
Abstract
Nocebo hyperalgesia has received sparse experimental attention compared to placebo analgesia. The aim of the present study was to investigate if personality traits and fear of pain could predict experimental nocebo hyperalgesia. One hundred and eleven healthy volunteers (76 females) participated in an experimental study in which personality traits and fear of pain were measured prior to induction of thermal heat pain. Personality traits were measured by the Big-Five Inventory-10. Fear of pain was measured by the Fear of Pain Questionnaire III. Heat pain was induced by a PC-controlled thermode. Pain was measured by a computerized visual analog scale. Stress levels during the experiment were measured by numerical rating scales. The participants were randomized to a Nocebo group or to a no-treatment Natural History group. The results revealed that pain and stress levels were significantly higher in the Nocebo group after nocebo treatment. Mediation analysis showed that higher levels of the Fear of Pain Questionnaire III factor “fear of medical pain” significantly increased stress levels after nocebo treatment and that higher stress levels were associated with increased nocebo hyperalgesic responses. There were no significant associations between any of the personality factors and the nocebo hyperalgesic effect. The results from the present study suggest that dispositional fear of pain might be a useful predictor for nocebo hyperalgesia and emotional states concomitant with expectations of increased pain. Furthermore, measurement of traits that are specific to pain experience is probably better suited for prediction of nocebo hyperalgesic responses compared to broad measures of personality.
Introduction
The nocebo hyperalgesic effect is defined as the increase in pain that follows the administration of an inert substance or procedure accompanied by suggestions of pain worsening.Citation1 Placebo analgesia is the opposite of nocebo hyperalgesia and is the reduction of pain after treatment by an inert substance or procedure administrated along with suggestions of pain relief. Nocebo hyperalgesia has received sparse scientific experimental attention compared to placebo analgesia.Citation2 The lack of studies investigating the nocebo effect in pain has been attributed to ethical constraints, which limit the experimental possibilities in both clinical and experimental settings.Citation3,Citation4 Nocebo-related effects can be produced in clinical settings, that is, by inducing negative expectations via information about the side effects of medications and procedures, which in turn reduce the efficacy of analgesic treatment.Citation5 However, the majority of studies on nocebo hyperalgesia have been performed in healthy volunteers. The existing studies on nocebo hyperalgesia have shown that negative emotional activation mediates the observed increase in painCitation6,Citation7 and that nocebo manipulations may affect physiological systems such as the hypothalamic–pituitary–adrenal axis,Citation8 cerebral pain systems,Citation9,Citation10 and pain processing in the spinal cord.Citation11 Anxiolytic drugs are capable of reversal of nocebo hyperalgesia, lending further support to the notion that emotional modulation is essential in nocebo hyperalgesic responding.Citation7
Studies on placebo analgesia have shown that there is substantial individual variability in placebo analgesic responding,Citation12 and it is likely that the same is true for nocebo hyperalgesia since nocebo hyperalgesia and placebo analgesia share common mechanisms.Citation13 The impact of global personality traits on placebo analgesia is unclear,Citation14 but there is evidence that the personality trait, neuroticism, is associated with reduced placebo analgesia.Citation15 Neuroticism is the tendency to experience negative emotions and cognitions that often accompany experiences of threat and punishment and is associated with elevated levels of anxiety, depression, anger, irritation, self-consciousness, rumination, and vulnerability.Citation16 Negative emotions increase pain,Citation17 and it is therefore reasonable to expect that individuals with high neuroticism are more prone to be affected by suggestions of pain increase compared to those with lower neuroticism. Personality traits, however, are general indicators of behavior and not specifically predictive of pain experience. Traits that are pain specific might be equally or more predictive of pain experience than general personality traits. One such trait is fear of pain.Citation18 Fear of pain refers to the dispositional tendency to react with negative emotions to pain and in the anticipation of pain.Citation18 High levels of fear of pain are shown to decrease placebo analgesic responses.Citation12,Citation19 To date, no previous experimental study has examined the impact of personality or fear of pain in nocebo hyperalgesia.
