
Abstract
Background
The economic burden of chronic noncancer pain (CNCP) remains insufficiently documented in primary care.
Purpose
To evaluate the annual direct health care costs and productivity costs associated with moderate to severe CNCP in primary care patients taking into account their pain disability.
Materials and methods
Patients reporting noncancer pain for at least 6 months, at a pain intensity of 4 or more on a 0 (no pain) to 10 (worst possible pain) intensity scale, and at a frequency of at least 2 days a week, were recruited from community pharmacies. Patients’ characteristics, health care utilization, and productivity losses (absenteeism and presenteeism) were documented using administrative databases, pharmacies’ renewal charts, telephone, and self-administered questionnaires. Patients were stratified by tertile of pain disability measured by the Brief Pain Inventory questionnaire.
Results
Patients (number =483) were, on average, 59 years old, mainly women (67.5%), and suffered from CNCP for a mean of 12 years at an average pain intensity of 6.5±1.9. The annual direct health care costs and productivity costs averaged CAD $9,565 (±$13,993) and CAD $7,072 (±$11,716), respectively. The use of complementary health care services accounted for almost 50% of the direct health care costs. The mean adjusted total direct health care costs (considering pain-related hospitalizations only) and productivity costs increased with more pain disability: low disability, CAD $12,118; moderate, CAD $18,278; and severe, CAD $19,216; P=0.001.
Conclusion
The economic burden of CNCP is substantial and increases with the level of pain disability, which suggests the need for and potential benefits of improving CNCP management through specific and adapted treatment plans targeting the impact of pain on daily functioning.
Introduction
Chronic noncancer pain (CNCP) is defined by the International Association for the Study of Pain as a pain persisting beyond the normal healing time for a specific illness or injury.Citation1 It is estimated that more than 25% of the Canadian population is affected by CNCP,Citation2,Citation3 a prevalence that tends to increase in our aging society.Citation4 Based on four European studies published between 1991 and 2002, Ospina and HarstallCitation5 estimated the prevalence of chronic pain to be 35.5%. Affected individuals report lower quality of life,Citation6 experience interferences in their daily activitiesCitation4,Citation7,Citation8 and are at higher risk of suffering from depression and anxiety disorders,Citation4,Citation8 sleep problems,Citation7 and additional comorbid conditions.Citation9
CNCP is associated with substantial direct health care costs. In Quebec (Canada), the annual direct health care costs associated with rheumatoid arthritis, fibromyalgia, and painful neuropathic disorders are estimated to average CAD $10,287 (±$12,728 [2002 values]; $12,257 [2011 values]),Citation10 CAD $4,065 (±$6,798 [2007 values]; $4,339 [2011 values]),Citation11 and CAD $4,163 (±$7,536 [2002 values]; $4,960 [2011 values])Citation12 per patient, respectively. Individuals with CNCP make more physician visits (mean of 12.9 visits per year versus 3.8 visits per year) and have longer hospital stays (mean of 3.9 days versus 0.7 days) than individuals without it.Citation13
Chronic pain also causes substantial productivity losses arising from work absences (absenteeism) and reduced productivity at work (presenteeism).Citation8 A Canadian survey revealed that individuals with CNCP missed an average of 9.3 (95% confidence interval [CI]: 4.7–13.7) workdays annually due to their pain, a number rising to 16.0 (95% CI: 5.1–26.9) among individuals with severe pain.Citation2 In Australia, the productivity costs associated with CNCP are estimated to amount to AU $5.1 billion annually.Citation14
Pain-related direct health care costs and productivity costs yield considerable global societal costs. Total CNCP expenditures represent more than 3% of Finland’s gross national productCitation15 and US $2.1 million per employer annually (1998 values) in the United States.Citation16 More severe pain disability seems to be associated with higher societal costs. Patients with arthritis and rheumatism reporting more disability incurred higher direct health careCitation17,Citation18 and productivity costs.Citation19,Citation20 In the United States, when these costs are considered, the total annual cost of pain was greater than the annual costs of treating heart disease, cancer, and diabetes respectively.Citation21
Although the vast majority of CNCP patients are followed-up in primary care,Citation8 most studies have evaluated the economic burden of CNCP in patients recruited in specialized clinics.Citation18,Citation22–Citation24 The objective of this project was, therefore, to describe the direct health care and productivity costs associated with CNCP among primary care patients. Patients with various diagnoses were considered and the costs were described as a function of their pain disability.
Materials and methods
Study design
As part of the ACCORD Program (Application Concertée des COnnaissances et Ressources en Douleur), a knowledge translation research program in the field of CNCP, a cohort study was conducted (one submitted paper is accepted for publication).Citation25,Citation26 In this cohort study, individuals with CNCP having an active analgesic prescription from a primary care physician were recruited from May 2009–January 2010 in community pharmacies. Patients completed a structured telephone interview and a self-administered questionnaire. Governmental administrative databases, the Régie de l’assurance maladie du Québec (RAMQ; Quebec health insurance board; QC, Canada) and the Maintenance et exploitation des données pour l’étude de la clientèle hospitalière (MED-ÉCHO – a hospitalization database), as well as community pharmacies’ renewal charts were used to document health care use and costs in the year preceding the recruitment. Ethical approvals were obtained from the Comité scientifique et d’éthique de la recherche of the Centre de santé et de services sociaux de Laval (Laval, QC, Canada) and from the Commission d’accès à l’information (QC, Canada). Each patient signed an informed consent form and received a financial compensation of $25 for completing the questionnaires. Pharmacists received a financial compensation of $50 for every consenting patient.
