
Abstract
Background
Pregabalin is an α2δ ligand indicated in the USA for treatment of a number of chronic pain conditions, including diabetic peripheral neuropathy, postherpetic neuralgia, pain associated with spinal cord injury, and fibromyalgia. A greater understanding of when patients first respond to treatment with pregabalin and when adverse events emerge, or worsen, could aid design of new proof-of-concept studies and help guide treatment of patients.
Methods
This was an analysis of five randomized, placebo-controlled, double-blind trials (between 8 and 16 weeks in duration) of flexible-dose pregabalin (150–600 mg/day). Individual patient data were pooled into three groups by disease condition: diabetic peripheral neuropathy or postherpetic neuralgia (n=514), spinal cord injury (n=356), and fibromyalgia (n=498). Responders were classified as having a ≥30% and/or ≥50% reduction in mean pain score from baseline; once a patient responded, they were not scored subsequently (and were excluded from the responder analysis). The emergence of adverse events at each week was also recorded.
Results
The majority of the 30% and 50% responders emerged within the first 3–4 weeks with pregabalin, but were more uniformly distributed across the 6 weeks of the analysis with placebo. The majority of common adverse events also emerged within the first 3–4 weeks of pregabalin treatment.
Conclusion
These data suggest that the majority of pain responders and common adverse events emerge within 3–4 weeks of treatment with pregabalin. These data could advise new proof-of-concept studies and guide clinical management.
Introduction
Pregabalin is an α2δ ligand that is indicated in the USA for the treatment of neuropathic pain associated with diabetic peripheral neuropathy (DPN), postherpetic neuralgia (PHN), spinal cord injury (SCI), and fibromyalgia (FM), and as adjunctive therapy for partial onset seizures.Citation1 Painful DPN and PHN are peripheral neuropathic pain syndromes affecting up to 20%–30% of patients with diabetesCitation2 or herpes zoster infection.Citation3,Citation4 Patients with SCI typically experience some form of chronic pain, with up to 40% experiencing neuropathic pain 5 years after injury.Citation5 FM is a chronic pain disorder, with widespread pain and tenderness being the characteristic symptoms.Citation6,Citation7 Estimates of the incidence of FM in the adult US population range from 2% to more recent estimates of 6%.Citation8,Citation9
Each of these chronic pain conditions have a substantial impact on patients’ health-related quality of life.Citation10–Citation12 They are also often challenging to treat, particularly so in patients who may not respond immediately to treatment due to subtherapeutic doses or being unable to tolerate therapy.Citation13–Citation15 Physicians treating these patients with pregabalin would benefit from a better understanding of when patients are most likely to respond in order to better plan their treatment strategy. Similarly, a greater understanding of when the most common adverse events (AEs) emerge or worsen could aid physicians and patients, particularly in cases where anticipation of mild AEs could facilitate improved medication adherence. Researchers designing proof-of-concept studies for new pain conditions could be guided by information on how quickly a treatment effect with pregabalin could be observed. Such information could help researchers avoid conducting unnecessarily long proof-of-concept studies. This is important, as guidelines for improving assay sensitivity in chronic pain clinical trials recommend shorter durations for proof-of-concept studies in order to maximize assay sensitivity.Citation16 At the same time, shorter duration proof-of-concept studies would be less expensive and would reduce the exposure of patients to a potentially ineffective therapy.
This study aimed to investigate the treatment response over the first 6 weeks of clinical trials of flexible-dose pregabalin in all chronic pain conditions for which pregabalin is an approved treatment option to determine when patients first respond to treatment and when new AEs emerge or worsen. In these trials, it was decided on a weekly basis over the first 3–4 weeks of the trial if each patient’s dose should be adjusted based on pain relief and AEs, after which patients completed the trial receiving their optimal dose. As the pregabalin dose was tailored to the patient’s needs, this type of study design is a better representation of real-world clinical practiceCitation17–Citation19 than a fixed-dose design, used to establish, typically for regulatory purposes, an effective dosing range for a population rather than an individual.
