
Abstract
Background
Previous research has shown positive relationships between dysfunctional cognitive styles and different aspects of pain (eg, pain frequency). One goal of our longitudinal study was to investigate potential risk factors for the incidence of headache (HA) and back pain (BP).
Methods
In the first wave (2003), questionnaires were sent to 6,400 children between the ages of 9 and 14 years. Those who answered in wave 1 were contacted again every year (four survey waves in total: 2003–2006). The data presented are based on the children’s self-reports in the second wave (2004) and third wave (2005). Potential risk factors (dysfunctional stress coping, pain catastrophizing, anxiety sensitivity, and somatosensory amplification) were collected in wave 2. Binary logistic regression analyses – for boys and girls – were performed to assess the predictive value of the risk factors for HA and BP in wave 3.
Results
In the comprehensive model, none of the examined variables predicted the incidence of HA. Anxiety sensitivity increased the risk that boys would report BP after 1 year by 50% and dysfunctional stress coping increased the risk by 40%. For girls, somatosensory amplification increased the risk of the incidence of BP 1 year later by 80%, whereas pain catastrophizing reduced the risk by 50%.
Conclusion
In this incidence sample, the amount of variance explained by the psychological variables investigated was very small. Integrating this result with existing findings from cross-sectional studies suggests that dysfunctional cognitive processing styles may develop more as a consequence or a concomitant feature of BP or HA, but play a less important role in its initial development.
Introduction
In recent years, pain in children and adolescents has attracted growing attention. Epidemiological studies show that headache (HA) and back pain (BP) frequently occur in this age group and are often accompanied by psychological problems.Citation1,Citation2 “Dysfunctional stress coping strategies” refer to maladaptive cognitive or behavioral reactions to stress and strain.Citation3 Postal surveys showed that children with recurrent HA (HA twice per week or more) used more dysfunctional stress coping strategies in stressful situations, such as passive avoidance, rumination, resignation, and irritable behavior, than did children without HA.Citation4 However, the causal relationships between stress, dysfunctional stress coping, and HA are still far from understood. Are stress and dysfunctional stress coping risk factors for the development of HA, or does HA increase the risk of stressful experiences and dysfunctional coping?Citation5,Citation6 With regard to BP, the situation is comparable. Stress as a causative factor has rarely been investigated in children.Citation7
Many researchers have investigated to what extent certain appraisals, expectations, and beliefs regarding pain and body sensations, such as pain catastrophizing, anxiety sensitivity, and somatosensory amplification, are correlated with pain. “Catastrophizing” denotes an exaggerated negative cognitive and behavioral preoccupation with pain,Citation8 characterized by an increased attentional focus on pain cognitions, an overestimation of the negative consequences of pain (eg, damage), and the experience of helplessness with regard to pain.Citation9 Several cross-sectional studiesCitation8,Citation10,Citation11 and one prospective studyCitation12 have found correlations between pain and catastrophizing in children. The construct of “anxiety sensitivity” originated in the context of models of panic disorder and was only subsequently examined with respect to its role in pain experiences.Citation13 Anxiety sensitivity is the disposition of a person to be fearful regarding their own bodily reactions, which are experienced as threatening and dangerous. High anxiety sensitivity increases the fear of pain and may result in avoidance behavior, which may maintain the pain.Citation14,Citation15 “Somatosensory amplification”Citation16 denotes the disposition to focus one’s attentions and perceptions on one’s bodily sensations. This focus is accompanied by a catastrophizing interpretation of these sensations. The concept overlaps to a certain extent with the construct of anxiety sensitivity, but the former places greater emphasis on the perceptional and attentional focus than the latter. Those with high somatosensory amplification may be more prone to chronic pain.Citation17 In their review, Duddu et alCitation18 conclude that the evidence points to a complex, but still unclear, relationship between somatic symptoms and underlying cognitions and illness behaviors.