Study population
The study was conducted in the Réseau universitaire intégré de santé de l’Université de Montréal (Montreal, QC, Canada), which encompasses six areas in the province of Quebec (Canada): Mauricie et Centre du Québec; Laval; Montréal; Laurentides; Lanaudière; and Montérégie, representing more than 40% of the population in this province. Based on the Quebec Health Ministry’s atlas, 513 community pharmacies were identified in this territory.Citation27 Among those, a random sampling stratified by region and weighted by the number of pharmacies located within each region was done. To recruit 60 pharmacies, selected pharmacies were sequentially contacted until the target numbers of pharmacies were reached in each region. To recruit 600 patients, each pharmacy had to identify between 10 and 15 consecutive and potentially eligible patients. During the course of the study, additional pharmacies were invited to participate, so as to compensate for those that did not recruit the expected number of patients.
To be eligible, patients had to: 1) be ≥18 years of age; 2) report suffering from noncancer pain for at least 6 months and for a minimum of 2 days per week; 3) rate their average pain in the past 7 days as ≥4 on a 0–10 intensity scale (0= no pain; 10= worst possible pain);Citation28 4) have an active analgesic prescription from a primary care physician; and 5) speak and read French or English. Patients reporting migraine as the only source of pain and those unable to provide informed consent were not eligible. The Canadian Pain Society and the World Health Organization define chronic pain as a pain lasting 6 months or more.Citation29,Citation30 This definition is currently used in research.Citation31 In order to ensure that patients’ pain had some impact on various aspects of their daily functioning, only those who reported pain at least 2 days a week were selected.
Direct health care and productivity costs
Direct health care costs
Direct health care costs, expressed in Canadian dollars, were estimated for each participant based on the health care resources used in the year preceding the recruitment.
All outpatient physician visits, as well as tests and interventions (related and unrelated to CNCP), were documented from the RAMQ database. In this database, a service code is assigned to each of these components, along with the specialty of the professional consulted, the date, the site, and the amount reimbursed by the RAMQ, which was used to estimate the cost of the services. A pain specialist (DL) reviewed all tests and interventions provided to cohort patients in order to identify those related to CNCP.
All visits to emergency rooms (ER) were considered. Costs of these visits were documented from the RAMQ database and they included the costs of the visit, tests and interventions, and physician consultations. For each ER visit, a unitary cost of CAD $270.54 (2011 values) was considered. This cost corresponds to the average provincial cost per ER according the Quebec Health Ministry (Direction de l’allocation des ressources, unpublished data) and accounts for expenses incurred by the health care institution itself, including overheads and consumables. The costs of physician consultation(s), test(s), and intervention(s) provided during the ER stay were those paid by the RAMQ during the year preceding the recruitment (May 2008–January 2009).
All hospitalizations and those related, or possibly related, to CNCP were considered. Hospitalizations were documented from the MED-ÉCHO database, where information regarding the admission date, the primary and secondary diagnoses, the length of stay, and the site are recorded. The hospitalization costs included those of the hospital stay, physician visits, tests, and interventions. The cost of hospital stay represents a per diem cost of CAD $948.73 (2011 values) according the Quebec Health Ministry (Direction de l’allocation des ressources, unpublished data), including overheads and consumables. This cost is the mean provincial cost per day of hospitalization, and it accounts for expenses related to the costs of nursing care, laboratory tests, medications, laundry, food, administration, and maintenance. Physician visit and test/intervention costs provided during hospitalizations were documented from the RAMQ database and corresponded to those reimbursed by the RAMQ from 2008–2009. The primary and secondary diagnostic codes associated with the hospitalizations were reviewed by a pain specialist (DL) (see ) to identify those related or possibly related to CNCP.
The use of nonpharmacological health care services was documented during the telephone interview by asking patients, “Now, I will read a list of different types of therapy that can be used to relieve pain. Please stop me each time I name a therapy you have used in the past.” Overall, 23 therapies were enumerated: relaxation/breathing techniques; meditation; hypnosis; visualization; individual distraction; individual psychotherapy; group psychotherapy; self-help support group; physiotherapy; occupational therapy; hydrotherapy/hot bath/aqua therapy; electrostimulation; intramuscular stimulation; ultrasounds; biofeedback; acupuncture; massotherapy; chiropractic; osteopathy; therapeutic touch; reflexology; Reiki; and magnet therapy. When patients identified a therapy that they had employed, the interviewer then asked them, “Have you used it in the past 6 months?” and if yes, “How frequently did you use it in the past 6 months? Every day, a few times every week, a few times every month, or a few times every year?” Those frequencies were translated into actual numbers of annual visits; every day =260 (annual number of weekdays); a few times every week =104; a few times every month =24; and a few times every year =2. The costs of each visit corresponded to the mean cost per visit in the Montreal area (QC, Canada) as a function of the type of professional consulted, and it varied between CAD $45 and CAD $90 (2007 values).Citation32
Prescribed analgesics dispensed 1 year prior to the recruitment were documented from the RAMQ database or from pharmacies’ dispensing charts; the latter allowed for the documentation of pharmacologic treatments of individuals not insured by the RAMQ for their medications. For each analgesic prescription (new and renewals), the following information was recorded: date of dispensation; common drug denomination; form; dosage; and quantity. Analgesics included acetaminophen, nonsteroidal antiinflammatory drugs, antidepressants, anticonvulsants, muscle relaxants, opioids, antiretroviral therapy, disease-modifying antirheumatic drugs, and antirheumatic biologic agents. Only antidepressants and anticonvulsants recommended for pain treatment were taken into account (see ),Citation33,Citation34 and they were documented for patients not reporting depression or epilepsy. Antiretrovirals were those recommended to treat zona-related painCitation35 (valacyclovir, famciclovir, acyclovir). Prescribed medications to prevent or control the gastrointestinal adverse effects that are frequently reported with analgesics were also documented (laxatives, antacids, gastroprotectants, and antiemetics). The costs of each medication corresponded to those reimbursed by the RAMQ (List of Medications 2011)Citation36 based on the form and the dosage of each product. The pharmacist’s fee for each medication dispensed was also considered. For patients insured by the RAMQ, we used the actual dispensing fee paid by the RAMQ. For patients not insured by the RAMQ, a fee of CAD $7.87, which corresponds to the mean dispensing fee paid by the RAMQ in 2011, was assumed.