Materials and methods
Study design
This was a pooled analysis of patient level data from five randomized, placebo-controlled, parallel-group, double-blind trials of flexible-dose pregabalin. Two trials were in patients with DPN or PHN (n=514). One, a 12-week study, consisted of 141 patients on pregabalin (150–600 mg/day in which dosage adjustments, based on efficacy and tolerability, were allowed for the first 3 weeks after which the patient remained on their optimized dose for the remainder of the trial) and 65 on placebo.Citation20 The second was an 8-week study consisting of 206 patients on pregabalin (150–600 mg/day, dosage adjustments for the first 4 weeks and optimized dose for the remainder of the trial) and 102 on placebo (ClinicalTrials.gov identifier NCT00301223).Citation21 Two trials were in patients with neuropathic pain associated with SCI (n=356). The first was a 12-week study consisting of 70 patients with SCI receiving pregabalin (150–600 mg/day, dosage adjustments for the first 3 weeks) and 67 on placebo.Citation22 The second was a 17-week study of 112 patients with SCI receiving pregabalin (150–600 mg/day, dosage adjustments for the first 4 weeks) and 107 placebo (ClinicalTrials.gov identifier NCT00407745).Citation23 Finally, there was a 15-week study in patients with FM (n=498), in which 250 patients were treated with pregabalin and 248 with placebo (ClinicalTrials.gov identifier NCT00830167).Citation24 The FM trial included a 3-week dose-escalation/optimization phase where, after escalation from 150 mg/day to either 300 or 450 mg/day, the dose could be further adjusted (increased or decreased between 300 and 450 mg/day) for an additional 2 weeks. Patients then continued on their optimized dose for a 12-week, fixed-dose treatment period. These trials were selected as their flexible dosing design is a closer representation of the optimal treatment approach, where pregabalin should be carefully titrated to the highest tolerable dose in order to maximize efficacy.Citation17–Citation19
All patients in these studies were ≥18 years of age and had an average pain score of ≥4 on the 11-point numeric rating scale, where 0 is no pain and 10 is worst possible pain, during the study screening period, with ≥4 pain diaries completed. Patients with DPN were diagnosed with type 1 or type 2 diabetes mellitus and painful, symmetrical sensorimotor polyneuropathy for ≥6 months. Patients with PHN had neuropathic pain for ≥3 months following healing of the herpes zoster viral rash. Patients with SCI had a complete or incomplete SCI of ≥12 months’ duration, with chronic pain experienced continuously for ≥3 months or with remissions and relapses for ≥6 months. Patients with FM had a primary diagnosis of FM according to the 1990 American College of Rheumatology criteria for FM (widespread pain present for ≥3 months and pain in ≥11 of 18 tender points).
In one study in patients with DPN/PHN, the mean patient age was 62.2 years and the mean duration of DPN and PHN was 37.2 months and 4.7 years, respectively.Citation20 In the second study in patients with DPN/PHN, the mean age was 60.0 years (placebo) and 60.1 years (pregabalin) and the mean duration of DPN was 3.0 years (placebo) and 2.8 years (pregabalin), and PHN was 1.3 (pregabalin and placebo) years.Citation21 In the two studies of patients with SCI, the combined mean age was 47.2 and 47.7 years and the mean duration of pain was 107.8 and 108.1 months, for placebo and pregabalin, respectively.Citation25 In the study of patients with FM, the mean age was 46.7 and 47.9 years and the mean duration since onset of FM was 62.0 and 69.6 months, for placebo and pregabalin, respectively.Citation24
In one study of patients with DPN/PHN, the average daily pregabalin dose over the full treatment period was 372.2 mg/day.Citation20 In patients with SCI, the average daily dose of pregabalin over both studies was 370.0 mg/day.Citation25 In the study of patients with FM, the majority (178 of 250 [71.2%]) received the higher dose of pregabalin (450 mg/day) during the maintenance phase.Citation24
Pain responders
New responders were classified as having a ≥30% and/or ≥50% reduction in mean pain score from baseline.Citation26 Once a patient responded, they were not scored subsequently and were excluded from the ongoing analysis. Mean pain score was determined as the mean score over the past 7 days as recorded by patients in a daily pain diary and measured using the 11-point numeric rating scale scored from 0 (no pain) to 10 (worst possible pain). At each week for the first 6 weeks, the numbers of new 30% and 50% responders were determined and the proportion was compared with the total number of patients remaining (ie, those who had not responded in previous weeks or were withdrawn from the trial) was calculated.