The objective of the present study was the unidirectional analysis of potential causal factors for the development of pain by means of a longitudinal design. Although temporal priority is not sufficient to establish a causal role for any factor, temporal priority is a necessary condition for such a causal role. We hypothesized that a dysfunctional cognitive processing style, operationalized as dysfunctional stress coping, catastrophizing, anxiety sensitivity, and somatosensory amplification, would increase the risk for the incidence of recurrent pain. In addition, the question of whether these factors exert a differential influence depending on the pain site (HA or BP) is addressed. Since there is evidence of sex-specific effects,Citation8,Citation19 whether the potential risk factors had a different effect in boys and in girls was also investigated.
Methods
Participants
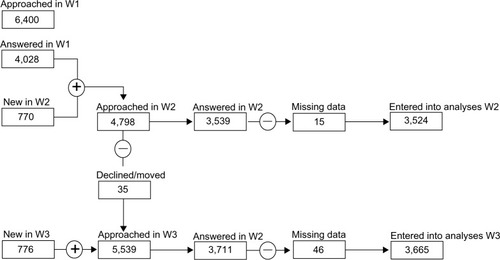
The “KiJuKo” study consisted of a postal survey that was conducted in four waves (W1–W4) in four consecutive years (2003–2006). In the first wave (W1: 2003), 6,400 randomly selected households with a child aged 9–14 years received questionnaires. All participants in W1 were invited to participate again in the following years. The data presented here are based on the children’s and adolescents’ questionnaires from the second (W2: 2004) and third (W3: 2005) waves.
The number of participants in W2 was n=3,524 (73.5% of those contacted). Responder characteristics and selection features are given in . The average age of the children in W2 was 11.25 years (± standard deviation 2.28 years; range 8–15 years) and the proportion of boys was 49.5%.Citation20
Figure 1 Flowchart showing numbers of participating children from W1 to W3.
Abbreviations: W1, wave 1 (2003); W2, wave 2 (2004); W3, wave 3 (2005).
Questionnaire
The KiJuKo questionnaire was developed on the basis of an extensive literature survey and clinical experience. Whenever possible, the operationalization of the potential risk factors was based on established instruments (see ). Detailed information regarding the development of the questionnaire and the procedures, as well as the results of the first wave, has already been published elsewhere.Citation21
Study design
In order to predict the incidence of HA and BP, the questionnaires of all children who did not have HA or BP in W2, but who developed HA or BP 1 year later in W3, were selected for the logistic regression (incidence samples: HA, n=1,665; BP, n=2,040; see and ).
Figure 2 Flowchart for the headache incidence sample.
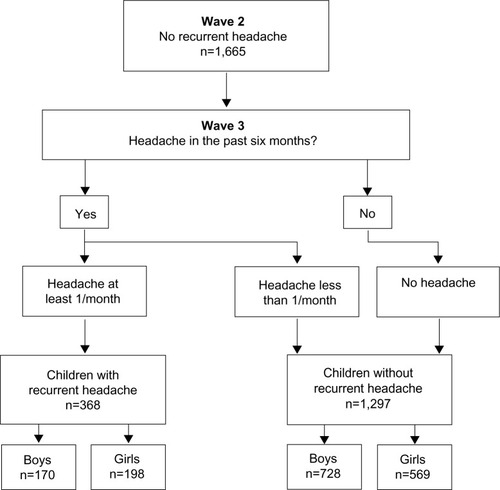
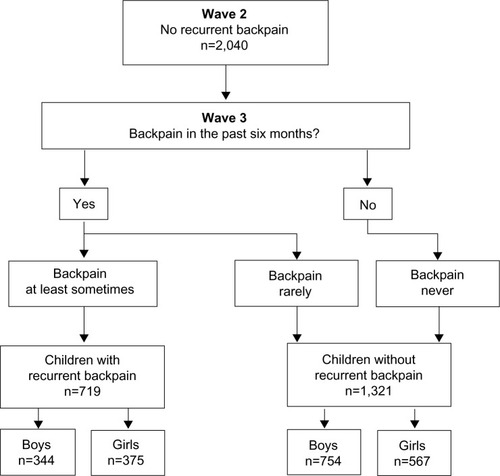
Figure 3 Flowchart for the back pain incidence sample.
In each wave, the reported HA frequencies within the last 6 months (based on the children’s own reports) were allocated to one of four categories: no HA, HA less than once per month, HA at least once per month, and HA at least once per week. For the regression, the criterion variable was dichotomized in two groups: recurrent HA in W3 “present”, ie, HA once or more per month (n=368, 22.1%), and “not present”, ie, HA less than once per month (n=1,297, 77.9%).