To document over-the-counter medications used to treat pain and adverse effects associated with analgesics, patients were asked during the telephone interview: “In the past 6 months, have you taken over-the-counter medications or natural products for pain and for drug-related side effects such as constipation, heartburn, and nausea or vomiting?” The frequency of use was described in terms of every day, a few times every week, a few times every month, and a few times every year, and was later translated into annual numbers of daily recommended doses: every day =365; a few times every week =104; a few times every month =24; and a few times every year =2. Unitary costs were estimated using the McKesson databaseCitation37 (McKesson distributes medications to more than 6,000 community pharmacies in Canada). Daily dosages represented the minimum recommended daily doses of each specific product in the Vigilance Santé ProgramCitation38 – a computerized program that is frequently used in community pharmacies.
Productivity costs
Productivity costs, described in terms of absenteeism and presenteeism, were solely considered for individuals who were currently employed at the time of the interview (full-or part-time job), and for those who were on temporary or permanent disability; they were not considered for unemployed individuals, nor for those who were retired. This information was assessed during the telephone interview, as participants had to choose one of the enumerated choices, which included full- and part-time work and permanent and temporary disabilities.
Absenteeism was documented during the telephone interview using the following question: “In the past 6 months, how many days of work did you miss because of your pain or medical appointment, or treatment for you pain?” To evaluate the annual costs of absenteeism, the reported number of days absent from work due to pain in the past 6 months was multiplied by 2. For individuals with a full- or part-time job, productivity costs were calculated by multiplying the annual number of workdays missed by the mean Canadian hourly wage (CAD $23.06 [2011 values])Citation39 and the mean number of hours worked daily (7.24 hours).Citation40 For individuals on temporary or permanent disability, productivity costs were calculated by multiplying the annual number of workdays missed by the minimum wage as estimated in 2011:Citation41 CAD $9.65/hour; 8 hours/day. For individuals on temporary disability, the annual number of workdays missed represented the reported number of days absent from work due to pain in the past 6 months, multiplied by 2, and for individuals on permanent disability, it corresponded to 260 (annual number of weekdays absent).
As for absenteeism, presenteeism was only estimated for individuals with a full- or part-time job and for those on permanent or temporary disability. Based on the method described by Hu et al,Citation42 presenteeism was evaluated during the telephone interview using the following question: “In the past 6 months, what percentage of your productivity at work did you lose, on average, because of your pain? Please answer using a scale from 0% to 100% where 0% means ‘no loss in productivity’ and 100% means the ‘loss of all productivity’.” Presenteeism was estimated by multiplying the time lost due to pain (the number of workdays with pain by the percent of productivity lost on those days), by the number of hours worked per day (7.24 hours)Citation40 and by the hourly wage (CAD $23.06 [2011 values]).Citation39
Pain disability
The impact of pain on daily functioning was assessed in the telephone interview using the interference items of the modified Brief Pain Inventory (BPI). The BPI is a widely used instrument in pain research and its psychometric qualities are well documented.Citation43,Citation44 It includes ten interference items. For each one, patients are asked to rate, on a 0–10 scale (0= does not interfere, 10= interferes completely), the extent to which pain interferes with various aspects of their daily living including general activity, walking ability, mood, normal work, relations with other people, sleep, enjoyment of life, self-care, recreational activities, and social activities. A global BPI score is derived by taking the average rating on the ten items.Citation43
Patients’ characteristics
Sociodemographic and pain characteristics were documented with the self-administered questionnaire and telephone interview. The characteristics of pain included its duration (time since onset) and frequency in the past week. The circumstances surrounding the onset of the pain and its location(s) were also recorded. Pain diagnoses were based on patients’ self-reports using the following question during the telephone interview: “I will read a list of diagnoses that can be at the origin of your pain. Please stop me each time I read a diagnosis corresponding to your condition.” The list included ten diagnoses, and patients had the opportunity to report diagnoses not included in the list. Diagnoses were then grouped into eight main categories: 1) back pain; 2) neck pain; 3) fibromyalgia; 4) neuropathic pain; 5) visceral pain; 6) inflammatory arthritic pain (for example, rheumatoid arthritis); 7) degenerative arthritic pain (for example, osteoarthritis); and 8) tendinitis, bursitis, capsulitis, and epicondylitis. The impact of pain on sleep was investigated using the Chronic Pain Sleep Inventory,Citation45 while depression and anxiety levels were measured using the Hospital Anxiety and Depression Scale.Citation46 Depression and anxiety scores were rated as “absent” (scores ≤7), “uncertain” (scores between 8–10), or “probable” (scores ≥11). The presence of comorbid conditions was assessed through the Charlson Comorbidity Index, an instrument that takes into account the number and seriousness of comorbid diseases.Citation47
Data analyses
Annual costs were described on the basis of a societal perspective, in terms of direct health care and productivity costs. They were adjusted to 2011 Canadian dollar values based on the consumer price index (Statistics Canada, Ottawa, ON, Canada).Citation48 Taking into account the resources used in the year preceding the recruitment, the costs of hospitalizations, the ER visits, the outpatient physician, and other health care professional visits, pharmacotherapy (prescribed and over-the-counter medications that were used to treat pain and adverse effects associated with analgesic medications), as well as the costs associated with productivity loss due to absenteeism and presenteeism, were computed for each patient. Thereafter, the total direct health care costs and the costs associated with productivity loss were computed. The mean (± standard deviation) of these costs was computed for the entire cohort, as well as by three subcohorts defined by the tertile of the global BPI scores labeled as mild, moderate, and severe disability. The statistical significance of the between subcohort differences was estimated using a univariate linear regression model and chi-square statistics for continuous (for example, annual health care resource use and health care costs) and categorical variables, respectively.