Adverse events
AEs were recorded for the full duration of each trial. In this analysis, AEs were assessed weekly where an emerging AE was scored if it appeared for the first time, or if it increased in severity. Data are shown as the percentage incidence at each week for the first 6 weeks, given that the majority of common AEs emerged within this time frame.
Results
Efficacy
The emergence of 30% and 50% responders was similar across disease groups with, responders typically being apparent within the first 3–4 weeks of the analysis.
In patients with DPN/PHN, the number of 30% responders peaked at week 3 with pregabalin (15.0%, 22.1%, 26.8%, and 19.1% by week for weeks 1–4, respectively) and week 4 with placebo (5.4%, 15.6%, 19.5%, and 24.2% for weeks 1–4, respectively, ). In total, 231 patients (66.8%) with pregabalin and 87 (52.4%) with placebo were 30% responders after 6 weeks. The number of 50% responders peaked at 3 weeks with pregabalin (5.5%, 9.1%, 12.9%, and 10.6% for weeks 1–4, respectively) and 4 weeks with placebo (0.6%, 4.9%, 8.2%, and 12.6% for weeks 1–4, respectively, ). In total, 144 patients (41.6%) with pregabalin and 51 (30.7%) with placebo were 50% responders in the 6-week analysis.
Figure 1 Thirty percent responders by week with pregabalin and placebo. Responders had a 30% reduction in mean pain score. Once a patient responded, they were not scored subsequently and were excluded from the analysis. Data are shown for patients with (A) DPN/PHN, (B) SCI, and (C) FM.
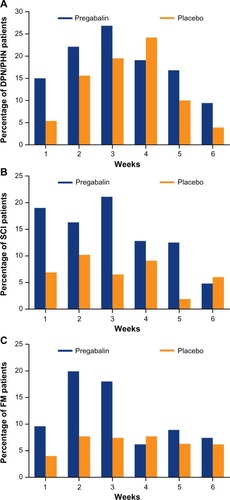
Figure 2 Fifty percent responders by week with pregabalin and placebo. Responders had a 50% reduction in mean pain score. Once a patient responded, they were not scored subsequently and were excluded from the analysis. Data are shown for patients with (A) DPN/PHN, (B) SCI, and (C) FM.
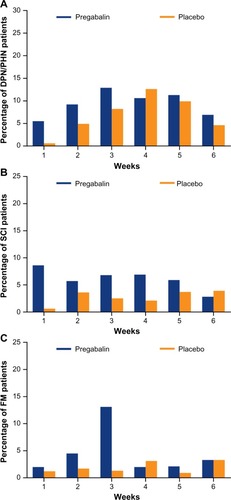
In patients with SCI, the majority of 30% responders emerged within the first 3 weeks of the SCI trials with pregabalin (19.0%, 16.3%, and 21.0% by week for weeks 1–3, respectively), but were more uniformly distributed across the duration of this analysis with placebo (6.9%, 10.2%, and 6.5% for weeks 1–3, respectively, ). In total, 103 patients (59.2%) with pregabalin and 56 (32.4%) with placebo were 30% responders in the 6-week analysis, with most of these emerging in the first 4 weeks. The majority of 50% responders emerged with the first 4–5 weeks of the trials with pregabalin (8.6%, 5.7%, 6.8%, 6.9%, and 5.9% for weeks 1–5, respectively) but were, again, more uniformly distributed across the duration of this analysis with placebo (0.6%, 3.6%, 2.5%, 2.1%, and 3.7% for weeks 1–5, respectively, ). In total, 53 patients (30.5%) with pregabalin and 24 (13.9%) with placebo were 50% responders in the 6-week analysis.
