
Abstract
An estimated one million individuals in the US are diagnosed with herpes zoster (HZ; shingles) each year. Approximately 20% of these patients will develop postherpetic neuralgia (PHN), a complex HZ complication characterized by neuropathic pain isolated to the dermatome that was affected by the HZ virus. PHN is debilitating, altering physical function and quality of life, and commonly affects vulnerable populations, including the elderly and the immunocompromised. Despite the availability of an immunization for HZ prevention and several approved HZ treatments, the incidence of PHN is increasing. Furthermore, management of the neuropathic pain associated with PHN is often suboptimal, and the use of available therapeutics may be complicated by adverse effects and complex, burdensome treatment regimens, as well as by patients’ comorbidities and polypharmacy, which may lead to drug–drug interactions. Informed and comprehensive assessments of currently available pharmacological treatment options to achieve effective pain control in the primary care setting are needed. In this article, we discuss the situation in clinical practice, review currently recommended prevention and treatment options for PHN, and outline practical considerations for the management of this neuropathic pain syndrome, with a focus on optimal, individual-based treatment plans for use in the primary care setting.
Postherpetic neuralgia
Postherpetic neuralgia (PHN), a neuropathic pain syndrome resulting from damage to nerve fibers, is the most common complication of herpes zoster (HZ; shingles), and the cause of the greatest HZ-related burden of illness.Citation1–Citation3 HZ is a viral disease caused by the reactivation of varicella zoster virus (VZV) that had remained latent in sensory ganglia since the primary infection (chicken pox), and is characterized by a painful skin rash, usually limited to the area innervated by a single sensory ganglion ().Citation4,Citation5 PHN is usually diagnosed in individuals who have recovered from the HZ skin rash but who have continued to experience pain for at least 3 months, although for some patients pain can persist for years.Citation1–Citation3,Citation6
Figure 1 Herpes zoster (shingles) rash.

PHN pain occurs in the same dermatomes as the HZ rash, and is likely the result of damage to the nervous system (which may include deafferentation, peripheral and/or central sensitization, myelin destruction, inflammation, and signaling errors in the brain) that occurred during the proliferation and spread of the virus during the acute HZ infection.Citation1,Citation3,Citation7 The syndrome has consequences permeating multiple aspects of patients’ lives, affecting their sleep, concentration, and mood, as well as impacting their physical functionality by interfering with activities of daily living.Citation8,Citation9
As many as 20% of patients with HZ develop PHN. Major risk factors include advanced age and decreased immunity.Citation1,Citation10–Citation12 Approximately half of all PHN cases occur in persons older than 60 years. Therefore, the incidence of HZ and risk of PHN is likely to increase as the population ages.Citation13,Citation14 The declining cell-mediated VZV immunity from immune senescence also contributes to the observed increased prevalence of PHN in the elderly.Citation15,Citation16 Finally, the severity of the acute HZ infection and the presence of a notable prodrome have also been associated with increased likelihood of experiencing PHN.Citation1,Citation10–Citation12
Practical considerations for management of PHN
For primary care providers, PHN may not present as a distinct entity but rather an extension of the original HZ infection, and monitoring for a global condition affecting multiple aspects of patients’ lives rather than for a localized post-HZ pain is paramount. Thus, practical management of PHN can be divided into prevention and treatment of HZ, and the more challenging task of managing the neuropathic pain syndrome and its consequences once PHN has developed ().Citation17,Citation18
Figure 2 Current postherpetic neuralgia (PHN) prevention and treatment options.