Multivariate linear regression models were also developed to predict the costs as a function of the BPI tertile after adjusting for the following confounders: age;Citation12,Citation17 sex;Citation12 duration of pain;Citation17,Citation49 and the Charlson comorbidity score.Citation22,Citation23,Citation50,Citation51 All variables associated with at least a 10% change in the cost estimate in the univariate analyses were included in the final multivariate model. Given the lack of precision in the identification of hospitalizations related to CNCP, all-cause hospitalizations were considered in this analysis. In a secondary analysis, only pain-related hospitalizations were reported. For each BPI tertile, the mean cost and its 95% CI were calculated. Gamma transformations of costs were employed in all cases.Citation52 Statistical analyses were carried out using SPSS Statistics Base 19.0 for Windows® (IBM Corporation, Armonk, NY, USA) and SAS® Software (version 9.1; SAS Institute Inc., Cary, NC, USA).
Results
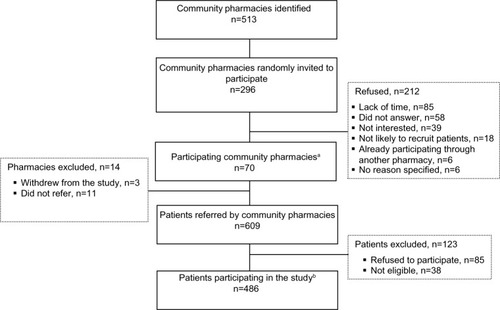
Between May and October 2009, a total of 296 community pharmacies were invited to participate; 84 pharmacies were recruited and 70 completed the study and recruited patients (). Between May 2009 and January 2010, pharmacists referred 609 potentially eligible patients, of whom 38 were ineligible and 85 refused to participate. Data from the community pharmacies’ renewal charts and from the RAMQ and the MED-ÉCHO databases were available for all participants (number [n] =486). Telephone interviews and self-administered questionnaires were completed by 485 and 483 individuals, respectively. Based on the BPI tertile scores, three subcohorts were created and included 483 individuals: mild disability, BPI scores between 0.0–4.30 (n=165); moderate disability, scores between 4.31–6.40 (n=160); and severe disability, scores between 6.41–10.0 (n=158).
Figure 1 Recruitment of pharmacies and patients.
Abbreviation: n, number.
As reported in , participants were middle aged (mean age: 59±13 years), mainly women (67.5%), Caucasian (96.3%), and French-speaking (90.5%). The majority reported having an elementary school diploma or less (27.3%) or a high-school diploma (35.2%) as their highest level of education. Differences were observed between the subcohorts of patients defined by BPI tertile scores; those reporting more severe pain disability were younger, reported lower familial income, and were more likely to be on permanent or temporary disability.
Table 1 Sociodemographic characteristics
Clinical and psychological characteristics
As reported in , on average, individuals suffered from pain for 12 years (±11 years). The proportion of patients reporting a pain duration of 4 years or more tended to be higher among those with more severe pain disability. In terms of pain frequency, the majority (75.2%) were suffering continuously. Patients reported a mean pain intensity score of 6.5 (±1.9) in the past week. Based on the Hospital Anxiety and Depression ScaleCitation46, 24.0% and 40.0% of participants probably suffered from depression and anxiety, respectively. The mean number of reported pain diagnoses per individual was 2.5 (±1.3), the most frequent being chronic back pain (64.0%) and degenerative osteopathies such as osteoarthritis and arthrosis (60.7%). Patients classified in the severe disability category reported more frequent and more intense pain than those in the mild and moderate categories. They were also more likely to feel depressed and anxious, experience more pain-related sleep problems, and suffer from multiple pain syndromes.