In patients with FM, the proportion of patients who were 30% responders peaked at week 2 with pregabalin (9.6%, 19.9%, and 18.0% by week for weeks 1–3, respectively) and weeks 2–4 with placebo (4.0%, 7.7%, 7.4%, and 7.7% for weeks 1–4, respectively, ). In total, 131 patients (52.4%) with pregabalin and 80 (32.3%) with placebo were 30% responders in this 6-week analysis, most of which emerged within the first 4 weeks. The proportion of patients who were 50% responders peaked at week 3 with pregabalin (2.0%, 4.5%, and 13.1% for weeks 1–3, respectively) and weeks 4–6 (1.2%, 1.6%, 1.3%, and 3.1% for weeks 1–4, respectively) with placebo (). In total, 60 patients (24.0%) with pregabalin and 26 (10.5%) with placebo were 50% responders in this 6-week analysis.
Emergence of adverse events
Similar to the analysis of responders, the majority of common AEs emerged within the time frame of this analysis and, for the most part, within the first 3–4 weeks.
In patients with DPN/PHN, the most common AEs (and their incidences) with pregabalin over the entire duration of the trials were dizziness (14.4%), peripheral edema (9.2%), somnolence (7.2%), and increased weight (6.3%).Citation20,Citation21 The majority of these instances of AEs emerged within 3–4 weeks of treatment with pregabalin, with the exception of peripheral edema, where the incidence was similar at each week from weeks 2–6 ().
Figure 3 Incidence of common adverse events with pregabalin. Numbers of the most common adverse events, either appearing for the first time or worsening in severity, by week for the first 6 weeks. Data are shown for patients with (A) DPN/PHN, (B) SCI, and (C) FM.
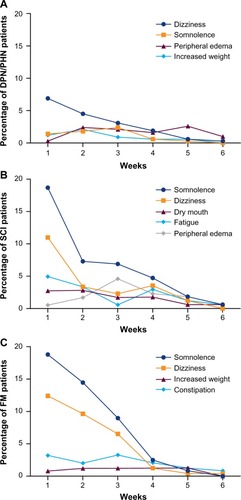
In patients with SCI, the most common AEs (and their incidences) with pregabalin across the duration of the trials were somnolence (35.7%), dizziness (20.9%), dry mouth (11.0%), fatigue (11.0%), and peripheral edema (10.4%).Citation25 The majority of these AEs emerged, or worsened, within the first 4 weeks of the trials. The incidence of most AEs peaked in the first week, with the exception of peripheral edema, which peaked at week 3 ().
In patients with FM, the most common AEs with pregabalin across the entire 15-week trial were somnolence, dizziness, increased weight, and constipation, with incidences of 46.4%, 29.6%, 15.6%, and 14.4%, respectively.Citation24 The majority of the total incidences of these AEs emerged within the first 4 weeks in this analysis. The incidence of somnolence and dizziness peaked at week 1, with a lower incidence at weeks 2 and 3, by which point the majority of incidences had emerged (). Constipation occurred at a similar incidence for each of the first 4 weeks, after which the incidence reduced.
Discussion
This analysis of five clinical trials of flexible-dose pregabalin for the treatment of those chronic pain conditions for which pregabalin is an approved therapy revealed that the majority of patients respond to treatment within the first 3–4 weeks of treatment. Similarly, the majority of the most common AEs in these trials had emerged within the first 3–4 weeks.