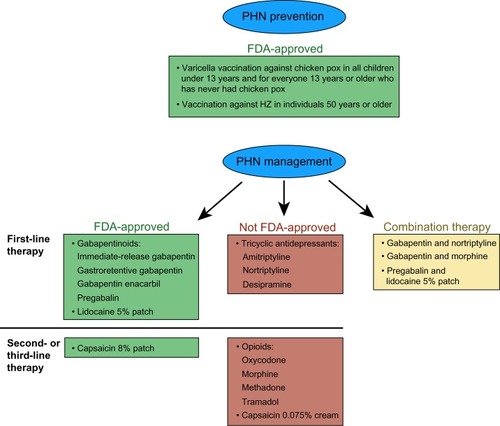
To date, no cure for PHN exists, only treatments that are palliative and that may shorten the duration and severity of the pain. Therefore, vaccinations to prevent initial chicken pox and thus VZV from ever gaining a foothold in the body in the first place, or vaccinations to prevent reactivation of VZV already present in the body remain a priority; however, there are uncertainties about the vaccines’ duration of protection and/or how frequently booster can be given.Citation19–Citation21 For patients who were exposed to VZV and who contracted acute HZ, the primary care provider may use antivirals, analgesics, or corticosteroids to decrease acute pain and possibly decrease the risk of developing PHN.Citation17,Citation22,Citation23
Despite the availability of vaccination, a communication gap between primary medical providers and patients hinders satisfactory prevention of VZV and HZ. PHN incidence is on the rise, the effective management of PHN remains an ongoing challenge, and no single best therapy has yet been identified.Citation24,Citation25 Current guidelines for management of PHN pain recommend gabapentinoids (gabapentin and pregabalin), tricyclic antidepressants (TCAs), opioids, topical agents, and combination therapies with different mechanisms of action ().Citation26–Citation28 However, the US Food and Drug Administration (FDA) has only approved four oral systemic medications, all of which are gabapentinoids, and two topical analgesics specifically for the management of pain associated with PHN ().
A carefully devised, individually based treatment plan is critical to ensure optimal outcomes in the management of PHN. Pain and its interference with daily activities are subjective symptoms and difficult to manage effectively, even more so in older patients, who are predominantly afflicted with PHN, and who are more likely to have multiple chronic health issues and declining function and frailty.Citation29,Citation30 A significant number of patients who develop chronic pain associated with PHN do not receive evidence-based, recommended treatment modalities, leaving many patients undertreated and dissatisfied with the treatment.Citation24,Citation31,Citation32 To ensure optimal results, the initial choice of PHN pain therapy should be guided not only by drug efficacy but also by the patient’s comorbidities, severity of PHN pain, the drugs’ adverse-event and drug-interaction profiles, titration regimen, and patient preference, especially since no single therapy has demonstrated superior effectiveness. Because PHN is a complex condition and should not be simplified to a localized area of pain, the most practical therapeutic approach may involve a systemic medication or combination therapy rather than topical analgesics alone. Finally, clear communication with the patient and frequent monitoring of adverse reactions and patient satisfaction with the treatment should be established.
Adverse effects can be a major limiting factor for many therapies. TCAs have anticholinergic adverse effects, and may cause balance problems and cognitive impairment in elderly patients.Citation33,Citation34 In addition, the recently published update of the Beers criteria by the American Geriatrics SocietyCitation35 identified TCAs as a class of drugs to avoid in older adults. Elderly patients treated with opioid analgesics can experience mobility problems, increased risk of hip fracture, and cognitive impairment.Citation30,Citation33,Citation36 Also, given the complexity of opioid management, the American Pain Society and American Academy of Pain Medicine have suggested cautious initiation and titration of opioids in frail older persons or those with comorbidities.Citation37 Gabapentinoids have a better safety profile than other oral therapeutics, although they can be associated with high incidence of dizziness, swelling, confused thinking, and somnolence.
Other factors, such as titration and treatment regimen, drug interactions, drug efficacy, and modes of administration or application, can also limit the use of several PHN treatment options. Topical agents, especially the lidocaine 5% patch, have a favorable safety profile, but they can be impractical for PHN involving the head and face, can have a burdensome application regimen (ie, capsaicin cream and patch), and can be ineffective as a monotherapy. Gabapentinoids can have complex and burdensome titration schedules often based on three-times-daily dosing. Among new formulations, gastroretentive gabapentin can simplify the patient’s daily medication burden, improve patient acceptance and compliance with simpler once-daily dosing, and lower incidence of adverse events compared with other gabapentinoids. Furthermore, both topical lidocaine patches and gabapentinoids are good candidates for combination therapy, due to their low propensity for interactions with other drugs.