Table 2 Clinical and psychosocial characteristics
Health care resource utilization and productivity losses
Individuals were hospitalized for an average of 1.9 (9.9) days annually, where 1.1 (8.3) days were possibly related to CNCP (). Overall, 19.7% of the cohort of patients were hospitalized (all causes considered) and 8.9% of the cohort of patients were hospitalized for a cause that was possibly related to pain (data not reported in table). During this 1-year period, participants visited the ER 0.9 times (±1.6) on average and saw primary care physicians and specialists for an average of 4.8 (±4.9) times and 2.1 (±3.1) times, respectively. Patients reporting more pain disability were more likely to have visited the ER or be seen by primary care physicians and specialists. The majority of participants (56.1%) reported at least one visit to a health care professional other than a physician (data not reported in table), with an annual number of visits per patient averaging 74.6 (±135.5). Physiotherapists and massage therapists were the most frequently seen with an average of 40.3 (±90.1) visits per patient and 13.5 (±48.8) visits per patient, respectively. In terms of pain medication, individuals took an average of 3.9 (±2.0) and 1.5 (±1.6) different prescribed and over-the-counter medications to treat pain and/or the adverse effects of pain treatments, respectively. The number of prescribed medications was the highest among patients classified in the severe pain disability subgroup. Patients with more pain disability were more likely to have opioid analgesics dispensed in the year prior to recruitment: mild, 49%; moderate, 68%; and severe, 80%; P=0.0001. Among those on opioids, 19 patients were dispensed a high oral morphine-equivalent dose (>200 mg per day). These patients were equally distributed across the pain disability subgroups (data not reported in table).
Table 3 Annual health care resource utilization and productivity losses per patient
Work productivity data revealed that individuals lost an equivalent of 69.4 (±111.3) workdays annually due to pain or its treatment; the number of days lost due to absenteeism and presenteeism averaged 57.3 (±106.3) days and 12.1 (±36.0) days, respectively. Annual workdays lost were higher in individuals with more severe pain disability.
Unadjusted direct health care and productivity costs
The mean annual total direct health care costs per patient averaged CAD $7,334 (±$9,276), CAD $11,128 (±$19,131), and CAD $10,311 (±$11,501) for patients with mild, moderate, and severe pain disability, respectively (). Major cost components included nonpharmacologic health care services, which accounted for 47.1% (CAD $4,505/CAD $9,565) of the total direct health care costs, hospitalizations and ER visits (24.6%), prescribed medications (20.5%), and outpatient medical visits (6.3%). For patients with mild, moderate, and severe pain disability, productivity costs per patient averaged CAD $4,523 (±$8,951), CAD $8,254 (±$13,386), and CAD $8,536 (±$12,077), respectively. Absenteeism and presenteeism costs accounted for 71.4% and 28.6% of those costs, respectively. When combining the direct health care costs and productivity costs, the mean annual costs per patient were equal to CAD $11,857 (±$13,685), CAD $19,382 (±$23,228), and CAD $18,847 (±$18,734) for patients with mild, moderate, and severe pain disability, respectively. The costs of hospitalizations, outpatient visits, prescribed medications, and total costs were found to be significantly and positively related to the level of pain disability.
Table 4 Crude annual direct health care costs and productivity costs (CAD dollars) per patient
Adjusted direct health care costs and productivity costs
Once they were adjusted for age, sex, pain duration, and Charlson comorbidity scores, the mean annual direct costs per patient averaged CAD $7,374 (95% CI: $5,819–$8,930), CAD $10,524 (95% CI: $8,383–$12,665), and CAD $9,546 (95% CI: $7,502–$11,590) for patients with mild, moderate, and severe pain disability, respectively (). Productivity costs were CAD $3,005 (95% CI: $1,587–$4,422), CAD $5,083 (95% CI: $2,647–$7,519), and CAD $5,385 (95% CI: $2,789–$7,981) for each group, with total costs adding up to CAD $12,913 (95% CI: $10,534–$15,292), CAD $17,970 (95% CI: $14,782–$21,159), and CAD $17,292 (95% CI: $14,075–$20,510). A significant positive association was observed between the level of pain disability, as well as the total adjusted direct health care costs (considering pain-related hospitalizations only) and productivity costs: mild disability, CAD $12,118; moderate disability, CAD $18,278; and severe disability, CAD $19,216; P=0.001.
Table 5 Adjusted annual direct health care costs and productivity costs (CAD dollars) per patient
Discussion
This is one of the rare studies providing a comprehensive evaluation of the economic burden of CNCP in a large cohort of patients followed up in primary care. The direct health care costs of CNCP in this cohort of patients represented nearly 60% of the total direct health care and productivity costs. The use of complementary health care services accounted for almost 50% of the direct costs. The total direct health care and productivity costs averaged CAD $16,636 per patient per year and varied according to the level of pain disability – the more disabled the patients were, the higher the costs were. Although high, these numbers represent only a portion of the true costs since they do not include other indirect costs such as patients’ travel expenses, paid household help, expenses incurred by family members, and so on.
Complementary health care services (for example, physiotherapy, massage therapy, occupational therapy) are known to be extensively used by individuals with CNCP,Citation7,Citation53 including those with chronic low back pain.Citation54 Not considering these costs may, therefore, lead to an important underestimation of the direct health care costs of CNCP and may explain discrepancies among studies. For example, Lachaine et alCitation12 estimated that the annual direct health care costs associated with neuropathic painful disorders in Quebec (Canada) averaged CAD $4,065 per patient (±$6,798 [2007 values]; $4,339 [2011 values]). In another study on the costs associated with fibromyalgia in Quebec,Citation11 the direct health care costs added up to CAD $4,163 (±$7,536 [2002 values]; $4,960 [2011 values]). Differences with our results might be explained by the fact that complementary health care services were not considered in these studies.