The total proportion of responders to emerge within the first 6 weeks in this analysis was similar to the proportion of responders reported at endpoint in each of the trials included in this analysis. For instance, the proportion of 30% responders at endpoint reported in the FM trial included in this analysis was 40.4% with pregabalin and 30.6% with placebo.Citation24 This is slightly lower than the proportion reported here, presumably as not all patients maintained a 30% response for the entire 15 weeks of the trial. Similarly, proportions of 30% responders at endpoint in the SCI (42% pregabalin, 16% placeboCitation5 and 45.7% pregabalin, 31.4% placeboCitation23) and DPN/PHN (59.0% pregabalin, 37.1% placeboCitation20 and 64.0% pregabalin, 52.0% placeboCitation21) trials were similar to the total proportion after 6 weeks in this analysis.
These data suggest that new proof-of-concept studies could be limited to as little as 3 weeks in duration as this time frame would be sufficient to capture the majority of responders and the most common AEs. For clinical practice, these data indicate that while most patients who will respond do so within the first 3–4 weeks, smaller numbers of new responders continue to emerge at weeks 5 and 6. Physicians treating patients with therapeutic doses of pregabalin can expect that if a patient will respond, it will likely be within the first 4 weeks; however, in some cases, it may be worthwhile to continue treatment for 6 weeks. This finding is not dissimilar to the reported time to onset for some antidepressants when improvement in depression is the primary endpoint. For example, while most patients who will ultimately respond to fluoxetine treatment do so within the first 2 weeks, approximately 25% of patients who respond only do so after 4 weeks of treatment.Citation27 Thus, if a patient has demonstrated a minimal or partial pattern of response to treatments for pain in the past, it would be important to observe the patient for a full 6 weeks on pregabalin, in order not to miss a pain response that could occur late in treatment.
DPN, PHN, neuropathic pain due to SCI, and FM are distinct diseases with only broad similarities as chronic pain conditions. This analysis looked at each of these conditions as they represent all of the chronic pain conditions for which pregabalin is approved by the US Food and Drug Administration as a treatment option.Citation1 As such, this analysis may offer guidance to physicians treating patients with pregabalin as an approved option. At the same time, the emergence of new responders and the majority of common AEs within 3–4 weeks in each of the conditions included in this analysis will give greater confidence to researchers planning a proof-of-concept study of pregabalin for another chronic pain condition that they will be able to observe most responses within this time frame.
The IMMPACT (Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials) considerations for improving assay sensitivity in chronic pain clinical trials recommend shorter durations for proof-of-concept studies in order to maximize assay sensitivity.Citation16 At the same time, results from a proof-of-concept trial with too short a duration may become a limitation when it comes to designing a longer duration confirmatory trial.Citation16 As such, finding the appropriate length for a new proof-of-concept trial in chronic pain can be challenging. Any data that can guide the decision-making process would be of great benefit. These analyses support the use of a 3- to 4-week proof-of-concept trial for pregabalin in chronic pain conditions.
These analyses included pregabalin data only from studies and treatment arms with a flexible dosing design, as this design is a closer representation of the recommended approach in clinical practice where pregabalin should be carefully titrated to the highest tolerable dose.Citation1,Citation17–Citation19 The recommended dosing for pregabalin in the USA is up to a maximum of 300 mg/day for DPN, between 300 and 600 mg/day for PHN, up to a maximum of 600 mg/day for SCI, and between 300 and 450 mg/day for FM.Citation1 For all conditions, it is recommended that treatment start at 150 mg/day and escalate to 300 mg/day within 1 week based on individual efficacy and tolerability.Citation1 Each of the trials in this analysis started with all patients receiving 150 mg/day before escalation to higher doses each week. As such, the emergence of 30% responders in this analysis after 1 week (15.0% with DPN/PHN, 19.0% with SCI, and 9.6% with FM) suggests a small degree of effectiveness of pregabalin, in some patients, before the optimal dose is reached. However, not all patients will respond to pregabalin at 150 mg/day, as also indicated here with higher numbers of responders at weeks 2 and 3. Current clinical guidelines support careful escalation to the highest tolerable approved dose,Citation1,Citation17–Citation19 with the reported average maintenance dose in the studies included in this analysis being ≥370 mg/day.