PHN prevention
Vaccination
With continued widespread use of varicella vaccine (Varivax®; Merck, Whitehouse Station, NJ, USA)Citation38 in childhood, primary medical providers may expect to prevent initial VZV infection (chicken pox) and subsequent HZ (shingles) later in life, but varicella vaccine failed to provide long-term protection from VZV.Citation19 One approach to the prevention of PHN in those already harboring VZV involves the administration of the VZ vaccine (Zostavax®; Merck), which has been approved by the FDA for individuals 50 years of age or older.Citation39 The Zostavax® vaccine, which activates specific T-cell production and thus prevents viral reactivations, was found to be effective in reducing the burden of illness due to HZ, incidence of HZ, and incidence of PHN, and was well tolerated, with minor systemic and injection-site adverse events.Citation20,Citation40,Citation41 However, despite the promising results of immunization, data are still insufficient to support long-term prevention of HZ and PHN, and similarly to varicella vaccine, the zoster vaccine protection my wane over time.Citation18,Citation20,Citation21,Citation42 Also, the vaccine remains widely underused, mainly due to the surprising lack of vigilant recommendation by primary care providers as well as lack of awareness of HZ and the HZ vaccine.Citation43,Citation44
Treatment of HZ
Although still controversial, early treatment of HZ with antiviral agents may decrease the risk of developing or duration of PHN.Citation45 Three antiviral agents are approved in the US for the treatment of HZ: acyclovir (Zovirax®; GlaxoSmithKline, Brentford, UK), famciclovir (Famvir®; Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA), and valacyclovir (Valtrex®; GlaxoSmithKline).Citation46–Citation48 To limit the amount of viral replication and reduce the duration of the HZ rash, antivirals should be administered within 72 hours of rash onset.Citation49 They may be beneficial as long as new lesions are actively being formed, which is important to note, since in clinical practice the diagnosis of HZ is rarely made within 72 hours. However, the safety and efficacy of antivirals in treating HZ or preventing PHN more than 72 hours after rash onset have not been established.Citation46–Citation48
Antivirals alone are not sufficient to relieve the acute pain associated with HZ. Mild-to-moderate pain can be controlled with a short-acting opioid with acetaminophen or a nonsteroidal anti-inflammatory agent, and gabapentinoids, followed by a TCA, can be added for more severe acute pain. Furthermore, the combination of gabapentin and valacyclovir administered acutely in patients with HZ may reduce the incidence of PHN.Citation50 Although not recommended routinely for treatment of HZ and most likely ineffective in preventing PHN, corticosteroids are often considered in clinical practice for HZ patients with limited contraindications.Citation17,Citation22,Citation23,Citation51
PHN management
Therapies approved by the FDA
Oral therapies
Gabapentinoids (also known as calcium channel α2-δ ligands) are the only oral medications to date approved by the FDA for the management of PHN, and they are an effective and one of the most commonly used first-line therapies for chronic PHN pain (). As gabapentinoids are excreted by the kidneys, dosages should be adjusted according to creatinine clearance in patients with renal impairment.
