusions
In conclusion, our study demonstrated significant alterations of FC and EC in post-ACLT rats after 3-week EA intervention at ST 32 and ST36 acupoints, mainly involving basal ganglia and limbic system neural connections. This study provides novel insights into the neural mechanisms underlying the analgesic effects of EA in rats following ACLT. By utilizing both FC and EC analyses, we were able to identify specific brain regions and connections that might be involved in the therapeutic effects of EA. These findings have important implications on the development of non-pharmacological treatments for chronic pain conditions, such as KOA.
Abbreviation
Acb, Accumbens; ACLT, Anterior cruciate ligament transection; ANOVA, analysis of variance; DPARSF, Data Processing Assistant for Resting-State fMRI; EA, Electroacupuncture; EC, Effective connectivity; GRE-EPI, Gradient Echo-Echo planar imaging; FC, Functional connectivity; FDR, False discovery rate; GCA, Granger causality analysis; IC, Internal capsule; KOA, knee osteoarthritis; MPT, Mechanical pain threshold; MTG, Middle temporal gyrus; MwoA, Migraine without aura; NRM, Nucleus raphe magnus; PAG, Periaqueductal grey; PWT, Paw withdrawal threshold; ROIs, Regions of interest; RPN, Raphe nuclei; rs-FC, rest-state functional connectivity; rs-fMRI, resting-state functional magnetic resonance imaging; SD, Sprague-Dawley; SPM12, Statistical parametric mapping 12; ZI, Zona incerta.
Ethics Approval and Informed Consent
All the experimental procedures and animal care were approved by the Ethical Committee of Guanghua Hospital of Integrative Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine (Approval No. 2022-K-30). National Institutes of Health Guide for the Care and Use of Laboratory Animals were followed in the entire process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Hall M, van der Esch M, Hinman RS. et al. How does Hip osteoarthritis differ from knee osteoarthritis? Osteoarthritis Cartilage. 2022;30(1):32–41. doi:10.1016/j.joca.2021.09.010
- Vina ER, Kwoh CK. Epidemiology of osteoarthritis: literature update. Curr Opin Rheumatol. 2018;30(2):160–167. doi:10.1097/BOR.0000000000000479
- Gao N, Shi H, Hu S, et al. Acupuncture enhances dorsal raphe functional connectivity in knee osteoarthritis with chronic pain. Front Neurol. 2022;12:813723. doi:10.3389/fneur.2021.813723
- Li B, Jing L, Jia L, et al. Acupuncture reduces pain in rats with osteoarthritis by inhibiting MCP2/CCR2 signaling pathway. Exp Biol Med. 2020;245(18):1722–1731. doi:10.1177/1535370220952342
- Guo J, Chen Y, Li Z, et al. The cerebral mechanism of acupuncture for treating knee osteoarthritis: study protocol for a randomized controlled trial. Trials. 2019;20(1):126. doi:10.1186/s13063-019-3233-7
- Zhao ZQ. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. 2008;85(4):355–375. doi:10.1016/j.pneurobio.2008.05.004
- Xiang X, Wang S, Shao F, et al. Electroacupuncture stimulation alleviates CFA-induced inflammatory pain via suppressing P2X3 expression. Int J Mol Sci. 2019;20(13):3248.
- Kelly RB, Willis J. Acupuncture for Pain. Am Fam Physician. 2019;100(2):89–96.
- Chen N, Wang J, Mucelli A, et al. Electro-acupuncture is beneficial for knee osteoarthritis: the evidence from meta-analysis of randomized controlled trials. Am J Chin Med. 2017;45(5):965–985.