Consistent with previous studies,Citation19,Citation28 these analyses demonstrated that the most common AEs with pregabalin (somnolence and dizziness) typically emerge within the first 2 weeks. Other common AEs in these trials also tended to emerge within the 6 weeks of this analysis. One possible exception was increased weight in patients with FM (with 14 of 39 total instancesCitation24 emerging in the first 6 weeks). This observation is consistent with previous analyses indicating that increased weight typically emerges following a longer period of pregabalin treatment (>56 days).Citation29
The ability to anticipate which AEs may emerge, and when, could potentially improve adherence to pregabalin, by managing patient expectations. Some observational studies of pregabalin have reported lower rates of AEs and this has been credited to ongoing discussions between physicians and their patients regarding potential AEs.Citation30 It could be that this is related to a reduction in the patient’s anxiety, which then alters how they would perceive the occurrence of a mild AE.Citation19
A prior analysis of 31 clinical trials of pregabalin in patients with peripheral neuropathic pain conditions demonstrated that the majority of incidences of some common AEs were transient and resolved prior to the end of their study.Citation19 For dizziness and somnolence, respectively, median times to resolution were 9.0 and 14.0 days, with 74.5% and 64.8% of incidences resolving prior to the end of the study.Citation19 Although it was not a part of the current analysis, this suggests that the majority of cases of somnolence and dizziness would emerge, and then improve or resolve, within the first 4–6 weeks of treatment.
The data in this analysis suggest that the majority of new responders and new AEs emerge within the first 3–4 weeks of treatment with pregabalin. These data could advise researchers planning new proof-of-concept studies of pregabalin in pain conditions and also guide clinical management of patients with DPN, PHN, neuropathic pain due to SCI, and FM.
Acknowledgments
This study was sponsored by Pfizer. Medical writing support was provided by Joshua Fink of Engage Scientific Solutions, and funded by Pfizer.
Disclosure
BP, BE, and AC are employees of Pfizer and hold stock in Pfizer. The authors report no other conflict of interest in this work.
References
- Lyrica® (pregabalin)Prescribing InformationNew York, NY, USAPfizer Inc2011 Available from: http://labeling.pfizer.com/ShowLabeling.aspx?id=561Accessed September 19, 2014
- DaviesMBrophySWilliamsRTaylorAThe prevalence, severity, and impact of painful diabetic peripheral neuropathy in type 2 diabetesDiabetes Care20062971518152216801572
- DworkinRHPortenoyRKPain and its persistence in herpes zosterPain1996672–32412518951917
- KawaiKGebremeskelBGAcostaCJSystematic review of incidence and complications of herpes zoster: towards a global perspectiveBMJ Open201446e004833
- SiddallPJMcClellandJMRutkowskiSBCousinsMJA longitudinal study of the prevalence and characteristics of pain in the first 5 years following spinal cord injuryPain2003103324925712791431
- WolfeFClauwDJFitzcharlesMAThe American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severityArthritis Care Res (Hoboken)201062560061020461783
- WolfeFSmytheHAYunusMBThe American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Report of the Multicenter Criteria CommitteeArthritis Rheum19903321601722306288
- WolfeFRossKAndersonJRussellIJHebertLThe prevalence and characteristics of fibromyalgia in the general populationArthritis Rheum199538119287818567