For immediate-release gabapentin (generic gabapentin or Neurontin®; Pfizer, New York, NY, USA), three-times-daily dosing is recommended ().Citation52 Although in clinical practice, alternate dosing may be prescribed, the recommended number of daily doses should not be exceeded. The most effective therapeutic dosage of immediate-release gabapentin is 1,800 mg/day,Citation53 while additional benefit of using greater dosages was not demonstrated, and long titration times to reach this optimal dosage may be required.Citation52 A retrospective study of medical claims revealed patients took on average 10 weeks to reach 1,800 mg/day immediate-release gabapentin, and only 14% of patients reached the target dosage.Citation54 Immediate-release gabapentin has been associated with a relatively high rate of adverse events (28% of patients reported dizziness and 21% of patients reported somnolence in clinical trials).Citation52
Table 1 Recommended dosages and side effects of medications for treating postherpetic neuralgia (PHN) pain
Treatment with immediate-release gabapentin may be inadequate, due to intolerable drug side effects, long titration periods to reach therapeutic dosages, and low compliance with frequent daily dosing. To improve the efficacy, safety, and tolerability of PHN therapy through simplified dosing regimens and shorten titration periods, two extended-release formulations of gabapentin were developed and recently approved by the FDA for the treatment of PHN: gastroretentive gabapentin (Gralise®; Depomed, Newark, CA, USA), approved in 2011,Citation55 and gabapentin enacarbil (Horizant®; XenoPort, Santa Clara, CA, USA), approved in 2012Citation56 (). The dosing regimen for gastroretentive gabapentin is reduced to once daily, and a majority of patients (over 90%) reach therapeutic dosage within 2 weeks.Citation57 Gabapentin enacarbil is dosed twice daily with a 4-day to 1-week titration period.Citation58 Neither of these new formulations was directly compared to the immediate-release gabapentin, but gastroretentive gabapentin was associated with fewer adverse events in clinical trials (11% for dizziness and 5% for somnolence),Citation55 while similar incidence of adverse events was reported for gabapentin enacarbil (22% for dizziness and 27% for somnolence).Citation55,Citation56
Pregabalin (Lyrica®; Pfizer) is a successor to immediate-release gabapentin, approved for the treatment of PHN in 2005.Citation59 It is dosed two or three times a day and requires a 1-week titration (), although a retrospective study of medical claims revealed patients required 5–9 weeks to reach therapeutic dosages.Citation59 In clinical trials, pregabalin was associated with slightly higher rates of adverse events than immediate-release gabapentin (approximately 29% of patients reported dizziness and 18% of patients reported somnolence).Citation59
Topical therapies
Two FDA-approved topical therapies are available for PHN treatment: the lidocaine 5% patch (Lidoderm®; Endo, Chadds Ford, PA, USA)Citation60 as a first-line therapy, and the capsaicin 8% patch (Qutenza®; Acorda Therapeutics, Ardsley, NY, USA)Citation61 as a second-line therapy (). The lidocaine 5% patch provides modest pain relief for some patients in comparison to oral therapies, but it has a favorable safety and tolerability profile (). The capsaicin 8% patch has shown only minimal analgesic efficacy in patients with PHN.Citation18 Initial pain during treatment with the capsaicin patch is a significant problem, and topical anesthetic is recommended before application. Also, the capsaicin 8% patch needs to be administered by or under close supervision of a medical provider or trained personnel, as capsaicin is a highly irritant material.Citation61
Therapies not approved by the FDA
Oral therapies
Tricyclic antidepressants
Although not approved by the FDA, TCAs have been commonly used for the treatment of pain associated with PHN since the early 1980s. Amitriptyline, nortriptyline, and desipramine are antidepressants currently recommended as first-line therapies (). Clinical experience indicates that TCAs can be efficacious in relieving neuropathic pain, although they display a relatively slow onset of action, and the medical literature shows that they do not work as well in patients with certain types of pain common in PHN (ie, burning pain or allodynia).Citation18,Citation62 TCAs are often poorly tolerated, and are associated with significant systemic adverse events and cardiac toxicity (), which require considerable caution when treating older patients, the population that is the most prevalent for developing PHN. Amitriptyline is the most widely prescribed TCA, but desipramine and nortriptyline are associated with fewer side effects.Citation18,Citation33,Citation63
Opioids
Natural and synthetic opioids (eg, oxycodone, morphine, methadone, and tramadol) are used in PHN management, although they are not approved by the FDA for that indication (). They are available as fast-acting (2–6 hours of analgesia) or as long-acting (8–24 hours of analgesia). Great concern exists regarding the risks of side effects, the possibility of misuse, and potential for abuse or diversion associated with opioids, and they have been recommended as a second-line therapy for the treatment of pain associated with PHN ().Citation18 Also, patients will develop physical dependence, and opioid analgesics must be used cautiously.