In patients with chronic pain, higher than normal absenteeism rates,Citation2 as well as significant interference with work performance,Citation8 have been reported. In our study, the mean annual cost associated with productivity losses represented about 40% of the total direct health care and productivity costs. This proportion is consistent with earlier observations made in individuals suffering from fibromyalgia syndromeCitation55 and chronic low back painCitation54 where the proportion of costs associated with productivity losses accounted for more than half of the total costs. Similar observations were also made by Guerriere et alCitation24 in a population of chronic pain patients waiting for treatment in tertiary care pain clinics. Although they remain insufficiently documented, presenteeism costs should be systematically taken into consideration, as illustrated by an Australian and an American study where these costs accounted for the majority of the CNCP costs.Citation14,Citation21
When combined, the direct health care costs and productivity costs led to mean annual total costs of CAD $16,636 per patient, which compares with previous estimates in fibromyalgia (US $15,000 [2009 values]; CAD $15,489 [2011 values]),Citation56 chronic low back pain (US $19,473 [2002 values]; CAD $23,566 [2011 values]),Citation54 and osteoarthritis (US $16,146 [2005 values]; CAD $18,189 [2011 values]).Citation57 Other studies have also reported that economic burden increases with the severity of pain disability. For example, among individuals with rheumatoid arthritis, increases in self-report disability status, as measured by the Health Assessment Questionnaire, were associated with higher costs.Citation17,Citation18,Citation58,Citation59 Costs incurred by chronic low back pain and by neuropathic pain were also found to vary as a function of the degree of disability levels.Citation54,Citation60 However, the present study is the first to demonstrate this association for a variety of chronic pain diagnoses in a primary care setting.
Strengths and limitations
Like any other study, the present one has some limitations that must be taken into consideration. Patients were recruited only if they had an active analgesic prescription from a primary care physician in their pharmacy chart. Our results cannot be extrapolated to those having no active analgesic prescriptions or only prescriptions from a specialist. Furthermore, some of our results are based on patient self-reports and may be influenced by social desirability (tendency to answer questions in a manner that will be viewed favorably by others) and memory biases. However, the research assistants who conducted the telephone interviews were well trained and used a structured interview protocol. Self-administered questionnaires were used to document more sensitive information such as levels of depression and anxiety. Some assumptions were also made to estimate the annual costs. Annual productivity costs, as well as annual use of over-the-counter medication and complementary health care services, were estimated using data covering a 6-month period. This may have resulted in an overestimation or underestimation of costs, as resource utilization rates may have changed over time. Furthermore, the frequency of use was not precisely documented. Finally, we took into account the direct costs to patients associated with different self-management techniques (eg cost of physiotherapy). However, we did not consider the impact this may have on caregiver time (eg time absent from work for the patient’s wife).
Despite those limitations, this study offers a comprehensive description of the direct health care costs and productivity costs associated with CNCP. The use of administrative databases and pharmacy charts enabled the precise documentation of prescribed pharmacological treatments of participants, as well as their use of health care resources. Furthermore, we also assessed the use of over-the-counter medication and complementary health care services, both documented through telephone interviews with the patients. The structured interview protocol also allowed for the documentation of productivity losses due to pain or its treatment, which were further translated into productivity costs based on the method previously described by Hu et al.Citation42
Conclusion
CNCP among primary care patients is associated with substantial economic burden not only for the health care system and the workforce, but also for patients themselves. These costs tend to increase as pain causes more limitations in a patient’s daily activities. Further research is clearly needed to improve the management of CNCP in primary care. Finding efficient strategies to reduce further chronicity of pain problems is certainly an avenue that needs to be explored, as it could alleviate not only the burden of illness, but also its associated costs.
Acknowledgments
We are grateful for the excellent collaboration of community pharmacists and patients who took part in this project. This work was conducted as part of the master research project of Alexandra Beaulieu-Boivin. We acknowledge her time and effort in the conduct of this analysis. Special thanks to Chantal Legris for the preparation and submission of this article. Lyne Lalonde and Sylvie Perreault are scientists supported by the Fonds de recherche du Québec – Santé.
Supplementary materials
Table S1 Hospitalization codes related or possibly related to chronic pain
Table S2 Documented analgesics
Disclosure
This study was funded by a team grant – Community Alliances for Health Research and Knowledge Exchange in Pain of the Canadian Institutes of Health Research (CIHR) in partnership with AstraZeneca Canada Inc. (Grant # 86787), and by Pfizer Canada Inc. The authors report no other conflicts of interest in this work.