In the present study, we measured global personality traits and fear of pain in healthy volunteers before induction of nocebo hyperalgesia in order to investigate their impact on the nocebo effect. We hypothesized that increased levels of the personality trait, neuroticism, would be associated with increased nocebo hyperalgesia. Likewise, based on previous findings that link increased fear of pain to reduced placebo analgesia, we expected that higher levels of fear of pain would be associated with higher levels of nocebo responses in pain. Finally, we expected that higher levels of both fear of pain and neuroticism would increase subjective negative emotional states after administration of nocebo treatment and thereby mediate the effect of neuroticism and fear of pain on the nocebo effect.
Methods
Subjects
One hundred and twenty healthy volunteers between the age of 19 and 38 were recruited by an advertisement at the University of Tromsø, Norway. Due to missing pain data in four subjects and missing questionnaire data in five subjects, 111 participants (female: n=76; mean age =22.21, standard deviation =3.10) were included in the statistical analyses. Exclusion criteria were current or previous severe disease (including chronic pain), pregnancy, cutaneous injuries on the arms and hands, and use of prescription medication (with the exception of oral contraceptives). All participants signed an informed consent form that stated they had no medical history of any serious diseases or injuries. All volunteers received a gift certificate worth 200 Norwegian Kroner. The study was approved by the Regional Committee for Medical Research Ethics, Region North, Project no 402/2012.
Design
A two group (Natural History, Nocebo) × three trials (Pretest, Posttest 1, Posttest 2) mixed design was used in the experiment. Four psychology students (two males and two females) with extensive experience with experimental laboratory work conducted the experiment. The experimenters were not informed of which group the subjects belonged to until after the pretest. After the pretest, the experimenters opened an envelope that stated whether the participant should receive the nocebo treatment or the no-treatment condition (Natural History group).
Group alignment was randomized by an algorithm at RANDOM.ORG.Citation20 Calculations of group size were based on data from a previous studyCitation6 in which mean differences between the Nocebo groups and the Natural History group were between 7 mm and 11 mm on a 100 mm visual analog scale (VAS). Expected standard deviation in the sample was 16 VAS points. By including 50 participants in each group and using an alpha of 5% with two-tailed testing, a power estimate of 87% was calculated. To ensure power in the analyses when assuming a loss of data of ~10% due to missing scores, experimenter error, etc, we recruited a total of 120 participants.
Pain stimuli
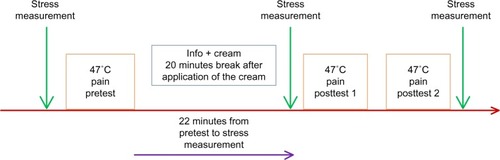
Pain was induced by contact with heat stimuli (30×30 mm aluminum contact thermode, [Pathway, Medoc, Israel]) applied to the right volar forearm. The thermode had a baseline temperature of 32°C when applied to the arm. The duration of the pain stimuli was 20 seconds with a plateau for ~16 seconds at 47°C in both the pretest and the posttests. The thermode rise/fall rate was 10°C/second.
Questionnaires
Personality was measured with the Big-Five Inventory-10 (BFI-10).Citation21 The BFI-10 is an abbreviated version of the BFI-44,Citation22 which measures the five-factor model of personality. The BFI-10 is considered to be a valid and reliable measure of the five-factor model of personality.Citation23 The five factors are Extraversion, Agreeableness, Conscientiousness, Neuroticism, and Openness. The BFI-10 is scored on a 5-point Likert scale.