- Ng MM, Leung MC, Poon DM. The effects of electro-acupuncture and transcutaneous electrical nerve stimulation on patients with painful osteoarthritic knees: a randomized controlled trial with follow-up evaluation. J Altern Complement Med. 2003;9(5):641–649. doi:10.1089/107555303322524490
- Mansour AR, Farmer MA, Baliki MN, et al. Chronic pain: the role of learning and brain plasticity Restor Neurol Neurosci. Restorative Neurology and Neuroscience. 2014;32(1):129–139. doi:10.3233/RNN-139003
- Cottam WJ, Iwabuchi SJ, Drabek MM, et al. Altered connectivity of the right anterior insula drives the pain connectome changes in chronic knee osteoarthritis. Pain. 2018;159(5):929–938. doi:10.1097/j.pain.0000000000001209
- Kang BX, Ma J, Shen J, et al. Altered brain activity in end-stage knee osteoarthritis revealed by resting-state functional magnetic resonance imaging. Brain Behav. 2022;12(1):e2479. doi:10.1002/brb3.2479
- Li Y, Wu F, Cheng K, et al. Mechanisms of acupuncture for inflammatory pain. Zhen Ci Yan Jiu. 2018;43(8):467–475. doi:10.13702/j.1000-0607.180196
- Chapin H, Bagarinao E, Mackey S. Real-time fMRI applied to pain management. Neurosci Lett. 2012;520(2):174–181. doi:10.1016/j.neulet.2012.02.076
- Apkarian AV, Bushnell MC, Treede RD, et al. Human brain mechanisms of pain perception and regulation in health and disease. Eur J Pain. 2005;9(4):463–484. doi:10.1016/j.ejpain.2004.11.001
- Guo X, Wang S, Chen YC, et al. Aberrant brain functional connectivity strength and effective connectivity in patients with type 2 diabetes mellitus. J Diabetes Res. 2021;2021:5171618. doi:10.1155/2021/5171618
- Dai P, Zhou X, Ou Y, et al. Altered effective connectivity of children and young adults with unilateral amblyopia: a resting-state functional magnetic resonance imaging study. Front Neurosci. 2021;15:657576. doi:10.3389/fnins.2021.657576
- Hamilton JP, Chen G, Thomason ME, et al. Investigating neural primacy in Major Depressive Disorder: multivariate Granger causality analysis of resting-state fMRI time-series data. Mol Psychiatry. 2011;16(7):763–772. doi:10.1038/mp.2010.46
- Jiao Q, Lu G, Zhang Z, et al. Granger causal influence predicts BOLD activity levels in the default mode network. Hum Brain Mapp. 2011;32(1):154–161. doi:10.1002/hbm.21065
- Zang ZX, Yan CG, Dong ZY, et al. Granger causality analysis implementation on MATLAB: a graphic user interface toolkit for fMRI data processing. J Neurosci Methods. 2012;203(2):418–426. doi:10.1016/j.jneumeth.2011.10.006
- Zhu Y, Dai L, Zhao H, et al. Alterations in effective connectivity of the hippocampus in migraine without aura. J Pain Res. 2021;14:3333–3343. doi:10.2147/JPR.S327945
- Mao CP, Chen FR, Huo JH, et al. Altered resting-state functional connectivity and effective connectivity of the habenula in irritable bowel syndrome: a cross-sectional and machine learning study. Hum Brain Mapp. 2020;41(13):3655–3666. doi:10.1002/hbm.25038
- Huang X, Zhang D, Wang P, et al. Altered amygdala effective connectivity in migraine without aura: evidence from resting-state fMRI with Granger causality analysis. J Headache Pain. 2021;22(1):25. doi:10.1186/s10194-021-01240-8
- Chen Y, Kang Y, Luo S, et al. The cumulative therapeutic effect of acupuncture in patients with migraine without aura: evidence from dynamic alterations of intrinsic brain activity and effective connectivity. Front Neurosci. 2022;16:925698. doi:10.3389/fnins.2022.925698