References
- Classification of chronic pain. Descriptions of chronic pain syndromes and definitions of pain terms. Prepared by the International Association for the Study of Pain, Subcommittee on TaxonomyPain Suppl19863S1S2263461421
- MoulinDEClarkAJSpeechleyMMorley-ForsterPKChronic pain in Canada – prevalence, treatment, impact and the role of opioid analgesiaPain Res Manag20027417918412518174
- BoulangerAClarkAJSquirePCuiEHorbayGLChronic pain in Canada: have we improved our management of chronic noncancer pain?Pain Res Manag2007121394717372633
- MillarWJChronic painHealth Rep199674475351588679957
- OspinaMHarstallCPrevalence of Chronic Pain: An OverviewEdmonton, ABAlberta Heritage Foundation for Medical Research2002 Available from: http://ihe.ca/documents/prevalence_chronic_pain_0.pdfAccessed April 6, 2011
- KerrSFairbrotherGCrawfordMHoggMFairbrotherDKhorKEPatient characteristics and quality of life among a sample of Australian chronic pain clinic attendeesIntern Med J200434740340915271174
- BreivikHCollettBVentafriddaVCohenRGallacherDSurvey of chronic pain in Europe: prevalence, impact on daily life, and treatmentEur J Pain200610428733316095934
- GurejeOVon KorffMSimonGEGaterRPersistent pain and well-being: a World Health Organization Study in Primary CareJAMA199828021471519669787
- McWilliamsLACoxBJEnnsMWMood and anxiety disorders associated with chronic pain: an examination in a nationally representative samplePain20031061–212713314581119
- FautrelBClarkeAEGuilleminFCosts of rheumatoid arthritis: new estimates from the human capital method and comparison to the willingness-to-pay methodMed Decis Making200727213815017409364
- LachaineJBeaucheminCLandryPAClinical and economic characteristics of patients with fibromyalgia syndromeClin J Pain201026428429020393262
- LachaineJGordonAChoinièreMColletJPDionDTarrideJEPainful neuropathic disorders: an analysis of the Régie de l’Assurance Maladie du Québec databasePain Res Manag2007121313717372632
- Agence d’évaluation des technologies et des modes d’intervention en santéManagement of Chronic (Non-Cancer) Pain: Organization of Health ServicesMontreal, QCAgence d’évaluation des technologies et des modes d’intervention en santé2006
- van LeeuwenMTBlythFMMarchLMNicholasMKCousinsMJChronic pain and reduced work effectiveness: the hidden cost to Australian employersEur J Pain200610216116616310720
- KumpusaloEMäntyselkäPTakalaJChronic pain in primary careFam Pract200017435210934187
- PizziLTCarterCTHowellJBVallowSMCrawfordAGFrankEDWork loss, healthcare utilization, and costs among US employees with chronic painDisease Management and Health Outcomes2005133201208
- MichaudKMesserJChoiHKWolfeFDirect medical costs and their predictors in patients with rheumatoid arthritis: a three-year study of 7,527 patientsArthritis Rheum200348102750276214558079
- YelinEWankeLAAn assessment of the annual and long-term direct costs of rheumatoid arthritis: the impact of poor function and functional declineArthritis Rheum19994261209121810366114
- ClarkeAEZowallHLevintonCDirect and indirect medical costs incurred by Canadian patients with rheumatoid arthritis: a 12 year studyJ Rheumatol1997246105110609195508
- BurtonWMorrisonAMacleanRRudermanESystematic review of studies of productivity loss due to rheumatoid arthritisOccup Med (Lond)2006561182716286432
- GaskinDJRichardPThe economic costs of pain in the United StatesJ Pain201213871572422607834
- MaetzelALiLCPencharzJTomlinsonGBombardierCCommunity Hypertension and Arthritis Project Study TeamThe economic burden associated with osteoarthritis, rheumatoid arthritis, and hypertension: a comparative studyAnn Rheum Dis200463439540115020333
- PenrodJRBernatskySAdamVBaronMDayanNDobkinPLHealth services costs and their determinants in women with fibromyalgiaJ Rheumatol20043171391139815229962
- GuerriereDNChoinièreMDionDThe Canadian STOP-PAIN project – Part 2: What is the cost of pain for patients on waitlists of multidisciplinary pain treatment facilities?Can J Anaesth201057654955820414821
- LalondeL [webpage on the Internet]Optimisation de la gestion de la douleur chronique en soins de première ligne [Optimizing the management of chronic pain in ambulatory primary care]ACCORD Regroupment des forces pour gérer la douleur chroniqueMontreal,QC2009 Available from: http://www.programmeaccord.org/volets/premiereligneAccessed April 22, 2013
- JouiniGChoiniereMMartinEPerreaultSBerbicheDLussierDPharmacotherapeutic management of chronic noncancer pain in primary care: lessons for pharmacistsJ Pain Res2014716317324711711
- Atlas de la santé et des services sociaux du Québec! [webpage on the Internet]QuébecSanté et Services sociaux Québec2014 Available from: http://www.msss.gouv.qc.ca/statistiques/atlas/atlas/index.phpAccessed May 12, 2014
- HoffmanDLSadoskyADukesEMAlvirJHow do changes in pain severity levels correspond to changes in health status and function in patients with painful diabetic peripheral neuropathy?Pain2010149219420120303665
- World Health OrganizationA new understanding of chronic painKaplunAHealth Promotion and Chronic Illness Discovering a New Quality of HealthCopenhagen, DenmarkWHO Regional Publications1992141226
- JoveyRDEnnisJGardner-NixJCanadian Pain SocietyUse of opioid analgesics for the treatment of chronic noncancer pain – a consensus statement and guidelines from the Canadian Pain Society, 2002Pain Res Manag20038Suppl A3A28A
- MerskeyHBogdukNClassification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definition of Pain TermsSeattle, WAIASP Press2011