Fear of pain was measured with the Norwegian version of the Fear of Pain Questionnaire III (FPQ-III).Citation12,Citation19,Citation24 FPQ-III consists of three subscales designed to tap fear related to severe pain (eg, breaking your arm), minor pain (eg, getting a paper cut in your finger), and medical pain (eg, having a blood sample drawn with a hypodermic needle). Each subscale consists of ten items. Each item is scored on a 5-point Likert scale. Previous studies have demonstrated good internal consistency for the measure and good test–retest reliability.Citation18,Citation25
Pain and negative emotional states measurements
During each pain stimulus, the participants reported their pain intensity on a computerized visual analog scale (COVAS; Medoc, Israel) ranging from 0 to 100, where 0 represented “no pain” and 100 represented the “most intense pain imaginable”. The mean of the continuous pain rating during the stimuli was used as the pain score for each subject in each trial. Subjective stress was measured by two adjective pairs, similar to those used in previous studies,Citation12,Citation26,Citation27 from the Norwegian translation of the Short Adjective Check List.Citation28 The adjective pairs were tense-relaxed and nervous-calm. The adjective pairs were converted to numerical rating scales, where a score of zero indicated complete relaxation/calmness and a score of ten indicated maximum tension/nervousness. The stress score was expressed as the mean score for the two adjective pairs. Stress measures were obtained before the pretest, immediately after the administration of the nocebo cream, and immediately after the posttest.
Nocebo cream
The university hospital pharmacy at the University Hospital of Northern Norway produced 100-mL tubes of nocebo cream (E45 Cream; Crookes Healthcare, UK). All tubes were numbered according to a list of codes and had an identical design. The code list was created by the university hospital pharmacy and was kept by the supervisor of the study (PMA), who did not participate in the experimental work. We chose the E45 cream as the nocebo cream based on its similarities to local anesthetic creams in color, odor, and consistency. A dose of 3 g of nocebo (E45) was used for each participant, similar to a previously published study.Citation6
Procedure
The experiment took place in a laboratory shielded from sound and electricity where a constant temperature of 20°C was maintained. Upon arrival at the laboratory, the participants signed an informed consent form. The participants received written information together with the consent form stating that the aim of the study was to test the physiological and psychological effects of a medical cream on heat pain. The participants were informed that they would receive a cream that increased pain or no treatment during the pain stimulation (Natural History group). The participants did not know what treatment they received or whether they participated in the control group until after the pretest.
After the experimenter received the signed consent, each participant was seated on a comfortable chair inside the cubicle. Then, the experimenters instructed the participant on how to use the COVAS and attached the thermode to the volar right forearm, at the dermatome corresponding to C8. Subsequently subjective stress was measured. Each participant then received a pain stimulus at 46°C for 5 seconds duration prior to the pretest to reduce novelty of the heat pain experience.
After a 2-minute break, the experimenter started the first pain stimulation (pretest). Following the pretest, the experimenter delivered information regarding the cream, followed by application of the cream to a 5×5 cm location on the right volar forearm. The instructions for the cream were as follows: the Nocebo group was told, “The cream that will be applied to your arm increases the effect of the heat pain and you will feel more pain after the application. The substance in this cream is used in many medical remedies. Even though the pain feels more intense, the cream will not inflict any burn wounds”. In the Natural History condition, no cream was applied and no information regarding medication was given. During the break, the participants in the Natural History group were told to relax for a few minutes and to wait for the procedure to continue.
Following a 20-minute application period, subjective stress was measured. Subsequently, the thermode was again attached to the forearm 1 cm below the site of the thermode stimulation in the pretest to avoid possible lesion-related hyperalgesia, and the experimenter initiated the last two pain stimulations (posttests). The interval between the posttests was 2 minutes. After the last posttest, the final subjective stress measurement was obtained. The experimental procedure had a total duration of ~45 minutes. shows an overview of the procedure.
Figure 1 Overview of the experimental procedure.