Information on the frequency of BP was collected by means of a 5-point rating scale ranging from “never” to “always”. For BP, a dichotomous variable was generated in analogy to the dependent variable HA, with BP classed as recurrent BP if the child reported having experienced BP at least “sometimes” in the last 6 months. In W3, the number of children with recurrent BP was 719 (35.2%) and without recurrent BP was 1,321 (64.8%). Thus, for both HA and BP, the variables were dichotomized. The cut-off was chosen between “never”/“not at all” (not present =0) and “rarely”/“a little” (present =1), because we assumed that younger children could distinguish more reliably between “no, I never had HA/BP” and “yes, I have had HA/BP” (independently of the frequency of the pain). As an added advantage, dichotomizing facilitates the interpretation of the results.
Apart from age and sex, potential predictors collected in W2 with the children’s and adolescents’ questionnaires (–) were the following variables: dysfunctional stress coping, pain catastrophizing, anxiety sensitivity, and somatosensory amplification. It should be noted that the pain catastrophizing items were only filled in by children 11 years and older, because pilot studies (data on file, 2003) had shown them to be too difficult for younger children.
Table 1 Dependent variable (criterion 1): headache frequency in the last 6 months (wave 3)
Table 2 Control variables for headache: age and sex (wave 2)
Table 3 Predictor variables for headache (wave 2)
Table 4 Dependent variable (criterion 2): back pain in the last 6 months (wave 3)
Table 5 Control variables for back pain: age and sex (wave 2)
Table 6 Predictor variables for back pain (wave 2)
The satisfactory internal consistency (Cronbach’s alpha: α≥0.7Citation22 in this study from 0.71 to 0.88; see ) allowed an aggregation of the items belonging to one predictor into a mean scale score per predictor. For the analyses, the predictor variables were dichotomized in the same way as the criterion variables, ie, the reference category is “no/never”.
Statistical analyses
The data were analyzed by means of a binary logistic regression following the recommendations of Field.Citation23 Multicollinearity was excluded on the basis of variance inflation factors and tolerances.Citation24 All variance inflation factor values lay within the range 1–2, indicating that no multicollinearity was present.
In a first step, the predictive values of age and sex with regard to recurrent HA and BP were examined through univariable analyses. Since, in these preliminary analyses, sex emerged as an important factor for the incidence of HA (P<0.05; odds ratio [OR] =1.67; 95% confidence interval [CI] =1.19–2.33) and BP (P<0.05; OR =1.81; 95% CI =1.05–3.09), further analyses were conducted separately for boys and girls. Age was analyzed as a continuous variable and was only relevant in the analyses regarding HA (P=<0.05; OR =1.14; 95% CI =1.01–1.28).
On the basis of these univariable models, all variables with a P-value <0.25 were entered into the multivariable regression model.Citation25 All statistical analyses were conducted using SPSS software (v 14; SPSS Inc., Chicago, IL, USA).
Results
The frequencies for the criterion, control, and predictor variables for HA are reported in – and for BP in –.
Prediction of HA incidence
For boys, none of the variables contributed to the development of HA, as no significant ORs were found in the univariable or multivariable analyses (). Age was included as a control variable in each univariable analysis, and it was found that regardless of the variable investigated the risk of developing HA decreased with increasing age (all ORs for age in these analyses lay between 0.76 and 0.87, P<0.05).
Table 7 Summary of univariable and multivariable logistic regression analyses predicting the incidence of headache in boys and girls
In the univariable analyses for girls, dysfunctional stress coping and somatosensory amplification emerged as influential factors for the incidence of HA 1 year later. For girls who used dysfunctional stress coping, the risk of developing HA was 2.1 times as great compared to girls who never used dysfunctional stress coping. Girls who interpreted bodily sensations in the sense of somatosensory amplification had a 1.5-fold increased risk of developing HA 1 year later. However, both variables lost their significance when they were considered in a multivariable model. Age was irrelevant in all analyses (P>0.10).