- Huo BB, Zheng MX, Hua XY, et al. Brain metabolism in rats with neuropathic pain induced by brachial plexus avulsion injury and treated via electroacupuncture. J Pain Res. 2020;13:585–595. doi:10.2147/JPR.S232030
- Xu G, Xiao Q, Zhou J, et al. Acupuncture and moxibustion for primary osteoporosis: an overview of systematic review. Medicine. 2020;99(9):e19334. doi:10.1097/MD.0000000000019334
- Zhang L, Li M, Li X, et al. Characteristics of sensory innervation in synovium of rats within different knee osteoarthritis models and the correlation between synovial fibrosis and hyperalgesia. J Adv Res. 2021;35:141–151. doi:10.1016/j.jare.2021.06.007
- Yang JH, Lv JG, Wang H, et al. Electroacupuncture promotes the recovery of motor neuron function in the anterior horn of the injured spinal cord. Neural Regen Res. 2015;10(12):2033–2039. doi:10.4103/1673-5374.172323
- Liu W, Wang X, Yang S, et al. Electroacupuncture improves motor impairment via inhibition of microglia-mediated neuroinflammation in the sensorimotor cortex after ischemic stroke. Life Sci. 2016;151:313–322. doi:10.1016/j.lfs.2016.01.045
- Huang C, Wang Y, Han JS, et al. Characteristics of electroacupuncture-induced analgesia in mice: variation with strain, frequency, intensity and opioid involvement. Brain Res. 2002;945(1):20–25. doi:10.1016/S0006-8993(02)02503-9
- Nie B, Chen K, Zhao S, et al. A rat brain MRI template with digital stereotaxic atlas of fine anatomical delineations in paxinos space and its automated application in voxel-wise analysis. Hum Brain Mapp. 2013;34(6):1306–1318. doi:10.1002/hbm.21511
- Jang S, Lee K, Ju JH. Recent updates of diagnosis, pathophysiology, and treatment on osteoarthritis of the knee. Int J Mol Sci. 2021;22(5):2619. doi:10.3390/ijms22052619
- Wang X, Chou XL, Zhang LI, et al. Zona incerta: an integrative node for global behavioral modulation. Trends Neurosci. 2020;43(2):82–87. doi:10.1016/j.tins.2019.11.007
- Huang H, Song X, Zhao L, et al. Opposing needling for analgesia and rehabilitation after unilateral total knee arthroplasty: a randomized, sham-controlled trial protocol. Trials. 2020;21(1):385. doi:10.1186/s13063-020-04251-z
- Cai FH, Li FL, Zhang YC, et al. Research on electroacupuncture parameters for knee osteoarthritis based on data mining. Eur J Med Res. 2022;27(1):162. doi:10.1186/s40001-022-00795-9
- Zhao C, Xu H, X A, et al. Cerebral mechanism of opposing needling for managing acute pain after unilateral total knee arthroplasty: study protocol for a randomized, sham-controlled clinical trial. Trials. 2022;23(1):133. doi:10.1186/s13063-022-06066-6
- Zhang S, Wang Y, Zhou M, et al. A bibliometric analysis of traditional Chinese non-pharmacological therapies in the treatment of knee osteoarthritis from 2012 to 2022. Front Neurosci. 2023;17:1097130. doi:10.3389/fnins.2023.1097130
- Raja SN, Carr DB, Cohen M, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
- Guo G, Kong Y, Zhu Q, et al. Cerebral mechanism of Tuina analgesia in management of knee osteoarthritis using multimodal MRI: study protocol for a randomised controlled trial. Trials. 2022;23(1):694. doi:10.1186/s13063-022-06633-x
- Wang QP, Nakai Y. The dorsal raphe: an important nucleus in pain modulation. Brain Res Bull. 1994;34(6):575–585. doi:10.1016/0361-9230(94)90143-0
- Grosso A, Cambiaghi M, Concina G, et al. Auditory cortex involvement in emotional learning and memory. Neuroscience. 2015;299:45–55. doi:10.1016/j.neuroscience.2015.04.068
- Lai HC, Lin YW, Hsieh CL. Acupuncture-Analgesia-mediated alleviation of central sensitization. Evid Based Complement Alternat Med. 2019;2019:6173412. doi:10.1155/2019/6173412