Statistical analyses
All data were analyzed in SPSS Version 22 (IBM Corporation, Armonk, NY, USA). Tests for normality were performed by the Kolmogorov–Smirnov test. Due to violations of the assumptions of normally distributed data for pain, stress, and questionnaire data, we used nonparametric statistics for correlation analysis (Spearman correlations) and for the group by trial analysis (Friedman test). Pairwise Wilcoxon tests were used for comparisons of trials within groups. Mann–Whitney U-tests were employed to test the differences between the groups at each trial. A P-value <0.05 was considered significant for the analyses except the group comparisons in the repeated measures of pain and stress data where Bonferroni corrections were employed to correct for multiple comparisons (P<0.05/three trials [Pretest, Post-test 1, Posttest 2] = P<0.0167). To test the hypothesis that fear of pain produces increased levels of stress that in turn causes increased pain, we performed a mediation analysis.Citation29,Citation30 Mediation is present when a predictor (eg, fear of pain) affects an independent variable (eg, pain) indirectly through at least one intervening variable (eg, stress). A simple mediation model involves three steps that uses simple and multiple regressions: first, the dependent variable is regressed on the independent variable; second, the mediator is regressed on the independent variable; and finally, the dependent variable is regressed on both the independent variable and the mediator.Citation31 The mediation analysis employed in the present study is an advanced development of the above mentioned model that uses nonparametric bootstrapping for testing of indirect effects and allows the test of effects of covariates for the model. For further mathematical and technical details, see Preacher and Hayes.Citation30
Results
Mean values for pain and stress are displayed in and , respectively. displays descriptive data for BFI-10 and FPQ-III in the present sample. shows the correlations between the FPQ factors and the personality factors. The Friedman test revealed that there were significant differences in pain ratings across trials (Pretest, Posttest 1, Posttest 2) in the Nocebo group (χ2(2)=73.71, P<0.001) and in the Natural History group (χ2(2)=25.96, P<0.001). Pairwise Wilcoxon tests displayed that pain scores were significantly different in both groups when comparing Pretest–Posttest 1, Pretest–Posttest 2, and Posttest 1–Posttest 2, all Z’s <−2.74, all P’s <0.001. Mann–Whitney U-tests were used for group comparisons in each trial (Pretest, Posttest 1, Posttest 2) and revealed that there was no significant group difference in the Pretest, but significantly higher pain reports in the Nocebo group compared to the Natural History group in both posttests (). When adjusting for multiple comparisons by Bonferroni corrections, all mean values in the posttests were still significantly higher in the Nocebo group compared to the Natural History group, and pain increased across time/posttests (). In the stress data, the Fried-man test showed that there were significantly different levels of stress across trials in the Nocebo group (χ2(2)=15.75, P<0.001) and in the Natural History group (χ2(2)=54.45, P<0.001). Pairwise Wilcoxon tests revealed that stress was higher in both posttests (both Zs <−3.54, both Ps <0.001) compared to the pretest in the Nocebo group but that there was no difference in stress when comparing the posttests in the Nocebo group (Z=−0.63, P=0.52). In the Natural History group, stress reports were higher in both posttests compared to the pretest (both Zs <−5.2, both Ps <0.001), but there was no significant difference between the posttests (Z=−0.34, P=0.72). Mann–Whitney U-tests showed that stress levels of the Nocebo group were significantly higher in both posttests compared to the Natural History group when considering the Bonferroni-adjusted P-value of 0.0167 ().
Table 1 Pain ratings in each trial and change scores
Table 2 Stress reports in each trial and change scores
Table 3 Big-Five Inventory-10 (BFI-10) and the Fear of Pain Questionnaire III (FPQ-III)
Table 4 Spearman correlations between the factors of the Fear of Pain Questionnaire III (FPQ-III) and the factors of the Big-Five Inventory-10 (BFI-10) for all participants
The effect of fear of pain on the nocebo hyperalgesic effect was tested by mediation analysisCitation30 with the change in pain (pretest−posttest) as the dependent variable and the change in stress (pretest−posttest) after the nocebo manipulation as the mediator. Before the mediation analysis, we performed a partial correlation analyses in each group to display the association between the change in pain and the three factors in FPQ-III and the five personality factors measured by the BFI-10. The control variables for the partial correlation were sex and age. Contrary to our hypothesis, there was no significant association between any of the personality factors and the change in pain in the Nocebo or the Natural History group. The only significant association in the Nocebo group was the correlation between the FPQ factor “fear of medical pain” and the change score in the Nocebo group (r=−0.29, P=0.03). In the Natural History group, the only significant correlation was between the FPQ factor “fear of medical pain” and the pain change score (r=−0.42, P=0.003). Thus, “fear of medical pain” was the only pain-related personality trait that was used as a dependent variable in the mediation models.