Prediction of BP incidence
In the univariable analyses for boys, dysfunctional stress coping, anxiety sensitivity, and somatosensory amplification exerted an influence on the development of BP after 1 year (). As in the case of HA in boys, age was relevant across all analyses (P<0.05; OR =1.07–1.21).
Table 8 Summary of univariable and multivariable logistic regression analyses predicting the incidence of back pain in boys and girls
The results of the multivariable model pointed to the importance of dysfunctional stress coping and anxiety sensitivity. The risk of developing BP increased by 1.4 if boys reported dysfunctional stress coping (reference: boys who reported that they “never” used these strategies). Anxiety sensitivity increased the risk by 1.5.
Age was shown to be relevant in the multivariable model (P<0.001; OR =1.17; 95% CI =1.08–1.25), ie, with every year of a boy’s life, the risk of developing BP increased by approximately 1.2. The model only explained a very small amount of variance (Nagelkerke’s R2: 0.049).
For girls, only somatosensory amplification was influential in univariable analyses. In the multivariable model, pain catastrophizing emerged as a further relevant factor separate from somatosensory amplification. Girls who focused more sensitively on bodily sensations had a 1.8-fold increased risk of reporting BP 1 year later. Increased pain catastrophizing reduced the risk of developing BP. Girls who reported a catastrophizing style of pain appraisal when they experienced pain had a reduced risk (0.5) of developing BP 1 year later. Age was not relevant in the multivariable model (P>0.10). This model also explained a very small amount of variance (Nagelkerke’s R2: 0.036).
Discussion
The purpose of the study was to examine the role of cognitive processing styles for the new occurrence of HA and BP in youths in a 1-year follow-up. To the best of the authors’ knowledge, this is the first study to contrast potential risk factors for the incidence of BP and HA.
In agreement with our expectations and the findings of existing research, several variables of those we examined proved to be predictors for the development of pediatric pain with differing risk profiles for the development of HA and BP. Our results confirmed existing findings concerning sex-specific effects: more girls than boys experience (6 months’ prevalence)Citation26 and develop (incidence) HA and BP.Citation27 Moreover, our results agree with reported findingsCitation19,Citation28 that different factors seem to be relevant for girls and for boys. For boys, none of the variables examined was a risk factor for the incidence of HA. For girls, dysfunctional stress coping and somatosensory amplification showed an influence on the development of HA when analyzed individually, but not when entered into the multivariable model.
For BP, univariable and multivariable analyses showed that dysfunctional stress coping and anxiety sensitivity predicted the development of BP 1 year later for boys. With respect to BP in girls, somatosensory amplification emerged as a factor increasing risk, while pain catastrophizing reduced the risk of developing recurrent BP 1 year later.
In the following discussion, we only refer to the results of the multivariable models, since it is only in this way that the relative impact of the individual variables can be assessed.
The present findings only agree partially with existing studies. Several authors found that children with recurrent HA exhibit more dysfunctional stress coping strategies than children without HA.Citation4,Citation29,Citation30 It was the aim of this study to investigate whether the incidence of HA and BP can be predicted on the basis of dysfunctional stress coping, ie, whether children who showed more dysfunctional stress coping at the time of the first survey would go on to develop recurrent HA 1 year later; clearly, this was not the case, as none of the variables investigated was a predictor for the development of HA. Other studies investigated only correlations between these variables in a cross-sectional study design.Citation30,Citation31 Studies that employed a longitudinal design investigated potential predictors that were not the focus of the present study.Citation32,Citation33
We used a strictly unidirectional design to assess whether cognitive processing styles influence the development of HA. Taken together, our findings and the reports of studiesCitation4,Citation29,Citation30 that found an association between HA and dysfunctional coping suggest that HA possibly precedes dysfunctional cognitive processing styles. The causal direction may be from HA to dysfunctional cognitive processes, rather than vice versa. It is possible that repeated experiences of HA lead to children developing dysfunctional pain coping.