- VincentALahrBDWolfeFPrevalence of fibromyalgia: a population-based study in Olmsted County, Minnesota, utilizing the Rochester Epidemiology ProjectArthritis Care Res (Hoboken)201365578679223203795
- DothAHHanssonPTJensenMPTaylorRSThe burden of neuropathic pain: a systematic review and meta-analysis of health utilitiesPain2010149233834420227832
- MurrayRFAsghariAEgorovDDImpact of spinal cord injury on self-perceived pre- and postmorbid cognitive, emotional and physical functioningSpinal Cord200745642943617228355
- ArnoldLMCroffordLJMeasePJPatient perspectives on the impact of fibromyalgiaPatient Educ Couns200873111412018640807
- DworkinRHO’ConnorABAudetteJRecommendations for the pharmacological management of neuropathic pain: an overview and literature updateMayo Clin Proc2010853 SupplS3S1420194146
- ArnoldLMClauwDJDuneganLJTurkDCA framework for fibromyalgia management for primary care providersMayo Clin Proc201287548849622560527
- FinnerupNBBaastrupCSpinal cord injury pain: mechanisms and managementCurr Pain Headache Rep201216320721622392531
- DworkinRHTurkDCPeirce-SandnerSConsiderations for improving assay sensitivity in chronic pain clinical trials: IMMPACT recommendationsPain201215361148115822494920
- AttalNCruccuGBaronREFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revisionEur J Neurol20101791113e8820402746
- FreemanRDurso-DecruzEEmirBEfficacy, safety, and tolerability of pregabalin treatment for painful diabetic peripheral neuropathy: findings from seven randomized, controlled trials across a range of dosesDiabetes Care20083171448145418356405
- FreynhagenRSerpellMEmirBA comprehensive drug safety evaluation of pregabalin in peripheral neuropathic painPain Pract2015151475724279736
- FreynhagenRStrojekKGriesingTWhalenEBalkenohlMEfficacy of pregabalin in neuropathic pain evaluated in a 12-week, randomised, double-blind, multicentre, placebo-controlled trial of flexible- and fixed-dose regimensPain2005115325426315911152
- GuanYDingXChengYEfficacy of pregabalin for peripheral neuropathic pain: results of an 8-week, flexible-dose, double-blind, placebo-controlled study conducted in ChinaClin Ther201133215916621444113
- SiddallPJCousinsMJOtteAGriesingTChambersRMurphyTKPregabalin in central neuropathic pain associated with spinal cord injury: a placebo-controlled trialNeurology200667101792180017130411
- CardenasDDNieshoffECSudaKA randomized trial of pregabalin in patients with neuropathic pain due to spinal cord injuryNeurology201380653353923345639
- OhtaHOkaHUsuiCOhkuraMSuzukiMNishiokaKA randomized, double-blind, multicenter, placebo-controlled phase III trial to evaluate the efficacy and safety of pregabalin in Japanese patients with fibromyalgiaArthritis Res Ther2012145R21723062189
- ParsonsBSaninLYangREmirBJuhnMEfficacy and safety of pregabalin in patients with spinal cord injury: a pooled analysisCurr Med Res Opin201329121675168323998397
- FarrarJTYoungJPJrLaMoreauxLWerthJLPooleRMClinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scalePain200194214915811690728
- NierenbergAAFarabaughAHAlpertJETiming of onset of antidepressant response with fluoxetine treatmentAm J Psychiatry200015791423142810964858
- Gil-NagelAZaccaraGBaldinettiFLeonTAdd-on treatment with pregabalin for partial seizures with or without generalisation: pooled data analysis of four randomised placebo-controlled trialsSeizure200918318419218951818
- CabreraJEmirBDillsDKevin MurphyTWhalenEClairACharacterizing and understanding body weight patterns in patients treated with pregabalinCurr Med Res Opin20122861027103722494020
- ToelleTVarvaraRNimourMEmirBBrasserMPregabalin in neuropathic pain related to DPN, cancer and back pain: analysis of a 6-week observational studyOpen Pain J20125111