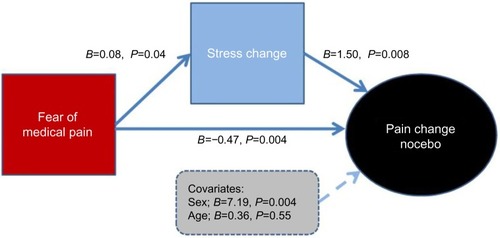
The mediation analysisCitation30 for the Nocebo group revealed that there was a direct effect of “fear of medical pain” on the change score in pain (B=−0.47, t=−2.99, P=0.004).
The total effect of “fear of medical pain” on pain change when controlling for sex and age was significant (B=−0.35, t=−2.17, P=0.03). The change in reported stress mediated the change in pain (nocebo effect), shown by the effect of “fear of medical pain” on the change in stress (B=0.08, t=2.06, P=0.04) and by the effect of stress change on pain change (B=1.50, t=2.73, P=0.008). The covariate sex was significant, showing that females reported a higher nocebo effect compared to males (B=7.21, t=3.03, P=0.004). There was no effect of the covariate age (P=0.55). The explained variance for the whole model was 32% (R2=0.32). shows an overview of the mediation model in the Nocebo group. When performing the same mediation model on the Natural History group, no significant mediation effects were found, and the relation of “fear of medical pain” to stress change was nonsignificant (B=0.03, t=0.77, P=0.43).
Figure 2 Overview of the mediation analysis for the Nocebo group.
Discussion
In line with our hypothesis, we found a significant association between increased levels of fear of medical pain and nocebo hyperalgesia. On the other hand, our data did not support the hypothesis that the personality trait, neuroticism, had an impact on reported pain increase after the nocebo manipulation. The mediation analysis showed that increased levels of the FPQ factor “fear of medical pain” increased stress levels after the nocebo treatment, and thereby potentiated the nocebo hyperalgesic effect (). Previous studies have suggested that increased level of negative emotions is central for nocebo hyperalgesia to occur,Citation3,Citation6 and the results support this by showing that verbal suggestions of pain increase heighten negative emotional states, which in turn increase pain.Citation32 The lack of association between personality traits and nocebo responding is similar to findings from several placebo analgesic studies in which the relation between placebo effects and personality factors is vague or absent.Citation14 Nonetheless, some studies have found an effect of specific traits,Citation15,Citation33,Citation34 and studies on this topic with larger samples are warranted.
Our finding that “fear of medical pain” predicted nocebo hyperalgesia and that neuroticism did not, supports the notion that the placebo and nocebo effects are modality-specific,Citation35 due to the fact that the FPQ-III is a measure specifically for pain and settings involving pain. It may therefore be difficult to relate nocebo effects in pain to superordinate personality traits measured by the five-factor model. In line with the principles of trait activation, which states that the activation/expression of a trait requires arousal by trait-relevant situational cues, “fear of medical pain” appears to tap emotional response patterns related to fear and anxiety in a pain-laboratory setting and possibly also in a clinical medical setting in which pain is anticipated. The other two factors on the FPQ-III were not related to the change in pain after nocebo manipulation in the present study. Both the factors “fear of minor pain” and “fear of severe pain” might represent pain situations that have less relevance as compared to the experimental setting that was used in the present study.