Topical therapy
Similarly to the capsaicin 8% patch, over-the-counter capsaicin 0.075% cream has shown minimal analgesic effect in patients with PHN, and it is recommended as a second- or third-line therapy ().Citation18 Initial pain during treatment with capsaicin cream, which has to be applied multiple times daily, is the leading cause of treatment discontinuations.Citation64
Combination therapies
A single drug is not capable of modifying all of the complex pain mechanisms that underlie PHN, and thus may not provide sufficient pain relief. Consequently, the use of at least two therapies with different, complementary mechanisms of action that target multiple sites along the PHN pain pathway () may result in better analgesia.Citation27,Citation28 In addition, it may be important to consider how therapeutics act on the ascending spinothalamic pain pathway (which communicates from the body to the brain, initiating the conscious realization of pain) or the descending corticospinal pain pathway (which communicates from the brain to the body, inhibiting pain). For example, there is logic to using gabapentin to calm the ascending pain pathway and decrease pain, and TCAs to enhance the descending pathway and modulate pain, or to using gabapentin and the topical lidocaine patch, which both affect the ascending pain pathway, with gabapentin affecting central sensitization and lidocaine affecting peripheral sensitization.
The most attractive agents for combination therapies are gabapentinoids and topical analgesics, due to their low propensity for interactions with other drugs.Citation52,Citation55,Citation56,Citation59–Citation61 The combination of pregabalin and the lidocaine 5% patch was effective in patients with PHN who did not previously respond to either medication as monotherapy, and the treatment was generally well tolerated, with most adverse events attributed to pregabalin.Citation18 Clinical studies suggest that gabapentin combined with nortriptyline or morphine yields better reduction in PHN pain than either agent alone.Citation18 The rate of adverse events was not higher for combined therapies than for monotherapies in clinical studies, but the rate of drug-specific adverse events remained high, especially for the TCA and opioid.Citation18
Clinical practice
Primary care is essential and frequently the front line in the diagnosis and treatment of PHN. Drug costs and insurance plans are an unfortunate reality in clinical practice, and are often major considerations and limiting factors in the management of PHN. Thus, because of cost, generic immediate-release gabapentin is often the first-choice medication. Unfortunately, the most effective dosage of 1,800 mg/day is frequently not attained,Citation54 which may leave patients undertreated. This may occur because treatment is terminated if any adverse events occur, or because in their attempt to avoid such adverse events as dizziness and somnolence, practitioners are tentative in the titration regimen they use. Although in certain patients, significant reductions in pain can be achieved at immediate-release gabapentin dosages lower than 1,800 mg/day, regular evaluations are crucial to ensure these patients continue to receive an adequate therapeutic response with lower dosages over time.
With failure of generic immediate-release gabapentin, other formulations of gabapentin are usually considered (most insurance plans will cover gastroretentive gabapentin or pregabalin). At this point, the most optimal choice should be based not just on costs but also on the profile of adverse events and ease of titration. The lidocaine 5% patch may be used in combination with any gabapentinoid for better management of pain, although it is expensive. The lidocaine 5% patch seems a better choice than the capsaicin 8% patch, which is not only expensive but also painful and not practical, as its application takes several hours of medical providers’ and patients’ time. Patients who have failed attempts at treatment may be referred to a specialty pain practice, where the approach is often to retry medications at lower dosages to avoid adverse events, or to get patients to therapeutic dosages to evaluate whether they had a true therapeutic failure or an inadequate trial leading to unsuccessful treatment. However, only a small proportion of patients suffering from PHN consult specialty care, so many of them remain undertreated and dissatisfied with the treatment. Thus, the ideal therapeutic approach may be better utilization of available treatment options and careful evaluation of PHN management at the level of primary care.
As the Patient Protection and Affordable Care Act is being implemented, a sizable physician shortage is predicted, and physician assistants and nurse practitioners are predicted to fill the gap in primary care.Citation65 Therefore, more mid-level providers may coordinate the acute treatment of HZ in urgent-care settings or primary care offices, and they will be responsible for the surveillance and management of PHN. PHN is a complex condition, is difficult to treat, and requires a methodical therapeutic approach, and physician assistants and nurse practitioners are critical in coordinating team-based and patient-centered care.
Conclusion
Optimal management of pain in PHN patients is complex and difficult. Although there are several therapeutic options, PHN treatment is often inadequate, leaving patients undertreated. Better utilization of available options and multimechanistic approaches to PHN management based on the patient’s individual characteristics may be the most beneficial. Primary care plays a crucial role in the development and implementation of the PHN treatment plan, and establishing effective communication with patients. Well-devised and well-executed PHN therapy will not only ensure sufficient pain relief but will also facilitate improvements in patients’ physical and psychosocial functions.