For boys, dysfunctional stress coping predicted the new onset of BP. Thus, one can conclude, with some caution, that a dysfunctional stress coping style in the sample described is only predictive for BP in boys. The first longitudinal study in children for the new onset of pain symptoms (lower BP) found that children who reported high levels of psychosocial difficulties, especially conduct problems and hyperactivity, were 1.6 times more likely to develop lower BP.Citation7 Mustard et al found that the risk of the incidence of BP was associated with both low (OR =1.86; 95% CI =1.14–3.03) and moderate/high (OR =1.85; 95% CI =1.07–3.02) levels of psychological distress.Citation34 On the other hand, Brattberg reported that stress perceived in childhood/adolescence did not predict future pain or stress.Citation35
In pediatric pain research, connections between catastrophizing and pain characteristics have been reported,Citation10,Citation12 with stronger catastrophizing in girls than in boys.Citation8 In the present study, however, pain catastrophizing appeared to be relevant for the development of BP in girls, but, surprisingly, in the opposite direction: catastrophizing reduced the risk of reporting BP 1 year later. This unexpected result has to be considered in the context of the fact that only children of 11 years and older filled in the questionnaire, because pilot studies showed the questions to be too difficult for younger children. However, the response rate for the Pain Catastrophizing Scale for Children items was still lower than for other items, something which was observed throughout all waves. This could be due to the fact that the questions may still have been challenging for the children. Therefore, this result will have to be confirmed in further longitudinal analyses before potential explanations can be sought.
For boys, anxiety sensitivity played a role in the development of BP, whereas, for girls, no influence on the development of HA or BP was found.Citation36 In line with existing research,Citation28 we found that girls achieved higher scores for Anxiety Sensitivity Index than boys. However, these scores do not appear to have a predictive role for BP; such a role we found only for boys.
For girls, somatosensory amplification maintains its risk-aggravating influence if it is considered in the comprehensive model. This result supports indications that those individuals who introspect and who have a tendency to select and focus on relatively weak or infrequent sensations (the main elements of somatosensory amplification) might be more prone to experiencing BP.Citation37
What was unexpected was the fact that the variables examined did not have an effect regarding the incidence of HA, but only regarding the development of BP. Future research will have to examine and replicate this result before definite conclusions can be reached.
When considering the results in comparison to those reported in the literature, it has to be taken into account that the present data were collected from a population sample. The findings of NagelCitation38 support the trend previously reported by Crombez et alCitation8 and Vervoort et al,Citation10 that catastrophizing is more pronounced in clinical samples than in population samples. This argument might also extend to the other psychological constructs and, in our view, may explain the diverging results.
Overall, only a small proportion of the observed variance (for BP: boys, 4.9%, girls, 3.6%) could be explained through the psychological variables we examined. For the prediction of the incidence of recurrent pain, other predictors, which were not considered in the present models, seem to be relevant (see, for example, Kröner-Herwig et alCitation39). Furthermore, it is conceivable that the factors investigated play a more prominent role in the maintenance or exacerbation of recurring pain than in its development.
Strengths and limitations
A particular strength of the present study is the collection of longitudinal data from a large population sample and its use of a strictly defined incidence sample. Moreover, in its investigation of pediatric pain, it was not limited to a single pain site or to the isolated consideration of single psychological variables.
The large population-based study design, however, necessitated the use of self-report measures and precluded any etiological, clinical diagnosis; as a consequence, it is not possible to distinguish between the various subtypes of HA and BP, and, in particular, whether it was a primary or secondary type. This limitation should be taken into account when interpreting the results.
In this study, the interval considered was 1 year. When interpreting the results, the possibility should be taken into account that the influence of certain risk factors may only be observable after a longer period of latency and may thus not be detectable on the basis of the 1-year follow-up data presented here.
A further limitation is the reduction of the sample size that resulted from the fact that we restricted ourselves to the analysis of incidence. This constituted a very strict criterion and thus led to a considerable reduction in the sample size. However, our methodology followed the methodological demands with regard to the development of prognostic modelsCitation40 that only those participants who do not exhibit a certain feature (eg, pain) at time t1, but develop this at a later time, t2, are included.
In this study, we considered pain frequency. Some researchers advocate the incorporation of pain intensity or impairment resulting from pain; these aspects were not discussed in the present study.
Conclusion
In a longitudinal design using strictly defined incidence samples, we investigated whether cognitive processing styles played a role in the development of HA and BP in boys and girls. Although the influence of the individual variables differed between HA and BP and between boys and girls, the overall role for cognitive styles on the initial development of these conditions was very small.