The present experiment was not designed to test for sex differences in the nocebo hyperalgesic response, but the results showed that females reported higher pain after the nocebo treatment compared to males. A previous studyCitation36 has found similar sex differences in nocebo responding in nausea, and others have suggested that pain-related anxiety might be higher in females.Citation37 Future studies could further investigate possible sex differences in nocebo hyperalgesia. One possibility of nocebo-related sex differences is the interaction of sex- and pain-related genetic expressions that in clinical studies have been shown to affect pain levels in chronic pain conditions.Citation38 A limitation in our experimental design is the lack of a group that received placebo cream without suggestions of any change in pain. The administration of medications itself may cause elevations in stress, and a group that received reduced or no information about the effect of the cream may have provided the opportunity to separate the stress induced by the nocebo information from the stress induced by the treatment itself.
Our results suggest that dispositional fear of pain might be useful in predicting nocebo hyperalgesic responding and the negative emotional states that contribute to the variability in these responses. Finding predictors for nocebo hyperalgesia is important since in clinical practice, nocebo responses are probably at least as important as placebo.Citation39 Fear and anxiety toward medical procedures are associated with negative treatment outcome,Citation40,Citation41 and even reduced placebo responding.Citation23 Furthermore, identification of patients with elevated levels of pain-related fear and anxiety might also aid medical professionals in performing adequate adaptions for the single patient in order to optimize treatment effects.
Acknowledgments
The present study was funded by the University of Tromsø, Tromsø, Norway.
Disclosure
The authors report no conflicts of interest in this work.
References
- PetersenGLFinnerupNBCollocaLThe magnitude of nocebo effects in pain: a meta-analysisPain201415581426143424780622
- EnckPBenedettiFSchedlowskiMNew insights into the placebo and nocebo responsesNeuron200859219520618667148
- CollocaLBenedettiFNocebo hyperalgesia: how anxiety is turned into painCurr Opin Anaesthesiol200720543543917873596
- CollocaLFinnissDNocebo effects, patient-clinician communication, and therapeutic outcomesJAMA2012307656756822318275
- MyersMGCairnsJASingerJThe consent form as a possible cause of side effectsClin Pharmacol Ther19874232502533621780
- AslaksenPMZwargMLEilertsenHIGoreckaMMBjorkedalEOpposite effects of the same drug: reversal of topical analgesia by nocebo informationPain20151561394625599299
- BenedettiFLanotteMLopianoLCollocaLWhen words are painful: unraveling the mechanisms of the nocebo effectNeuroscience2007147226027117379417
- BenedettiFAmanzioMVighettiSAsteggianoGThe biochemical and neuroendocrine bases of the hyperalgesic nocebo effectJ Neurosci20062646120141202217108175
- FreemanSYuREgorovaNDistinct neural representations of placebo and nocebo effectsNeuroimage201511219720725776211
- KongJGollubRLPolichGA functional magnetic resonance imaging study on the neural mechanisms of hyperalgesic nocebo effectJ Neurosci20082849133541336219052227
- GeuterSBuchelCFacilitation of pain in the human spinal cord by nocebo treatmentJ Neurosci20133334137841379023966699
- LybyPSAslaksenPMFlatenMAVariability in placebo analgesia and the role of fear of pain – an ERP studyPain2011152102405241221875771
- PetrovicPPlacebo analgesia and nocebo hyperalgesia – two sides of the same coin?Pain20081361–25618367334
- LundKPetersenGLErlandsenMThe magnitude of placebo analgesia effects depends on how they are conceptualizedJ Psychosom Res Epub2015516
- PeciñaMAzharHLoveTMPersonality trait predictors of placebo analgesia and neurobiological correlatesNeuropsychopharmacology201238463964623187726