We conducted a comprehensive literature search for peer-reviewed articles about HZ and PHN using the PubMed search engine and relevant Medical Subject Headings (MeSH) terms and keywords. Identified studies included those that evaluated the treatment of HZ and/or PHN in terms of efficacy and safety. The same search was repeated for review articles, including meta-analyses and systematic reviews. Additional searches included bibliographies of the retrieved articles, and Medline searches using the names of authors who had published several articles on HZ or PHN. We first reviewed titles and abstracts for relevance, and selected articles were then reviewed on their entirety. Included articles were English-language studies, addressed epidemiology and burden of HZ, were prospective or retrospective studies that provided clinical information on treated patients, provided detailed methodology and clear outcome measures, demonstrated treatment/prevention of HZ or PHN as a primary purpose, and described treatments feasible for an outpatient setting approved by the FDA or adhering to current guidelines on the care of PHN patients.Citation26–Citation28 Studies and reviews that included other conditions were only included if results were reported separately for each condition. Studies that described case reports or case series were excluded.
Acknowledgment
Iwona Bucior, PhD of Depomed Inc., provided medical writing support.
Disclosure
The authors report no conflicts of interest in this work.
References
- WatsonPPostherpetic neuralgiaAm Fam Physician201184669069221916395
- TontodonatiMUrsiniTPolilliEPost-herpetic neuralgiaInt J Gen Med2012586187123109810
- HarpazRNagelMASchmaderKTyringSKYawnBPRoundtable on postherpetic neuralgia – what, why, how long, and what’s next?Popul Health Manag201215638539023088665
- FrischSGuoAMDiagnostic methods and management strategies of herpes simplex and herpes zoster infectionsClin Geriatr Med201329250152623571042
- Centers for Disease Control and PreventionShingles (herpes zoster)2011 Available from: http://www.cdc.gov/shingles/aboutAccessed January 15, 2014
- RedaHGreeneKRiceFLRowbothamMCPetersenKLNatural history of herpes zoster: late follow-up of 3.9 years (n=43) and 7.7 years (n=10)Pain2013154102227223323719573
- BaronRMechanisms of postherpetic neuralgia – we are hot on the scentPain2008140339539619004555
- PickeringGLeplegeAHerpes zoster pain, postherpetic neuralgia, and quality of life in the elderlyPain Pract201111439740221199312
- DroletMBrissonMLevinMJA prospective study of the herpes zoster severity of illnessClin J Pain201026865666620842005
- WeaverBAHerpes zoster overview: natural history and incidenceJ Am Osteopath Assoc2009109Suppl 2S2S619553632
- JungBFJohnsonRWGriffinDRDworkinRHRisk factors for postherpetic neuralgia in patients with herpes zosterNeurology20046291545155115136679
- OpsteltenWZuithoffNPvan EssenGAPredicting postherpetic neuralgia in elderly primary care patients with herpes zoster: prospective prognostic studyPain2007132Suppl 1S52S5917379412
- ChristensenKDoblhammerGRauRVaupelJWAgeing populations: the challenges aheadLancet200937496961196120819801098
- US Census BureauNational population projection summary tables2012 Available from: http://www.census.gov/prod/2011pubs/12statab/pop.pdfAccessed January 15, 2014
- BennettGJWatsonCPHerpes zoster and postherpetic neuralgia: past, present and futurePain Res Manag200914427528219714266
- JohnsonRWHerpes zoster and postherpetic neuralgia: a review of the effects of vaccinationAging Clin Exp Res200921323624319571648
- GanEYTianEATeyHLManagement of herpes zoster and post-herpetic neuralgiaAm J Clin Dermatol2013142778523456596
- HardenRNKayeADKintanarTArgoffCEEvidence-based guidance for the management of postherpetic neuralgia in primary carePostgrad Med2013125419120223933906