- BeaudryN [webpage on the Internet]Les tarifs des spécialistes de la santé en 2007 [The rates of health care professionals in 2007]Montreal, QCNormandin Beaudry Communiqué. 2007;10(12). Available from: http://www.normandin-beaudry.ca/publications/communiques/archives/2007/vol10-n12.fr.htmlAccessed November 4, 2013
- MoulinDEClarkAJGilronICanadian Pain SocietyPharmacological management of chronic neuropathic pain – consensus statement and guidelines from the Canadian Pain SocietyPain Res Manag2007121132117372630
- O’ConnorABDworkinRHTreatment of neuropathic pain: an overview of recent guidelinesAm J Med2009122Suppl 10S22S3219801049
- HarpazROrtega-SanchezIRSewardJFAdvisory Committee on Immunization Practices (ACIP) Centers for Disease Control and Prevention (CDC)Prevention of herpes zoster: recommendations of the Advisory Committee on Immunization Practices (ACIP)MMWR Recomm Rep200857RR-5130 quiz CE2–CE418528318
- Régie de l’assurance maladie du QuébecList of MedicationsGatineau, QCService des relations avec la clientele2011 Available from: https://www.prod.ramq.gouv.qc.ca/DPI/PO/Commun/PDF/Liste_Med/Liste_Med/liste_med_mod1_2011_12_16_en.pdfAccessed April 22, 2013
- McKesson Canada [homepage on the Internet]McKesson CanadaSan Francisco, CAMcKesson Corporation2013 Available from: https://www.mckesson.caAccessed September 9, 2013
- Vigilance Santé [homepage on the Internet]Vigilance SantéRepentigny, QCVigilance Santé2013 Available from: http://www.vigilance.caAccessed September 9, 2013
- Statistics Canada [webpage on the Internet]Salaires horaires moyens des employés selon certaines caractéristiques et occupations, données non désaisonnalisées, par province (mensuel) (Canada)Ottawa, ONGovernment of Canada2005 Available from: http://www.statcan.gc.ca/tables-tableaux/sum-som/l02/cst02/labr69a-fra.htmAccessed September 9, 2013
- Statistics Canada [webpage on the Internet]Labour force survey estimates (LFS), by sex and detailed age group annual (persons x 1,000)Ottawa, ONGovernment of Canada2014 Available from: http://www5.statcan.gc.ca/cansim/a05?lang=eng&id=2820002Accessed September 9, 2013
- Commission des normes du travail du Québec [webpage on the Internet]History of the minimum wageQuébec, QCCommission des norms du travail Québec Available from: http://www.cnt.gouv.qc.ca/en/wages-pay-and-work/wages/history-of-the-minimum-wage/index.htmlAccessed August 26, 2013
- HuXHMarksonLELiptonRBStewartWFBergerMLBurden of migraine in the United States: disability and economic costsArch Intern Med1999159881381810219926
- CleelandCSRyanKMPain assessment: global use of the Brief Pain InventoryAnn Acad Med Singapore19942321291388080219
- TylerEJJensenMPEngelJMSchwartzLThe reliability and validity of pain interference measures in persons with cerebral palsyArch Phys Med Rehabil200283223623911833028
- KosinskiMJanagapCCGajriaKScheinJPsychometric testing and validation of the Chronic Pain Sleep InventoryClin Ther200729Suppl2562257718164922
- ZigmondASSnaithRPThe hospital anxiety and depression scaleActa Psychiatr Scand19836763613706880820
- CharlsonMEPompeiPAlesKLMacKenzieCRA new method of classifying prognostic comorbidity in longitudinal studies: development and validationJ Chronic Dis19874053733833558716
- Consumer Price Index, historical summary (1994 to 2013) [webpage on the Internet]OttawaStatistics Canada, Government of Canada [updated January 24, 2014]. Available from: http://www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/econ46a-eng.htmAccessed May 12, 2014
- VerstappenSMVerkleijHBijlsmaJWDeterminants of direct costs in Dutch rheumatoid arthritis patientsAnn Rheum Dis200463781782415194577
- WalenHRCronanPABigattiSMFactors associated with healthcare costs in women with fibromyalgiaAm J Manag Care20017Spec NoSP39SP4711599674
- WolfeFRossKAndersonJRussellIJHebertLThe prevalence and characteristics of fibromyalgia in the general populationArthritis Rheum199538119287818567
- ManningWGThe logged dependent variable, heteroscedasticity, and the retransformation problemJ Health Econ199817328329510180919
- FlemingSRabagoDPMundtMPFlemingMFCAM therapies among primary care patients using opioid therapy for chronic painBMC Complement Altern Med200771517506893
- EkmanMJönhagenSHunscheEJönssonLBurden of illness of chronic low back pain in Sweden: a cross-sectional, retrospective study in primary care settingSpine (Phila Pa 1976)200530151777178516094281
- RobinsonRLBirnbaumHGMorleyMASisitskyTGreenbergPEClaxtonAJEconomic cost and epidemiological characteristics of patients with fibromyalgia claimsJ Rheumatol20033061318132512784409
- SilvermanSDukesEMJohnstonSSBrandenburgNASadoskyAHuseDMThe economic burden of fibromyalgia: comparative analysis with rheumatoid arthritisCurr Med Res Opin200925482984019220165
- WhiteAGBirnbaumHGJanagapCButeauSScheinJDirect and indirect costs of pain therapy for osteoarthritis in an insured population in the United StatesJ Occup Environ Med2008509998100518784547
- JacobssonLTLindrothYMarsalLJuranEBergströmUKobeltGRheumatoid arthritis: what does it cost and what factors are driving those costs? Results of a survey in a community-derived population in Malmö, SwedenScand J Rheumatol200736317918317657670
- PugnerKMScottDIHolmesJWHiekeKThe costs of rheumatoid arthritis: an international long-term viewSemin Arthritis Rheum200029530532010805355
- TarrideJEColletJPChoinièreMRousseauCGordonAThe economic burden of neuropathic pain in CanadaJ Med Econ200691–45568