- DeYoungCGPersonality neuroscience and the biology of traitsSoc Personal Psychol Compass201041211651180
- RhudyJLMeagherMWThe role of emotion in pain modulationCurr Opin Psychiatry2001143241245
- McNeilDWRainwaterAJ3rdDevelopment of the fear of pain questionnaire-IIIJ Behav Med19982143894109789168
- LybyPSAslaksenPMFlatenMAIs fear of pain related to placebo analgesia?J Psychosom Res201068436937720307704
- RANDOM.ORG [homepage on the Internet];Ireland: True Random Number Service Available from: https://www.random.org/Accessed October 2, 2015
- RammstedtBJohnOPMeasuring personality in one minute or less: a 10-item short version of the big five inventory in English and GermanJ Res Pers2007411203212
- JohnOPDonahueEMKentleRLThe Big Five Inventory – Versions 4a and 54Berkeley, CAUniversity of CaliforniaBerkeleyInstitute of Personality and Social Research1991
- HahnEGottschlingJSpinathFMShort measurements of personality – validity and reliability of the GSOEP big five inventory (BFI-S)J Res Pers2012463355359
- LybyPSForsbergJTAsliOFlatenMAInduced fear reduces the effectiveness of a placebo intervention on painPain201215351114112122464696
- RoelofsJPetersMLDeutzJSpijkerCVlaeyenJWThe fear of pain questionnaire (FPQ): further psychometric examination in a non-clinical samplePain2005116333934615979794
- AslaksenPMBystadMVambheimSMFlatenMAGender differences in placebo analgesia: event-related potentials and emotional modulationPsychosom Med201173219319921217098
- AslaksenPMFlatenMAThe roles of physiological and subjective stress in the effectiveness of a placebo on experimentally induced painPsychosom Med200870781181818725424
- MackayCCoxTBurrowsGLazzeriniTAn inventory for the measurement of self-reported stress and arousalBr J Soc Clin Psychol1978173283284687885
- PreacherKJHayesAFSPSS and SAS procedures for estimating indirect effects in simple mediation modelsBehav Res Methods Instrum Comput200436471773115641418
- PreacherKJHayesAFAsymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator modelsBehav Res Methods200840387989118697684
- BaronRMKennyDAThe moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerationsJ Pers Soc Psychol1986516117311823806354
- RhudyJLBartleyEJWilliamsAEHabituation, sensitization, and emotional valence modulation of pain responsesPain2010148232032720022696
- YuRGollubRLVangelMKaptchukTSmollerJWKongJPlacebo analgesia and reward processing: integrating genetics, personality, and intrinsic brain activityHum Brain Mapp20143594583459324578196
- PecinaMLoveTStohlerCSGoldmanDZubietaJKEffects of the Mu opioid receptor polymorphism (OPRM1 A118G) on pain regulation, placebo effects and associated personality trait measuresNeuropsychopharmacology201540495796525308352
- BenedettiFMaybergHSWagerTDStohlerCSZubietaJKNeurobiological mechanisms of the placebo effectJ Neurosci20052545103901040216280578
- KlosterhalfenSKellermannSBraunSGender and the nocebo response following conditioning and expectancyJ Psychosom Res200966432332819302890
- GoffauxPMichaudKGaudreauJChalayePRainvillePMarchandSSex differences in perceived pain are affected by an anxious brainPain201115292065207321665365
- OlsenMBJacobsenLMSchistadEIPain intensity the first year after lumbar disc herniation is associated with the A118G polymorphism in the opioid receptor mu 1 gene: evidence of a sex and genotype interactionJ Neurosci201232299831983422815498
- CollocaLMillerFGThe nocebo effect and its relevance for clinical practicePsychosom Med201173759860321862825
- VarelmannDPancaroCCappielloECCamannWRNocebo-induced hyperalgesia during local anesthetic injectionAnesth Analg2010110386887020042440
- WangFShenXXuSNegative words on surgical wards result in therapeutic failure of patient-controlled analgesia and further release of cortisol after abdominal surgeriesMinerva Anestesiol2007747–835336518612266