- GoldmanGSKingPGReview of the United States universal varicella vaccination program: herpes zoster incidence rates, cost-effectiveness, and vaccine efficacy based primarily on the Antelope Valley Varicella Active Surveillance Project dataVaccine201331131680169422659447
- DroletMOxmanMNLevinMJVaccination against herpes zoster in developed countries: state of the evidenceHum Vaccin Immunother2013951177118423324598
- BilckeJOgunjimiBHulstaertFVan DammePHensNBeutelsPEstimating the age-specific duration of herpes zoster vaccine protection: a matter of model choice?Vaccine201230172795280021964056
- FashnerJBellALHerpes zoster and postherpetic neuralgia: prevention and managementAm Fam Physician201183121432143721671543
- ThakurRPhilipAGChronic pain perspectives: treating herpes zoster and postherpetic neuralgia: an evidence-based approachJ Fam Pract201261Suppl 9S9S1523000670
- SaksGMUnmet need in the treatment of postherpetic neuralgiaAm J Manag Care201319Suppl 1S207S21323448093
- KlompasMKulldorffMVilkYBialekSRHarpazRHerpes zoster and postherpetic neuralgia surveillance using structured electronic dataMayo Clin Proc201186121146115321997577
- DubinskyRMKabbaniHEl-ChamiZBoutwellCAliHPractice parameter: treatment of postherpetic neuralgia: an evidence-based report of the Quality Standards Subcommittee of the American Academy of NeurologyNeurology200463695996515452284
- DworkinRHO’ConnorABAudetteJRecommendations for the pharmacological management of neuropathic pain: an overview and literature updateMayo Clin Proc201085Suppl 3S3S1420194146
- AttalNCruccuGBaronREFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revisionEur J Neurol20101791113e8820402746
- RastogiRMeekBDManagement of chronic pain in elderly, frail patients: finding a suitable, personalized method of controlClin Interv Aging20138374623355774
- AbdullaAAdamsNBoneMGuidance on the management of pain in older peopleAge Ageing201342Suppl 1i1i5723420266
- GlauserTASalinasGDNevinsHWilliamsonJCWallaceMSAbdolrasulniaMCommunication gaps between physicians and patients with postherpetic neuralgia: results from a national study on practice patternsJ Pain Res2011440741522247624
- DworkinRHPanaritesCJArmstrongEPMaloneDCPhamSVIs treatment of postherpetic neuralgia in the community consistent with evidence-based recommendations?Pain2012153486987522356792
- DworkinRHSchmaderKETreatment and prevention of postherpetic neuralgiaClin Infect Dis200336787788212652389
- PickeringGPereiraBClereFCognitive function in older patients with postherpetic neuralgiaPain Pract Epub5232013
- American Geriatrics Society Beers Criteria Update Expert PanelAmerican Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adultsJ Am Geriatr Soc201260461663122376048
- LabiancaRSarzi-PuttiniPZuccaroSMCherubinoPVellucciRFornasariDAdverse effects associated with non-opioid and opioid treatment in patients with chronic painClin Drug Investig201232Suppl 15363
- ChouRFanciulloGJFinePGClinical guidelines for the use of chronic opioid therapy in chronic noncancer painJ Pain200910211313019187889
- MerckVarivax [prescribing information]2013 Available from: http://www.merck.com/product/usa/pi_circulars/v/varivax/varivax_pi.pdfAccessed January 15, 2014
- MerckZostavax [prescribing information]2006 Available from: http://www.merck.com/product/usa/pi_circulars/z/zostavax/zostavax_pi2.pdfAccessed January 15, 2014
- OxmanMNLevinMJJohnsonGRA vaccine to prevent herpes zoster and postherpetic neuralgia in older adultsN Engl J Med2005352222271228415930418
- GagliardiAMGomes SilvaBNTorloniMRSoaresBGVaccines for preventing herpes zoster in older adultsCochrane Database Syst Rev201210CD00885823076951
- SchmaderKEOxmanMNLevinMJPersistence of the efficacy of zoster vaccine in the shingles prevention study and the short-term persistence substudyClin Infect Dis201255101320132822828595