Acknowledgments
This research project has been supported by a grant from the German Ministry of Education, Research and Science (BMBF) (Grant 01 EM 0521) as part of the German Headache Consortium. We acknowledge the support by the German Research Foundation and the Open Access Publication Fund of the Göttingen University.
Supplementary material
Table S1 Instruments with which the predictor variables (wave 2) were measured
References
- HampelPPetermannFDickowBStressverarbeitungsfragebogen von Janke und Erdmann angepasst für Kinder und Jugendliche (SVF-KJ) [Stress Management Questionnaire by Janke and Erdmann Adapted for Children and Adolescents (SVF-KJ)]GöttingenHogrefe2001
- BarskyAJWyshakGKlermanGLThe somatosensory amplification scale and its relationship to hypochondriasisJ Psychiatr Res1990243233342090830
- ReissSPetersonRAGurskyDMMcNallyRJAnxiety sensitivity, anxiety frequency and the prediction of fearfulnessBehav Res Ther198624183947307
- BlaisMAOttoMWZuckerBGThe anxiety sensitivity index: item analysis and suggestions for refinementJ Pers Assess20017727229411693859
- CrombezGBijttebierPEcclestonCThe child version of the pain catastrophizing scale (PCS-C): a preliminary validationPain200310463964612927636
- NagelASchmerzkatastrophisierung bei Kindern und Jugendlichen mit Kopfschmerzen: Validierung einer Deutschen Version der Pain Catastrophizing Scale for Children [Pain Catastrophizing in Children and Adolescents with Headache: Validity of a Germany Version of the Pain Catastrophizing Scale for Children] [diploma thesis]GöttingenGeorg-August-Universität Göttingen2006 German
Disclosure
The authors report no conflicts of interest in this work.
References
- Roth-IsigkeitAThyenURaspeHHStövenHSchmuckerPReports of pain among German children and adolescents: an epidemiological studyActa Paediatr20049325826315046285
- HeinrichMMorrisLKröner-HerwigBSelf-report of headache in children and adolescents in Germany: possibilities and confines of questionnaire data for headache classificationCephalalgia20092986487219250286
- LazarusRSFolkmanSStress, Appraisal, and CopingNew York, NYSpringer Publishing Company1984
- SaileHScallaPChronische Kopfschmerzen und Stress bei Kindern [Chronic headaches and stress in children]Z Klin Psychol Psychiatr Psychother200635188195 German
- WaldieKEChildhood headache, stress in adolescence, and primary headache in young adulthood: a longitudinal cohort studyHeadache20014111011168598
- Bandell-HoekstraIAbu-SaadHHPasschierJKnipschildPRecurrent headache, coping, and quality of life in children: a reviewHeadache20004035737010849029
- JonesGTWatsonKDSilmanAJSymmonsDPMacfarlaneGJPredictors of low back pain in British schoolchildren: a population-based prospective cohort studyPediatrics200311182282812671119
- CrombezGBijttebierPEcclestonCThe child version of the pain catastrophizing scale (PCS-C): a preliminary validationPain200310463964612927636
- SullivanMJLBishopSRPivikJThe Pain Catastrophizing Scale: development and validationPsychol Assess19957524532
- VervoortTGoubertLEcclestonCBijttebierPCrombezGCatastrophic thinking about pain is independently associated with pain severity, disability, and somatic complaints in school children and children with chronic painJ Pediatr Psychol20063167468316093515
- LynchAMKashikar-ZuckSGoldschneiderKRJonesBAPsychosocial risks for disability in children with chronic back painJ Pain2006724425116618468
- VervoortTEcclestonCGoubertLBuysseACrombezGChildren’s catastrophic thinking about their pain predicts pain and disability 6 months laterEur J Pain201014909619359203
- ReissSPetersonRAGurskyDMMcNallyRJAnxiety sensitivity, anxiety frequency and the prediction of fearfulnessBehav Res Ther198624183947307
- AsmundsonGJNortonPJVelosoFAnxiety sensitivity and fear of pain in patients with recurring headachesBehav Res Ther19993770371310452173