- Borsook D, Upadhyay J, Chudler EH, et al. A key role of the basal ganglia in pain and analgesia--insights gained through human functional imaging. Mol Pain. 2010;6:27. doi:10.1186/1744-8069-6-27
- Gagnon CM, Scholten P, Atchison J, et al. Structural MRI Analysis Of Chronic Pain Patients Following Interdisciplinary Treatment Shows Changes In Brain Volume And Opiate-Dependent Reorganization Of The Amygdala And Hippocampus. Pain Med. 2020;21(11):2765–2776. doi:10.1093/pm/pnaa129
- Zanghì E, Corallo F, Lo Buono V. Diffusion tensor imaging studies on subjects with suicidal thoughts and behaviors: a descriptive literature review. Brain Behav. 2022;12(9):e2711. doi:10.1002/brb3.2711
- Mitrofanis J. Some certainty for the ”zone of uncertainty”? exploring the function of the zona incerta. Neuroscience. 2005;130(1):1–15. doi:10.1016/j.neuroscience.2004.08.017
- Roger M, Cadusseau J. Afferents to the zona incerta in the rat: a combined retrograde and anterograde study. J Comp Neurol. 1985;241(4):480–492. doi:10.1002/cne.902410407
- Yan M, Xiong M, Wu Y, et al. LRP4 is required for the olfactory association task in the piriform cortex. Cell Biosci. 2022;12(1):54. doi:10.1186/s13578-022-00792-9
- Kuner R, Kuner T. Cellular circuits in the brain and their modulation in acute and chronic pain. Physiol Rev. 2021;101(1):213–258. doi:10.1152/physrev.00040.2019
- Yi M, Zhang H. Nociceptive memory in the brain: cortical mechanisms of chronic pain. J Neurosci. 2011;31(38):13343–13345. doi:10.1523/JNEUROSCI.3279-11.2011
- Bushnell MC, Ceko M, Low LA. Cognitive and emotional control of pain and its disruption in chronic pain. Nat Rev Neurosci. 2013;14(7):502–511. doi:10.1038/nrn3516
- Iyer A, Tole S. Neuronal diversity and reciprocal connectivity between the vertebrate hippocampus and septum. Wiley Interdiscip Rev Dev Biol. 2020;9(4):e370. doi:10.1002/wdev.370
- Ma Y, Wang S, Tian Y, et al. Disruption of persistent nociceptive behavior in rats with learning impairment. PLoS One. 2013;8(9):e74533. doi:10.1371/journal.pone.0074533
- Ma ZZ, Lu YC, Wu JJ, et al. Acupuncture induces reduction in limbic-cortical feedback of a neuralgia rat model: a dynamic causal modeling study. Neural Plast. 2020;2020:5052840. doi:10.1155/2020/5052840
- Mithani K, Davison B, Meng Y, et al. The anterior limb of the internal capsule: anatomy, function, and dysfunction. Behav Brain Res. 2020;387:112588. doi:10.1016/j.bbr.2020.112588
- Cardin F, Ambrosio F, Amodio P, et al. Quality of life and depression in a cohort of female patients with chronic disease. BMC Surg. 2012;12 Suppl 1(Suppl 1):S10. doi:10.1186/1471-2482-12-S1-S10
- Wang X, Li JL, Wei XY, et al. Psychological and neurological predictors of acupuncture effect in patients with chronic pain: a randomized controlled neuroimaging trial. Pain. 2023;164(7):1578–1592. doi:10.1097/j.pain.0000000000002859
- Zhang M, Liu Y, Zhao M, et al. Depression and anxiety behaviour in a rat model of chronic migraine. J Headache Pain. 2017;18(1):27.
- Vuralli D, Wattiez AS, Russo AF, et al. Behavioral and cognitive animal models in headache research. J Headache Pain. 2019;20(1):11.
- Burma NE, Leduc-Pessah H, Fan CY, et al. Animal models of chronic pain: advances and challenges for clinical translation. J Neurosci Res. 2017;95(6):1242–1256.
- Zhao Z, Huang T, Tang C, et al. Altered resting-state intra- and inter- network functional connectivity in patients with persistent somatoform pain disorder. PLoS One. 2017;12(4):e0176494.