- CohenEJPrevention of herpes zoster: we need to do betterJAMA Ophthalmol2013131339639823494045
- JavedSJavedFMaysRMTyringSKHerpes zoster vaccine awareness among people ≥50 years of age and its implications on immunizationDermatol Online J2012188222948052
- BruxelleJPinchinatSEffectiveness of antiviral treatment on acute phase of herpes zoster and development of post herpetic neuralgia: review of international publicationsMed Mal Infect2012422535822169279
- GlaxoSmithKline AustraliaZovirax [prescribing information]2013 Available from: http://www.gsk.com.au/products_prescription-medicines_detail.aspx?view=153Accessed February 6, 2014
- NovartisFamvir [prescribing information]2013 Available from: http://www.pharma.us.novartis.com/product/pi/pdf/Famvir.pdfAccessed February 3, 2014
- GlaxoSmithKlineValtrex [prescribing information]2013 Available from: http://us.gsk.com/products/assets/us_valtrex.pdfAccessed January 15, 2014
- WoodMJShuklaSFiddianAPCrooksRJTreatment of acute herpes zoster: effect of early (<48 h) versus late (48–72 h) therapy with acyclovir and valaciclovir on prolonged painJ Infect Dis1998178Suppl 1S81S849852981
- LapollaWDigiorgioCHaitzKIncidence of postherpetic neuralgia after combination treatment with gabapentin and valacyclovir in patients with acute herpes zoster: open-label studyArch Dermatol2011147890190721482862
- HanYZhangJChenNHeLZhouMZhuCCorticosteroids for preventing postherpetic neuralgiaCochrane Database Syst Rev20133CD00558223543541
- PfizerNeurontin [prescribing information]2012 Available from: http://labeling.pfizer.com/ShowLabeling.aspx?id=630Accessed January 15, 2014
- BackonjaMGlanzmanRLGabapentin dosing for neuropathic pain: evidence from randomized, placebo-controlled clinical trialsClin Ther20032518110412637113
- JohnsonPBeckerLHalpernRSweeneyMReal-world treatment of post-herpetic neuralgia with gabapentin or pregabalinClin Drug Investig20133313544
- DepomedGralise [prescribing information]2012 Available from: http://www.gralise.com/lib/PDFS/GRALISE_PI.pdfAccessed January 15, 2014
- XenoPortHorizant [prescribing information] Available from: http://www.horizant.com/docs/Horizant_PrescribingInformation.pdfAccessed January 15, 2014
- IrvingGASweeneyMTolerability and safety of gastroretentive once-daily gabapentin tablets for the treatment of postherpetic neuralgiaJ Pain Res2012520320822792006
- ZhangLRainkaMFreemanRA randomized, double-blind, placebo-controlled trial to assess the efficacy and safety of gabapentin enacarbil in subjects with neuropathic pain associated with postherpetic neuralgia (PXN110748)J Pain201314659060323602345
- PfizerLyrica [prescribing information]2013 Available from: http://labeling.pfizer.com/ShowLabeling.aspx?id=561Accessed January 15, 2014
- EndoLidoderm [prescribing information] Available from: http://www.endo.com/File%20Library/Products/Prescribing%20Information/LIDODERM_prescribing_information.htmlAccessed January 15, 2014
- Acorda TherapeuticsQutenza [prescribing information] Available from: http://www.qutenza.com/_docs/qutenza_full_PI_.pdfAccessed January 15, 2014
- SaartoTWiffenPJAntidepressants for neuropathic pain: a Cochrane reviewJ Neurol Neurosurg Psychiatry201081121372137320543189
- WatsonCPVernichLChipmanMReedKNortriptyline versus amitriptyline in postherpetic neuralgia: a randomized trialNeurology1998514116611719781549
- WatsonCPTylerKLBickersDRMillikanLESmithSColemanEA randomized vehicle-controlled trial of topical capsaicin in the treatment of postherpetic neuralgiaClin Ther19931535105268364943
- StempniakMClosing the primary care gapHosp Health Netw2013873455223617120
- WolffKJohnsonRFitzpatrickTBFitpatrick’s color atlas and synopsis of clinical dermatology5th EdNew YorkMcGraw-Hill Education2005