- NortonPJAsmundsonGJAnxiety sensitivity, fear, and avoidance behavior in headache painPain200411121822315327826
- BarskyAJWyshakGKlermanGLThe somatosensory amplification scale and its relationship to hypochondriasisJ Psychiatr Res1990243233342090830
- AkISayarKYontemTAlexithymia, somatosensory amplification and counter-dependency in patients with chronic painThe Pain Clinic2004164351
- DudduVIsaacMKChaturvediSKSomatization, somatosensory amplification, attribution styles and illness behaviour: a reviewInt Rev Psychiatry200618253316451877
- HampelPPetermannFAge and gender effects on coping in children and adolescentsJ Youth Adolesc2005347383
- GassmannJMorrisLHeinrichMKröner-HerwigBOne-year course of paediatric headache in children and adolescents aged 8–15 yearsCephalalgia2008281154116218727649
- Kröner-HerwigBHeinrichMMorrisLHeadache in German children and adolescents: a population-based epidemiological studyCephalalgia20072751952717598791
- NunnallyJCBernsteinIHPsychometric Theory3rd edNew YorkMcGraw-Hill1994
- FieldADiscovering Statistics Using SPSS3rd edLondonSage Publications Ltd2009
- TabachnickBGFidellLSUsing Multivariate Statistics4th edBostonAllyn and Bacon2001
- HosmerDWLemeshowSApplied Logistic Regression2nd edNew YorkJohn Wiley & Sons, Inc2000
- BrattbergGWickmanVPrevalence of back pain and headache in Swedish school children: a questionnaire surveyThe Pain Clinic19925211220
- BrattbergGThe incidence of back pain and headache among Swedish school childrenQual Life Res19943Suppl 1S27S317866367
- WalshTMStewartSHMcLaughlinEComeauNGender differences in Childhood Anxiety Sensitivity Index (CASI) dimensionsJ Anxiety Disord20041869570615275947
- Luka-KrausgrillUReinholdBKopfschmerzen bei Kindern: Auftretensrate und Zusammenhang mit Streß, Streßbewältigung, Depressivität und sozialer Unterstützung [Headaches in children: incidence rate and association with stress, stress management, depression and social support]Zeitschrift für Gesundheitspsychologie19964137151 German
- Bandell-HoekstraIEAbu-SaadHHPasschierJFrederiksCMFeronFJKnipschildPCoping and quality of life in relation to headache in Dutch schoolchildrenEur J Pain2002631532112161097
- LateefTMMerikangasKRHeJHeadache in a national sample of American children: prevalence and comorbidityJ Child Neurol20092453654319406755
- LaimiKMetsähonkalaLAnttilaPOutcome of headache frequency in adolescenceCephalalgia20062660461216674770
- RheeHPrevalence and predictors of headaches in US adolescentsHeadache20004052853810940091
- MustardCAKalcevichCFrankJWBoyleMChildhood and early adult predictors of risk of incident back pain: Ontario Child Health Study 2001 follow-upAm J Epidemiol200516277978616150891
- BrattbergGDo pain problems in young school children persist into early adulthood? A 13-year follow-upEur J Pain2004818719915109969
- DeaconBJValentinerDPGutierrezPMBlackerDThe Anxiety Sensitivity Index For Children: factor structure and relation to panic symptoms in an adolescent sampleBehav Res Ther20024083985212074377
- HasenbringMIRusuACTurkDCFrom Acute to Chronic Back Pain: Risk Factors, Mechanisms, and Clinical ImplicationsOxfordOxford University Press2012
- NagelASchmerzkatastrophisierung bei Kindern und Jugendlichen mit Kopfschmerzen: Validierung einer Deutschen Version der Pain Catastrophizing Scale for Children [Pain Catastrophizing in Children and Adolescents with Headache: Validity of a German Version of the Pain Catastrophizing Scale for Children] [diploma thesis]GöttingenGeorg-August-Universität Göttingen2006 German
- Kröner-HerwigBMorrisLHeinrichMBiopsychosocial correlates of headache: what predicts pediatric headache occurrence?Headache20084852954418042227
- HöflerMStatistik in der Epidemiologie psychischer Störungen[Statistics in the Epidemiology of Mental Disorders]BerlinSpringer Verlag2004 German